


Abstract
This study aimed to estimate the radiation absorbed doses to normal tissues and tumor lesions during radioimmunotherapy with 177Lu-cG250. Serial planar scintigrams after injection of 111In-cG250 or 177Lu-cG250 in patients with metastasized renal cell carcinoma were analyzed quantitatively. The estimated radiation doses were correlated with observed hematologic toxicity. In addition, the accuracy of the predicted therapeutic absorbed doses, based on diagnostic 111In-cG250 data, were determined. Methods: Twenty patients received a diagnostic tracer activity of 111In-cG250 (185 MBq), followed by radioimmunotherapy with 177Lu-cG250. The administered activity of 177Lu-cG250 was escalated by entering 3 patients at each activity level starting at 1,110 MBq/m2, with increments of 370 MBq/m2. After each diagnostic and therapeutic administration, whole-body scintigraphic images and pharmacokinetic data were acquired. Hematologic toxicity was graded using the Common Toxicity Criteria, version 3.0. Diagnostic 111In-cG250 data were used to simulate 177Lu and 90Y data by correcting for the difference in physical decay. Absorbed doses were calculated for the whole body, red marrow, organs, and tumor metastases for the therapeutic 177Lu-cG250, simulated 177Lu-cG250, and simulated 90Y-cG250 data. Results: Observed hematologic toxicity, especially platelet toxicity, correlated significantly with the administered activity (r = 0.85), whole-body absorbed dose (r = 0.65), and red marrow dose (r = 0.62 and 0.75). An inverse relationship between the mass and absorbed dose of the tumor lesions was observed. Calculated mean absorbed doses were similar for the simulated and measured 177Lu-cG250 data. Absorbed doses (whole body and red marrow) based on the simulated 177Lu-cG250 data correlated with the observed platelet toxicity (r = 0.65 and 0.82). The tumor–to–red marrow dose ratio was higher for radioimmunotherapy with 177Lu-cG250 than for radioimmunotherapy with 90Y-cG250, indicating that 177Lu has a wider therapeutic window for radioimmunotherapy with cG250 than 90Y. Conclusion: In patients with metastasized renal cell carcinoma, hematologic toxicity after treatment with 177Lu-cG250 can be predicted on the basis of administered activity and whole-body and red marrow–absorbed dose. Diagnostic 111In-cG250 data can be used to accurately predict absorbed doses and myelotoxicity of radioimmunotherapy with 177Lu-cG250. These estimations indicate that in these patients, higher radiation doses can be guided to the tumors with 177Lu-cG250 than with 90Y-cG250.
Renal cell carcinoma (RCC) is a disease with approximately 58,000 new patients each year in the United States and accounts for 3% of all malignancies (1). The only curative option to date for RCC is (partial) nephrectomy. Prognosis of untreated metastasized RCC is poor, with a median survival of 12 mo. With the advent of targeted agents, this prognosis has increased dramatically, more than doubling overall survival (2). However, side effects of these compounds are common and often severe (3). Therefore, we aim to develop an effective radioimmunotherapeutic approach for the treatment of RCC using the radiolabeled anti-CAIX antibody cG250.
The main goal in radioimmunotherapy is to maximize the absorbed dose to the tumor, while maintaining the dose to healthy tissues at acceptable levels. The dose-limiting normal tissue in radioimmunotherapy is the red marrow. Thrombocytopenia and leukopenia are generally the initial and most severe manifestations of myelotoxicity after radioimmunotherapy (4).
In several studies, methods are defined to estimate the red marrow dose based on blood activity data or planar scintigrams (5–8). Previous studies on the relationship between radiation dose estimates and myelotoxicity were variable (7,9–15). Results might have been influenced by the used method to calculate the red marrow dose, the radionuclide used, or patient-specific factors. Recently, Baechler et al. showed, for example, that the elapsed time since the last chemotherapy is an important parameter in the prediction of toxicity (16).
The ability to predict the therapeutic dose to tumor lesions and healthy organs could provide tools for treatment planning. For individual dosing, each radioimmunotherapy treatment can be preceded by a diagnostic infusion of the same monoclonal antibody (mAb) labeled with a γ-emitter (11). The analysis of the images of an antibody labeled with 111In could potentially be used to predict the targeting of the same antibody labeled with the β-emitting radionuclide 90Y or 177Lu. In a study of DeNardo et al., mAb Lym-1 labeled with 111In was used to calculate the absorbed doses for 90Y-Lym-1 in patients with non-Hodgkin lymphoma (17). Vallabhajosula et al. used 111In-J591 as a surrogate for 90Y-J591 (10). However, because 90Y is not suitable for imaging as it is a pure β-emitting radionuclide, the accuracy of these dosimetric predictions could not be proven.
