


Abstract
Previous studies demonstrated that chemotherapy-induced changes in tumor glucose metabolism measured with 18F-FDG PET identify patients who benefit from preoperative chemotherapy and those who do not. The prognosis for chemotherapy metabolic nonresponders is poorer than for metabolic responders. Therefore, we initiated this prospective trial to improve the clinical outcome of metabolic nonresponders using a salvage neoadjuvant radiochemotherapy. Methods: Fifty-six patients with locally advanced adenocarcinomas of the esophagogastric junction were included. Tumor glucose uptake was assessed by 18F-FDG PET before chemotherapy and 14 d after initiation of chemotherapy. PET nonresponders received salvage neoadjuvant radiochemotherapy, whereas metabolic responders received neoadjuvant chemotherapy for 3 mo before surgery. Results: Thirty-three patients were metabolic responders, and 23 were nonresponders. Resection was performed on 54 patients. R0 resection rate was 82% (95% confidence interval [CI], 66%–91%) in metabolic responders and 70% (95% CI, 49%–84%) in metabolic nonresponders (P = 0.51). Major histologic remissions were observed in 12 metabolic responders (36%; 95% CI, 22%–53%) and 6 nonresponders (26%; 95% CI, 13%–46%). One-year progression-free rate was 74% ± 8% in PET responders and 57% ± 10% in metabolic nonresponders (log rank test, P = 0.035). One-year overall survival was comparable between the groups (∼80%), and 2-y overall survival was estimated to be 71% ± 8% in metabolic responders and 42% ± 11% in PET nonresponders (hazard ratio, 1.9; 95% CI, 0.87–4.24; P = 0.10). Conclusion: This prospective study showed the feasibility of a PET-guided treatment algorithm. However, by comparing the groups of nonresponding patients in the current trial and the previous published MUNICON (Metabolic response evalUatioN for Individualisation of neoadjuvant Chemotherapy in Esophageal and esophagogastric adeNocarcinoma) I trial, increased histopathologic response was observed after salvage radiochemotherapy, but the primary endpoint of the study to increase the R0 resection rate was not met. The prognosis of the subgroup of PET nonresponders remains poor, indicating their different tumor biology.
Patients with locally advanced adenocarcinomas of the esophagus or esophagogastric junction (AEG) are frequently offered preoperative treatment using chemotherapy alone or radiochemotherapy (1–4). One rationale for giving neoadjuvant treatment is preoperative downsizing of the tumor resulting in higher R0 resection rates. Indeed, several randomized trials showed significantly higher R0 resection rates after neoadjuvant chemotherapy than with surgery alone (1,5,6), and overall survival (OS) was significantly increased by the use of preoperative therapy (3–5). Therefore, neoadjuvant treatment is now widely accepted as a standard of care for locally advanced disease, but there is still debate whether radiochemotherapy or chemotherapy should be the preferred approach for patients presenting with locally advanced adenocarcinomas of the AEG (7).
Neoadjuvant chemotherapy is only beneficial in a subgroup of patients (8). A maximum of 40%–50% of the patients respond to standard chemotherapy or radiochemotherapy regimens (9,10). Because patients who do not respond to chemotherapy may be compromised by toxic side effects and the delay caused by an ineffective therapy, it is desirable to have a diagnostic test for early prediction of nonresponse in order to individualize—that is, change the treatment regimen—in these patients. Unfortunately, so far no robust pretherapeutically available molecular marker predicting response or prognosis is available for esophageal and gastroesophageal cancer (11).
18F-FDG PET/CT has shown promising results in assessing early therapy response and tumor control as well as prognosis in AEG (12,13). Recently, our group presented the results of the MUNICON (Metabolic response evalUatioN for Individualisation of neoadjuvant Chemotherapy in Esophageal and esophagogastric adeNocarcinoma) trial (14). In this prospective, nonrandomized clinical trial, patients without metabolic response in PET performed 2 wk after the start of induction chemotherapy were taken off chemotherapy and underwent early tumor resection. In contrast, patients demonstrating a metabolic response received a full course (up to 12 wk) of preoperative chemotherapy. Even though the OS of metabolic nonresponders was significantly lower than that of PET responders, it was still higher than that of a historical control undergoing 3 mo of ineffective chemotherapy (12). To explore this further, we initiated the MUNICON II trial, in which we investigated whether early PET nonresponders can benefit from a preoperative salvage neoadjuvant radiochemotherapy. For this purpose we assessed R0 resection rate, histopathologic response, event-free survival, and OS and compared the parameters with ones from metabolic responders who continued chemotherapy before surgery.
