


Abstract
A new tracer, 4′-[methyl-11C]-thiothymidine (11C-4DST), has been developed as an in vivo cell proliferation marker based on the DNA incorporation method. This study evaluated the potential of 11C-4DST PET/CT for imaging proliferation in non–small cell lung cancer (NSCLC), compared with 18F-FDG PET/CT. Methods: Eighteen patients with lung lesions were examined by PET/CT using 11C-4DST and 18F-FDG. We constructed decay-corrected time–activity curves of 9 major regions as the mean standardized uptake value. We then compared the maximum standardized uptake value (SUVmax) of lung tumors on both 11C-4DST and 18F-FDG PET/CT with the Ki-67 index of cellular proliferation and with CD31-positive vessels as a marker of angiogenesis in surgical pathology. Results: NSCLC was pathologically confirmed in 19 lesions of 18 patients. Physiologic accumulation of 11C-4DST was high in liver, kidney, and bone marrow and low in aorta, brain, lung, and myocardium. Biodistribution of 11C-4DST was almost stable by 20 min after injection of 11C-4DST. Mean 11C-4DST SUVmax for lung cancer was 2.9 ± 1.0 (range, 1.5–4.7), significantly different from mean 18F-FDG SUVmax, which was 6.2 ± 4.5 (range, 0.9–17.3; P < 0.001). The correlation coefficient between SUVmax and Ki-67 index was higher with 11C-4DST (r = 0.82) than with 18F-FDG (r = 0.71). The correlation coefficient between SUVmax and CD31 was low with both 11C-4DST (r = 0.21) and 18F-FDG (r = 0.21), showing no significant difference between the tracers. Conclusion: A higher correlation with proliferation of lung tumors was seen for 11C-4DST than for 18F-FDG. 11C-4DST PET/CT may allow noninvasive imaging of DNA synthesis in NSCLC.
Uncontrolled proliferation is a distinctive characteristic of cancer cells (1). The ability to image cellular proliferation would offer the possibility of distinguishing between benign and malignant tissues, measuring tumor activity, and evaluating response to therapy (2). Cellular proliferation is thus a key characteristic in oncology, and its imaging has been a critical goal of nuclear medicine.
Proliferating cells synthesize DNA during the S phase of the cell cycle. The pyrimidine analog thymidine is incorporated into DNA but not into RNA. DNA incorporation of 3H-thymidine is considered the gold standard for characterizing cell proliferation (1,2).
The first PET tracer for imaging cellular proliferation was thymidine labeled with 11C at the methyl group (methyl-11C-thymidine) (3). However, degradation in vivo resulted in ambiguous evidence for imaging of cellular proliferation. Assessment of thymidine flux from blood into DNA has been clarified in a multicompartment, metabolite-corrected kinetic model of imaging data using thymidine labeled with 11C at the 2-position (2-11C-thymidine) in somatic and brain tumors (4–7). However, the complexity of 2-11C-thymidine PET in terms of methods and analysis seems likely to preclude widespread clinical use in cellular proliferation imaging. Although 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) has achieved good clinical results for cellular proliferation imaging (8), 18F-FLT is not incorporated into DNA because of the lack of a 3′-hydroxyl, unlike thymidine. As a result, 18F-FLT imaging is regarded as the salvage pathway of DNA synthesis (2).
Toyohara et al. developed 4′-thiothymidine labeled with 11C at the methyl group (4′-[methyl-11C]-thiothymidine [11C-4DST], previously designated as 11C-S-dThd) as a new candidate tracer for cell proliferation imaging that is resistant to degradation by thymidine phosphorylase and is incorporated into DNA (9,10). Moreover, 14C-4DST has shown significantly higher uptake into proliferating tissues than FLT labeled with 3H at the methyl group, a result supported by an animal study using 11C-4DST (10). In a human study using 11C-4DST, Toyohara et al. showed that true input curves after metabolite analysis and dynamic brain tumor imaging resulted in a linear Patlak plot over 10–90 min after injection and suggested metabolic incorporation of 4DST into higher molecules, such as DNA (11).
An 11C-4DST PET study of patients with brain tumor showed that 11C-4DST PET is feasible for brain tumor imaging and can be performed with acceptable dosimetry and pharmacologic safety at a suitable dose for adequate imaging (11). Individual-organ and total-body doses associated with 11C-4DST are reportedly lower than those with 18F-FLT (11,12). Although the short physical half-life of 11C places a significant limitation on counting statistics and commercial convenience for widespread routine clinical use, diagnosis using multiple tracers to determine tumor characteristics is possible, and repeated scans during the course of therapy are feasible given the lower radiation burden.
These results indicate that 11C-4DST has great potential for imaging cell proliferation, but this potential needs to be confirmed in a variety of cancers. Tumor cell proliferation is one of the most significant predictors of prognosis for patients with cancers such as non–small cell lung cancer (NCSLC) (13). The present study evaluated the potential of 11C-4DST PET/CT, compared with 18F-FDG PET/CT, for imaging proliferation in NSCLC.
