


Abstract
For the past decade, PET with 18F-fluoro-ethyl-tyrosine (18F-FET) has been used in the evaluation of patients with primary brain tumors (PBTs), but so far series have reported only a limited number of patients. The purpose of this systematic review and metaanalysis was to assess the diagnostic performance of 18F-FET PET in patients with suspicion of PBT. Methods: We examined studies published in the literature using MEDLINE and EMBASE databases. Inclusion criteria were use of 18F-FET PET for initial assessment of patients with a newly diagnosed brain lesion; patients who had no radiotherapy, surgery, or chemotherapy before 18F-FET PET; and use of histology as a gold standard. Metaanalysis was performed on a per-patient basis. We secondarily performed receiver-operating-characteristic analysis of pooled patients to determine tumor-to-background ratio (TBR) of 18F-FET uptake and best diagnostic value. Results: Thirteen studies totaling 462 patients were included. For the diagnosis of PBT, 18F-FET PET demonstrated a pooled sensitivity of 0.82 (95% confidence interval [CI], 0.74–0.88), specificity of 0.76 (95% CI, 0.44–0.92), area under the curve of 0.84 (95% CI, 0.80–0.87), positive likelihood ratio of 3.4 (95% CI, 1.2–9.5), and negative likelihood ratio of 0.24 (95% CI, 0.14–0.39). Receiver-operating-characteristic analysis indicated that a mean TBR threshold of at least 1.6 and a maximum TBR of at least 2.1 had the best diagnostic value for differentiating PBTs from nontumoral lesions. Conclusion: 18F-FET PET demonstrated excellent performance for diagnosing PBTs. Strict standardization of PET acquisition protocols and prospective, multicenter studies investigating the added value over current MRI are now needed to establish 18F-FET PET as a highly relevant tool for patient management.
Although primary brain tumors represent only 1%–2% of adult cancers, the Central Brain Tumor Registry of the United States estimated that almost 230,000 new patients with primary brain tumor or central nervous system tumor were diagnosed between 2004 and 2007 (1). A newly diagnosed mass with ring-enhancement on MRI may be of tumoral origin (tumor, glioma, or metastasis) or nontumoral origin (abscess, parasite, demyelination, infarct, or old hematoma). Gliomas constitute the most frequent brain tumors, and their histologic differentiation and grading is predictive of aggressiveness and outcome (2). Although grade I and II tumors are considered low-grade, with a protracted natural history, the frequent grade III (anaplastic astrocytoma) and grade IV (glioblastoma) are often referred to as malignant glioma and lead to death within weeks to months without treatment. Even with treatment, median survival rates are in the range of 15–18 mo for glioblastoma and 2–3 y for anaplastic astrocytoma.
Although morphologic assessment by MRI is precise, it lacks specificity and does not allow for easy determination of tumor activity and metabolism. MR spectroscopy allows the presence of neuronal and membrane metabolites to be assessed but without sufficient anatomic discrimination. Molecular imaging with PET allows information on tumor metabolism to be gained, identifying zones of highest activity and determining the extension of increased growth activity (3). PET with 18F-FDG is unreliable at predicting the tumoral nature of a lesion, because of unspecific uptake in inflammation and in relatively benign tumors and high normal brain uptake.
18F-fluoro-ethyl-tyrosine (18F-FET) is an artificial amino acid taken up into upregulated tumoral cells but not incorporated into proteins (contrary to natural amino acids such as 11C-methionine) (4,5). 18F-FET allows good-contrast images to be obtained in both high- and low-grade tumors (6). However, the 18F-FET uptake is not reliably linked to tumor grading, and dynamic analysis over time helps in differentiating low- from high-grade tumors (7). Among other applications, 18F-FET PET has shown value in the diagnosis of brain tumor recurrence after initial surgery or radiotherapy and for directing biopsy or radiosurgery (8). Because 18F-FET has lower uptake by inflammatory cells than 11C-methionine or 18F-FDG, it is useful in the differentiation of tumor from treatment-induced necrosis (9). Early changes in 18F-FET uptake have been suggested as a surrogate to predict tumor response to treatment and prognosis (10). However, only a few studies with limited patient populations have been published for evaluating 18F-FET PET in newly identified brain lesions.
The purpose of this report was to systematically review studies in the literature, to assess the diagnostic performance of 18F-FET PET in patients for whom primary brain tumors and glioma are suspected, and to assess the performance of 18F-FET uptake quantification.
MATERIALS AND METHODS
Data Sources and Search
We performed a systematic search in the medical databases PUBMED and EMBASE for English and non-English publications from January 1977 to January 2011 using the following search: “(“O-(2-fluoroethyl)tyrosine” [all fields] OR “(18F)fluoroethyltyrosine” [all fields] OR “Tyrosine/diagnostic use” [Mesh]) AND (“Brain Neoplasms/radionuclide imaging” [Mesh] OR “Glioma” [all fields]) AND (“Humans” [Mesh])”. Errata, reviews, and preclinical, animal, and nonradiopharmaceutical studies were excluded.
Study Selection
We considered studies using 18F-FET PET for the initial assessment of newly diagnosed brain tumor in humans. Inclusion criteria were 18F-FET PET used as an initial diagnostic tool in patients with newly diagnosed brain lesion; patients who had no radiotherapy, surgery, or chemotherapy before the 18F-FET PET study; and use of histology as the gold standard to assess diagnostic performance. Studies in abstract form, case reports, and papers written in a language other than English, French, or German were excluded. Studies including fewer than 10 patients with newly diagnosed brain lesions were not retained.
Data Extraction and Quality Assessment
Data were extracted from the publications for the following information: first author, year of publication, study population (number of patients who underwent 18F-FET for the initial assessment of brain tumor and surgery or biopsy for histologic diagnosis, sex, age, and histology), 18F-FET results (tumoral or nontumoral maximal target-to-background ratio [TBR] or mean TBR, when available), and time between injection and image acquisition. Data were recorded at the patient level, when possible. Study quality and applicability were assessed using both checklists of the Quality Assessment of Diagnostic Accuracy Studies (QUADAS, scale 0–14) and Standards for Reporting Studies of Diagnostic Accuracy (STARD, scale 0–25) (11,12).
