


Abstract
New antitumor agents have resulted in significant survival benefits for cancer patients. However, several agents may have serious cardiovascular side effects. Left ventricular ejection fraction measurement by 99mTc multigated radionuclide angiography is regarded as the gold standard to measure cardiotoxicity in adult patients. It identifies left ventricular dysfunction with high reproducibility and low interobserver variability. A decrease in left ventricular ejection fraction, however, is a relatively late manifestation of myocardial damage. Nuclear cardiologic techniques that visualize pathophysiologic processes at the tissue level could detect myocardial injury at an earlier stage. These techniques may give the opportunity for timely intervention to prevent further damage and could provide insights into the mechanisms and pathophysiology of cardiotoxicity caused by anticancer agents. This review provides an overview of past, current, and promising newly developed radiopharmaceuticals and describes the role and recent advances of scintigraphic techniques to measure cardiotoxicity. Both first-order functional imaging techniques (visualizing mechanical [pump] function), such as 99mTc multigated radionuclide angiography and 99mTc gated blood-pool SPECT, and third-order functional imaging techniques (visualizing pathophysiologic and neurophysiologic processes at the tissue level) are discussed. Third-order functional imaging techniques comprise 123I-metaiodobenzylguanidine scintigraphy, which images the efferent sympathetic nervous innervations; sympathetic neuronal PET, with its wide range of tracers; 111In-antimyosin, which is a specific marker for myocardial cell injury and necrosis; 99mTc-annexin V scintigraphy, which visualizes apoptosis and cell death; fatty-acid-use scintigraphy, which visualizes the storage of free fatty acids in the lipid pool of the cytosol (which can be impaired by cardiotoxic agents); and 111In-trastuzumab imaging, to study trastuzumab targeting to the myocardium. To define the prognostic importance and clinical value of each of these functional imaging techniques, prospective clinical trials are warranted.
The development of new antitumor agents, especially molecular targeting agents, has significantly improved the treatment options for cancer patients in the past decade. Although these advances have prolonged survival, several agents may have serious cardiovascular side effects. Trastuzumab (Herceptin; Genentech), a humanized monoclonal antibody against human epidermal growth factor receptor type 2 (HER2), is one such agent that is new and successful but has been associated with cardiac dysfunction (1). In a recent analysis of the incidence of cardiac adverse events in patients with early breast cancer who were treated with trastuzumab in an adjuvant setting (Herceptin Adjuvant Trial), trastuzumab was discontinued because of cardiac disorders in approximately 5% of patients. At a median follow-up of 3.6 y, the incidence of cardiac endpoints (severe congestive heart failure, significant left ventricular ejection fraction [LVEF] decrease) was higher in the trastuzumab group than in the observation group (2). Preliminary analysis from randomized controlled trials and case control studies showed a pooled incidence of cardiotoxicity of 10% in trastuzumab-containing arms, whereas the pooled incidence of cardiotoxicity in studies using a nontrastuzumab comparative arm was 2% (3). Therefore, close monitoring of patients treated with trastuzumab is warranted.
Of the classic cytotoxic agents, anthracyclines are well known for their dose-dependent acute and chronic, irreversible and progressive cardiomyopathy. In trials of adjuvant anthracycline-based treatment for breast cancer, a 5-y incidence of chronic heart failure of up to 3.2% has been reported, depending on the type of combination regimen and on the cumulative dose of anthracycline (4). It has been suggested that the combination of anthracyclines and taxanes, which are currently the standard treatment for node-positive breast cancer, further increases cardiotoxicity (5,6). Furthermore, up to 0.5% of adults will be a survivor of some form of childhood cancer treated with anthracyclines (7). A large proportion of these survivors are at risk for developing cardiomyopathy, necessitating close follow-up evaluation and regular assessment.
Furthermore, patients may be treated with both anthracyclines and trastuzumab. It was recently demonstrated that patients treated with anthracyclines and cyclophosphamide, followed by trastuzumab and paclitaxel, showed a 3-y cumulative incidence of cardiac events, congestive heart failure, and cardiac death of 4.1%, compared with 0.8% in patients treated with anthracyclines and cyclophosphamide alone (8). Also, a recent meta-analysis of the National Surgical Adjuvant Breast and Bowel Project B-31 and North Central Cancer Treatment Group trials demonstrated that patients treated with trastuzumab in addition to sequential anthracycline-taxane had a 2.0% incidence of symptomatic heart failure events, compared with 0.45% in the chemotherapy-alone arm (9).