MATERIALS AND METHODS
Patient Characteristics
Inclusion criteria in this study were identical to the previously published MUNICON I trial (14), in which patients with locally advanced AEG type I (distal esophageal adenocarcinoma) or type II (gastric cardia cancer) according to classification of Siewert and Stein were selected (15). Eligibility criteria comprised cT3/4 staging based on CT and endoscopic ultrasound, exclusion of distant metastases by PET, no known medical contraindications against chemotherapy with platinum plus 5-fluorouracil, or unacceptable risks for esophagectomy, as indicated by the score of Bartels et al. (16). Indication of therapy was discussed in a multidisciplinary tumor board in all patients. None of the patients had been included in the previously published studies. All participants were at least 18 y or older and provided written informed consent.
Study Design
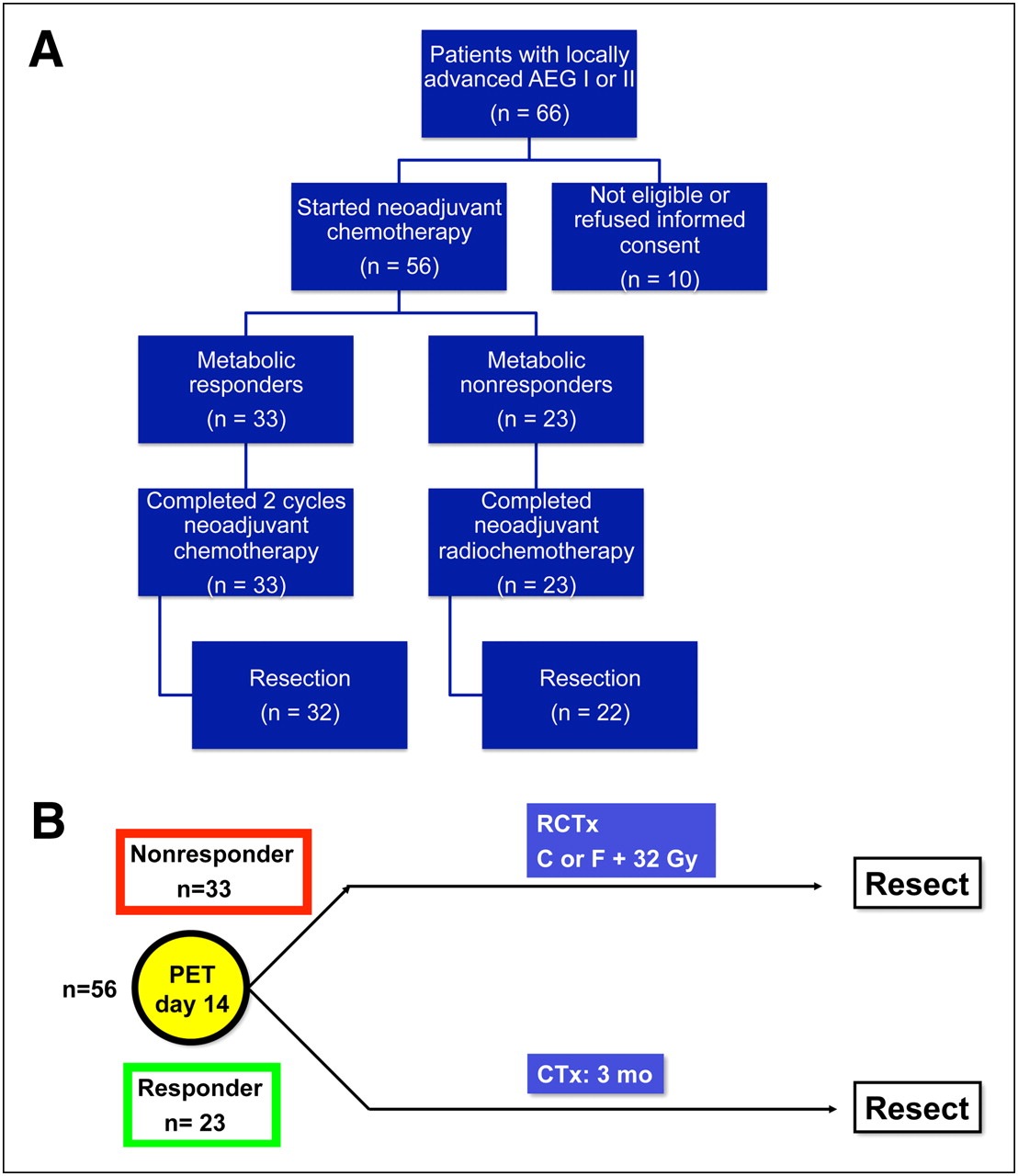
The MUNICON II trial was initiated as a single-center prospective nonrandomized exploratory phase II study. The protocol was approved by the local ethics committee. The study was assigned the number 2005-0041-23-19 in the European Clinical Trials Database (EudraCT) and sponsored by the Klinikum rechts der Isar, Technische Universität München. Figure 1A displays the trial design.