MATERIALS AND METHODS
Patients
This prospective study was approved by the institutional review board at our facility, and written informed consent was obtained from all patients before participation. A total of 18 patients (12 men and 6 women; mean (±SD) age, 68.1 ± 9.4 y; range, 55–84 y) with histologically confirmed NSCLC were included in this study. All patients underwent chest CT before 11C-4DST and 18F-FDG PET/CT examinations, which were performed before surgical resection of the lung lesion.
11C-4DST PET/CT Examination
The 11C-4DST was synthesized as previously described (11). PET/CT images were obtained using a system (Biograph 16; Siemens) consisting of a PET scanner and multidetector-row CT scanner (16 detectors), measuring from vertex to thigh. All subjects fasted for 5 h before receiving an intravenous injection of 11C-4DST within the range of 666–777 MBq. Low-dose CT was performed first and was used for attenuation correction and image fusion. Emission images were acquired in 3-dimensional mode for 2 min/bed position to obtain an image at 5 min after intravenous injection of 11C-4DST and 2.5 min/bed position to obtain images at 20, 40, 60, and 80 min after intravenous injection of 11C-4DST. PET data were reconstructed using a gaussian filter with an ordered-subset expectation maximization algorithm (3 iterations, 8 subsets). Images with 11C-4DST were obtained from all patients at 40 min after intravenous injection of 11C-4DST. Additional 11C-4DST images were obtained from some patients at 5 min (n = 5), 20 min (n = 6), 60 min (n = 9), and 80 min (n = 9) after intravenous injection of 11C-4DST.
18F-FDG PET/CT Examination
An in-house cyclotron and automated synthesis system (F100; Sumitomo Heavy Industries) was used in accordance with the authorized procedure to synthesize 18F-FDG. All subjects fasted for 5 h before blood glucose levels were measured and 18F-FDG intravenously injected (370 MBq). PET/CT images were obtained at 60 min after injection with the same method as for 11C-4DST. For 13 patients, 18F-FDG PET/CT scans were obtained 90 min or more after the 11C-4DST PET/CT scans. For the other patients, the interval between 11C-4DST and 18F-FDG PET/CT was 2 d for 1 patient, 5 d for 1 patient, 11 d for 1 patient, and 23 d for 2 patients.
PET Data Analysis
All 11C-4DST and 18F-FDG PET/CT scans were evaluated by 2 experienced nuclear medicine physicians who were unaware of the clinical data. Regions of interest were placed in the lung lesion according to CT images obtained from PET/CT, and maximum standardized uptake value (SUVmax) and mean standardized uptake value (SUVmean) were determined for 11C-4DST and 18F-FDG PET/CT images, respectively. Regions of interest were placed in the following organs: ascending aorta (blood pool), brain, lungs, myocardium, liver, kidneys, muscle, and bone marrow. The decay-corrected time–activity curves of 9 regions (8 organs and the tumor) were identified as the mean of SUVmeans recorded from 18 patients according to imaging time.
Ki-67 and CD31 Staining
Staining was performed using the ChemMate EnVision method (Dako) with an auto-staining system (Dako Autostainer) in accordance with the protocol provided by the manufacturer. Formalin-fixed and paraffin-embedded sections (3 μm) of resected specimens from lung cancer were taken for immunohistochemical staining. Antigen was retrieved by heating after immersion of tissue slides into citrate buffer (pH 6.0) in an autoclave at 121°C for 10 min. Mouse monoclonal antibodies specific for Ki-67 (MIB-1; Dako) and CD31 (JC70A; Dako) were used at dilutions of 1:25 and 1:40, respectively. This study also used 3,3′-diaminobenzidine as the final chromogen and hematoxylin as the nuclear counterstain.
Ki-67 index was estimated by counting the percentage of Ki-67–positive cell nuclei per 2,500–10,000 tumor cells in 5 regions with ×200 magnification of the tumor part showing the greatest staining density, in most instances corresponding to the areas of highest mitotic activity.
Microvessel density was assessed using the criteria of Weidner et al. (14). Areas of highest neovascularization were identified as regions of invasive carcinoma with the highest numbers of discrete microvessels stained for CD31. Vessel number was assessed by counting CD31-positive vessels (with a clearly defined lumen or well-defined linear vessel shape but not single endothelial cells) in 5 representative regions with ×200 magnification. Histopathologic slides were examined by a pathologist who was unaware of clinical data and PET findings.
Statistical Analysis
The significance of differences between SUVmax and SUVmean for 11C-4DST and 18F-FDG in the primary lesion was determined using paired t tests. Correlations between 11C-4DST and 18F-FDG uptake and Ki-67 labeling index or number of CD31-stained vessels were assessed using linear regression analysis. Statistical significance was considered to be present for values of P less than 0.05.
RESULTS
Pathologic Findings
Pathologic analysis revealed adenocarcinoma in 15 patients (16 lesions), squamous cell carcinoma in 2 patients, and large cell carcinoma in 1 patient. In 2 patients, the adenocarcinoma was bronchioloalveolar carcinoma. The mean diameter of the lung lesion was 27.2 ± 14.4 mm (range, 12.0–62.0 mm). Lymph node metastases were histopathologically diagnosed in 5 patients (Table 1).