During a phase I study at our institution, patients with progressive clear cell RCC could receive multiple therapeutic doses of 177Lu-cG250. Before each therapeutic administration, patients received a diagnostic infusion with 111In-cG250. We used the pharmacokinetic and scintigraphic data to estimate radiation doses of the therapeutic injections to normal tissues and metastases and investigated whether these doses correlated with the observed hematologic toxicity. We investigated whether the dosimetric analysis of the diagnostic injections could be used to predict the radiation doses of the therapeutic injections after the first treatment cycle. Furthermore, absorbed dose predictions were made for radioimmunotherapy with 90Y-cG250 to determine the most suitable β-emitter for radioimmunotherapy with the radiolabeled anti-CAIX antibody in these patients.
MATERIALS AND METHODS
Patients
Dosimetric data of 20 patients with progressive metastasized RCC (16 men, 4 women) who had all undergone a nephrectomy of the tumorous kidney were included. The mean age of the patients was 58 y (range, 29–74 y). The study (Clinical Trials NCT00142415) was approved by the regional Medical Ethical Review Committee of the Radboud University Nijmegen Medical Centre and the Institutional Review Board of the Ludwig Institute for Cancer Research. The study was monitored by Omnicare Corp., commissioned by the Ludwig Institute for Cancer Research. Written informed consent was obtained from all patients before study entry.
mAb cG250 and Radiolabeling
cG250 is a high-affinity (Ka = 4 × 109 M−1) chimeric, IgG1 mAb, reactive with the CAIX antigen, a transmembrane glycoprotein overexpressed on the cell surface of most (>95%) clear cell RCCs (18). Vials (10 mg/mL) of clinical-grade cG250 were obtained from the Ludwig Institute for Cancer Research. cG250 was conjugated with DOTA (Macrocyclics) as described previously (19) at Memorial Sloan-Kettering Cancer Center. The cG250–DOTA conjugate was radiolabeled with 111In (Covidien) for tracer injections in a 0.25 M ammonium acetate buffer, pH 5.4, for 30 min at 45°C. cG250–DOTA was labeled with 177Lu (IDB Holland) for therapeutic injections in a 0.25 M ammoniumacetate buffer, pH 5.4, for 60 min at 45°C. All labeling procedures using 111In or 177Lu were performed under strict metal-free conditions. All radiolabeled cG250 preparations were purified by gel filtration on a PD-10 column (GE Healthcare) eluted with phosphate-buffered saline supplemented with 5 mM diethylenetriaminepentaacetic acid and 10 mM ascorbic acid. For all preparations, the amount of non–mAb-associated radiolabel was determined by instant thin-layer chromatography (ITLC) with ITLC silica gel strips (Pall Corp. Life Sciences), using 0.1 M citrate buffer, pH 6.0, as the mobile phase (Rf, 0 for radiolabeled antibody and 0.8–1 for free and chelated radionuclides) (18). The radiochemical purity was greater than 99% for 111In-DOTA-cG250 and 99.3% ± 0.9% for 177Lu-DOTA-cG250. The immunoreactive fraction determined as described previously was 90.1% ± 5.3% and 89.8% ± 6.8% for the 111In-cG250 and 177Lu-cG250 preparations, respectively.
Study Design
In this phase I study, the maximum-tolerated dose (MTD) of 177Lu-cG250 radioimmunotherapy was determined by entering 3 patients at each activity level, starting at 1,110 MBq/m2, with dose increments of 370 MBq/m2. The MTD was defined as the administered activity at which no more than 1 of 6 patients showed dose-limiting toxicity (DLT). DLT was defined as grade 3 or greater nonhematologic toxicity or grade 4 or greater hematologic toxicity (platelets < 25 × 109/L or leukocytes < 1.0 × 109/L), lasting for more than 4 wk, or the occurrence of hemoglobin less than 4.9 mmol/L or thrombocytes less than 10 × 109/L at any time point. The administered 177Lu dose was calculated with the formula from a study of Mosteller (20).
Toxicity was monitored weekly, by determining the hematologic and blood chemistry laboratory parameters, and was scored according to the U.S. National Cancer Institute Common Toxicity Criteria (version 3.0).
All radioimmunotherapy administrations were preceded by a diagnostic tracer of 111In-cG250 (185 MBq; 10 mg of cG250; total volume, 5 mL) to visually assess preferential uptake of the radiolabeled antibody in the tumor lesions and to exclude the presence of human antichimeric antibodies.
Patients received 1 (n = 23), 2 (n = 13), or 3 (n = 4) cycles of treatment. The clinical results of this study will be described in another paper. In the current paper, dosimetric analysis of the first treatment cycle of the first 20 patients is performed. Analysis of the last 4 patients has not been performed because of logistic reasons. Dosimetric analyses of the second and third treatment cycles were not incorporated, to avoid confusion and because of the limited amount of data.
Imaging and Pharmacokinetics
After each 111In-cG250 administration, 3 whole-body scintigrams were acquired (directly after injection, at 2–4 d after injection, and at 5–7 d after injection). The images were recorded in conjugate view using a double-head γ-camera (ECAM, Siemens Inc.), equipped with parallel-hole medium-energy collimators. Symmetric energy windows were set at 15% of the 111In photopeaks at 172 and 247 keV. Images consisted of summed counts collected in both windows. The scan speed was 8, 6, and 4 cm/min at days 0, 2–4, and 5–7 after injection, respectively. The matrix size was 256 × 1,024, with a pixel size of 2.4 × 2.4 mm. Images obtained after infusion of 177Lu-cG250 were recorded using a symmetric 15% energy window of 208 keV at the same time points and with the same scan speeds as after the 111In-cG250 infusion.