Statistical Analysis
All analyses were performed at the patient level. Dichotomized histologic diagnosis (tumor or not, glioma or not) according to the classification of tumors of the central nervous system of the World Health Organization (WHO) (2) and the third edition of the International Classification of Diseases for Oncology (ICD-O-3) was used as the gold standard. Gliomas were defined by ICD-O-3 codes 9380-9384, 9391-9460, and 9480. Each study had its own criteria for defining 18F-FET PET positivity. For data synthesis, we applied the bivariate mixed-effects regression model. Average sensitivity, specificity, likelihood ratio (LR), and odds ratio and the respective 95% confidence intervals were calculated from the maximum likelihood estimates and graphically assessed by summarized receiver-operating-characteristic curves. Heterogeneity of the results between the studies was assessed graphically on Forest plots and statistically using the χ2 test and Cochran Q. The I2 statistic, which describes the percentage of total variation across studies attributable to heterogeneity rather than chance, was used to statistically quantify inconsistency of the results between the studies. Publication bias was assessed by the Funnel plot asymmetry test (13). By convention, in the figures and the text we have used the small letter n when describing the number of studies and the capital letter N when describing the number of patients.
Secondary analyses were performed at the patient level, using dichotomized histology diagnosis (tumor or not, glioma or not) as the gold standard and mean TBR (mean activity of the lesion divided by mean activity of the contralateral brain) or maximum TBR (maximum activity of the lesion divided by mean activity of the contralateral brain) as the dependent parameter to determine the best diagnostic threshold for both measures. For computing TBR, authors used a region of interest manually drawn around the tumor based on MRI T1- or T2-weighted images (14–16) or increased 18F-FET uptake (7,17,18), an automated region-of-interest drawing based on areas with increased 18F-FET uptake above 3 SDs of the mean standardized uptake value of the control region (19), or a fixed 25-mm2 elliptic region of interest centered on the area of greatest 18F-FET uptake (20,21). In 3 studies, the method for region-of-interest definition was not specified (22–24). To determine mean TBR and maximum TBR thresholds providing the best diagnostic performance, we performed receiver-operating-characteristic analysis on pooled patients. ANOVA was also applied to assess the difference between mean TBR and maximum TBR according to glioma WHO grade. Statistics were performed with Stata 11.1 (StataCorp), and a P value less than 0.05 was considered statistically significant.
RESULTS
Study Characteristics
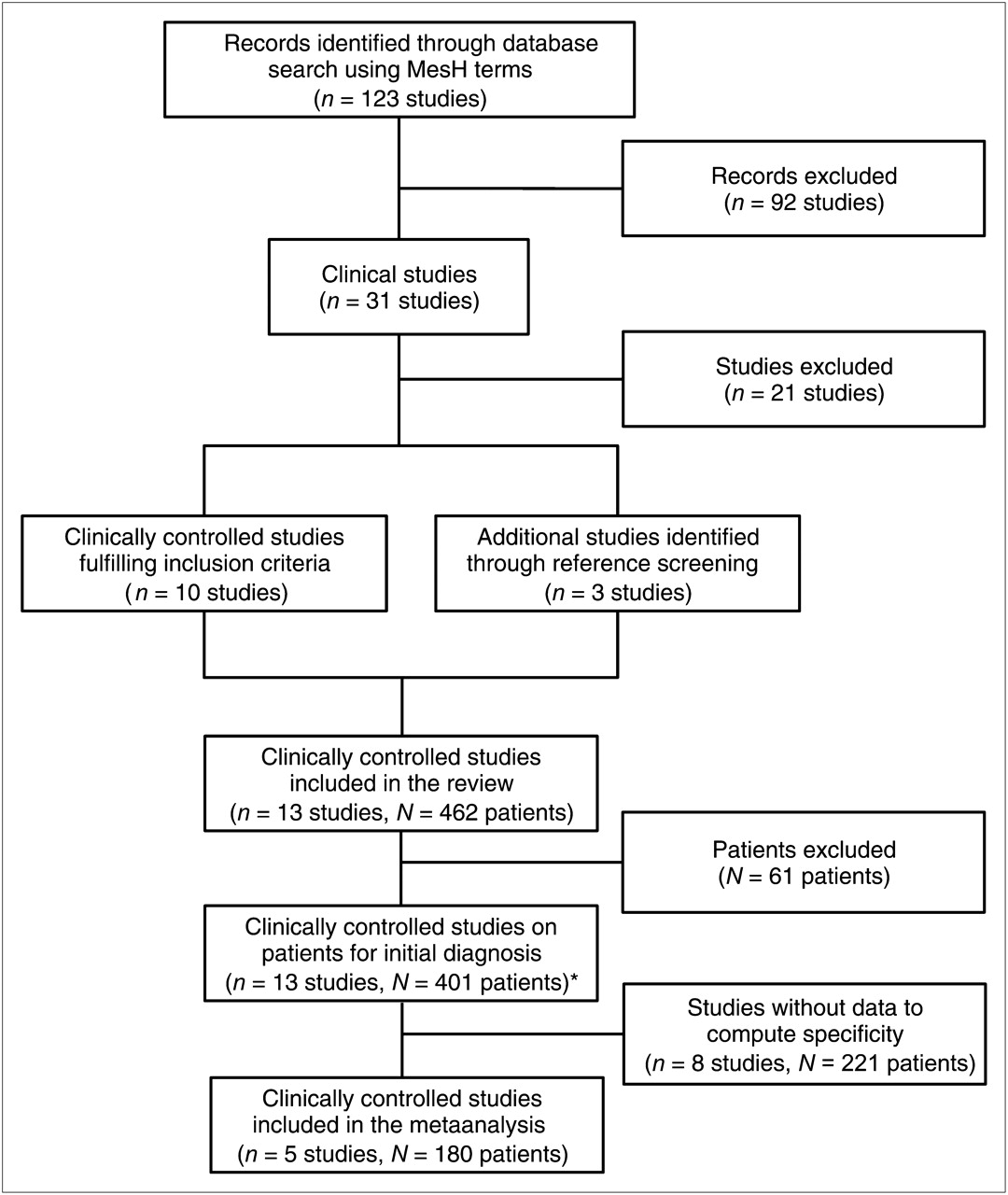
In total, 123 papers were identified in PUBMED and EMBASE databases. After the exclusion of non–18F-FET reports (n [studies] = 75), errata (n = 1), reviews (n = 9), and preclinical (n = 6) and animal studies (n = 1), 31 articles about the clinical use of 18F-FET PET in patients were found (Fig. 1). After applying the inclusion criteria, 10 studies remained, excluding reports on recurrent disease (n = 13), studies not reporting 18F-FET results (n = 3), reports on fewer than 10 primary brain lesions (n = 3), and studies on nontumoral brain lesions (n = 2). Three more studies were found through reference screening of the excluded papers (Fig. 1).
