


Abstract
3′-deoxy-3′-18F-fluorothymidine (18F-FLT) is a radiopharmaceutical depicting tumor cell proliferation with PET. In malignancies of the lung, breast, head and neck, digestive tract, brain, and other organs, quantitative assessment of 18F-FLT targeting has been shown to correlate with the proliferation marker Ki-67 and with clinical outcome measures such as time to progression and overall survival (OS). The aim of this study was to assess various PET segmentation methods to estimate the proliferative volume (PV) and their prognostic value for OS in patients with suspected high-grade glioma. Methods: Twenty-six consecutive patients underwent preoperative 18F-FLT PET/CT and T1-weighted MRI of the brain after contrast application. The maximum standardized uptake value (SUVmax) of all tumors was calculated, and 3 different segmentation methods for estimating the PV were used: the 50% isocontour of the SUVmax signal for the PV50%, the signal-to-background ratio (SBR) for an adaptive threshold delineation (PVSBR) method, and the iterative background-subtracted relative threshold level (RTL) method to estimate the PVRTL. The prognostic value of the SUVmax and the different PVs for OS were assessed. Results: Twenty-two patients had glioblastoma multiforme, 2 had anaplastic oligodendroglioma, 1 had anaplastic ependymoma, and 1 had anaplastic astrocytoma. The median OS was 397 d (95% confidence interval, 204–577); 19 patients died during the follow-up period. The PVSBR showed a significantly (P = 0.002) better association with OS than did SUVmax, PVRTL, and PV50%. Receiver-operating-characteristic analysis resulted in a threshold volume for the PVSBR of 11.4 cm3, with a sensitivity and specificity of 70% and 83%, respectively, for the prediction of OS. Kaplan–Meier analyses showed a significant discrimination between short and long OS (P = 0.024, log rank) for this threshold. Conclusion: The PV as determined by 18F-FLT PET is associated with OS in high-grade malignant gliomas. The SBR method yielded the best results to predict short and long OS.
Gliomas are relatively uncommon neoplasms. Most gliomas (especially astrocytic, oligodendroglial, and mixed oligoastrocytic tumors) are diffuse tumors, characterized by extensive, diffuse infiltrative growth in the surrounding brain parenchyma. Ependymal tumors are generally more circumscribed. Glioblastoma, the most malignant diffuse astrocytic tumor, is also by far the most frequent glioma. Despite treatment, most patients with a glioblastoma die within 2 y after diagnosis (median survival, 14.6 mo; 2-y survival, 26.5% (1)). Standard treatment consists of maximal surgical resection, external-beam radiotherapy (EBRT) to the tumor or resection cavity as characterized by contrast enhancement on MRI, and concurrent and adjuvant chemotherapy in patients younger than 60 y (1). The extent of resection together with the age and Karnofsky performance status are important features determining overall survival (OS) (2–6). However, the diagnostic work-up of primary glioma still leaves room for improvement. In diffuse infiltrating glioma, contrast enhancement on MRI is not always present and not fully representative of the most malignant parts of the tumor (7). Therefore, more advanced imaging techniques are being explored to better guide surgery and radiotherapy.
18F-FDG is the most commonly used radiopharmaceutical for PET of a wide variety of malignancies. However, for brain tumors the specificity of 18F-FDG is low because of the high uptake in the normal brain cortex. The PET tracer 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) specifically reflects cellular proliferation, lacks any significant uptake in the normal brain, and may thus be more suitable for molecular imaging of gliomas (8). Intracellular uptake of 18F-FLT is facilitated both by active transport through sodium-dependent nucleoside transporters and by passive diffusion (9). In the cell, 18F-FLT is monophosphorylated by the cytosolic enzyme thymidine kinase 1 and subsequently trapped intracellularly without being incorporated into the DNA (10). Because thymidine kinase 1 is upregulated in the S-phase of the cell cycle, 18F-FLT uptake represents the proliferation rate of the tissue. Chen et al. showed that 18F-FLT PET is more sensitive than 18F-FDG PET at detecting recurrent high-grade tumors. The maximum standardized uptake value (SUVmax) of 18F-FLT correlated better with the proliferation marker Ki-67 and proved to be a more powerful predictor of tumor progression and survival (11). Other investigators confirmed the correlation of 18F-FLT with Ki-67 (12–14). However, the relevance of the proliferative volume (PV) of brain tumors as determined with 18F-FLT has not been studied as a prognostic indicator in glioma patients.