Trial profile and study design of MUNICON trial. C = cisplatin; F = 5-fluorouracil; CTx = chemotherapy; RCTx = radiochemotherapy.
According to the study protocol, metabolic response was assessed by 18F-FDG PET scans before and 2 wk after the start of chemotherapy. Metabolic responders (defined by a mean standarized uptake value [SUV] decrease of 35% or more, as previously reported (13,14)) continued chemotherapy for a maximum of 12 wk before undergoing surgery, whereas metabolic nonresponders (<35% mean SUV decrease) discontinued chemotherapy and proceeded to radiochemotherapy followed by surgery (Fig. 1B).
Specific Procedures
PET/CT.
Patients underwent 18F-FDG PET/CT scans 60 min after injection of approximately 370 MBq of 18F-FDG on a Sensation 16 Biograph PET/CT scanner (Siemens). A standardized 18F-FDG PET/CT protocol was used, including 6 h of fasting, blood glucose levels less than 150 mg/dL, diluted oral contrast (Telebrix, 300 mg; Guerbet), and low-dose CT (26 mAs, 120 kV, 0.5 s per rotation, 5-mm slice thickness) from the base of the skull to mid thigh for attenuation correction. Semiquantitative analysis of the PET/CT studies was performed by our standard method (14,17) using a circular region of interest (ROI) (diameter, 1.5 cm) with the TrueD software (Siemens Medical Solutions) and was normalized for injected dose and patients’ body weight. Compared with the MUNICON I trial, all patients underwent PET on a combined PET/CT scanner. The almost simultaneous coregistered data acquisition allows a better localization and characterization of malignant lesions because of the additional anatomic information generated by the CT component. As previously shown by Souvatzoglou et al., SUVs of cancer lesions and normal organs are comparable between PET and PET/CT (18).
The mean activity administered at PET 1 was 447 MBq of 18F-FDG (median, 448 MBq; range, 341–547 MBq) and 406 MBq of 18F-FDG at PET 2 (median, 421 MBq; range, 282–535 MBq).
The mean time interval between 18F-FDG injection and start of the emission scan was 63 min at PET 1 (median, 61 min; range, 55–100 min) and 63 min at PET 2 (median, 55–77 min). The mean difference within 1 patient was 7 min (median, 5 min; range, 0–42 min). In the patient with a time difference of 42 min, the PET scanner had to be restarted, causing the time delay. The second highest time differences were 22, 20, and 15 min.
The mean blood glucose level was 99 mg/dL at PET 1 (median, 96 mg/dL; range, 67–148 mg/dL) and 100 mg/dL at PET 2 (median, 95 mg/dL; range, 67–148 mg/dL). As no patient presented a blood glucose level above 150 mg/dL, no patient had to be excluded. However, in 1 patient the initially scheduled PET/CT was rescheduled a day later because the blood glucose level was above 150 mg/dL at the first presentation.
Chemotherapy.
