


Abstract
We evaluated 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) uptake in patients with newly diagnosed and recurrent gliomas and correlated the results with tumor grade and proliferative activity. Methods: 18F-FLT PET was investigated retrospectively in 56 patients, including 36 with newly diagnosed gliomas and 20 with recurrent gliomas. The standardized uptake values for tumor and normal contralateral hemisphere were calculated, and the tumor-to-normal (T/N) ratio was determined. Tumor grading and proliferative activity were estimated in tissue specimens. Results: There was a significant difference in T/N ratio among different grades of newly diagnosed gliomas and between low- and high-grade newly diagnosed and recurrent gliomas. 18F-FLT uptake correlated more strongly with the proliferative activity in newly diagnosed gliomas than in recurrent gliomas. Conclusion: 18F-FLT PET seems to be useful in the noninvasive assessment of grade and proliferation in gliomas, especially newly diagnosed gliomas.
In the management of primary brain gliomas, accurate pathologic grading of the primary lesion is essential, since histologic features are a major independent prognostic factor next to patient age and performance status (1). Because tissue sampling is often obtained by stereotactic biopsy and, therefore, represents only a small part of the primary tumor, there is a probability that the true tumor grade will be underestimated (2). Thus, noninvasive imaging-based technology for the detection of malignant progression is required to select the best possible treatment regimen.
PET with the glucose analog 18F-FDG gives metabolic information on the whole tumor in vivo and can guide stereotactic biopsies toward the most metabolically active part of the tumor (3). On 18F-FDG PET scans, high-grade brain tumors show 18F-FDG accumulation similar to that of normal gray matter, whereas low-grade brain tumors exhibit 18F-FDG activity similar to that of white matter. Therefore, high-grade tumors may be obscured by adjacent cortical activity, and low-grade tumors may not be distinguishable from adjacent normal white matter (4).
11C-methionine, an amino acid, is another PET tracer that can be used for brain tumor imaging (3,5,6). 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) has been investigated as a promising PET tracer for evaluating tumor proliferating activity in brain tumors (5–13). 18F-FLT is trapped within the cytosol after being monophosphorylated by thymidine kinase-1, a principle enzyme in the salvage pathway of DNA synthesis (14). Therefore, the accumulation of 18F-FLT is dependent on the presence of thymidine kinase-1, which is closely associated with cellular proliferation. Although Jacobs et al. (6) evaluated 18F-FLT PET, including kinetic modeling, in newly diagnosed and recurrent gliomas, they analyzed the data of both groups together. In several clinical studies, 18F-FLT has been validated for evaluation of tumor grade and cellular proliferation in newly diagnosed gliomas (5,10). To our knowledge, this is the first clinical study to compare these characteristics between newly diagnosed and recurrent gliomas using 18F-FLT PET. The purpose of this study was to retrospectively evaluate 18F-FLT uptake in patients with newly diagnosed and recurrent gliomas and to correlate the results with tumor grade and proliferative activity as indicated by the Ki-67 index.
MATERIALS AND METHODS
Patients
This study was approved by our institutional review board, and written informed consent was obtained from all patients.
A total of 56 patients (22 men, 34 women; mean age, 52.9 y; age range, 12–86 y) with brain gliomas who underwent 18F-FLT PET between June 2006 and August 2011 were retrospectively selected. The clinical characteristics of the patients investigated are shown in Table 1. Of the patients, 36 had newly diagnosed gliomas and 20 had recurrent gliomas that had been treated previously. Among the latter 20 patients, 4 had been treated with surgery; 12 with surgery, chemotherapy, and radiotherapy; and 4 with surgery and radiotherapy. The median interval between the initial diagnosis and the recurrence was 105 wk (range, 12–750 wk).
Clinical Characteristics of 56 Patients with Brain Gliomas
Pathologic diagnosis had been obtained by stereotactic biopsy or open surgery. The median interval between the 18F-FLT PET scan and the pathologic diagnosis was 9 d (range, 1–42 d) for newly diagnosed gliomas and 14 d (range, 6–30 d) for recurrent gliomas. The tumor was graded according to the World Health Organization classification for neuroepithelial tumors (15). The distribution of tumor grades and types according to the World Health Organization classification was as follows: 12 grade II astrocytomas, 1 grade II oligoastrocytoma, 1 grade II ependymoma, 7 grade III anaplastic astrocytomas, 4 grade III anaplastic oligoastrocytomas, and 31 grade IV glioblastomas.