Patient Characteristics
Whole-Body Imaging
Maximum-intensity-projection images and axial images of 11C-4DST PET are shown in Figures 1 and 2, respectively. High physiologic 11C-4DST uptake was observed in the salivary glands, liver, spleen, kidneys, bladder, and bone marrow. In contrast, the brain, lungs, myocardium, muscle, and blood pool showed low physiologic 11C-4DST uptake.

Maximum-intensity-projection images of 11C-4DST PET (A) and 18F-FDG PET (B) in patient 1 with lung adenocarcinoma. Compared with physiologic 18F-FDG uptake, physiologic 11C-4DST uptake is high in salivary glands, liver, and bone marrow and low in brain, kidney, and muscle. Focal uptake in lung tumor in right lower lobe is confirmed on 11C-4DST PET and 18F-FDG PET images (arrow). 11C-4DST uptake in tumor lesion is lower than 18F-FDG uptake.

Axial images of CT (A), 11C-4DST PET (B), and 18F-FDG PET (C) in patient 1 with lung adenocarcinoma in right lower lobe (arrow). Radioactivity of 11C-4DST in ascending aorta (representing blood pool) was lower than that of 18F-FDG. Both 11C-4DST and 18F-FDG clearly accumulate in lung lesions, and 11C-4DST uptake (SUVmax, 4.7) is lower than 18F-FDG uptake (SUVmax, 10.9). On Ki-67 immunohistochemistry (D), Ki-67–positive nuclei (colored brown) show estimated proliferation rate of 81%.
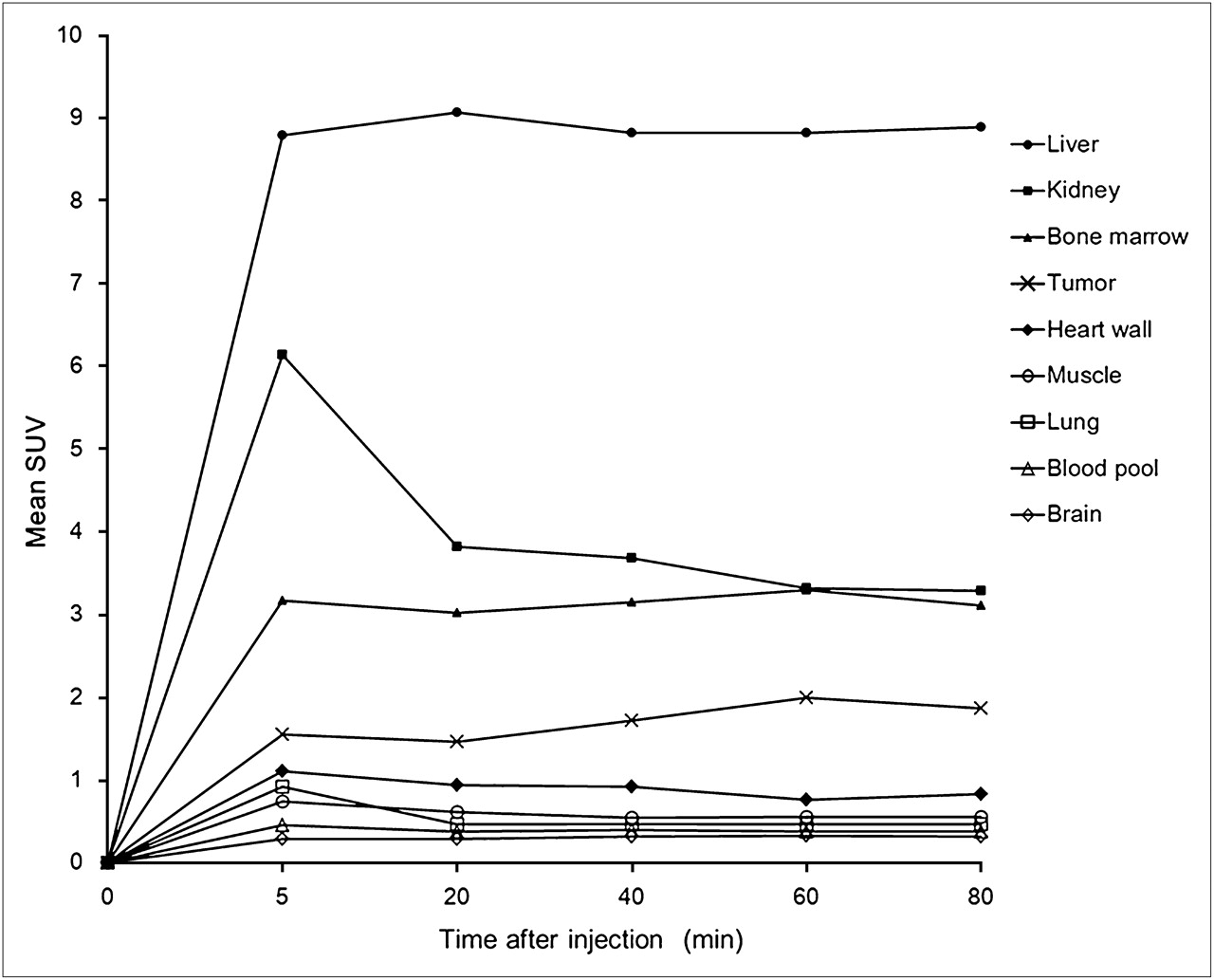
Figure 3 illustrates the decay-corrected time–activity curves of 11C-4DST in patients with lung cancer. Radioactivity in the blood pool was low by 5 min after injection, and levels in myocardium, lung, and muscle decreased slightly over time. Radioactivity was excreted from the kidneys and was considered to peak less than 5 min after 11C-4DST injection. In the liver and bone marrow, radioactivity remained high from 5 min onward after 11C-4DST injection. Uptake of 11C-4DST in the tumor was relatively high from 5 min onward after 11C-4DST injection and increased slightly over time.