All patients started with 2 wk of neoadjuvant chemotherapy. The mean time interval between baseline PET/CT and start of chemotherapy was 6 d (median, 5 d; range, 1–34 d). The mean time interval between start of chemotherapy and second 18F-FDG PET/CT scan was 13 d (median, 13 d; range, 11–19 d). Metabolic responders continued this neoadjuvant chemotherapy for a maximum of 2 cycles. Chemotherapy consisted of cisplatin (Medac GmbH) (50 mg/m2) given on days 1, 15, and 29 (1-h infusion time) plus folinic acid (Medac GmbH) (500 mg/m2 over 2 h) and 5-fluorouracil (Hexal AG) (2,000 mg/m2 over 24 h) on days 1, 8, 15, 22, 29, and 36, repeated on day 49. In 10 patients with a glomerular filtration rate less than 60 mL/kg/min, cisplatin was replaced by oxaliplatin (Sanofi-Aventis Group) (85 mg/m2 over 2 h). In 8 patients younger than 60 y with a good health status, paclitaxel (Bristol Myers Squibb) (80 mg/m2 over 3 h) was given additionally on days 0, 14, and 28. Adverse events were documented according to the National Cancer Institute Criteria, version 3.0.
Radiochemotherapy.
After 2 wk of neoadjuvant chemotherapy, metabolic nonresponders started concurrent radiochemotherapy. Concurrent chemotherapy consisted of cisplatin (6 mg/m2 on days 1–5 and 8–12, 1-h infusion), or 5-fluorouracil (250 mg/m2, continuous infusion) if renal function did not allow cisplatin therapy. Radiation therapy was performed with photons from a linear accelerator with an energy of 6 MeV or greater. All patients received 3-dimensional conformal treatment planning. The planning target volume comprised the macroscopic tumor as visible on the CT and PET scans with a safety margin of 1.0–1.3 cm. The safety margin in the craniocaudal direction along the esophagus was 4–5 cm, to account for submucosal spread. A total dose of 32 Gy was applied at 1.6 Gy/fraction twice daily, 10 fractions/wk with a minimum interval of 6 h between the 2 daily fractions. The dose was prescribed to a reference point within the planning target volume according to International Commission on Radiation Units and Measurements 50.
Restaging.
Restaging comprising endoscopy and CT was performed before and after the second cycle of chemotherapy.
Surgery.
Abdominothoracic esophagectomy was performed in patients with AEG I tumors (19). Transhiatal extended gastrectomy was performed in patients with AEG II, with intraoperative frozen sections proving a proximal tumor-free resection margin. Otherwise, an abdominothoracic esophagectomy Ivor–Lewis procedure was performed in AEG II tumors. Surgery was conducted within 4–6 wk after the last administration of chemotherapy or chemoradiotherapy.
Pathology.
Histopathologic response and tumor regression were assessed according to a previously published scoring system (20), differentiating between histopathologic responders (≤10% residual tumor) and histopathologic nonresponders (≥10% residual tumor). Involvement of the oral, aboral, and circumferential resection margins was specified according to previously published criteria (21) by 2 pathologists.
Follow-up.
Patients were followed exactly as they were in the MUNICON I trial, including CT and endoscopy at 3-mo intervals during the first year after surgery. Thereafter, follow-up was performed at 6-mo intervals. Survival was calculated from the day of the second PET/CT scan. Event-free survival was calculated up to the time of death or relapse, whichever occurred first.
Statistics.
According to the study protocol, R0 resection rate was the primary endpoint. On the basis of the results of MUNICON I, an improvement of R0 resection rate in metabolic nonresponders from 74% to 94% in MUNICON II was assumed. Therefore, a total of 23 PET nonresponders had to be included to detect this clinically relevant effect size at an α-error level of 0.05 (1-sided) with a power of 0.80. Secondary endpoints were OS, time to progression (TTP), postoperative complications and mortality, and histopathologic remission.
Differences in frequencies were analyzed using Fisher exact tests. Confidence intervals (CIs) for proportions were calculated according to the Wilson test. Survival probabilities (±SE) were estimated and illustrated according to Kaplan–Meier. Statistical comparisons between different groups of patients were performed with a log-rank test, and hazard ratios were calculated using the Cox proportional hazards model. All tests were 2-sided and performed at the 5% level of significance using PASW Statistics (version 18.0; SPSS Inc.).
RESULTS
Patients
From September 28, 2005, until November 28, 2008, 66 patients were screened. After assessment of eligibility, 10 patients proved ineligible or refused informed consent. Thus, 56 patients (5 women and 51 men) were treated in the study (Fig. 1A). The median age was 62 y (range, 35–77 y). Thirty-nine patients (70%) had AEG type I and 17 patients (30%) had type II. Eastern Cooperative Oncology Group performance status was 0 in 77% of the patients and 1 in 23%. The clinical stage as determined by endoscopic ultrasound was uT3 in 54 patients (94%). All patients presented with clinical signs of lymph node involvement (Table 1).