Blood samples were drawn directly; at 30, 60, and 120 min; and at 2–4 and 5–7 d after the 111In-cG250 and 177Lu-cG250 infusions. The activity concentration in the serum from these samples was counted in a shielded 7.6-cm (3-in) well-type γ-counter (Wizard; LKB/Wallac, Perkin-Elmer). To correct for radioactive decay, reference samples containing a known fraction of the administered activity were measured simultaneously. The activity concentrations in the serum samples were corrected for the hematocrit content in the patient's blood to obtain blood activity concentrations.
Dosimetry
The radiation absorbed doses to the whole body, liver, red marrow, lungs, heart, testes, normal kidney, and metastases delivered by therapeutic 177Lu-cG250 injections were calculated according to the MIRD scheme (21).
Metastatic lesions measurable on CT and visualized in at least 1 of the scintigraphic images were analyzed. The volume
Residence times of the source organs and metastases were calculated using SPRIND, a software package for integrated data processing for internal dose assessment (6). Regions of interest for source organs and tumors were drawn on both anterior and posterior scintigraphic images. The counts within the regions of interest were corrected for attenuation and background contribution as described by Visser et al. (6). The geometric mean was calculated, and the data were integrated over time using the trapezoid method. After the last scan, SPRIND assumes only physical decay of the radionuclide in the source organs. To calculate the absorbed doses, residence times were imported into the software package OLINDA/EXM (22). Radiation absorbed doses to the whole body and organs of interest were calculated using the adult male and the adult female phantom. The sphere model was used to determine the radiation absorbed doses to the metastases (22).
The red marrow–absorbed dose was calculated using 2 methods. First, the absorbed dose to the red marrow was calculated using the scintigraphic images. In SPRIND, regions of interest were drawn over the left and right part of the cranium. The residence times of the left and right cranium were summed and divided by the fraction of the red marrow mass in the cranium to the total red marrow mass in the body, for which the default value of 0.119 was taken from the reference man according to the International Commission on Radiological Protection (23). The second method was the blood-based method as described by Shen et al. (5). This method was also implemented in SPRIND (Visser et al. (6)).
Predictive Dosimetry
Dosimetric data obtained after the diagnostic 111In-cG250 infusion were used to calculate the predicted therapeutic doses from 177Lu-cG250, assuming identical biodistribution and biologic clearance of 111In-cG250 and 177Lu-cG250. Simulated 177Lu scans were generated by correcting the 111In whole-body scintigrams for the difference in physical decay of 111In and 177Lu. Each 111In-cG250 scintigram (anterior and posterior images) was multiplied pixelwise by et(λIn − λLu) (t = time after injection) to obtain simulated whole-body scintigrams for 177Lu. The resulting simulated 177Lu scintigrams were used to calculate residence times with SPRIND and the simulated absorbed doses with OLINDA for the organs of interest and metastases.
The blood-based red marrow–absorbed dose for 177Lu was also simulated. To simulate the blood residence time of 177Lu, 111In-cG250 blood data and reference samples were used to determine the biologic clearance of activity from the blood, and physical clearance was incorporated by multiplication with e−λLut.
To provide insight in the absorbed doses for radioimmunotherapy with 90Y-cG250, the same methods were used to simulate 90Y data.
Statistical Analysis
The Pearson correlation coefficient was determined to evaluate the relationship between the image- and the blood-based methods to calculate the red marrow dose, between tumor mass and tumor-absorbed dose, and between calculated absorbed doses for 177Lu-cG250 and simulated data. Hematologic toxicity was correlated with administered activity, whole-body dose, red marrow dose, and the electron contribution of the red marrow dose. In addition, the relationship between hematologic toxicity and the simulated whole-body and red marrow dose was determined. The tumor–to–red marrow dose ratios were determined to compare (simulated) 177Lu-cG250 data with simulated 90Y-cG250 data.
RESULTS
Patients
All 20 patients completed the full course of 111In-cG250 and 177Lu-cG250 radioimmunotherapy. In each patient, only data from the first treatment cycle were used for dosimetric analysis. DLT was noted in 1 patient at the 1,850 MBq/m2 activity level. Because the other 5 patients who received this activity showed no DLT, the administered activity was further incremented. At the 2,590 MBq/m2 activity level, DLT was seen in all 3 patients; therefore, the administered activity was reduced to 2,405 MBq/m2. This activity level proved to be safe in 6 patients (only 1 of 6 patients had DLT), and by definition the latter dose was designated as the MTD.
Data
Imaging data after the treatment were used to determine the absorbed dose in the organs of interest and metastases after administration with 177Lu-cG250. The diagnostic 111In-cG250 data were also used to evaluate the predictive value of the simulated 177Lu-cG250 data and to calculate absorbed doses for radioimmunotherapy with 90Y-cG250.