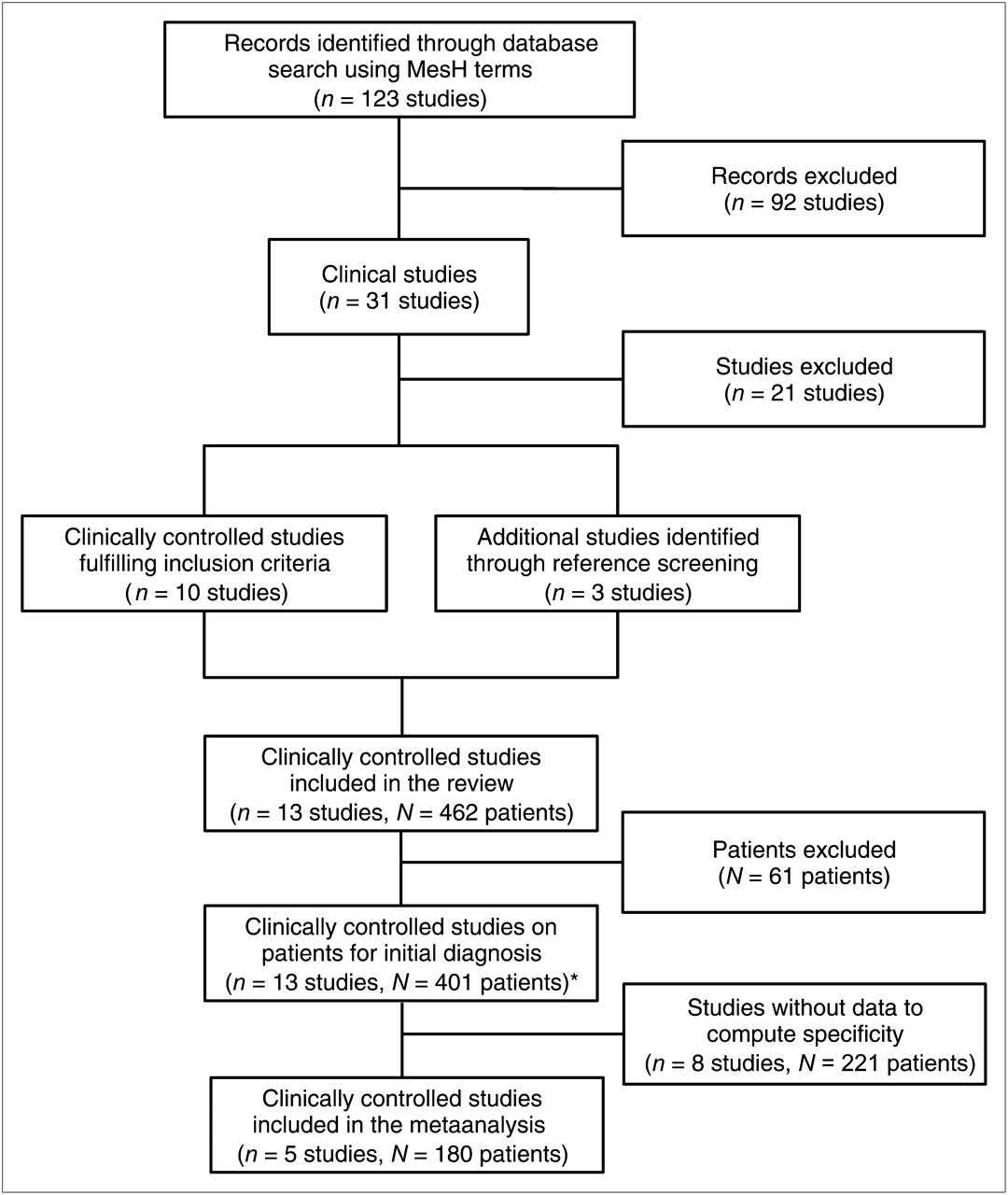
Flowchart of study selection. *Among these, subpopulation of 12 studies representing 390 patients reported TBR data, which were used for deriving TBR thresholds yielding best diagnostic performance.
Thus, 13 studies (7,14–25) totaling 462 patients (Table 1) remained. Some studies reported results in mixed populations including primary and recurrent disease (studies 1, 9, 11, 12, and 13, Table 1) or did not report histology results for all the patients (study 2, Table 1). From these studies only patients with 18F-FET PET for primary assessment of the lesion and a subsequent biopsy or resection were included. Patients who underwent surgery or biopsy or any therapy before 18F-FET PET, as well as patients who underwent 18F-FET PET for recurrent tumor, were excluded. Thus, 401 patients were finally retained (median age, 45 y; mean age ± SD, 45 ± 11 y; sex ratio, 0.7:1 M:F). Of these patients, 356 (89%) had a tumor, of which 338 (84%) were gliomas. Eighteen patients had nonglioma brain tumor: lymphoma (N [patient] = 5), metastasis (N = 4), hemangioblastoma (N = 3), cavernoma (N = 1), germinoma (N = 1), teratoma (N = 1), medulloblastoma (N = 1), pinealoblastoma (N = 1), and primitive neuroectodermique tumor (N = 1). Nonmalignant lesions were due to gliosis (N = 17), infectious disease (N = 11), infarct (N = 4), hemorrhage (N = 4), demyelination (N = 4), encephalitis (N = 2), aneurysm (N = 1), adenoma (N = 1), and cortical dysplasia (N = 1).