In this study, we evaluated the potential of 18F-FLT PET to predict outcome in patients with brain tumors. Because 18F-FLT accumulation is dependent on disruption of the blood–brain barrier (15), only patients with suspected high-grade glioma were included in this study. 18F-FLT uptake in the tumors was determined quantitatively, and the PV of brain tumors was estimated using different methods for image segmentation.
MATERIALS AND METHODS
Patients
From July 2007 to August 2008, patients in whom intracranial high-grade glioma was suspected on the basis of a preoperative MRI and in whom surgery was indicated were considered eligible for this prospective study. Exclusion criteria were age younger than 18 y, a Karnofsky score below 70, pregnancy, or breast-feeding. Patients were followed until July 2011.
The study was approved by the Institutional Review Board of the Radboud University Nijmegen Medical Centre. Written informed consent was obtained from all patients.
Imaging Protocol
Preoperative T1-weighted MR images (3-dimensional rapid gradient echo; resolution, 1 × 1 × 1 mm; repetition time, 2,300 ms; inversion time, 1,100 ms; echo time, 4.71 ms) were obtained on a 3-T whole-body MRI system (TIM TRIO; Siemens), before and after contrast administration (0.1 mmol/kg bolus, 0.5 mM gadoteric acid [Dotarem; Guerbet]). The contrast-enhanced tumor volume (T1-ce) was manually delineated using the Pinnacle3 radiotherapy treatment planning system (Philips) by subtracting the precontrast hyperintense volume of the tumor from the contrast-enhanced volume.
Patients underwent a preoperative 18F-FLT PET/CT scan at most 3 d before surgery, with the exception of 2 patients (5 and 11 d). 18F-FLT was obtained from the Department of Nuclear Medicine and PET Research, VU Medical Centre, Amsterdam, The Netherlands. Synthesis was performed as described previously (16,17). 18F-FLT PET and CT images were acquired on a hybrid PET/CT scanner (Biograph; Siemens). Emission images of the head were recorded 60 min after intravenous injection of 18F-FLT, with a median activity of 221 MBq (range, 108–277 MBq), for 10 min in 3-dimensional mode and reconstructed using the ordered-subset implementations iterative algorithm (4 iterations, 16 subsets, and 5-mm 3-dimensional gaussian filter). In addition, low-dose CT images (40 mAs, 130 kV) were acquired for anatomic correlation and attenuation-correction purposes. PET, CT, and MRI scans were coregistered and fused with software developed in-house.
The SUVmax of all tumors was derived from the coregistered 18F-FLT PET/CT on the Pinnacle3 radiotherapy planning system. The SUVmax was defined as the mean SUV of the hottest voxel of the tumor and its 8 surrounding voxels in a transversal slice (0.01 cm3). Three different segmentation methods for estimating the PV were applied using Pinnacle3 scripts developed in-house. The 50% isocontour of the SUVmax was used as a fixed lower threshold for calculating the proliferative volume PV50%. The signal-to-background ratio (SBR) as an adaptive threshold delineation method for calculating the proliferative volume PVSBR has been described in detail by Schinagl et al. (18) and Daisne et al. (19). In brief, the threshold was derived from the following formula: threshold = a + b × 1/SBR, in which the parameters a and b are scanner-specific variables determined by a phantom experiment (18,19). The iterative background-subtracted relative threshold level (RTL) method was described in detail by van Dalen (20). In brief, to get a first volume estimate, the RTL of 50% was initially used. This volume was converted to an average diameter via D = (V × 6/π)1/3. The appropriate RTL for this diameter was calculated, and this process was iterated until the change of the RTL was less than 1%. The volume calculated with this optimal RTL was used as the proliferative RTL volume PVRTL. For the background activity, a volume of 0.65 cm3 of normal-appearing tissue at the contralateral hemisphere—or in the case of a midline tumor, the contrafrontal or occipital hemisphere—was used.