The 177Lu-cG250 data of 2 patients had to be excluded from the analysis because of incomplete or inconsistent scintigraphic data. Another patient (patient 17) showed an unexpected high uptake in the liver and red marrow after injection of 177Lu-cG250 because of the presence of human antichimeric antibodies or the presence of aggregates in the radiolabeled antibody preparation. The dosimetric results of this patient were therefore excluded from the analysis. Subsequently, dosimetry data of 17 patients have been analyzed in this study.
For the 177Lu-cG250 and 111In-cG250 data, 40 and 48, respectively, metastases were used for tumor-absorbed dose calculations. The weight of these tumors, determined on the CT images, ranged from 0.6 to 319 g.
A complete set of blood activity data was acquired from 15 (177Lu-cG250) and 16 (111In-cG250) patients. These pharmacokinetic data were used to calculate the blood-based red marrow–absorbed dose in these patients.
177Lu-cG250 Radiation Doses
The estimated mean radiation absorbed doses after 177Lu-cG250 radioimmunotherapy were 0.24 ± 0.04 mGy/MBq for the whole body, 0.49 to 1.90 mGy/MBq for the healthy organs, and 0.44 ± 0.07 mGy/MBq (image-based) and 0.35 ± 0.07 mGy/MBq (blood-based) for the red marrow (Table 1).
Radiation Absorbed Dose in Whole Body, Organs, and Metastases for 177Lu-cG250, Simulated 177Lu-cG250, and Simulated 90Y-cG250 (mGy/MBq)
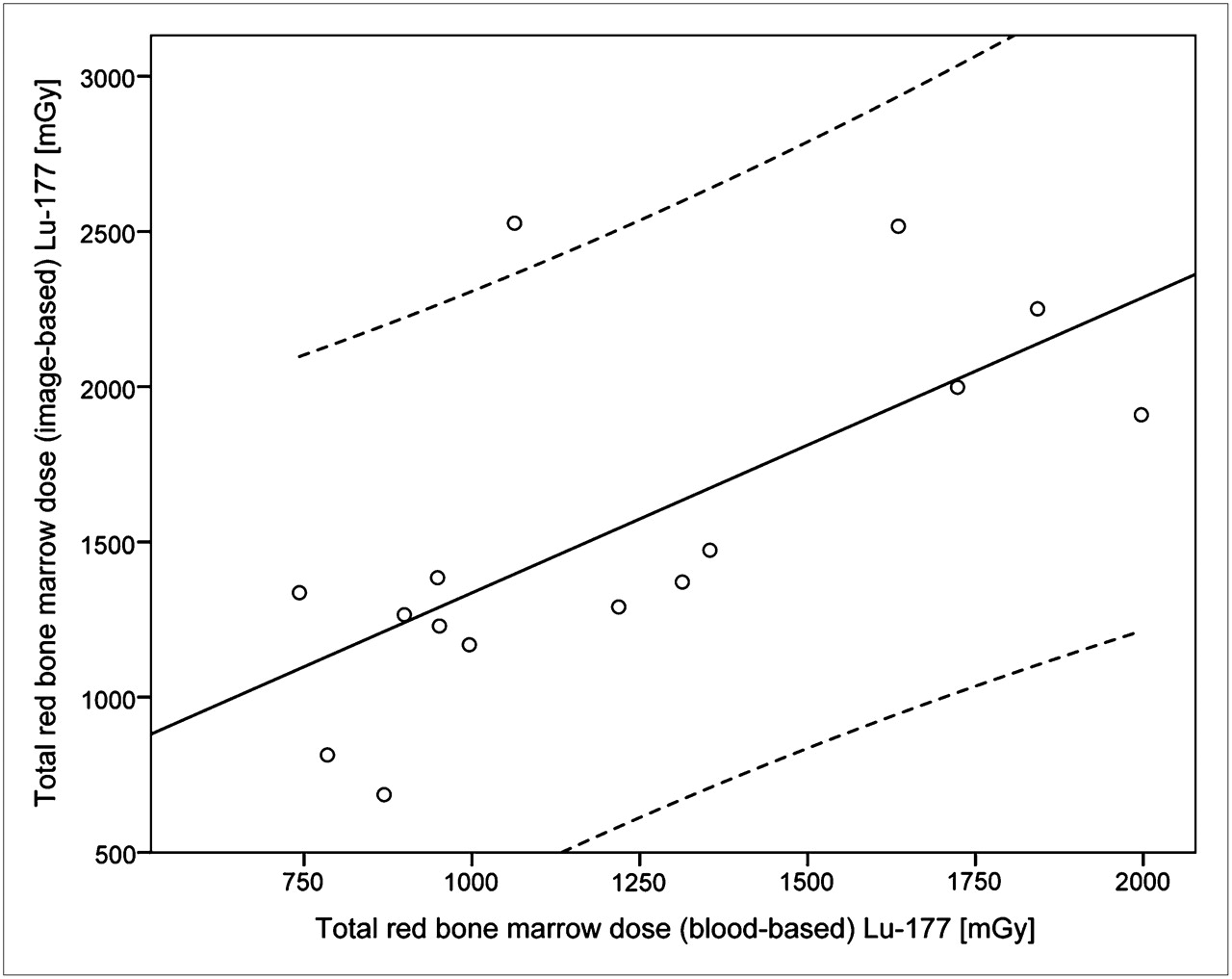
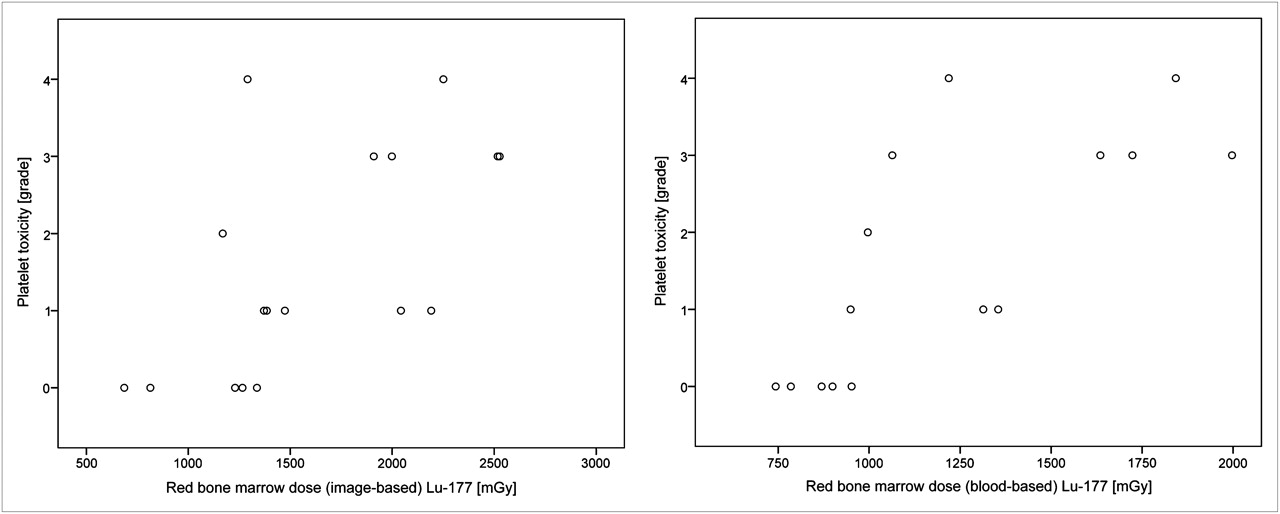