Both early- and late-onset cardiac effects of anticancer treatment are reported. Early-onset effects occur within 1 y of treatment and can be subacute or chronically progressive. Acute or subacute cardiotoxicity with anthracyclines occurs during or immediately after infusion, is usually self-limiting, and resolves when therapy is discontinued. Late-onset cardiotoxicity, however, occurs more frequently in children and can be noted more than 1 y after treatment (10). Also, cardiac abnormalities may start early and can progress over time to overt cardiomyopathy. Oeffinger et al. showed in a group of more than 10,000 survivors of childhood cancer that the risk of dying from cardiac disease was 8 times higher than in the healthy population (11). In a recent study by van der Pal et al., 27% of adult childhood cancer survivors had an abnormal cardiac function (12). The strongest predictors were anthracycline dose, cardiac irradiation, and younger age at diagnosis. At 6 y after anthracycline therapy, subclinical heart failure occurs in up to 65% of childhood cancer survivors (13). Besides trastuzumab and anthracyclines, several other anticancer agents may have cardiotoxic effects (Table 1) (14). Patients who have been treated with both cardiotoxic chemotherapy and radiotherapy that included the heart in the irradiated volume are especially prone to cumulative negative cardiovascular effects.
Cardiovascular Adverse Effects of Several Anticancer Agents
POTENTIAL MECHANISMS OF CARDIOTOXICITY
Characterization of the mechanism of trastuzumab- and anthracycline-induced cardiotoxicity may play an important role in developing strategies to prevent cardiac dysfunction. However, a clear understanding of the pathophysiology of cardiotoxicity is still lacking. This is particularly true for the pathophysiology of cardiac dysfunction associated with trastuzumab. Trastuzumab trials report a high incidence of fall in ejection fraction (8,15,16). The end of trastuzumab and start of treatment for heart failure often results in improvement of LVEF, although data on late-onset cardiomyopathy are still awaited (17). Targeting the ErbB2 receptor may not be cardiotoxic per se but, instead, could block some homeostatic pathways in the heart (18). It has been shown that the HER2-HER4-neuregulin system in the heart may attenuate the response of cardiomyocytes to oxidative stress and is temporarily upregulated in response to cardiomyocyte stress. Inhibition of HER2 causes mitochondrial dysfunction in cardiomyocytes (19–21). Therefore, trastuzumab-induced cardiotoxicity may be due to direct binding of trastuzumab to the HER2 receptor expressed on the myocardium (22), and increased oxidative stress (e.g., due to anthracycline use) increases the risk for trastuzumab-associated cardiotoxicity.
Trastuzumab-induced cardiac dysfunction seems to be different from anthracycline-induced cardiac dysfunction, leading to irreversible cardiac damage. Proposed mechanisms of anthracycline-induced cardiotoxicity include free radical–mediated myocardial injury, alteration in adrenergic function (which will be discussed in detail in the paragraph covering 123I-labeled metaiodobenzylguanidine [MIBG] scintigraphy), myocyte death from calcium overload, injury due to direct interaction with the actin–myosin contractile system (as exemplified in the paragraph on 111In-antimyosin imaging), interactions with histamine as a mediator, inhibition of protein synthesis, and formation of toxic doxorubicin metabolites and proinflammatory cytokines. Although the anticancer effects of anthracyclines are mediated through DNA damage, they also cause iron-based oxygen free radical–induced oxidative stress on cardiac muscle cells (14). Free radicals induce the peroxidation of myocyte membranes and subsequent influx of intracellular calcium (23). Increased cytoplasmic calcium can activate proteases, alter myocardial contractility, and induce myocyte death. Because the capacity of cardiomyocytes for mitosis is limited, loss of myocytes will result in a permanent reduction in myocyte numbers and thus an increased vulnerability to normal age-dependent cell loss and an increased risk for the development of clinically overt heart failure (24,25).