For determining the variability of the segmentation methods, the mean and SD of the 3 different segmented PVs were calculated for each patient. The SD of the different segmented volumes was plotted against the mean of the different segmented volumes
Statistics
The Cox proportional hazards regression model (univariate Cox regression) with a backward likelihood ratio was used to assess the significance on OS of the covariates sex, age at operation, operation type (biopsy or resection), Karnofsky score at the time of surgery, the preoperative T1-ce volume, the SUVmax, and the different PVs. The significant covariates were used for multivariate regression with backward likelihood ratio. With receiver-operating-characteristic (ROC) curve analysis, we identified the threshold of the various PVs for patients with longer OS. Kaplan–Meier analysis with a log-rank statistical test was used to test the power of 18F-FLT PET for predicting OS. All statistical analyses were performed with SPSS (version 16.0; IBM) for Windows (Microsoft).
RESULTS
Twenty-six patients (mean age, 52 y; age range, 35–67 y; 20 men, 6 women) were included in the study. Detailed patient characteristics are provided in Table 1. Tumor debulking was performed in 17 patients (4 gross total, 13 partial debulking), and in 9 patients the diagnosis was made using biopsy results. Most patients (n = 22) were diagnosed with glioblastoma. In the other patients, the diagnosis was anaplastic oligodendroglioma (ODIII; n = 2), anaplastic ependymoma (EIII; n = 1), and anaplastic astrocytoma (AIII; n = 1). Three patients had prior surgery because of a lower-grade tumor at respective intervals of half a year (diagnosis, grade II astrocytoma), 4 y (diagnosis, AIII), and 6 y (diagnosis, grade II oligodendroglioma) before. Two of these patients received prior EBRT. After the operation, all patients diagnosed with glioblastoma without previous treatment were treated with adjuvant EBRT and temozolomide chemotherapy conforming to the Stupp schedule (1), with the exception of 2 eligible patients (one patient refused adjuvant treatment, and the other had chronic lymphocytic leukemia and therefore received only EBRT). The patients diagnosed with glioblastoma and previously irradiated were treated with adjuvant temozolomide chemotherapy only. Patients with an ODIII were treated with EBRT after surgical resection. The patients with an AIII and EIII were first treated with EBRT and later adjuvant temozolomide chemotherapy. Eight patients underwent a second surgery, and 3 patients (all glioblastoma) received dendritic cell therapy after a second surgery. The median OS was 397 d (95% confidence interval, 204–577; range, 51–1379 d), and 19 patients died during the follow-up period (Table 1).
Patient Characteristics
As shown in Table 2 and exemplified by Figure 1, in 18 patients (69%) the PVSBR was the largest volume, compared with the PVRTL, PV50%, and T1-ce volume (Wilcoxon signed rank test: P < 0.001, P = 0.09, and P = 0.003, respectively). Furthermore, the variability between the various methods for calculating the PV increased with increasing PV (Fig. 2).