Study Characteristics
Performance for Diagnosis of Brain Tumor and Glioma
The study selection process is summarized in the flowchart described in Figure 1. From the 13 selected studies, 5 studies with a total of 180 patients were used in the bivariate mixed-effects regression model. The other 8 studies could not be included for this analysis because they did not report true-negative and false-positive cases to compute specificity nor did they use dichotomized 18F-FET PET results.
After the pooling of datasets, the summarized receiver-operating-characteristic curve for the diagnosis of brain tumor versus nontumor brain lesion is presented in Figure 2. 18F-FET PET demonstrated an overall sensitivity of 0.82 (95% confidence interval [CI], 0.74–0.88), specificity of 0.76 (95% CI, 0.44–0.92), positive LR of 3.4 (95% CI, 1.2–9.5), negative LR of 0.24 (95% CI, 0.14–0.39), diagnostic odds ratio of 14 (95% CI, 3–60), and area under the curve (AUC) of 0.84 (95% CI, 0.80–0.87).
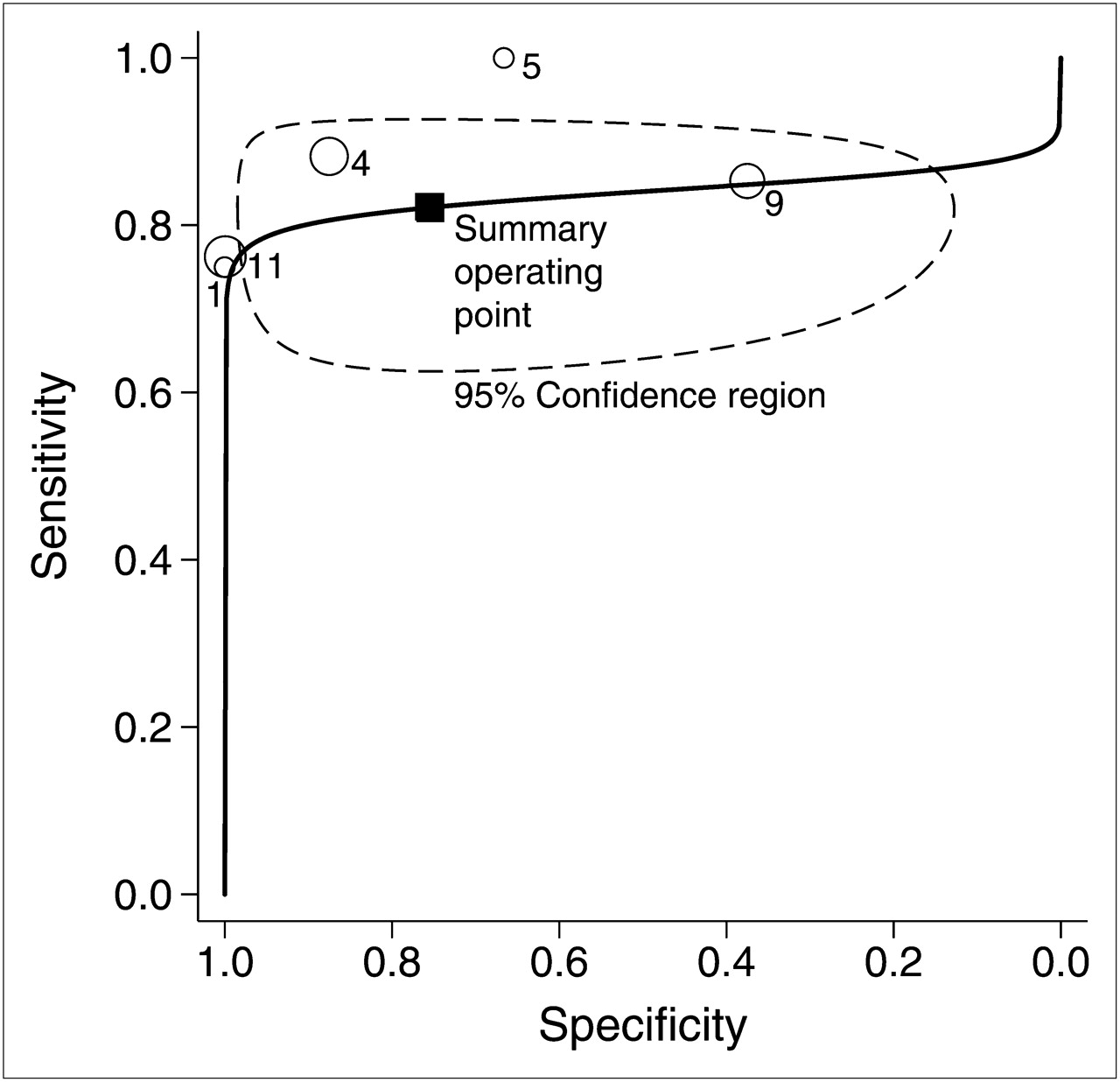
Summarized receiver-operating-characteristic curve for diagnosis of brain tumor vs. nontumoral brain lesion.
For the diagnosis of brain glioma versus nonglioma brain lesion, 18F-FET PET demonstrated a sensitivity of 0.84 (95% CI, 0.74–0.90), specificity of 0.62 (95% CI, 0.31–0.86), positive LR of 2.2 (95% CI, 0.9–5.2), negative LR of 0.26 (95% CI, 0.11–0.58), diagnostic odds ratio of 9 (95% CI, 2–43), and AUC of 0.85 (95% CI, 0.81–0.88).