The results of the image- and blood-based methods to calculate the red marrow–absorbed dose correlated significantly (r = 0.68, P = 0.005, Fig. 1). Observed thrombocyte toxicity correlated significantly with the administered activity (r = 0.85), whole-body dose (r = 0.65), and image- and blood-derived red marrow dose (r = 0.62 and 0.75, respectively, Fig. 2). Leukocyte toxicity correlated significantly with the administered activity (r = 0.66) and the blood-based red marrow dose (r = 0.53). However, there was no significant relationship between the leukocyte toxicity and the whole-body dose or the image-based red marrow dose. The correlations are summarized in Tables 2 and 3.
Pearson Correlation Coefficients (and Its 2-Tailed Significance) Between Toxicity Grade and Administered Activity or Absorbed Dose Calculations for 177Lu-cG250
Pearson Correlation Coefficients (and Its 2-Tailed Significance) Between Toxicity Grade and Administered Activity or Absorbed Dose Calculations for Simulated 177Lu-cG250 (mGy)
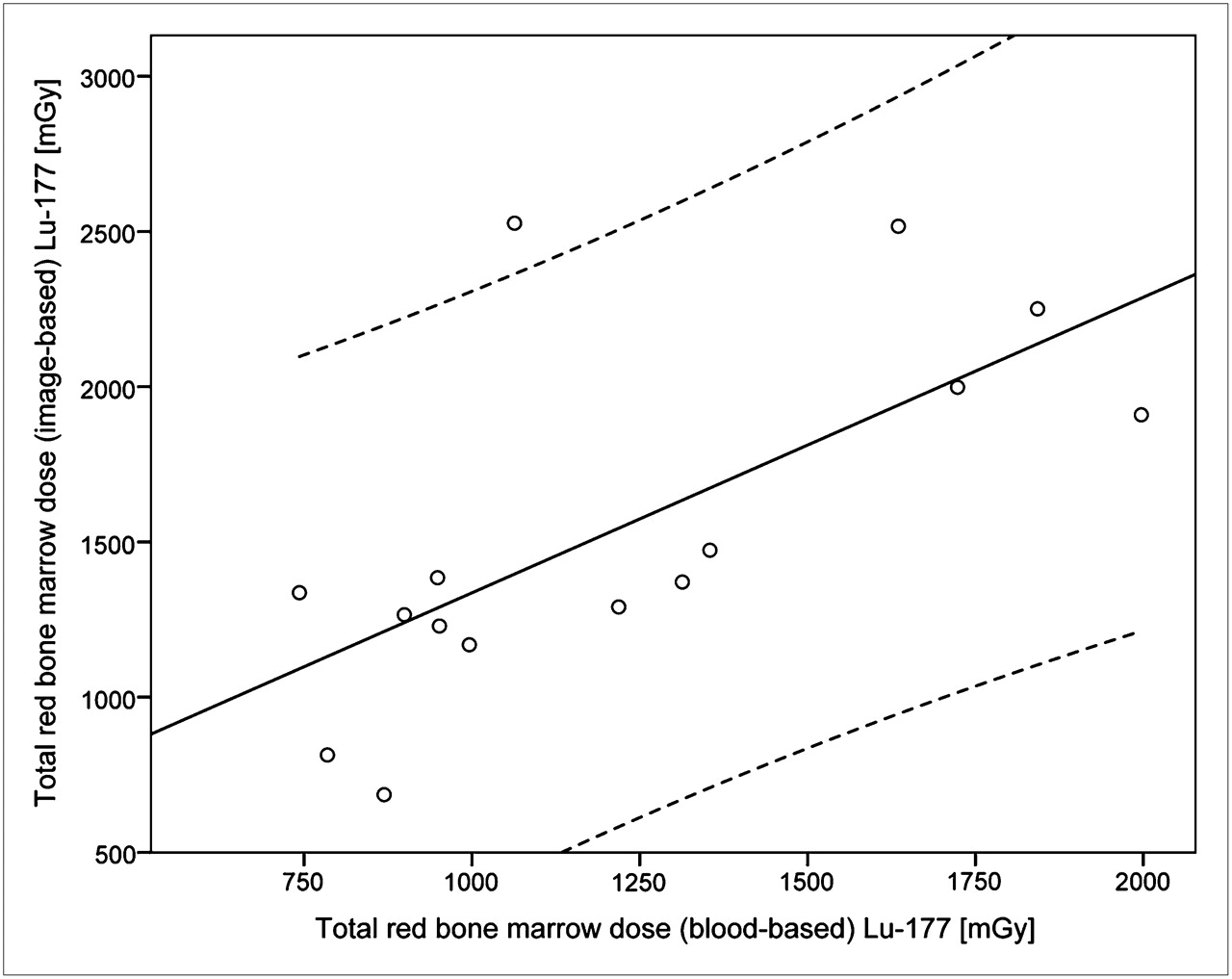
Total red marrow dose based on image-based method plotted against total red marrow dose based on blood-based method (r = 0.68, P = 0.005). Striped line is 95% confidence interval.

Platelet toxicity (grade according to Common Toxicity Criteria, version 3.0) plotted against red marrow dose based on image-based method (r = 0.62, P = 0.007) and blood-based method (r = 0.75, P = 0.001).
Absorbed doses to the tumor lesions varied widely from 0.47 to 17.29 mGy/MBq. The mean tumor–to–red marrow dose ratio for 177Lu-cG250 was 13.0 and 16.3, respectively, for the image- and blood-based methods. The total tumor dose during the first treatment cycle varied from 1.9 to 92.0 Gy. The radiation dose to the tumor lesions correlated inversely with the mass of the tumor lesions (r = −0.44, P < 0.005, Fig. 3).