SUVmax, PVs, and Enhanced T1 Tumor Volumes for Different Patients

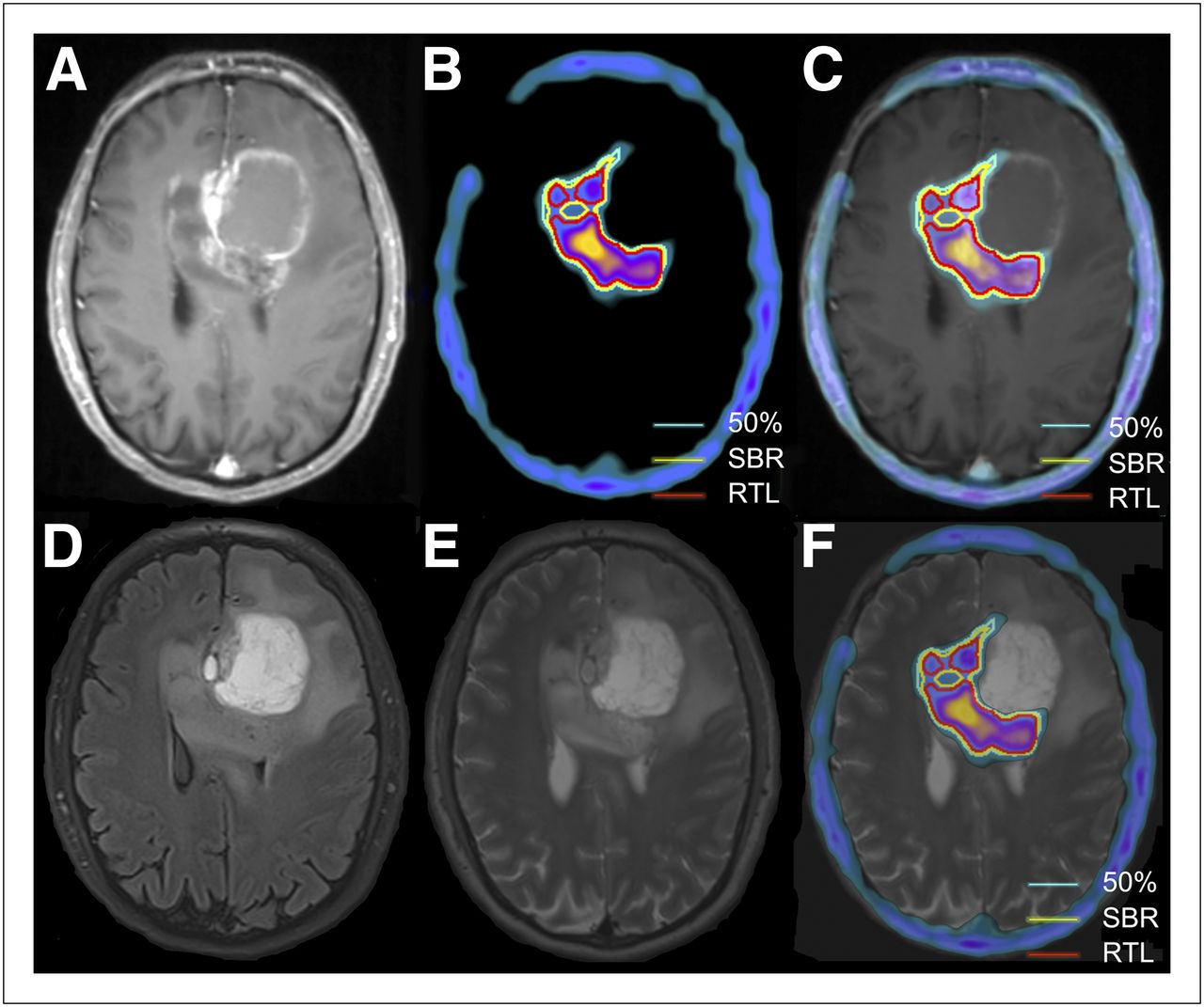
(A) T1-weighted MR image after contrast, showing left frontal ring-enhanced glioblastoma tumor with infiltration via corpus callosum to right side. (B) 18F-FLT PET image with different segmented PVs. (C) Fused 18F-FLT PET and T1-weighted MR image after contrast. (D) Fluid-attenuated inversion recovery MR image. (E) T2-weighted MR image. (F) Fused 18F-FLT PET and T2-weighted MR image, showing most active localization of tumor in infiltrative part. 50% = PV of tumor based on 50% isocontour of SUVmax.