Assessment of Heterogeneity, Inconsistency, and Quality of Studies
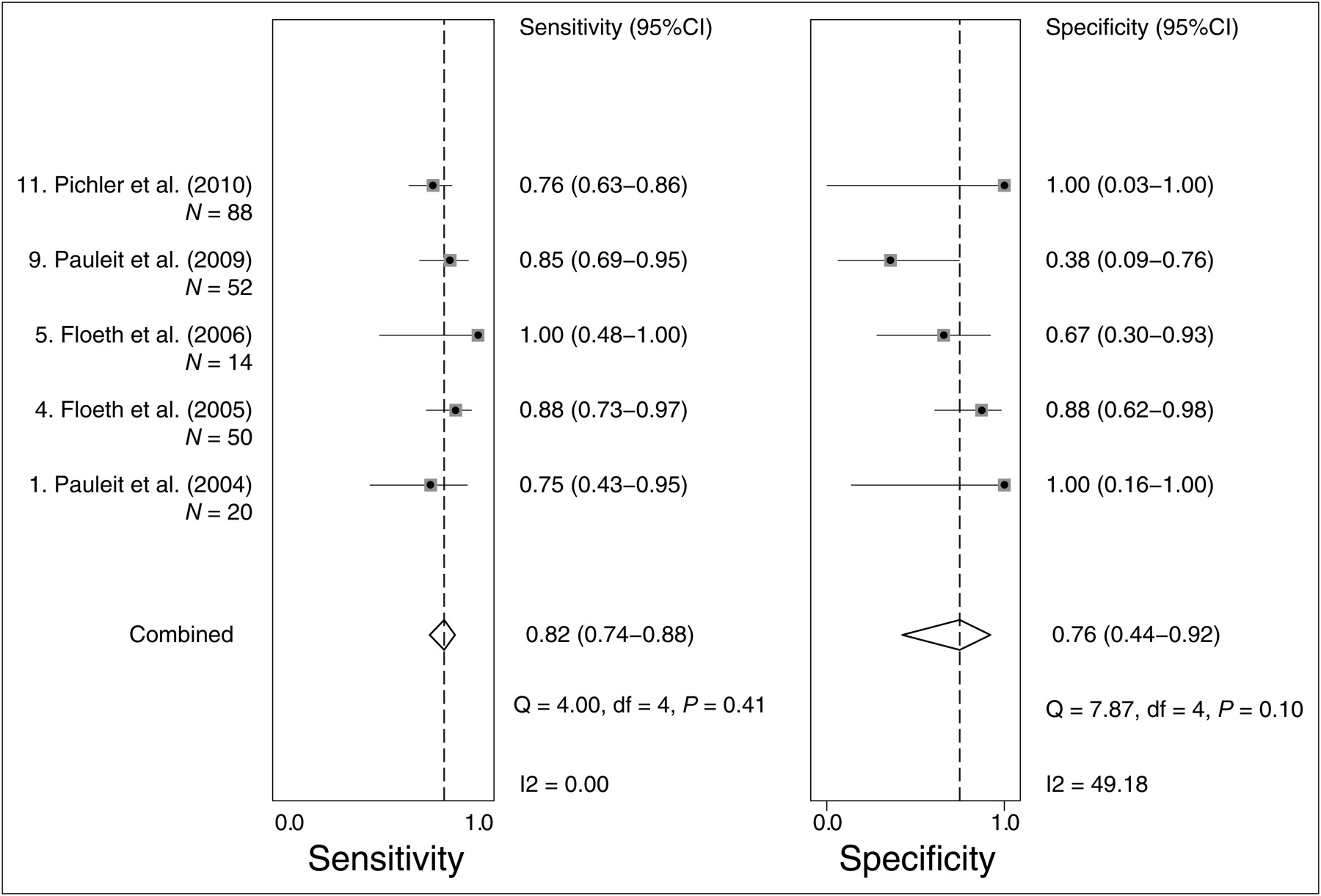
A Forest plot for the diagnosis of brain tumor versus nontumor brain lesion (Fig. 3) did not show any significant performance heterogeneity (Cochran Q = 1.1, P = 0.28) or inconsistency between studies for the diagnosis of brain tumor and (I2 = 0% attributable to heterogeneity rather than chance).
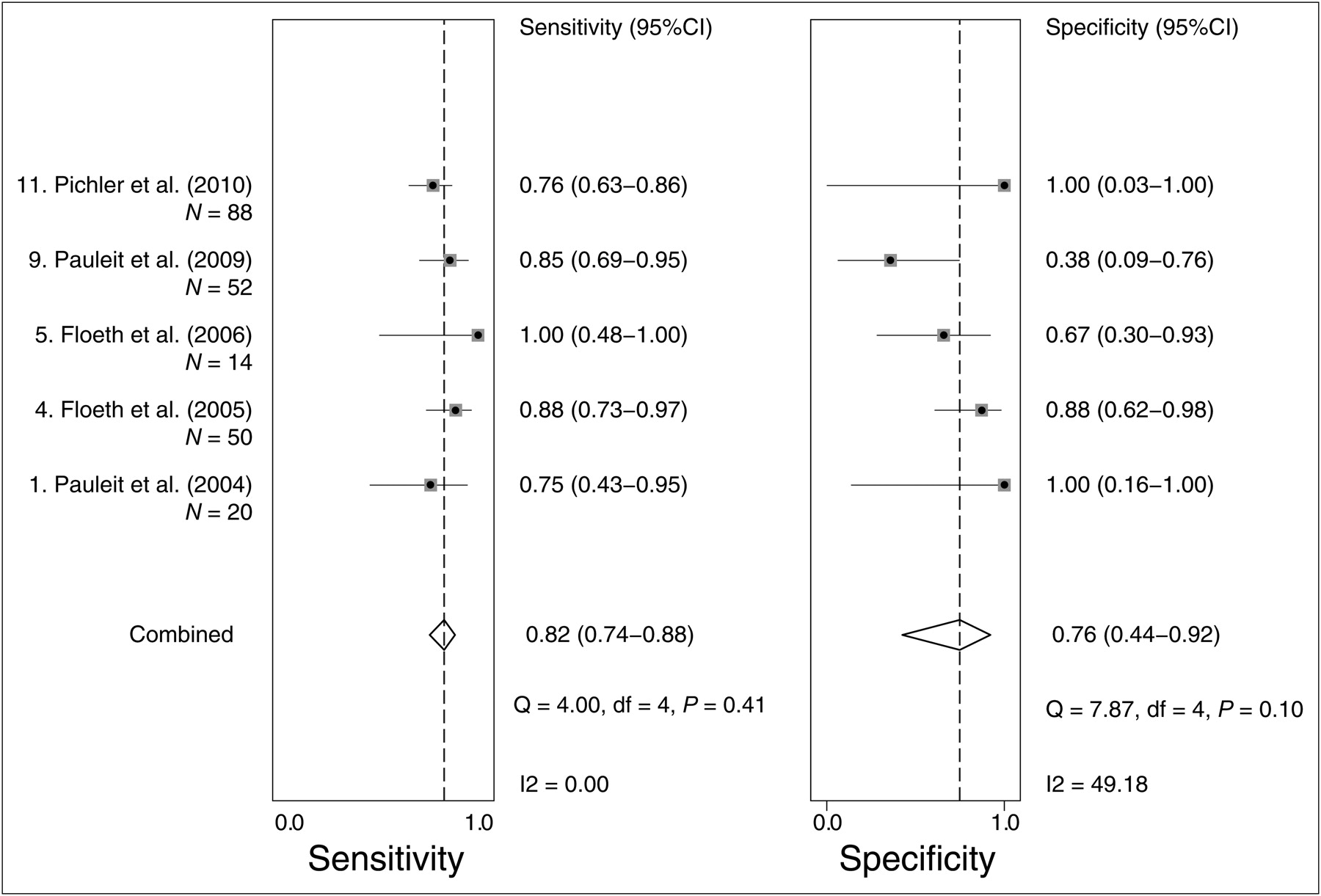
Forest plot for brain tumor diagnosis of studies included in metaanalysis.