Decay-corrected time–activity curves of 11C-4DST for major organs, measured as SUVmean.
Comparison of 11C-4DST and 18F-FDG Uptake in Lung Lesions
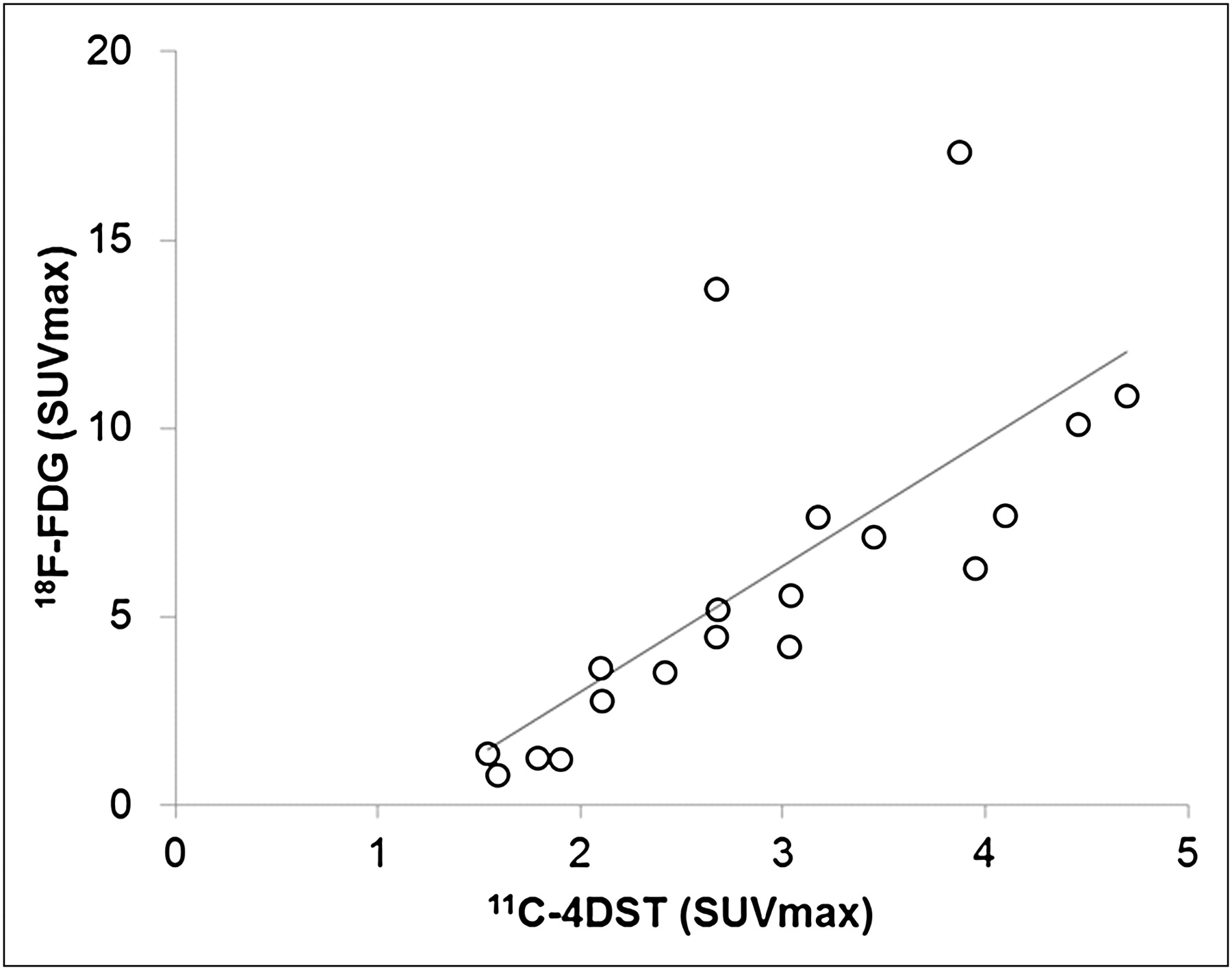
All malignant lesions showed focal increases in uptake of 11C-4DST and 18F-FDG (Table 1). The mean SUVmax and SUVmean of 11C-4DST for lung lesions were 2.9 ± 1.0 (range, 1.5–4.7) and 1.7 ± 0.4 (range, 1.0–2.5), respectively. The mean SUVmax and SUVmean of 18F-FDG for lung lesions were 6.2 ± 4.5 (range, 0.9–17.3) and 2.6 ± 1.4 (range, 0.6–5.8), respectively. Uptake by lung tumors was significantly higher for 18F-FDG than for 11C-4DST (P < 0.001). Linear regression analysis of 11C-4DST and 18F-FDG yielded a correlation coefficient of 0.73 (P < 0.001) for SUVmax (Fig. 4) and 0.79 (P < 0.001) for SUVmean.