Baseline Characteristics of Patients Evaluated with 18F-FDG PET for Metabolic Response to Neoadjuvant Chemotherapy
Chemotherapy
Thirty-eight patients (68%) were treated with cisplatin, folinic acid, and 5-fluorouracil; 8 (14%) received additional paclitaxel; and 10 (18%) received oxaliplatin, folinic acid, and 5-fluorouracil. For the 56 evaluable patients, cisplatin, folinic acid, and 5-fluorouracil were given to 23 responders and 15 nonresponders; oxaliplatin, folinic acid, and 5-fluorouracil were administered in 7 responders and 3 nonresponders; and paclitaxel, cisplatin, folinic acid, and 5-fluorouracil were given to 3 responders and 5 nonresponders. Frequent grade 3/4 adverse events in 56 treated patients were as follows: dysphagia, 11%; diarrhea, 9%; emesis, 2%; and nausea, 2%.
Radiochemotherapy
Twenty-three PET nonresponders were referred to radiochemotherapy and received the total dose of 32 Gy and chemotherapy with cisplatin or 5-fluorouracil. Dysphagia was observed in 9% and nausea in 4%.
Metabolic Response
After 2 wk of chemotherapy, metabolic response was assessed in 56 patients: 33 (59%; 95% CI, 46%–71%) were metabolic responders and 23 (41%; 95% CI, 29%–54%) metabolic nonresponders. There were no statistically significant differences in baseline characteristics of metabolic responders versus nonresponders with regard to age, sex, performance status, tumor localization, T and N category, or histologic subtype according to Laurén (Table 1). Metabolic response rates for patients in the different chemotherapy regimens were not significantly different (Table 2).
Metabolic Response Rates with Different Chemotherapy Regimens in 56 Evaluable Patients
Surgery
Fifty-four of 56 patients (96%) underwent surgical resection: esophagectomy in 49 (90%) and transhiatal extended gastrectomy in 5 (10%, all AEG II) patients. Because of tumor progression, 2 patients did not undergo resection (1 in each arm).
Of the 54 resected patients, 43 patients (80%) had tumor-free resection margins (R0 resection). R0 resection (complete resection with no microscopic residual tumor) was achieved in 27 PET responders (82%; 95% CI, 66%–91%) and 16 PET nonresponders (70%; 95% CI, 49%–84%; P = 0.51) (Table 3). Because of this lower than expected R0 resection rate in PET nonresponders, which did not exceed the presumed lower limit of interest of 74%, the 1-sided primary study endpoint was not met.
Surgical Outcome After Neoadjuvant Chemotherapy (Responders) and Neoadjuvant Radiochemotherapy (Nonresponders)
The postoperative mortality rate (30-d and in-hospital mortality) was 2% (1/54 patients; 95% CI, 0.01%–10%). Postoperative complications including nonsurgical morbidity were reported in 61% (20 patients; 95% CI, 44%–75%) of PET responders and in 70% (16 patients; 95% CI, 49%–84%) of PET nonresponders, with no statistical difference for metabolic responders versus nonresponders (P = 0.68) (Table 3).
Pathology
In the group of metabolic responders, 12 patients (36%; 95% CI, 22%–53%) achieved a major histopathologic response (<10% residual tumor), whereas in the PET nonresponders, 6 patients (26%; 95% CI, 13%–46%) demonstrated a histopathologic response after radiochemotherapy (Table 4). This difference was not statistically significant (P = 0.51). In the group of histopathologic responders, the SUV decrease was not statistically different in patients achieving complete histologic response (median decrease, 46%; interquartile range, 30%–56%, n = 5), compared with those with subtotal histologic remission (median decrease, 37%; interquartile range, 21%–52%; n = 13; P = 0.294).