18F-FLT Synthesis and PET
18F-FLT was synthesized using the method described by Machulla et al. (16). The radiochemical purity of the produced 18F-FLT was greater than 98%.
All acquisitions were performed using an ECAT EXACT HR+ scanner (Siemens Medical Solutions, USA, Inc.). PET scans were acquired in the 3-dimensional mode. Sixty minutes after an intravenous injection of 18F-FLT (3.7 MBq/kg), a 5-min transmission scan was obtained using an external source of 68Ge for the purpose of attenuation correction. This acquisition was immediately followed by an emission scan for 15 min. PET images were reconstructed with ordered-subset expectation maximization using 6 iterations and 16 subsets.
Data Analysis
The images were visually analyzed by 2 experienced nuclear physicians independently, with side-by-side reference to MR or CT images for exact localization of the tumor. Any difference of opinion was resolved by consensus. Tumor lesions were identified as areas of focally increased uptake, exceeding that of normal brain background.
Semiquantitative analysis was performed using the standardized uptake value (SUV). The region of interest was placed over the entire tumor using the transverse PET image. For the reference tissue, a circular region of interest of 15 × 15 mm was manually placed on the uninvolved contralateral hemisphere in the plane that showed maximum 18F-FLT tumor uptake. Radioactivity concentrations measured in the region of interest were normalized to injected dose per patient’s body weight by calculation of SUV. The maximal SUV for tumor and the mean SUV for reference tissue were calculated. The tumor–to–contralateral normal brain tissue (T/N) ratio was determined by dividing the tumor SUV by the SUV of the contralateral hemisphere.
Ki-67 Immunohistochemistry
Formalin-fixed, paraffin-embedded sections of resected specimens from brain tumors were made for immunohistochemical staining. The Ki-67 index was estimated as the percentage of Ki-67–positive cell nuclei per 500–1,000 cells in the region of the tumor with the greatest staining density.
Statistical Analysis
All semiquantitative data were expressed as mean ± SD. Differences in T/N ratio among glioma grades were compared using ANOVA. The significance of individual differences was evaluated using the Tukey honestly significant difference test. Differences in T/N ratio between low- and high-grade gliomas were analyzed using the Mann–Whitney U test. The Ki-67 index and the T/N ratio were compared using linear regression analysis. Differences were considered statistically significant at a P value of less than 0.05.
RESULTS
18F-FLT Uptake and Glioma Grade
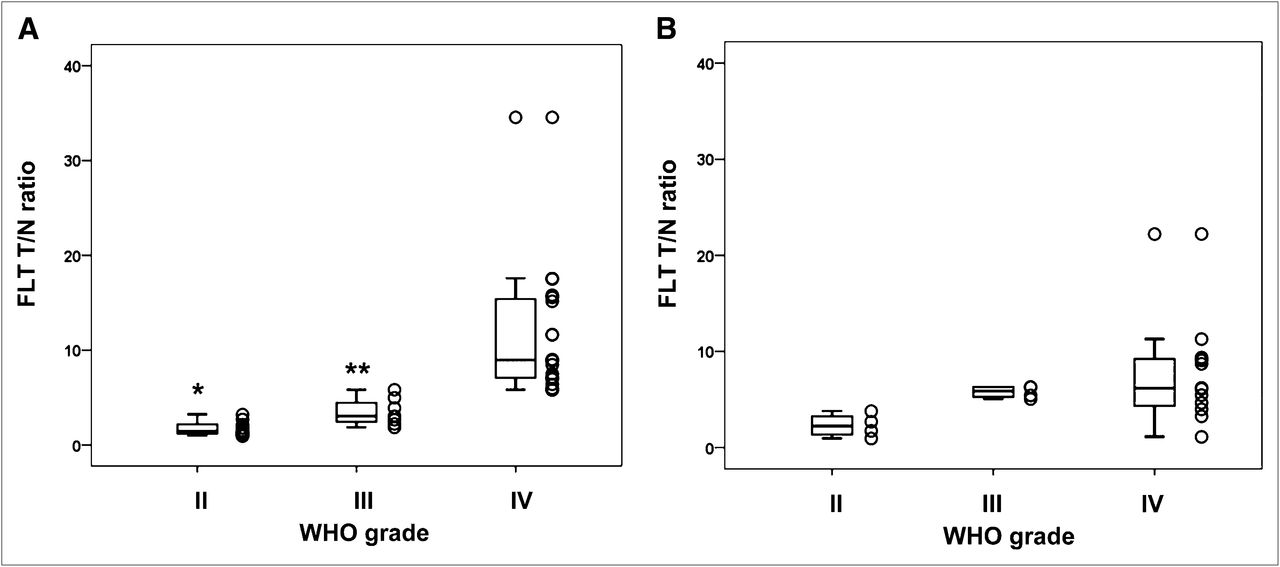
In newly diagnosed gliomas, 18F-FLT PET detected 2 of 10 grade II gliomas, 5 of 7 grade III gliomas, and all 19 grade IV gliomas. The mean (±SD) T/N ratios were 1.73 ± 0.76 in grade II gliomas, 3.51 ± 1.48 in grade III gliomas, and 11.63 ± 6.89 in grade IV gliomas. There was a significant difference between gliomas of grades II and IV (P < 0.001) and gliomas of grades III and IV (P < 0.004) (Fig. 1A). No significant difference in T/N ratio was noted between gliomas of grades II and III (P = 0.77). When grades III and IV were grouped together as high-grade gliomas, the mean (±SD) value of T/N ratio in high-grade gliomas (9.44 ± 6.94) was significantly higher than that in low-grade gliomas (1.73 ± 0.76) (P < 0.001). Figure 2 shows a typical case of newly diagnosed grade IV glioma.