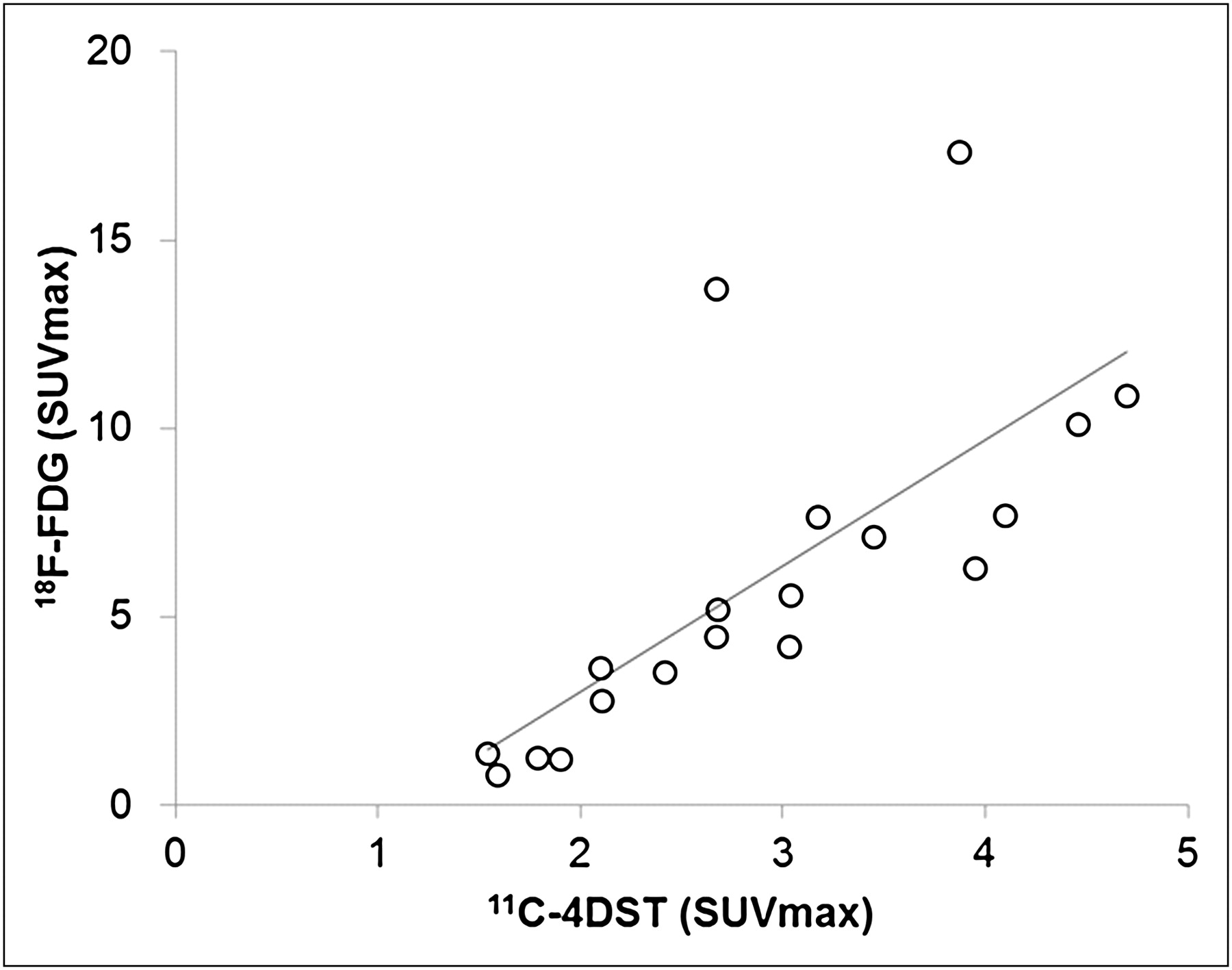
Linear regression analysis showing significant correlation of SUVmax (r = 0.73, P < 0.001) between 11C-4DST uptake and 18F-FDG uptake in lung lesion.