ROLE OF SURVEILLANCE AND EARLY DETECTION OF CARDIOTOXICITY
Preclinical studies are warranted to further unravel the different mechanisms of cardiotoxicity and provide tools for its early detection. The early identification of patients who are susceptible to cardiotoxicity may prevent morbidity and mortality (26–28). Because of the observed cardiac toxicity in the metastatic setting, for adjuvant phase III studies with trastuzumab, strict cardiac criteria have been developed and rigorous, though arbitrary, cardiac monitoring with early stopping rules have been incorporated. These rules and criteria have limited the incidence of the development of clinically overt heart failure and cardiac death but also posed the question of whether a potentially lifesaving anticancer treatment with trastuzumab was unnecessarily withheld in too large a percentage of patients (29). Therefore, reliable, noninvasive techniques are needed that can accurately predict clinically relevant treatment-induced heart failure, preferably when toxicity is still at a subclinical stage. This is especially important when alternative treatment strategies are available that can be used without compromising the outcome of cancer treatment. For example, sequential anthracycline-taxane–based chemotherapy incorporating trastuzumab may be replaced by the combination of docetaxel, carboplatin, and trastuzumab, which has similar efficacy (30). Also, potentially cardioprotective medication, for example, angiotensin blockers, may be started in the early phase to prevent deterioration of cardiac function (31,32). These new treatment options underscore the importance of surveillance and timely detection of any cardiac dysfunction during and after a potentially cardiotoxic cancer treatment.
NONINVASIVE IMAGING OF CARDIOTOXICITY
Over the years, several imaging modalities have been developed that vary considerably in precision, ease of use, availability, and costs. LVEF may be measured by planar multigated radionuclide angiography (MUGA), quantitative gated blood-pool SPECT (GBPS), 2- and 3-dimensional echocardiography, radiographic contrast angiography, or cardiac MRI. Of the currently clinically available methods, conventional echocardiography, electrocardiography, and tissue Doppler imaging lack the sensitivity required to detect the early stages of cardiomyopathy. The potential of newer echocardiographic methods, such as real-time 3-dimensional echocardiography, tissue Doppler imaging with myocardial strain, and strain rate imaging is, however, encouraging (33–36). Also, minimally invasive methods, such as measurement of blood and serum markers of endothelial damage and biochemical cardiac markers, are promising (33,37–44).
Together with echocardiography, MUGA is the most widely accepted method to assess patients’ LVEF during cancer treatment (45). Serial MUGA is the gold standard for assessing LVEF and is still regarded as the best noninvasive method for identifying subclinical left ventricular dysfunction in adult patients treated with cardiotoxic agents (45–47). Despite the portability, lack of radiation, and increased availability, 2-dimensional echocardiography is less sensitive for the detection of a decline in LVEF and has a poorer specificity and reproducibility and a higher interobserver- and intraindividual variability than MUGA (48,49). These shortfalls in 2-dimensional echocardiography are caused by constraints due to dependency on acoustic windows and variable operator skills. This technique suffers from gain-dependent edge identification and transducer positioning artifacts during imaging. The geometric assumptions are especially disadvantageous as these do not hold true when the left ventricle undergoes progressive dilatation in heart failure and when the left ventricle volume increases or becomes more spheric, with altered relationship between length and diameter. However, the interobserver variability for real-time 3-dimensional echocardiography, which provides volumetric measurements without geometric assumptions, is significantly lower than for 2-dimensional echocardiography (50). Whether this technique shows a reproducibility comparable to MUGA, however, still needs to be investigated by direct comparison of the limits of agreement of each technique in the same patients. Nevertheless, in most clinical protocols and guidelines, no clear preference for MUGA or ultrasound is given. In most institutions, MUGA is performed during rest; however, this test can also be performed during exercise. Theoretically, exercise MUGA should detect left ventricular dysfunction at an earlier stage than MUGA at rest, because heart failure starts with a compensatory mechanism—that is, an atrial contribution to left ventricular filling as a compensatory response to abnormal early left ventricular filling during exercise—to maintain the end-diastolic volume index (end-diastolic volume during exercise divided by end-diastolic volume at rest). If this compensatory mechanism fails, left ventricular dysfunction first manifests during exercise. However, conflicting results exist on the superior prognostic value of exercise MUGA, compared with MUGA at rest (51,52). Furthermore, because certain cancers and coronary heart disease have age and smoking as 2 common major risk factors, many of these patients undergo gated myocardial perfusion SPECT to rule out ischemic heart disease. In these scans, the LVEF is a routinely obtained byproduct. It is, however, less accurate than LVEF measurement obtained with MUGA, because it detects myocardial contours instead of quantitating cardiac blood pool and thus suffers from potential spillover effects from the myocardium in the left ventricular cavity and underestimation of either end-diastolic or systolic left ventricular volume. It has already been shown that these techniques are not interchangeable, because real-time 3-dimensional echocardiography slightly underestimates LVEF, compared with MUGA, although the correlation between the 2 modalities is strong (46,48). Tissue velocity imaging and speckle tracking radial strain are also relatively new techniques that require a learning curve and hands-on training, because a certain level of experience is essential (53). Strain data are sensitive to the placement of the region of interest and require higher-quality images than the routine optical interpretation (53,54). Mavinkurve et al. recently showed that myocardial strain and strain rate were significantly lower in survivors of childhood cancer than in healthy controls (55).