Relationship between World Health Organization grade and 18F-FLT T/N ratio in newly diagnosed gliomas (A) and recurrent gliomas (B). Box plots show median, 25th percentile, and 75th percentile of data, with minimum and maximum represented by whiskers. *P < 0.001 as compared with grade IV group. **P < 0.004 as compared with grade IV group.

Radiologic images of 27-y-old woman with newly diagnosed World Health Organization grade IV glioblastoma. Transverse T1-weighted MR image with contrast enhancement (A) shows enhanced mass in right frontal lobe. Transverse 18F-FLT PET image (B) shows increased uptake (T/N ratio = 11.67) in tumor.
In recurrent gliomas, 18F-FLT PET detected 1 of 4 grade II gliomas, 3 of 4 grade III gliomas, and all 12 grade IV gliomas. The mean (±SD) T/N ratios were 2.31 ± 1.23 in grade II gliomas, 5.79 ± 0.62 in grade III gliomas, and 7.63 ± 5.43 in grade IV gliomas. No significant differences in T/N ratio were noted among glioma grades (II vs. III, P = 0.52; II vs. IV, P = 0.12; III vs. IV, P = 0.75) (Fig. 1B). There was a significant difference between the mean (±SD) T/N ratios in high-grade gliomas (7.17 ± 4.73) and low-grade gliomas (2.31 ± 1.23) (P < 0.01) although P value was weaker than that for newly diagnosed gliomas.
18F-FLT Uptake and Ki-67 Immunohistochemistry
In newly diagnosed gliomas, linear regression analysis indicated a significant correlation between T/N ratio and the Ki-67 index (r = 0.81, P < 0.001; Fig. 3A). In recurrent gliomas, although there was a correlation between T/N ratio and the Ki-67 index (r = 0.50, P < 0.03; Fig. 3B), the correlation was weaker.

Linear regression analysis demonstrates significant correlation between 18F-FLT T/N ratio and proliferative activity (Ki-67 index) in newly diagnosed gliomas (A) (r = 0.81, P < 0.001) and recurrent gliomas (B) (r = 0.50, P < 0.03).
DISCUSSION
In the present study, we evaluated 18F-FLT uptake in patients with newly diagnosed and recurrent gliomas. 18F-FLT PET was found to be useful in the assessment of grade and proliferation in gliomas, especially newly diagnosed gliomas.
With respect to the mechanism of 18F-FLT uptake by brain tumors, breakdown of the blood–brain barrier (BBB) has been reported to contribute considerably to tracer uptake (9). 18F-FLT permeates the cell membrane by facilitated diffusion (17) and is phosphorylated by thymidine kinase-1, which leads to intracellular trapping (17,18). During DNA synthesis, the concentration of thymidine kinase-1 increases about 10-fold and is, therefore, an accurate reflection of cellular proliferation (18). Choi et al. (8) suggested that both thymidine kinase-1 activity and BBB permeability are major factors in 18F-FLT uptake by brain lesions. However, Jacobs et al. (6) reported that 18F-FLT could detect tumor regions that did not present with gross destruction of the BBB as shown by gadopentetate dimeglumine enhancement on MRI. The regional distribution of 18F-FLT uptake with and without gadopentetate dimeglumine enhancement on MRI suggests the presence of various tissue compartments in which 18F-FLT uptake may be due to breakdown of the BBB, increased transport, increased proliferation, or a variable combination of these mechanisms. Unfortunately, we did not take the opportunity to compare 18F-FLT PET images with gadopentetate dimeglumine enhancement or any other MRI parameter. Further studies are needed to evaluate the relationship between 18F-FLT uptake and gadopentetate dimeglumine enhancement in newly diagnosed and recurrent gliomas.