Ki-67 and CD31 Immunohistochemistry
Ki-67 immunohistochemical staining was assessed in all 19 lesion specimens obtained by surgical resection. The mean interval between 11C-4DST PET/CT and surgery was 15 ± 27 d (range, 1–110 d). All NSCLC specimens contained Ki-67–positive cells. The mean proliferation fraction was 50.9% ± 29.1% (range, 4%–92%) (Table 1). Linear regression analysis identified a significant correlation between the SUVmax of 11C-4DST and Ki-67 index (r = 0.82; P < 0.001; Fig. 5A). A significant correlation was also observed between the SUVmax of 18F-FDG uptake and Ki-67 index (r = 0.71; P < 0.001; Fig. 5B), but this correlation was lower than that for 11C-4DST.

Linear regression analysis showing significant correlation between SUVmax of 11C-4DST and proliferative activity (Ki-67 index) (A) (r = 0.82; P < 0.001). Significant correlation is also observed between SUVmax for 18F-FDG uptake and Ki-67 index (B) (r = 0.71; P < 0.001).
CD31 immunohistochemical staining was assessed in all 19 lesion specimens obtained by surgical resection. All NSCLC specimens contained CD31-positive vessels (Table 1). Linear regression analysis indicated no significant correlation between SUVmax for 11C-4DST and microvessel density as determined by CD31 staining (r = 0.21; P < 0.001). Likewise, no significant correlation was observed between CD31-microvessel density and SUVmax for 18F-FDG (r = 0.21; P < 0.001), which was equal to that for 11C-4DST.
DISCUSSION
In the present study, 11C-4DST (r = 0.82) showed a higher correlation with cell proliferation as evaluated by Ki-67 index in NSCLC than did 18F-FDG (r = 0.71), confirming 11C-4DST PET/CT as a useful noninvasive modality for imaging DNA synthesis by NSCLC.
Proliferation rate is a known prognostic marker for the survival of patients with NSCLC (15). PET proliferation imaging should thus have an impact on oncology as a noninvasive clinical approach, and the present study demonstrated the high potential of 11C-4DST. The structure of 11C-4DST has the 4′-oxo of thymidine replaced by 4′-sulfur, so as to closely resemble the structure of thymidine (16). An in vitro study proved that 3H-4DST is incorporated into DNA (17), and 14C-4DST was confirmed to show metabolism similar to that of thymidine, maintaining stability in the blood (9,10). In a human study, Toyohara et al. used Patlak graphical analysis to obtain the 11C-4DST flux constant (Ki), and Ki values of 11C-4DST correlated well with standardized uptake value (11). These data support the idea that 4DST would be incorporated into DNA in the human body. However, DNA incorporation of 4DST does not entirely mean that 4DST can quantify the DNA synthesis ratio. 4DST uptake reflects multiple steps: sustained delivery and transport of the tracer, metabolic trapping as a phosphorylated form, or DNA synthesis. The rate-limiting step for tissue retention of 4DST should thus be determined to clarify the trapping mechanisms of 4DST.
In a human study, 11C-4DST was metabolized to hydrophilic metabolites, and at least 5 radioactive metabolites were detected. In urine, 2 hydrophilic metabolites were dominant, and one of these was also commonly detected in plasma (11).
Serum thymidine may compete with nucleoside tracers for the active site of nucleoside carriers in cell membranes and for the active site of the trapping enzyme, thymidine kinase 1. Currently, we have no detailed information on the affinities or subtype selectivities of 4DST toward nucleoside transporters and thymidine kinase. Despite a high serum thymidine concentration, previous rodent studies of 11C-4DST have been performed with no phosphorylase pretreatment (9,10). Therefore, in contrast to 18F-FLT, competition of endogenous thymidine for 11C-4DST uptake appears negligible.
Although the detailed mechanisms underlying 11C-4DST uptake are not well understood in humans, the biodistribution of 11C-4DST was nearly identical to that of 18F-FLT, which is linked to the S-phase–specific enzyme thymidine kinase, suggesting that 11C-4DST PET may reflect cell proliferation via this kinase (18,19). In addition, low 11C-4DST uptake in myocardium indicated a low affinity for TK2, a mitochondrial isozyme unrelated to cellular proliferation.
Uptake of 11C-4DST by NSCLC was about 50% lower than that of 18F-FDG, as seems similar to the relationship between 18F-FLT and 18F-FDG. We were able to measure 11C-4DST uptake for tumor lesions because we placed regions of interest on solitary lung lesions based on CT results; therefore, negative findings for the lesion were not obtained for our study cases. Given the small number of cases showing lymph node metastasis in this study, evaluating the potential of 11C-4DST for diagnosing lymph node metastasis is difficult. A relatively low accumulation of 11C-4DST could lead to failure to detect some lesions, representing a crucial problem as seen for 18F-FLT. As a result, 11C-4DST PET may be best positioned for prediction of patient prognosis rather than detection or staging of cancers. We performed 18F-FDG examinations after the completion of 11C-4DST examinations for most of the patients included in this study. This protocol could provide information within half a day regarding staging of lung cancer by 18F-FDG and proliferation in the primary lesion by 4DST labeled with 11C, which shows a relatively short half-life.