Histopathologic Outcome After Neoadjuvant Chemotherapy (Responders) and Neoadjuvant Radiochemotherapy (Nonresponders)
Survival and TTP
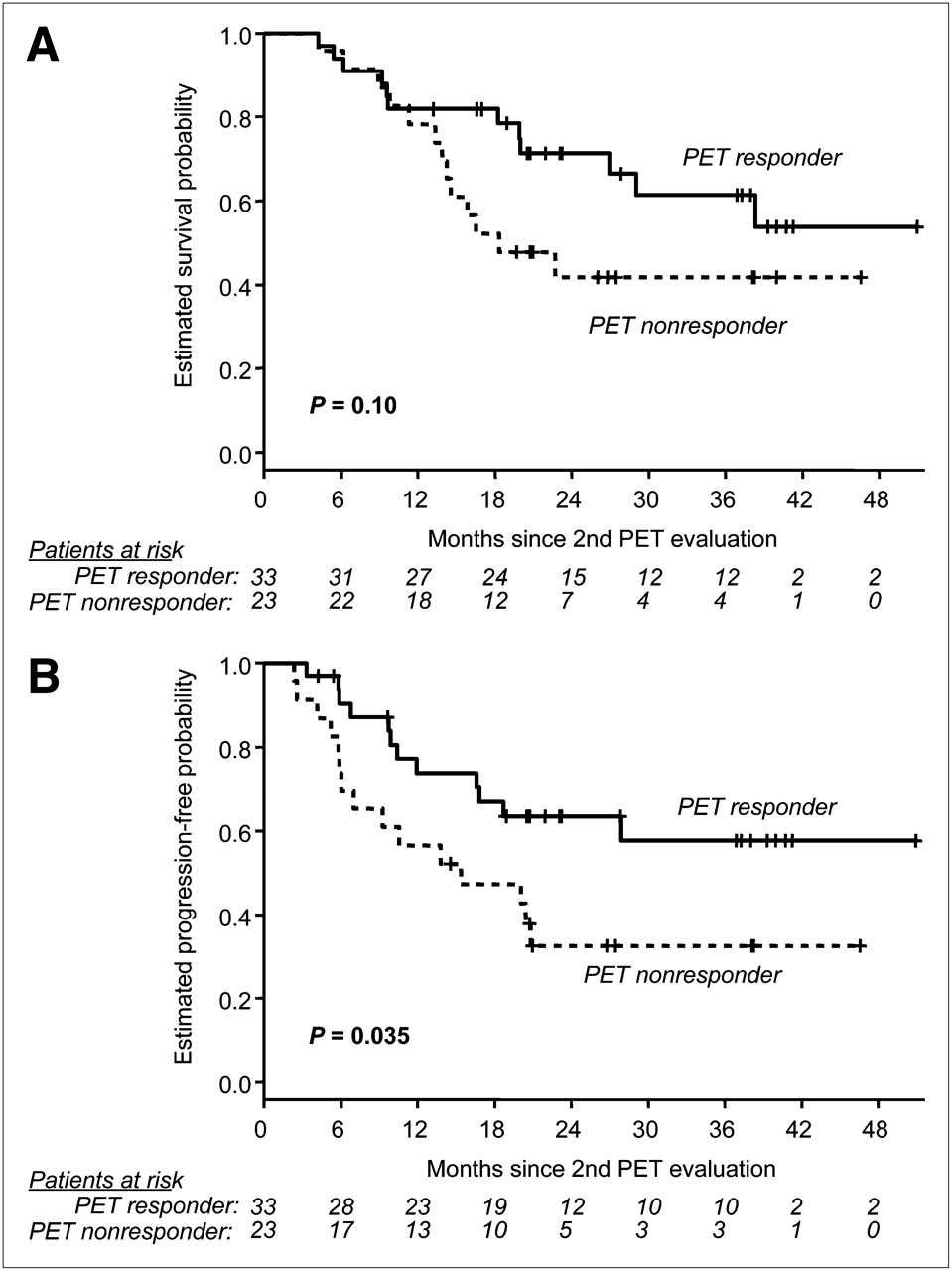
The median follow-up time was 38 mo (range, 14–54 mo). During this time, 25 patients died (12 responders and 13 nonresponders). The median OS was 38.3 mo for the whole study population and 18.3 mo for the group of PET nonresponders. For PET responders, median OS has not been reached. One-year OS was comparable between the groups (∼80%), and 2-y OS was estimated to be 71% ± 8% in metabolic responders and 42% ± 11% in PET nonresponders (hazard ratio, 1.9; 95% CI, 0.87–4.24; P = 0.10) (Fig. 2A).