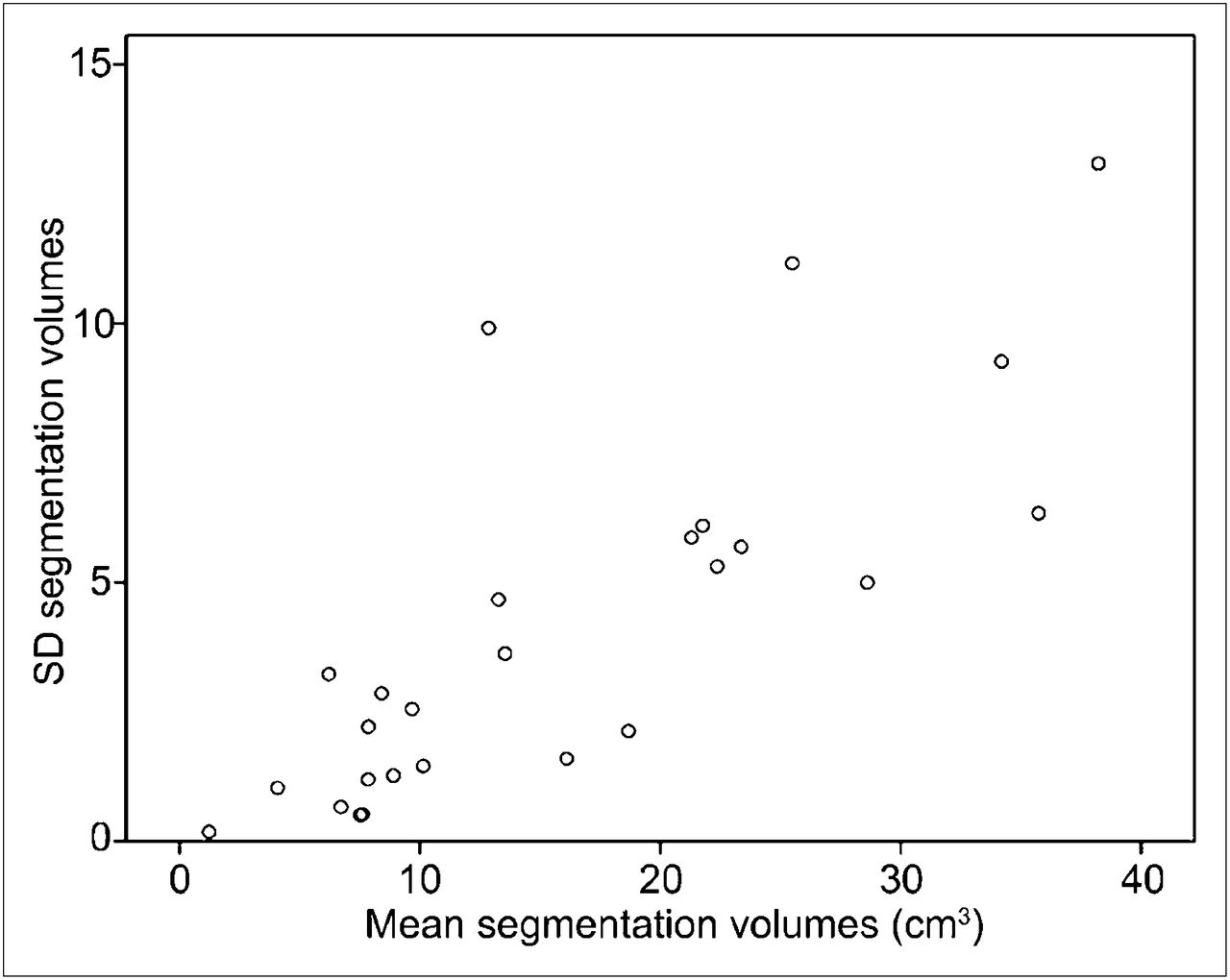
Correlation between tumor volume and variability between different segmented volumes. SDs between different segmented volumes are plotted against means of different segmented volumes, showing increasing SD with increasing volume.