The correlation coefficient for 18F-FDG uptake and proliferative activity (Ki-67) in pulmonary nodules has been reported to be in the range of 0.59–0.73 (20–22). Our result (r = 0.71) supports this finding. Yamamoto et al. revealed a high correlation coefficient (r = 0.81) between 18F-FDG uptake and proliferative activity, compared with an estimated 0.63 among patients with adenocarcinoma, which was the most common tumor in our study (23). The correlation coefficient for 18F-FLT uptake and proliferative activity in pulmonary nodules was within the range of 0.77–0.87 (8). However, this coefficient was calculated from lesions that included inflammatory lesions. The correlation coefficient for 18F-FLT uptake (SUVmax) and proliferative activity in any NSCLC was estimated to be within the range of 0.59–0.83. Our study showed 11C-4DST to have a higher correlation coefficient (r = 0.82) than 18F-FDG (r = 0.71) for uptake and proliferative activity in NSCLC. However, further study with larger numbers of patients is needed to evaluate the reliability of 11C-4DST as a proliferation imaging tracer.
Regarding angiogenesis, no significant correlation between 18F-FDG uptake and CD31-microvessel density has been reported (24), again supported by the present results. The correlation coefficient between 11C-4DST uptake and CD31-microvessel density was low, with no difference from that between 18F-FDG uptake and CD31-microvessel density. According to the regional time–activity curve, 11C-4DST uptake for lung lesions increased slightly over time, even though radioactivity in the ascending aorta (representing the blood pool) remained low over the course of 80 min from injection. These results might indicate that 11C-4DST uptake for tumor lesions did not depend on blood flow, with steady uptake by the tumor and incorporation into DNA in relation to cell proliferation. Toyohara et al. used Patlak graphical analysis to obtain the 11C-4DST Ki, and Ki values of 11C-4DST correlated well with standardized uptake value (11). Our study showed a higher correlation coefficient between 11C-4DST uptake and Ki-67% index. As a result, 11C-4DST was expected to work as a marker of DNA synthesis.
One limitation of this study was that we could not obtain dynamic 11C-4DST scan data, because of the nonintegrated dynamic scan mode in the PET/CT scanner. We failed to obtain a specific regional time–activity curve and 11C-4DST flux estimate from Patlak plot analysis; however, the 11C-4DST biodistribution tendency was same as the study data in patients with brain tumor described by Toyohara et al. (11). Another limitation was the relatively long period between 11C-4DST scanning and surgery, compared with other studies, and 2 patients showed exceptionally long intervals of 37 and 110 d, attributed to events largely unrelated to this study. However, SUVmax and SUVmean in these 2 patients were plotted near the correlation line obtained from linear regression analysis.
We set a duration of more than 90 min between 11C-4DST and 18F-FDG studies, when the 2 scans were obtained on the same day (13 patients). The effect of remnant radioactivity from the 11C-4DST scan on 18F-FDG uptake in patients undergoing 2 sessions of PET within a single day can be considered negligible. For a study with 11C-methionine and 18F-FDG, a 90-min interval has been considered to avoid contamination by sites of high 11C-methionine accumulation, such as the liver (unpublished data). Because high-accumulation sites tended to be similar for 11C-4DST and 11C-methionine, we applied the same interval to the studies with 11C-4DST and 18F-FDG.
We set a common scan time of 40 min after 11C-4DST injection. According to the regional time–activity curve, the radioactivity level in tumors increased slightly over time, whereas that in the blood pool was stable from 5 min after injection. The scanning time at 20 min after 11C-4DST was the same as that at 40 and 60 min, but a relatively high deviation in 11C-4DST biodistribution was confirmed in our study and in a study on a patient with a brain tumor (11). Tumor-to-blood ratio was thus highest at 60 min after 11C-4DST injection, representing the best time for tumor imaging. However, scan images obtained within 40 min after injection yielded almost the same tumor-to-blood ratio. To reduce the injected radiation dose, 40 min rather than 60 min appears to represent the best scan time for evaluation of lung tumor.
Respiratory artifacts can be observed on CT images and induce errors in attenuation-corrected PET images (25), including standardized uptake value (26). To minimize this effect, PET and CT acquisitions were performed during shallow breathing (27). All lung nodules in this study were over 1 cm in diameter and not close to the diaphragm. Our study results could avoid artifacts.