There are certain circumstances in which one technique is favored over the other. In pediatric patients, echocardiography is preferred because of the lack of ionizing radiation (56). In obese patients, however, adequate echocardiographic windows will be difficult to attain. Furthermore, the usefulness of echocardiography is limited in other variations of thoracic anatomy, such as emphysema, tight intercostal spaces, and heavily calcified ribs. Three-dimensional echocardiography is dependent on the patients’ ability to hold their breath and requires a longer offline analysis. MUGA is less feasible in patients with arrhythmias due to poor electrocardiography-based triggering, which is more often seen in patients with heart failure. Regrettably, the choice of technique used is often not determined by the question of which method is more accurate or more suitable for the individual patient but is rather governed by the availability of local resources and personal experience. Therefore, all the described noninvasive techniques should be used as complementary.
For a long time, nuclear cardiac imaging has played a pivotal role both in identifying patients at risk and in preventing and reducing cardiac injury resulting from cytotoxic agents. The following paragraphs concentrate on the role of several established and experimental scintigraphic techniques that may be of value in the early identification of patients who are at risk for cancer treatment–induced cardiomyopathy (Table 2).
Single-Photon Techniques for Early Detection of Cardiotoxicity
99MTC MUGA
The standard method to detect cardiotoxicity in the management of adult patients treated with cardiotoxic agents is serial ejection fraction measurement (10). MUGA, also called radionuclide ventriculography or equilibrium radionuclide angiocardiography, is a noninvasive technique that makes use of 99mTc-erythrocyte labeling, applying an in vivo, an in vitro, or a combined in vivo–in vitro approach, as described in detail in the guidelines for radionuclide imaging of cardiac function of the European Association of Nuclear Medicine and European Society of Cardiology (57). Each of the 3 approaches has its advantages and disadvantages, which should be noted, because optimal red blood cell labeling is a prerequisite to accurate LVEF calculation. In short, the labeling technique makes use of the binding of the radionuclide 99mTc to erythrocytes facilitated by stannous chloride, which dilutes the 99mTc and prevents it from leaking out of the red blood cells during the procedure. This technique enables the cardiac blood pool to be visualized with a γ-camera. As the γ-camera images are acquired, the simultaneously registered patient's heartbeat is used to gate the acquisition. Gating means that the heart cycle is split into 16 or 32 time bins based on the electrocardiography. Then, the image information obtained in every respective time bin of all heart actions is summarized to obtain a favorable image quality. The final result is a series of images of the heart, 1 at each stage of the cardiac cycle. Fourier analysis provides a functional image (a parametric map of sequential contractions, or phase imaging), which permits precise quantification of left ventricular volume and dyssynchrony, with high reproducibility. A major strength of this technique is that the quantitative computation of ejection fraction and chamber volumes does not depend on mathematic assumptions of ventricular geometry.