Absorbed dose in metastases for 177Lu-cG250 radioimmunotherapy plotted against weight of metastatic lesions on logarithmic scales (r = −0.44, P < 0.005). Striped line is 95% confidence interval.
Simulated 177Lu-cG250 Radiation Doses
The simulated 177Lu-cG250 absorbed doses for the whole body, organs, and metastases based on the diagnostic 111In-cG250 data are presented in Table 1. The calculated doses were similar to the doses as derived from the 177Lu-cG250 images (Fig. 4). However, for the individual patient, slight differences were found. For example, the largest differences in calculated red marrow dose were −20.0% and 14.9% for the image-based method and −25.5% and 7.7% for the blood-based method. There is a significant correlation between the 177Lu-cG250 and simulated absorbed dose calculations for the whole body, liver, heart wall, red marrow, lungs, testes, and metastases (r = 0.82–0.98, P < 0.001). In contrast, the calculated kidney-absorbed dose of the simulated data in comparison to the 177Lu-cG250 data did not show any correlation (r = −0.28).

Mean absorbed dose (±SD) in organs of interest, whole body, and metastases for 177Lu-cG250, simulated 177Lu-, and 90Y-cG250 data. RM = red marrow.
Thrombocyte and leukocyte toxicity correlated significantly with the simulated whole-body and red marrow (image-based) dose (r = 0.55–0.82, P < 0.05). In addition, thrombocyte toxicity correlated significantly with the blood-based red marrow dose (r = 0.65, P < 0.01). These correlations are summarized in Tables 2 and 3. For the simulated 177Lu-cG250 data, the tumor–to–red marrow dose ratio was 11.9 (image-based) and 15.7 (blood-based).