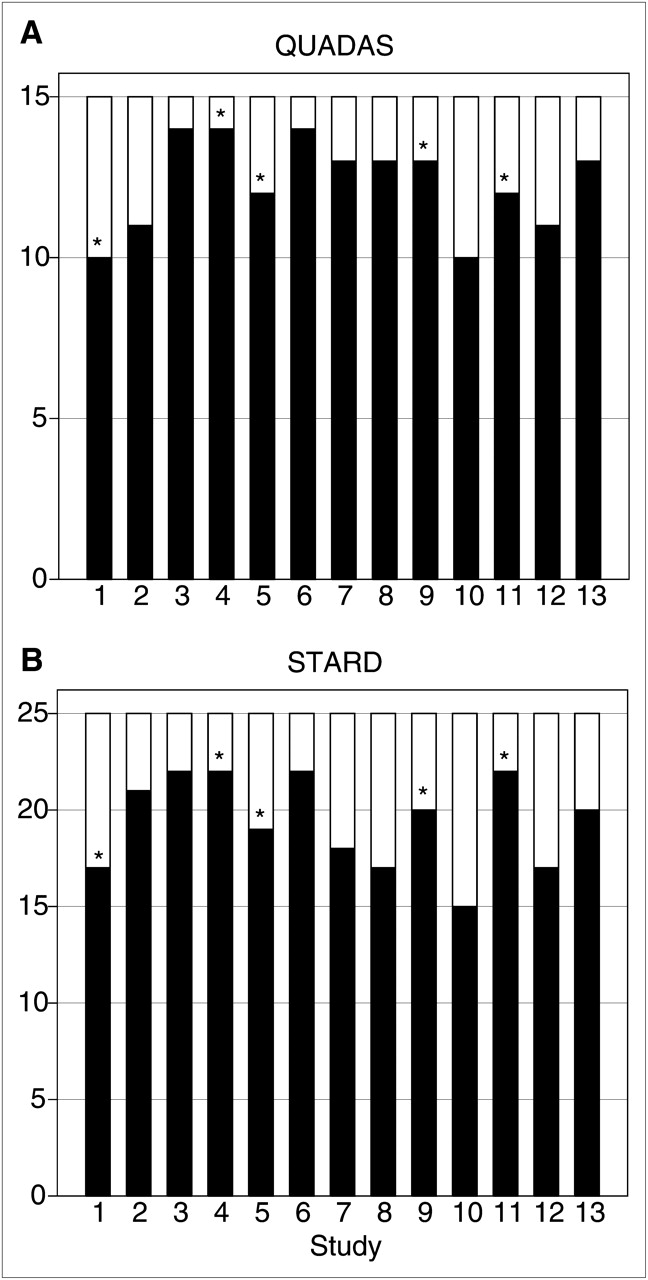
For the diagnosis of glioma, analysis demonstrated no significant performance heterogeneity (Cochran Q = 3.5, P = 0.09) or inconsistency (I2 = 42%), although specificity significantly changed between studies (Cochran Q = 15.3, P < 0.01). Funnel plots (not shown) did not demonstrate any publication bias for brain tumor (P = 0.5) or for glioma diagnosis (P = 0.99). The assessment of study quality by QUADAS and STARD criteria is graphically summarized in Figure 4.