Both the final LVEF and magnitude of decrease are important determinants. Guidelines for monitoring cardiotoxicity by serial MUGA were based primarily on the work of Schwartz et al. (58), who had experience with nearly 1,500 patients over a 7-y period. Use of these guidelines resulted in a 4-fold reduction in the incidence of overt heart failure (10). The guidelines recommended that the cardiotoxic agent not be started if baseline LVEF was 30% or less and advised discontinuation in patients with more than a 10% decrease in LVEF, resulting in LVEF values of less than 50%. Because of a moderate agreement between left ventricular systolic function determined by MUGA and echocardiography, these guidelines cannot be directly applied to LVEF measured by echocardiography (59). Furthermore, it is important to have a baseline LVEF measurement, and for follow-up it must be emphasized that the same technique should be applied consistently throughout the treatment. On the basis of insights from different types of cardiomyopathy, it is likely that diastolic dysfunction occurs before the deterioration of systolic function. Diastolic dysfunction can be examined by means of both echocardiographic acquisition and MUGA as reflected by a reduction in peak filling rate (10). Monitoring of LVEF by MUGA has been shown to be a cost-effective approach. The overall costs of MUGA studies are lower than the 1-y costs of caring for additional cases of congestive heart failure that are prevented by routine LVEF monitoring (60).
It is not known how long follow-up of LVEF should continue after discontinuation or completion of treatment. Although the development of overt cardiomyopathy is more common within the first year after the discontinuation of therapy, cardiomyopathy can progress in the years thereafter. The increased survival among children and young adults after anthracycline therapy has shown that long-term cardiotoxicity may appear years to decades after treatment. An alarming fraction of more than 65% of survivors of leukemia in childhood has shown progressive cardiac abnormalities 6 y after completing anthracycline therapy (61–63). For trastuzumab, this information may unfortunately probably never become available, because in the 4 large-scale randomized adjuvant trastuzumab trials, prospective cardiac monitoring will not be continued beyond 18–60 mo (64).
99MTC GATED BLOOD-POOL SPECT
The same cardiac blood-pool labeling method as described in the “99mTc MUGA” section can be scanned in a 3-dimensional rather than a planar view by means of SPECT. The GBPS processing software is under clinical evaluation as an all-in-one technique, providing information on LVEF, right ventricular ejection fraction, and wall motion derived from a single examination. These parameters can be assessed by this tomographic technique because it differentiates the left and right ventricles without any overlap. The software allows sophisticated wall motion analysis, which seems valuable in monitoring and tailoring the treatment of congestive heart failure patients.
Regarding LVEF, numerous studies have described a good correlation between GBPS and MUGA (65–67). GBPS, however, tends to underestimate LVEF values and is less reliable in patients with normal small cavities. In addition, in GBPS the right ventricular ejection fraction should be interpreted with caution (68). The method of calculating right ventricular ejection fraction needs to be improved before routine clinical application can be recommended (69,70).
123I-LABELED MIBG SCINTIGRAPHY
LVEF at rest is used by most oncologists to guide anticancer treatments. However, because of the compensatory reserve of the myocardium, which enables adequate ventricular output even in the presence of dysfunctional myocytes, LVEF at rest can underestimate actual cardiac damage (45,71). Some patients with normal resting LVEF show an abnormal response to exercise. Furthermore, several reports have shown that the LVEF at rest correlates poorly with early myocardial damage as determined with endomyocardial biopsy (72–74). A certain critical mass of cell damage must occur before LVEF begins to decrease (75). In fact, clinically overt cardiomyopathy is a late manifestation of progressive subclinical myocardial damage (76). Detection of myocardial injury before irreversible severe left ventricular dysfunction has occurred would be a logical approach. 123I-labeled MIBG scintigraphy is a technique that may provide such an approach (10,45).
MIBG is a guanethidine analog that shares the same uptake, storage, and release pathway as norepinephrine. Unlike norepinephrine, MIBG is not metabolized by catechol-O-methyl transferase and monoamine oxidase and thus has longer residence in adrenergic receptors (77). When labeled with 123I, MIBG can be used to generate a scintigraphic image of the efferent sympathetic nervous innervations of the heart. The sympathetic nervous system uses norepinephrine as its neurotransmitter and acts via adrenoceptors in the target tissue (78). A compensatory sympathetic drive, which increases the contractility, conduction, and heart rate, is activated in a condition of decreased myocardial performance. Neurohumoral responses to congestive heart failure primarily augment renin–angiotensin and sympathetic adrenergics to preserve organ perfusion. Vasoconstriction increases afterload and further lowers cardiac output. Therefore, patients with congestive heart failure have higher levels of circulating noradrenaline and plasma renin. These may contribute to vasoconstriction and progressive impairment of left ventricular function (79).