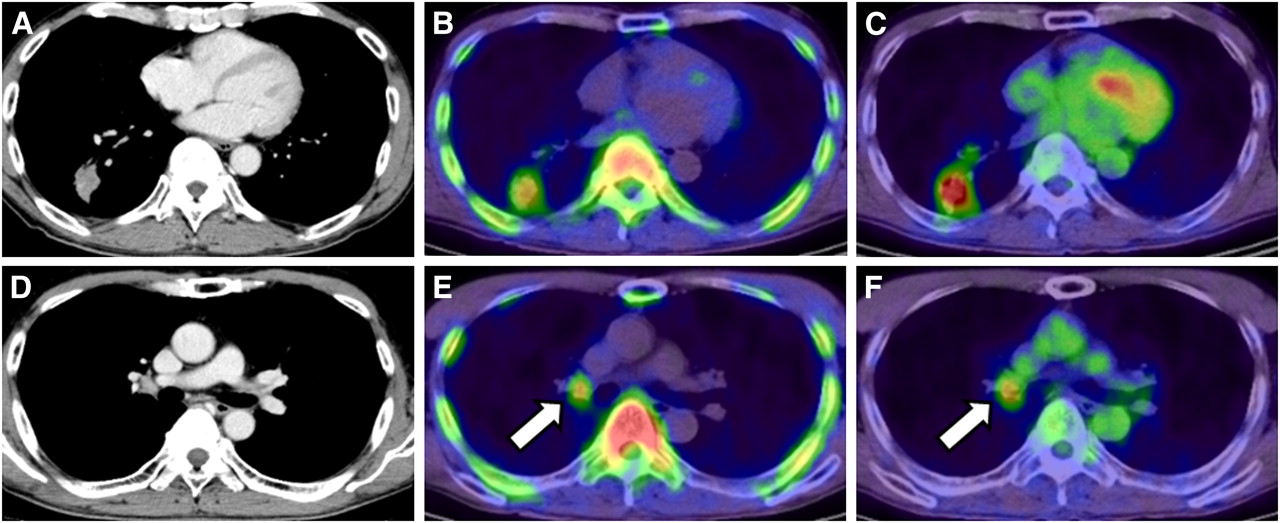
11C-4DST also accumulated at lymph node metastases (Fig. 6.), but evaluation of lymph nodes requires further investigation because of the small number of patients with lymph node metastases (n = 5).
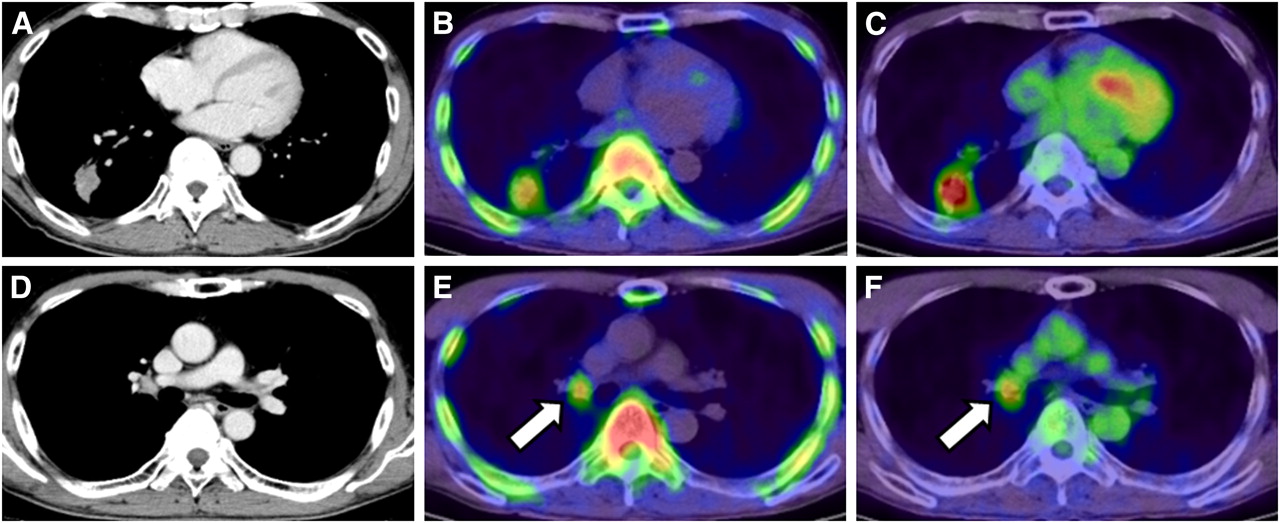
Axial images of CT (A), 11C-4DST PET (B), and 18F-FDG PET (C) in patient 9 with lung adenocarcinoma in right lower lobe. Right hilar lymph node metastasis is confirmed on CT (D), and uptake on both 11C-4DST PET (E) and 18F-FDG PET (F) identifies lesion (arrow). However, 11C-4DST image is clearer than 18F-FDG image because of low physiologic 11C-4DST in mediastinum as blood pool.
The potential of 11C-4DST PET for distinguishing between inflammation and malignancy could not be evaluated in this study.
The most crucial application for cell proliferation is monitoring antiproliferative therapy, and Toyohara et al. showed a case in which 11C-4DST PET had potential for monitoring cancer treatment response (11). Further clinical studies are needed to address these issues.
CONCLUSION
Proliferation of lung tumors correlated better with 11C-4DST uptake than with 18F-FDG uptake, supporting 11C-4DST PET/CT as a noninvasive modality for imaging DNA synthesis in NSCLC.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Takashi Sato, Toshiaki Fujita, Shingo Kawaguchi, and Yoshiaki Taguchi for technical support. This work was supported by grant 21 A-26 from the National Center for Global Health and Medicine and grant-in-aid 22390241 for scientific research (B) from the Japan Society for the Promotion of Science. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 21, 2011.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication July 11, 2011.
- Accepted for publication October 4, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}