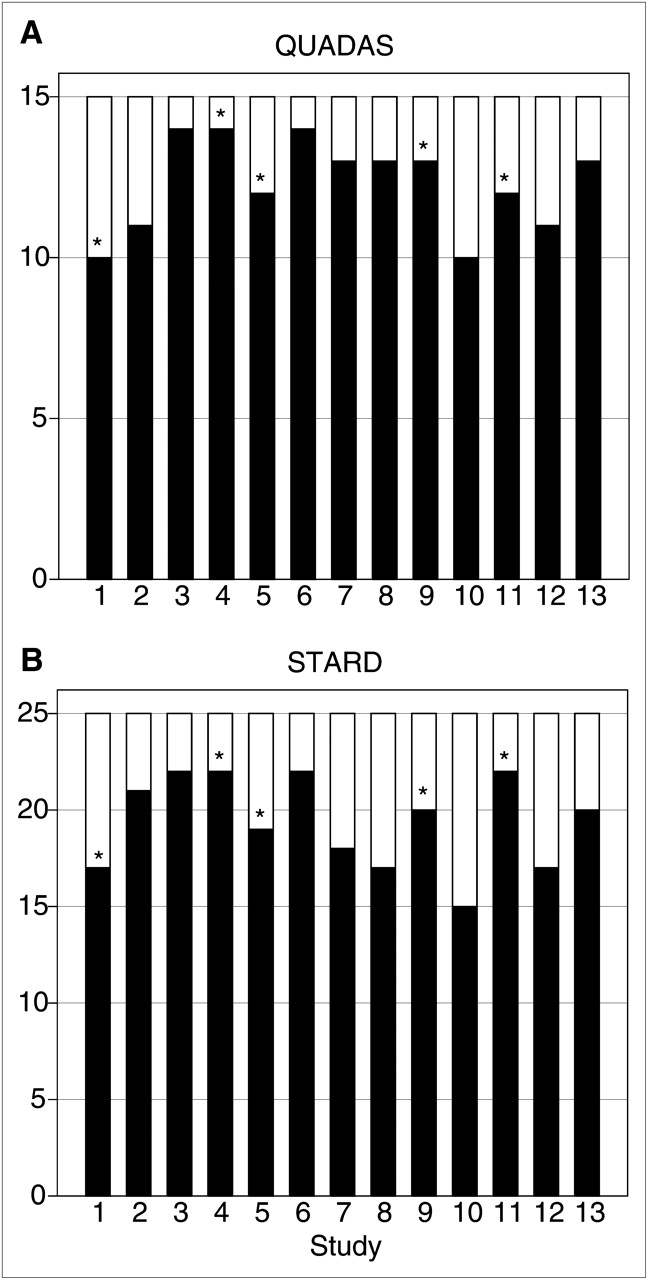
Study quality grading using QUADAS scores (range, 0–14) (A) and STARD scores (range, 0–25) (B). *Included in metaanalysis.
Quantitative Threshold for Diagnosing Brain Tumor and Glioma
From the 13 studies selected, 9 indicated the mean TBR (N = 271) (14–18,20–22,24) and 5 the maximum TBR (N = 183) (7,15,16,19,23). Receiver-operating-characteristic curve analysis showed that a mean TBR of at least 1.6 and maximum TBR of at least 2.1 had the best value for the diagnosis of brain tumor, reaching a sensitivity, specificity, and accuracy of 0.77 (95% CI, 0.71–0.82), 0.81 (95% CI, 0.64–0.92), and 0.77 (95% CI, 0.72–0.86), respectively, for mean TBR and 0.65 (95% CI, 0.56–0.71), 0.73 (95% CI, 0.39–0.94), and 0.66 (95% CI, 0.54–0.83), respectively, for maximum TBR. For the diagnosis of brain glioma, a mean TBR of at least 1.7 and maximum TBR of at least 2.1 had the best diagnostic performances, with a sensitivity, specificity, and accuracy of 0.71 (95% CI, 0.65–0.77), 0.72 (95% CI, 0.57–0.84), and 0.71 (95% CI, 0.65–0.79), respectively, for mean TBR and 0.65 (95% CI, 0.56–0.71), 0.56 (95% CI, 0.31–0.79), and 0.64 (95% CI, 0.47–0.72), respectively, for maximum TBR.
Interestingly, mean TBR and maximum TBR were significantly higher in high-grade gliomas than in low-grade gliomas (1.7 ± 0.7 vs. 2.6 ± 1.0, P < 0.001, and 2.2 ± 0.9 vs. 3.1 ± 1.1, P < 0.001, respectively). This difference is illustrated in Figure 5, showing the mean TBR and maximum TBR in function with the tumor histology classified in nontumoral, grade I–II and grade III–IV gliomas.

TBR comparison according to histologic WHO grading. Solid bars = mean TBR; open bars = maximum TBR. *P < 0.001 vs. nontumoral lesions or WHO grade I–II; †P = 0.055 vs. nontumoral lesions.
DISCUSSION
This systematic review and metaanalysis shows that 18F-FET PET has excellent performance for the diagnosis of brain tumor and glioma in the initial evaluation of newly diagnosed brain lesions. In this population, we found that 18F-FET has good sensitivity (82% and 84%) and average specificity (76% and 62%), respectively, for the diagnosis of brain tumor and glioma. Regarding clinical utility, the high positive LR and low negative LR suggest that 18F-FET PET is excellent at confirming and excluding brain tumor or glioma.
18F-FET has been known to distinguish between proliferative tumor and nontumoral lesion (5,9). Initial comparison studies demonstrated that 18F-FET uptake ratios correlated with 11C-methionine uptake (6) but with a lesser uptake by inflammatory cells (26–28), allowing a better discrimination between infectious and tumoral lesions (29) or between tumor recurrence and radionecrosis (9). After early studies in recurrent tumor, several studies assessed 18F-FET PET performance in the initial evaluation of isolated brain tumor (30). Among the 13 studies included in this systematic review, only 5 reported enough details to compute sensitivity and specificity, highlighting the need of better methodology, larger multicenter studies, and standardized reporting of 18F-FET PET. In a large study (n = 176) by Möller-Hartmann et al. (31), MRI had a diagnostic accuracy of 55%, increasing to 71% when 1H-MR spectroscopy was added, which is lower than the AUC of 84% (80%–87%) reported in our study. Hence, the ability of 18F-FET PET to assess the tumoral nature of isolated brain lesions seems superior to that of MRI alone. This is in line with results from Pauleit et al. (20), reporting that PET/MRI fusion to guide diagnostic biopsy increased specificity from 53% for MRI alone to 94%. Similarly, Floeth et al. (22) reported that the combination of MRI with 18F-FET PET and MR spectroscopy yielded a diagnostic accuracy of 97%.