123I-MIBG scintigraphy has been shown to have a good reproducibility and appears to be sufficiently sensitive to detect abnormalities of myocardial adrenergic innervation before left ventricular function is reduced (80). After intravenous administration of 123I-MIBG, the left ventricle myocardium can be visualized within a few minutes. This initial concentration, measured 15 min after injection, apparently depends primarily on blood flow (81). It reflects both the extravesicular and the intravesicular accumulation of 123I-MIBG in cardiac neurons. The extravesicular concentration of 123I-MIBG decreases rapidly, whereas the intravesicular concentration remains relatively constant. The concentration plateaus after 4 h, indicating the adrenergic neuron terminal concentration (82). Therefore, the 123I-MIBG uptake at 4 h after injection is used to explore specific neuron injury and impairment of the norepinephrine uptake function.
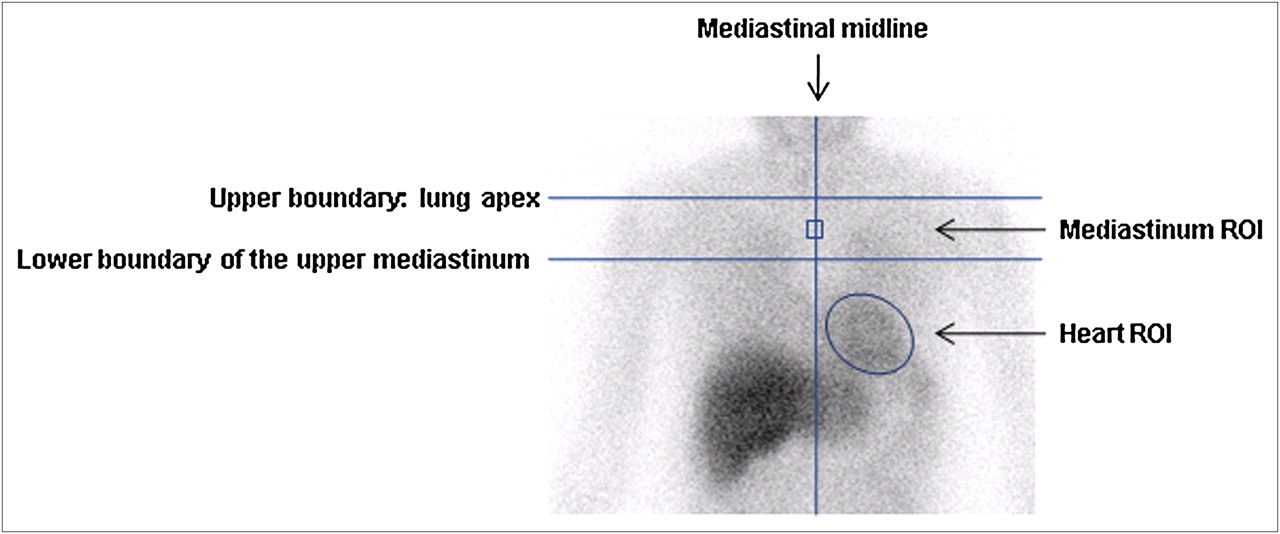
123I-MIBG uptake is often expressed semiquantitatively by drawing regions of interest over the myocardium and mediastinum for calculation of a heart-to-mediastinum count ratio. The same regions of interest are applied for the early 15-min postinjection and late 4-h postinjection images, to calculate the 4-h washout rates (Fig. 1). For this purpose, counts are normalized for injected dose and corrected for decay. The delayed image is a result of washout from the early image and thus is considered to contain combined information regarding both the accumulation on the early image and the washout rate. These relatively simple measures have been widely used in many studies, which support the usefulness of 123I-MIBG scintigraphy in predicting the severity and prognosis of heart failure. An association has been found between the heart-to-mediastinum ratio on the delayed image, the washout rate, brain natriuretic peptide serum norepinephrine concentration, and heart-type fatty acid binding protein, which is a marker for ongoing myocardial damage (83,84). Another report indicated that the heart-to-mediastinum ratio reflected myocardial contractile reserve (85). Furthermore, it was successfully used in monitoring the effect of ameliorating treatment; the improvement rating has been shown to be an excellent predictor of prognosis (86,87). Merlet et al. showed in patients with heart failure and LVEF less than 45% that a heart-to-mediastinum ratio of less than 1.2 was a strong predictor of mortality (88). Nakata et al. showed that a heart-to-mediastinum ratio of less than 1.74 was an independent predictor of cardiac death (89). The normal reference value of heart-to-mediastinum ratios varies widely between institutions, ranging from 1.4 to 2.8, emphasizing the need to internationally standardize the acquisition protocols and methods for quantitation to create appropriate conditions to perform large-scale clinical studies with the aim of establishing evidence for the usefulness of 123I-MIBG (90).