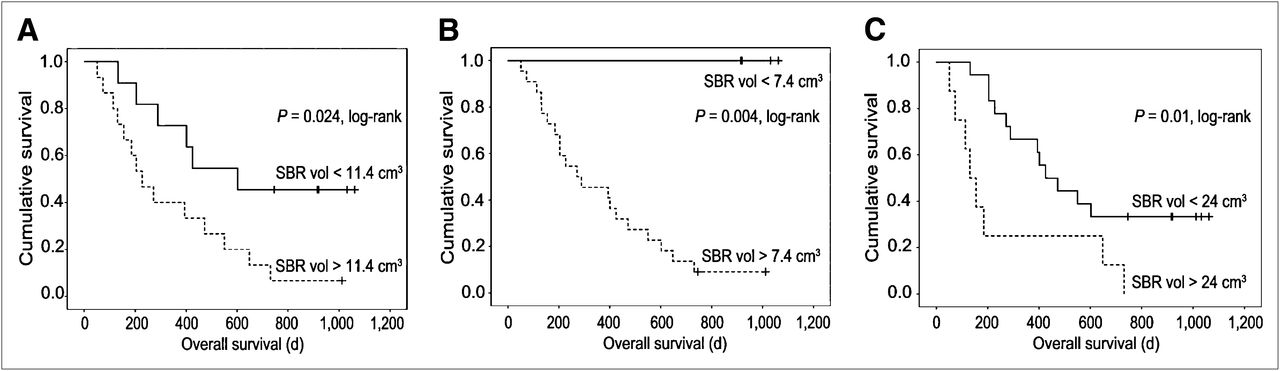
The T1-ce, SUVmax, and PVs were independent significant predictors of survival in a univariate Cox regression model, and multivariate Cox regression showed significance only for the PVSBR (Table 3). ROC analysis resulted in a volume threshold for the PVSBR of 11.4 cm3 (area under the curve, 85%; sensitivity, 70%; specificity, 83%). Kaplan–Meier analyses showed a significant discrimination between short and long survival (P = 0.024; log rank) for this threshold (Fig. 3A). A volume of less than 7.4 cm3 PVSBR was indicative of long-term survival (P = 0.004; log rank; Fig. 3B), and a PVSBR of more than 24 cm3 indicated a poor prognosis with no survivors beyond 2 y (P = 0.01; log rank; Fig. 3C). ROC analysis was not significant for T1-ce, SUVmax, and PV50%. ROC analysis for PVRTL resulted in a volume threshold of 8.9 cm3 (area under the curve, 78%; sensitivity, 70%; specificity, 67%). However, Kaplan–Meier analysis was not significant for this volume threshold.
Cox Regression Results

Kaplan–Meier estimates of OS using PVSBR. (A) PVSBR of 11.4 cm3 significantly differentiates 2 groups of patients, with sensitivity of 70%, specificity of 83%, and area under the curve of 85%. (B) PVSBR of less than 7.4 cm3 indicates relatively long-term survival (>4 y). (C) PVSBR of more than 24 cm3 indicates poor prognosis, with no patient surviving more than 2 y.
DISCUSSION
In this study, we demonstrate that the PV of high-grade glioma calculated from a single pretherapy 18F-FLT PET/CT scan predicts OS of high-grade glioma patients. For this purpose, the PVSBR proved to be the method of choice. The T1-ce, SUVmax, and other PVs were also independent significant predictors of the OS, but PVRTL failed to identify a clear threshold value, and ROC analysis for T1-ce, SUVmax, and PV50% was not significant.
Earlier publications have shown that quantitative analysis of 18F-FLT PET may also discriminate recurrent tumor from posttreatment radionecrosis (21). Furthermore, the potential of sequential 18F-FLT PET has been reported for early outcome predictions of systemic therapy in patients with recurrent malignant glioma (22,23).