In the present study, the T/N ratio of high-grade gliomas was significantly higher than that of either newly diagnosed or recurrent low-grade gliomas. Although this finding is similar to those from previous studies by Chen et al. (7) and Choi et al. (8), T/N ratios were very different. This difference might be explained by the inhomogeneity of the examination protocols such as differences in the start time for imaging, the calculation method for SUV, or the patient populations. Their studies (7,8) analyzed the data of newly diagnosed and recurrent tumors together. On the other hand, in the present study, data for newly diagnosed and recurrent gliomas were analyzed separately. Furthermore, in the present study, there was a significant difference in T/N ratio among the grades of newly diagnosed gliomas but not of recurrent gliomas. Of the 20 patients with recurrent gliomas, 16 (80%) had received chemoradiotherapy or radiotherapy before the PET study. Radiation and chemoradiotherapy, used as an adjuvant therapy for gliomas, can cause loosening of endothelial tight junctions, vascular leakage, or endothelial cell death and thus can increase vascular permeability (19). Radiation could also act to increase vascular permeability not only in the BBB but also in the blood–tumor barrier (19). We suspect that in addition to increased proliferation, breakdown of the BBB and blood–tumor barrier in recurrent gliomas contributes to the degree of 18F-FLT uptake. Furthermore, there is a biologic difference between newly diagnosed and recurrent gliomas. In recurrent gliomas, recurrent tumor and treatment-induced necrosis frequently coexist.
Barwick et al. (20), in a review article, mentioned that 18F-FLT uptake reflected tumor proliferation when compared with histopathologic Ki-67 expression in non–small cell lung cancer, colorectal cancer, lymphoma, and gliomas. Choi et al. (8) evaluated 18F-FLT uptake and proliferative activity in 9 patients with gliomas, including 1 recurrent glioma. They showed a significant correlation (r = 0.817) between 18F-FLT uptake and Ki-67 index. Chen et al. (7) evaluated 18F-FLT uptake and proliferative activity in 14 patients with gliomas, including 6 previously treated with radiation. They also showed a significant correlation (r = 0.84) between 18F-FLT uptake and Ki-67 index. In the present study, although 18F-FLT uptake correlated significantly with Ki-67 index in both newly diagnosed and recurrent gliomas, the correlation in recurrent gliomas was not as significant as that in newly diagnosed gliomas. In addition to increased proliferation, breakdown of the BBB and blood–tumor barrier may contribute to the degree of 18F-FLT uptake in previously treated gliomas. Kinetic analysis of 18F-FLT PET might clarify whether the transport effect or metabolic trapping largely contributes to the increased uptake of 18F-FLT in the tumor (6).
Jacobs et al. (6) compared 18F-FLT with 11C-methionine in gliomas and showed that 11C-methionine was more sensitive for tumor detection. An amino acid PET tracer such as 11C-methionine and MRI may be the best mode for the initial diagnosis of gliomas. In contrast to amino acid tracers, 18F-FLT allows for noninvasive assessment of tumor proliferation. Schiepers et al. (13) evaluated the kinetics of 18F-FLT during treatment monitoring of recurrent high-grade glioma. Further studies including kinetic analysis are needed to evaluate the clinical usefulness of 18F-FLT PET in gliomas for assessing therapeutic response and survival in larger study groups.
CONCLUSION
18F-FLT PET seems to be useful in the noninvasive assessment of grade and proliferation in gliomas, especially newly diagnosed gliomas. 18F-FLT PET might not provide information at the initial diagnosis of gliomas additional to that provided by amino acid PET tracers and MRI. Further studies might identify the role of 18F-FLT in assessing the response to antiproliferative treatment in patients with recurrent gliomas.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 18, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 18, 2012.
- Accepted for publication July 5, 2012.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.