Calculation of heart-to-mediastinum count ratio of 123I-MIBG. Region of interest (ROI) is drawn around left ventricle and in mediastinum. Mediastinal position of ROI is standardized in relation to lung apex, lower boundary of upper mediastinum, and mediastinal midline. Same ROIs are applied for early 15-min postinjection and late 4-h postinjection images, to calculate 4-h washout rates. where H is decay-corrected average counts of heart ROI, and M is decay-corrected average counts of mediastinum ROI.
where H is decay-corrected average counts of heart ROI, and M is decay-corrected average counts of mediastinum ROI.
Several studies showed that 123I-MIBG uptake in the heart is lower in patients treated with anthracyclines than in patients who are not treated with anthracyclines and that the 123I-MIBG uptake decreased in a dose-dependent way. This phenomenon appeared earlier than morphologic changes and alterations in LVEF (10,91). Furthermore, an unexpectedly high incidence of late cardiac abnormalities has been reported in patients who were studied during long-term follow-up.
Two mechanisms have been suggested to explain decreased 123I-MIBG uptake in a heart with doxorubicin cardiomyopathy: decreased 123I-MIBG uptake due to the destruction of adrenergic nerve tissue and functional alteration of adrenergic nerves, such as hyperexcitation of nerve endings as a compensatory mechanism for impaired cardiac pump function (92,93). Furthermore, it has been shown that myocardial 123I-MIBG uptake is related to age. A decrease in myocardial 123I-MIBG uptake is observed with aging, especially in those patients older than 60 y (94). Therefore, myocardial 123I-MIBG uptake has to be corrected for age. It has also been shown that pathologic findings correspond to the 123I-MIBG SPECT findings (95). The reduction in myocardial accumulation of 123I-MIBG was larger in left ventricular than in right ventricular myocardium, in which the adrenergic nervous system is predominant (96). Atrophic and fibrotic nerve fibers were reduced markedly in the segment of the left ventricle in which 123I-MIBG uptake was decreased (95). The subendocardial layer appeared to be more vulnerable than the subepicardium to doxorubicin (92).
CARDIAC SYMPATHETIC NEURONAL IMAGING USING PET
Shortly after 1231-MIBG came into use, PET was established for characterization of the cardiac autonomic nervous system. PET provides several advantages over SPECT. Because of its higher spatial and temporal resolution and the routinely available attenuation correction, PET allows for detailed tracer kinetic analysis and enables noninvasive quantitative measurement of neurophysiologic processes at the tissue level. A major disadvantage, however, is the complex, laborious, and demanding radiolabeling of most of the ligands (Table 3), requiring specific knowledge and a sophisticated infrastructure. Specific yields of the tracer are variable and often low. Thus, only a few PET centers are capable of producing this class of PET tracers. Nevertheless, PET of sympathetic neuronal function has been successfully applied to gain mechanistic insights into myocardial biology and pathology.
Radiotracers for Sympathetic Neuronal PET
A series of different pre- and postsynaptic tracers has been developed (Table 3). The physiologic properties of these tracers, which often more closely resemble the endogenous neurotransmitters than 1231-MIBG, are well understood, and the variety of available tracers may allow for more detailed analysis of neuronal signaling (78). Radiochemical purity and specific activity are critical factors in practical applications. Low specific activity resulting in exposure of the myocardium to unlabeled catecholamines has to be prevented so that competition with the labeled tracer does not hamper image quality and to avoid pharmacologic action due to adrenoceptor activation. The presynaptic tracers are divided into 2 groups (Table 3): the radiolabeled catecholamines (true catecholamines) and the radiolabeled catecholamine analogs (78,97).