For quantitative analysis of PET, mainly the SUV is calculated or more sophisticated kinetic models are used (11,23,24). The mean SUV of the tumor is often calculated after manual delineation of the tumor. The major disadvantages of this approach are the operator dependency and the susceptibility to window-level settings. The SUVmax is not operator-dependent but is subject to variability in data acquisition and processing (18,25). With automated methods, these confounding factors have less influence on the results. User-independent segmentation algorithms for calculating the PV are much less prone to such errors. Segmentation with the RTL method incorporates the size of the tumor into the algorithm, is independent of the SBR, and inherently assumes spheroid tumor volumes (20). This method might be the better solution for solid tumors. However, high-grade gliomas are heterogeneous and may present as multifocal lesions. Therefore, the RTL algorithm might be less suitable for the evaluation of multiple lesions than the SBR method. Because of these multifocal and heterogeneous aspects of gliomas, a proliferative volume appears more representative than the SUVmax for predicting the OS. Whereas the SUVmax is the representation of 1 point in the tumor, the proliferative volume takes into account both the degree of proliferation and the volume, which expresses enhanced proliferation.
One of the limitations of 18F-FLT might be that a disruption of the blood–brain barrier is required for tumor targeting (9). Especially for low-grade gliomas, this requirement can be a restricting factor. For this reason, we selected only high-grade gliomas, in which the blood–brain barrier is always disrupted. Remarkably, we observed that the intracerebral uptake of 18F-FLT was not limited to areas of contrast enhancement as seen on MRI and in fact exceeded the area of contrast enhancement on the MRI in most cases. This finding implies that the uptake of 18F-FLT is not limited to a damaged blood–brain barrier as defined by contrast enhancement on MRI. One explanation might be the difference in resolution between PET and MRI. In areas of necrosis, in which mostly a ring of contrast enhancement is found, the uptake of 18F-FLT in this ring is mostly high and the segmented volume is expanded partly inside the necrotic area. Another possible explanation is that the size of gadoteric acid contrast is larger than 18F-FLT. 18F-FLT uptake might therefore already occur in an area of earlier and less severe blood–brain barrier damage. This area might be associated with the relative cerebral blood volume (rCBV), which has a stronger predictive value than conventional MRI in cerebral glioma (26,27). In low-grade glioma, the rCBV might reflect better the histopathology of the tumor (26). Weber et al. showed that in 75% of brain glioma cases, the 18F-FLT uptake is correlated to the rCBV (28). A limitation of 18F-FLT can be the 18F-FLT uptake in the bone marrow of the skull, which might interfere with calculation of the tumor volume. Another limitation of our study might be the different treatments of the patients. Although almost all patients received radiotherapy and chemotherapy, not all patients underwent a second operation. Additionally, 3 patients had previously undergone surgery, and of those, 2 received adjuvant radiotherapy. Whether and how pretreatment influenced 18F-FLT targeting cannot be established, but pretreatment apparently did not negatively affect the correlation of the PV and patient survival. However, the interpretation of the statistical analysis should be done with caution because of the limited number of patients relative to the number of variables.
The use of static rather than dynamic PET obviously prevents kinetic modeling. Because the Ki-67 index correlates best with the Ki derived from dynamic PET, static scanning may be considered a limitation of our study (13,14). Wardak et al. reported a better predictive value with a combination of kinetic parameters for the OS and progression-free survival than with single kinetic parameters and the SUV (29). However, this is probably not a major issue in imaging glioma, because others also showed good correlation of SUVmax with the Ki-67 index (30). Additionally, calculation of the PV does not require kinetic modeling.
CONCLUSION
We have shown that a single pretreatment 18F-FLT PET/CT and subsequent calculation of the PV predicts OS in high-grade glioma, also providing thresholds that separate patients with long survival from those with a poor prognosis. The PVSBR method provides a simple, user-independent, clinically easily performed method for assessing the volume of the proliferative part of the tumor. These are important factors for implementing this technique into neurooncology clinical practice. The PVSBR might assist in clinical decision making on the choice of treatment. Furthermore, our findings may serve as a basis for future studies in which the proliferative part of tumors is subject to different therapeutic interventions (surgery, radiosurgery, stereotactic radiotherapy, or systemic targeted therapy). Whether the PVSBR can be used for monitoring and adjusting treatment of glioma is a question that will have to be resolved in future studies.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
The study was supported in part by an unrestricted grant from Schering Plough. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 17, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 24, 2012.
- Accepted for publication July 2, 2012.





{kind=link}
{kind=link}
{kind=link}