Regarding the ability to distinguish between tumor subgroups, mean TBR and maximum TBR indices have emerged as measures, allowing inter- and intrapatient comparisons, because the normal brain background is quite variable on consecutive PET examinations even in the same patient. Our analysis pinpointed thresholds (mean TBR ≥ 1.6 and maximum TBR ≥ 2.1 for brain tumor) that are consistent with the studies by Pauleit et al. (mean TBR ≥ 1.6 for tumoral tissue) (20) and Pöpperl et al. (maximum TBR > 2.0 for recurrence) (30). For glioma, low-grade tumors had significantly lower mean TBR (1.7 ± 0.7 vs. 2.6 ± 1.0, P < 0.001) and maximum TBR (2.2 ± 0.9 vs. 3.1 ± 1.1, P < 0.001) than high-grade tumors. Using dynamic acquisitions, Pöpperl et al. (7) previously reported accurate distinction between low- and high-grade untreated gliomas, with 94% sensitivity, 100% specificity, and 0.97 AUC. It has not been established whether the eventual combination of MRI eventually with fractional anisotropy and diffusion tensor imaging, MR spectroscopy, and dynamic 18F-FET PET could provide better performance (32,33), but it is currently being investigated using the latest hybrid PET/MRI scanners (34).
Of increased interest is the initial assessment of brain lesions by 18F-FET PET and MRI to guide radiotherapy. For instance, Weber et al. (35) compared 18F-FET–based biologic tumor volume for radiotherapy planning in high-grade glioma with conventional MRI–based gross tumor volume. They found that biologic tumor volume and gross tumor volume differed in size and localization in two thirds of the patients. Similar differences were confirmed in a recent study by Niyazi et al. (36). They found that the addition of 18F-FET PET resulted in larger target volumes on 3D conformal radiotherapy planning than with MRI alone (416.5 vs. 343.5 cm3, P < 0.001). Using composite target volumes, Weber et al. (37) demonstrated that 90% of tumor recurrences occurred within the 95% isodose line, suggesting that radiotherapy planning with 18F-FET PET and MRI may reduce noncentral tumor control failure. Although the impact on survival of 18F-FET PET and MRI combination for radiotherapy adaptation remains to be verified, its value for response assessment is established: Piroth et al. (10) showed that 18F-FET PET is sensitive at distinguishing between responders and nonresponders in patients with glioblastoma early after radiochemotherapy. The value of 18F-FET PET is also established for noninvasively distinguishing between radionecrosis and tumor recurrence (9,30). Interestingly, 18F-FET PET-based response to therapy can predict failure of antiangiogenic therapy and was used to monitor glioblastoma response to paclitaxel (38). Thus, mounting evidence suggests that pretreatment baseline 18F-FET PET in patients with brain tumors is of importance for guiding tumor diagnosis and biopsy and is effective for radiotherapy planning and for assessment of tumor response to radiotherapy or chemotherapy.
Despite a small number of studies, most of these were of good quality (QUADAS scores > 10 and STARD scores > 18), using the WHO classification as the histologic gold standard. Furthermore, the absence of publication bias (tendency to report more studies with positive results) and inconsistency between studies strengthens the validity of our results. However, limitations are worth mentioning. First, only 5 studies were included in the metaanalysis, mainly because of the absence of true-negative cases. Second, the determination of an optimal common TBR threshold from our metaanalysis must be taken with caution. Indeed, differences in uptake kinetics between low- and high-grade tumors, the use of late summed images (e.g., adding early, 10–20 min after injection, to late, >30 min after injection, frames) (7,19), and different methodologies to define regions of interest will certainly influence the optimal threshold.
On the basis of our metaanalysis, we would recommend future investigations to apply strict standardization of PET acquisition protocols for better 18F-FET PET intercenter reproducibility and multicenter data analysis, as recommended by recent European Association of Nuclear Medicine and German brain PET guidelines with amino acid analogs (39,40). The inclusion of more true-negative cases would help in better determining the specificity. Importantly, the cost-effectiveness of 18F-FET PET in the management of patients with brain tumors will need to be investigated in the clinical setting.
CONCLUSION
This systematic review and metaanalysis provide evidence that 18F-FET PET has good diagnostic performance for the initial assessment of patients with new, isolated brain lesions. Strict standardization of PET protocols and large, prospective, multicenter studies investigating the added value over current MRI are now in need and could help in establishing 18F-FET PET as a highly relevant tool for patient management, from the planning of biopsy or radiation therapy, to the assessment of new therapies, or even to the avoidance of unnecessary treatments and their associated costs.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication August 11, 2011.
- Accepted for publication September 28, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [18F]-fluoroethyl-L-tyrosine (FET) in glioblastoma (FIG) TROG 18.06 study: protocol for a prospective, multicentre PET/CT trial
- Amino Acid PET in Neurooncology
- Amino Acid PET in Neurooncology
- Does Blood-Brain Barrier Disruption Define the Glioma Extracellular Metabolome?
- PET/MRI in Pediatric Neuroimaging: Primer for Clinical Practice
- Comparison of 11C-Methionine and 18F-FDG PET/CT for Staging and Follow-up of Pediatric Lymphoma
- TSPO Imaging in Glioblastoma Multiforme: A Direct Comparison Between 123I-CLINDE SPECT, 18F-FET PET, and Gadolinium-Enhanced MR Imaging
- The Usefulness of Dynamic O-(2-18F-Fluoroethyl)-L-Tyrosine PET in the Clinical Evaluation of Brain Tumors in Children and Adolescents
- Prediction of Glioma Recurrence Using Dynamic 18F-Fluoroethyltyrosine PET
- Comparison of the Amino Acid Tracers 18F-FET and 18F-DOPA in High-Grade Glioma Patients
- Pituitary Incidentaloma Found on O-(2-18F-Fluoroethyl)-L-Tyrosine PET
- Clinical Impact of Amino Acid PET in Gliomas
- A Meta-Analysis on the Diagnostic Performance of 18F-FDG and 11C-Methionine PET for Differentiating Brain Tumors
- Reply: Discriminating Ability of 18F-FET PET for Several Cerebral Neoplastic Lesions
- Radiolabeled Amino Acids for Oncologic Imaging
- Diagnostic Performance of 18F-FET PET in Newly Diagnosed Cerebral Lesions Suggestive of Glioma