Simulated 90Y-cG250 Radiation Doses
Simulated mean radiation absorbed doses for radioimmunotherapy with 90Y-cG250 were 0.64 mGy/MBq for the whole body, 1.45–4.32 mGy/MBq for the normal organs, and 0.90 mGy/MBq (image-based) and 0.81 mGy/MBq (blood-based) for the red marrow (Table 1). Radioimmunotherapy with 90Y-cG250 resulted in a theoretic mean absorbed dose of 9.76 mGy/MBq to the metastases. The tumor–to–red marrow dose ratio for this simulated 90Y-cG250 data was 10.8 and 12.0 for, respectively, the image- and blood-based methods. Mean absorbed doses to the bone marrow (mGy/MBq) were approximately 2–3 times higher than the (simulated) 177Lu-cG250 data (Fig. 4).
DISCUSSION
This study was designed to estimate the radiation absorbed doses to normal tissues and tumor lesions during radioimmunotherapy with 177Lu-cG250 in patients with clear cell RCC. Radiation-induced myelotoxicity was dose limiting in these patients. An accurate estimation of the red marrow dose is essential for reliable predictions of the maximum activity that can be administered safely. The radiation dose to the red marrow can be estimated using the activity levels in the blood (5), as long as the radiolabeled antibody does not bind specifically to the cells in the bone marrow. However, various other imaging methods to estimate the red marrow dose have been described (6–8). DeNardo et al. showed, for example, that an image-based method, unlike the blood-based method, was able to predict thrombocytopenia and leukopenia (7). In the present study, both the blood-based method and an image-based method were used to estimate the red marrow dose. The calculated mean absorbed doses for both methods were in the same range, 0.35 versus 0.44 mGy/MBq. In addition, there was a significant correlation between the red marrow dose calculated with both methods (r = 0.68, P = 0.005). The blood-based red marrow–absorbed dose was 0.35 ± 0.07 mGy/MBq for 177Lu-cG250, which is somewhat higher than reported by Vallabhajosula et al. (10) for radioimmunotherapy with 177Lu-J591 (0.32 ± 0.10 mGy/MBq). This slight difference in red marrow dose is in agreement with the difference in MTD: 2,405 MBq/m2 for 177Lu-cG250 and 2,590 MBq/m2 for 177Lu-J591 (10).
In this patient population, the observed hematologic toxicity ranged from grade 0 to grade 4. The relationship among hematologic toxicity, the administered activity, and the absorbed dose calculations (whole body, red marrow) were analyzed. Myelotoxicity, especially thrombocyte toxicity, correlated significantly with the administered activity, whole-body dose, and red marrow dose. The correlation between myelotoxicity and the blood-based red marrow dose was higher than that between myelotoxicity and the image-based method. Therefore, in these patients, the blood-based method was a better predictor of myelotoxicity. Although the overall correlation between calculated red marrow dose and observed myelotoxicity is high, individual patients have had more severe toxicity than others at the same dose level, limiting the use of calculated dosimetry as a predictor of the biologic event of myelotoxicity. Larger patient cohorts will have to be studied to accurately determine whether dosimetric analyses can be used to predict the toxicity of individual patients.
In a series of previous radioimmunotherapy studies, no correlations were found between radiation absorbed doses and myelotoxicity (7,9,12,13). On the other hand, Divgi et al. (14) showed a significant correlation between the whole-body absorbed dose and the hematologic toxicity after radioimmunotherapy with 131I-cG250. Juweid et al. (15) described a significant correlation between the calculated red marrow dose and hematologic toxicity for radioimmunotherapy with a 131I-labeled anti–carcinoembryonic antigen antibody. Furthermore, Vallabhajosula et al. (10) showed that myelotoxicity correlated with the administered activity and red marrow–absorbed dose for radioimmunotherapy with 177Lu-J591. Moreover, Vallabhajosula et al. (10) showed that the blood-based red marrow dose correlated best with the fractional decrease of thrombocytes. Similarly, in our study the blood-based red marrow dose correlated best with the thrombocyte toxicity grade (r = 0.75).
Normal organs receiving the highest absorbed doses were the liver, kidney, and testes, with a mean dose of 1.26, 1.30, and 1.90 mGy/MBq, respectively. This dose was 5.8, 6.0, and 8.8 Gy, respectively, at MTD, for a mean body surface area of 1.79 m (2,24). The liver and kidney doses were well below the threshold for deterministic effects, which are, respectively, 30 and 23 Gy (25,26). On the basis of experiments using external-beam radiation therapy, it was suggested that a fractionated dose of 2 Gy or more to the testes could cause permanent infertility (27). This dose was exceeded for radioimmunotherapy with 177Lu-cG250, but the fertility status of men in this study was not investigated. However, in dosimetry, the testis dose is primarily derived from the blood-pool activity in and around the organ and not from the organ itself, possibly leading to an overestimation of the testis dose.