(A) OS in 56 patients assessed with PET for early metabolic response. (B) TTP in 56 patients assessed with PET for early metabolic response.
The median time to progression was 28 mo for the whole study population and 15.4 mo for the group of PET nonresponders. For PET responders, TTP has not been reached. One-year progression-free rate was 74% ± 8% in PET responders and 57% ± 10% in metabolic nonresponders. The corresponding 2-y progression-free proportion was estimated to be 64% ± 9% for PET responders and 33% ± 10% for PET nonresponders (hazard ratio, 2.22; 95% CI, 1.04–4.77; P = 0.035) (Fig. 2B).
Relapse
Thirty-nine percent of PET responders and 65% of PET nonresponders displayed relapse of disease (P = 0.10). Interestingly, in 30% of the patients with PET-responding disease this relapse was due to distant metastases whereas 48% of PET-nonresponding patients had distant metastases (P = 0.102) (Table 5).
Relapse After Neoadjuvant Chemotherapy (Responders) and Neoadjuvant Radiochemotherapy (Nonresponders)
DISCUSSION
In the MUNICON II prospective clinical trial, neoadjuvant chemotherapy was switched to neoadjuvant radiochemotherapy in metabolic nonresponding patients to improve the histopathologic response, R0 resection rate, and prognosis of patients with gastroesophageal cancer. However, although histopathologic response was observed, the primary endpoint of the study to increase the R0 resection rate was not met. Because the survival in metabolic responders (the subgroup of patients who received the same therapy in the MUNICON I and MUNICON II trials) was almost identical to the survival in the previously published MUNICON I trial, the MUNICON II trial confirms the feasibility of an early evaluation and a response-guided treatment algorithm with PET in patients with locally advanced AEG I and II.
To draw definitive conclusions, it needs to be further explored in a randomized, controlled trial whether salvage radiochemotherapy, compared with other treatment strategies in metabolically nonresponding patients, has any positive impact on outcome. To answer this question, a multicenter setting would be necessary. An international multicenter trial investigating this particular question is under way (22). Our current study was clearly a hypothesis-generating trial, and we were trying to determine whether salvage radiochemotherapy could change the clinical course of patients receiving neoadjuvant chemotherapy who did not achieve a response. A strength of this trial—and previous studies from our group—is the homogeneity of the study population with regard to histology, tumor localization, T and N stages, and type of surgery; all patients underwent standardized staging procedures and were seen by a multidisciplinary treatment team before the start of treatment. This strength is reflected by the fact that the median TTP and OS did not differ significantly across the trials. Table 6 summarizes the major findings of the MUNICON I and MUNICON II trials. Nevertheless, conclusions from historic comparisons must be drawn with caution and prospective randomized clinical trials are urgently necessary to investigate the promising results obtained in a single-center study.
Comparison of Major Findings of MUNICON I and MUNICON II Trials
As in our previous trials, tumors were assessed by a single-slice ROI. Indeed, there is debate whether single-slice ROI is the most accurate way to analyze tumor response (23). On the other hand, we recently compared different SUV-based methods for response prediction to neoadjuvant radiochemotherapy in locally advanced rectal cancer. Of note, despite the different characteristics of the ROI methods, early and late changes in SUV measured were similar regardless of the method used (24). Most importantly, our threshold and the method that we used to measure response in the present study were established and validated prospectively in previous trials. Therefore, we decided to keep this established and validated method to measure response by single-slice ROI in the MUNICON II trial.
18F-FDG PET has shown promising results in assessing response to therapy and local tumor control and in prognosis (25–30). However, most of these studies investigated late response assessment after 6 or more weeks of chemotherapy and radiochemotherapy. Recently Kim et al. indicated a relatively strong concordance of 71% between histopathologic complete response and metabolic complete response (31). However, the main drawback of late response assessment is that it does not allow the therapy to be modified for patients. This is in contrast to early PET response evaluation, in which PET-nonresponding patients can be offered a different, more effective therapeutic strategy. In the present study, a salvage radiochemotherapy was offered to patients not responding to chemotherapy.
Even though radiation dose was relatively low and no new radiosensitizers were applied, in the current MUNICON II trial 26% of initial metabolic nonresponders during chemotherapy had a major histopathologic response after radiochemotherapy, whereas almost no histopathologic response after radiochemotherapy was observed in PET nonresponders continuing with chemotherapy in previous trials. Thus, the chosen radiochemotherapy regimen was active enough to induce tumor cell kill in a subset of patients. Nonetheless, whereas only 9% of the PET responders undergoing chemotherapy without radiation had a local recurrence, 17% of the PET nonresponders undergoing radiochemotherapy had local treatment failure. Even more pronounced is the observation that almost 50% of the PET nonresponders had progressive disease shortly after radiochemotherapy because of distant metastases, indicating the unfavorable tumor biology that could not be reversed by radiation plus a relatively smooth concurrent chemotherapy. One reason for choosing this moderate-intensity radiochemotherapy schedule was the awareness that more aggressive regimens inevitably result in higher toxicity, lead to a higher preoperative drop-out rate, and are associated with a higher postoperative morbidity and mortality (32,33). In addition to higher response rates, greater histopathologic response has been shown to be induced by neoadjuvant radiochemotherapy than by chemotherapy alone in the phase III PreOperative Chemotherapy or Radiochemotherapy in Esophago-gastric Adenocarcinoma Trial (34). However, this trial and a recent meta-analysis did not show a statistically significant survival benefit for radiochemotherapy compared with chemotherapy alone (4).
Complete tumor resection is an accepted prognostic factor in primary surgery of esophageal cancer (19,35). The prognostic significance of a histopathologic response is less clearly defined, although some studies demonstrated a significant correlation with survival (36,37). On the basis of the fact that radiochemotherapy results in higher histopathologic response rates, we hypothesized that salvage radiochemotherapy in chemotherapy PET nonresponders may increase the number of patients with histopathologic major remissions as well as possibly lead to a higher rate of R0 resections. This is the reason why we chose the R0 resection rate as the primary endpoint of this study. However, neoadjuvant radiochemotherapy was not able to increase the R0 resection rate in the present study, although major histopathologic remission after radiochemotherapy was observed in 6 patients (16%).
CONCLUSION
Salvage neoadjuvant radiochemotherapy in metabolic nonresponders leads to local remissions in a considerable number of patients but was not able to change the clinical course in general because of the systemic disease. Future investigations could address whether the prognosis can be improved by adding other systemically active drugs.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We gratefully acknowledge the assistance provided by the PET technologists and chemists and by the personnel of the Munich Center for Clinical Studies. This work was supported by the German Research Foundation (DFG) within the SFB Initiative 824 (collaborative research center) “Imaging for Selection, Monitoring and Individualization of Cancer Therapies” (SFB824, project B1). No other potential conflict of interest relevant to this article was reported.
Footnotes
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication November 23, 2010.
- Accepted for publication May 6, 2011.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Advances in diagnosis and management of cancer of the esophagus
- Histology-based Prediction of Therapy Response to Neoadjuvant Chemotherapy for Esophageal and Esophagogastric Junction Adenocarcinomas Using Deep Learning
- Effect of Pathologic Tumor Response and Nodal Status on Survival in the Medical Research Council Adjuvant Gastric Infusional Chemotherapy Trial
- Standardized Uptake Decrease on [18F]-Fluorodeoxyglucose Positron Emission Tomography After Neoadjuvant Chemotherapy Is a Prognostic Classifier for Long-Term Outcome After Multimodality Treatment: Secondary Analysis of a Randomized Trial for Resectable Stage IIIA/B Non-Small-Cell Lung Cancer
- Predictive Value of Positron Emission Tomography/Computed Tomography to Assess Early Treatment Response to Dual Human Epidermal Growth Factor Receptor 2 (HER2) Blockade Without Chemotherapy for HER2-Positive Metastatic Breast Cancer: Are We Ready to Embrace This "Early Metabolic Look" Strategy?
- 18F-FLT PET Evaluation of Radiation Response
- Value of Functional Imaging by PET in Esophageal Cancer
- Locally Advanced Gastroesophageal Junction Tumor: A Treatment Dilemma
- Measuring Tumor Metabolism by 18F-FDG PET Predicts Outcome in a Multicenter Study: A Step Off in the Right Direction
- Critical Appraisal of Locoregional Failure and Systemic Disease Progression After Preoperative Chemoradiation of Esophageal Adenocarcinoma