To accurately estimate the tumor-absorbed dose, the tumor-specific volume and background-correction factor were determined by CT. The total tumor dose varied widely from 0.47 to 17.3 mGy/MBq, mainly because of differences in uptake of the radiolabeled antibody in the lesions. In 17 of the 40 tumors, 177Lu-cG250 activity was highest at the last scintigraphic acquisition, indicating that there is a slow accumulation of radiolabeled cG250 during 5–7 d. Because there were no scintigraphic data available beyond 5–7 d after injection, the tumor-absorbed dose might be slightly underestimated if only physical decay is considered. Conversely, an overestimation of the tumor dose could have occurred because of biologic clearance of the radiolabel after the last imaging time point. As described in several other studies (9,11,28), an inverse relationship between tumor dose and tumor mass was observed in this study. Tumor doses exceeding 50 Gy are considered to be required to achieve a therapeutic response in these patients (29). In this study, only 2 of 40 tumor lesions received a tumor dose of greater than 50 Gy during the first treatment cycle. Twelve of 40 tumors received a tumor dose greater than 25 Gy during the first cycle, suggesting that for these tumors a tumor-sterilizing dose can be reached during subsequent treatment cycles.
Diagnostic 111In-cG250 data were used to predict therapeutic absorbed doses by correcting scintigrams and blood activity data for the physical decay difference between the radionuclides. The simulated absorbed doses were compared with the measured absorbed doses for 177Lu-cG250. There was no significant difference between the mean absorbed doses for the simulated and measured 177Lu-cG250 data. In addition, the simulated absorbed dose correlated significantly with the absorbed dose after radioimmunotherapy for the whole body, liver, heart wall, red marrow, lungs, testes, and tumor lesions (r = 0.818–0.982, P < 0.001). The calculated kidney-absorbed dose for 177Lu-cG250 in comparison to the simulated data based on the 111In-cG250 data did not correlate, because of the high and time-dependent activity in the colon, overlapping the kidney region. In this study, it was shown that simulations, based on diagnostic data, can be used not only to predict the absorbed doses but also to predict myelotoxicity, because the simulated whole-body and red marrow–absorbed dose correlated significantly with thrombocyte and leukocyte toxicity. These results provide tools for treatment planning, because a toxicity risk assessment can be made before radioimmunotherapy.
Another suitable radionuclide for radioimmunotherapy with cG250 is 90Y (30). An advantage of 90Y is the long range of the β-emissions, which could overcome the intratumoral heterogeneity of the antibody uptake. A disadvantage is the inability to reliably image the 90Y activity distribution, because of the absence of γ-emissions. We showed that the 111In-cG250 scintigrams and pharmacokinetic data could be used to accurately estimate the radiation doses after radioimmunotherapy with 177Lu-cG250. Therefore, it was assumed that 90Y-cG250 absorbed doses can also be predicted using the 111In-cG250 data. The calculated absorbed doses (mGy/MBq) for 90Y-cG250 were approximately 2–3 times higher than for 177Lu-cG250—in the same range as described by Vallabhajosula et al. (10), who reported a 3-times higher bone marrow dose for radioimmunotherapy with 90Y-J591 than with 177Lu-J591. Considering the ratio of blood-based red marrow dose between 177Lu and simulated 90Y found in the present study and assuming this is the main determinant of MTD, the anticipated MTD of 90Y-cG250 radioimmunotherapy would be around 25–28 MBq/kg, which is substantially lower than that of 177Lu-cG50. However, because myelotoxicity from 90Y radioimmunotherapy cannot be predicted by the blood-based red marrow dose (10), a clinical trial is warranted to investigate the MTD and tumor doses of 90Y-cG250 radioimmunotherapy in metastasized RCC patients. A more relevant parameter to compare tumor doses of 90Y and 177Lu-cG250 is the ratio between the tumor and red marrow dose, rather than the absolute doses to the tumor and the red marrow. The tumor–to–red marrow dose ratio was higher for (simulated) 177Lu-cG250 than for 90Y-cG250. The tumor-absorbed dose depends on the accumulation of radioactive cG250. Because of the slow accumulation of cG250 in the metastases and the longer half-life of 177Lu than of 90Y, the radiation dose that can be guided to the tumor lesions is anticipated to be higher for radioimmunotherapy with 177Lu-cG250.
CONCLUSION
In patients with RCC, hematologic toxicity, especially thrombocyte toxicity, after radioimmunotherapy with 177Lu-cG250 can be predicted on the basis of administered activity and whole-body and red marrow doses. Diagnostic 111In-cG250 data can be used to predict absorbed doses for radioimmunotherapy with 177Lu-cG250 and 90Y-cG250. In these patients, treatment with 177Lu-cG250 provides a higher tumor–to–red marrow dose ratio than treatment with 90Y-cG250.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank all nuclear medicine technicians of the Nuclear Medicine Department of the Radboud University Nijmegen Medical Centre for the excellent acquisition, storage, and handling of the scintigrams used in this study. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Dec. 12, 2011.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication June 24, 2011.
- Accepted for publication September 7, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}