The radiolabeled true catecholamines behave identically to the endogenous neurotransmitters and are therefore metabolically active, possibly complicating kinetic data analysis. Catecholamine analogs work as false neurotransmitters: although they share the same uptake mechanism as the endogenous neurotransmitters, they are incapable of following the entire metabolic pathway of true catecholamines. Postsynaptic tracers (Table 3) transmit the sympathetic signal to the target tissue. Compared with the presynaptic tracers, only a small number of tracers for postsynaptic neuronal imaging have been established clinically.
A major challenge in the design of receptor ligands is to find a ligand that can easily be radiolabeled; has high selectivity and affinity; has high metabolic stability, low toxicity, and low lipophilicity, to avoid binding to inactive internalized receptors; and has high specific and low nonspecific binding (97). All these requirements hampered the development of a broad range of radioligands and prohibited widespread clinical use of adrenergic receptor PET.
111IN-ANTIMYOSIN AND 99MTC-LABELED ANNEXIN V
Although radionuclide-labeled antimyosin and annexin V are no longer commercially available, previous studies using these agents have provided insight into the mechanisms of the development of, progression of, or recovery from anticancer treatment–induced heart failure.
The immunoscintigraphic agent 111In-antimyosin was a specific marker for myocardial cell injury and necrosis. It has been studied in conditions such as myocardial infarction, myocarditis, cardiac transplant rejection, and doxorubicin cardiotoxicity (98). Binding of this antibody to intracellular myosin takes place only when sarcolemmal disruption occurs and the cell is irreversibly damaged (98), which may occur in doxorubicin cardiotoxicity. With electron microscopy, morphologic changes were observed, including distended sarcotubular systems, myofibrillar loss, and cytoplasmic vacuolization (73). Morphologic damage in the myocytes and subsequent diffuse myocyte lysis produce the progressive functional cardiac deterioration in these patients (75). This finding is in agreement with the results of several studies. Positive correlation was observed between the cumulative doxorubicin dose administered and the uptake of antimyosin in the myocardium. In these studies, global myocardial antimyosin uptake was quantified by calculating the heart-to-lung ratio on the images acquired at 24–48 h after injection (71,99–102). It was reported that intense antimyosin uptake preceded significant ejection fraction deterioration with continuation of therapy (71,98,102,103). Valdés Olmos et al. reported heart-to-lung ratios of 1.87 in most patients who developed congestive heart failure with additional anthracycline administration (103). In patients with improvement or normalization of the LVEF, generally less intense cardiac uptake (heart-to-lung ratio range, 1.20–1.88) was seen; the heart-to-lung ratio in these patients, who continued chemotherapy without complications, was consistently lower (P < 0.01) than in patients with persistently decreased LVEF and comparable to values of patients who had normal LVEF. Because of its high sensitivity, 111In-antimyosin scintigraphy was useful in the identification of patients at risk for cardiotoxicity (104,105). The specificity of this agent, however, was a concern (102). The extended case report of Nousiainen et al. suggests that patients with a history of severe anthracycline-induced cardiomyopathy have persistent myocardial cell injury up to 10 y after the development of heart failure. These findings seem to be present regardless of recovery of left ventricular function (106). It is, therefore, not known whether abnormal antimyosin uptake is temporary or permanent.
99mTc-annexin V was used to image cell death and apoptosis. The application of this radiopharmaceutical in animal experiments contributed to the knowledge of myocardial injury at the biochemical or cellular level (107). Apoptosis or programmed cell death of cardiomyocytes has been suggested to be an important contributor in the pathophysiology of cardiovascular disease. Apoptotic cardiomyocytes have been identified during anthracycline use but also during hypoxia, ischemia, cardiac overload, acute myocardial infarction, and end-stage heart failure. In apoptotic cells, a cascade of events is initiated. The early stages of apoptosis include the activation of proteases and sphingomyelinases and result in exposure of phosphatidylserine molecules on the outer surface of the cell membrane. 99mTc-annexin V has a high affinity for the exposed phosphatidylserine molecule and thus allows imaging of apoptotic cell death. These early stages of apoptosis precede the characteristic morphologic changes of plasma membrane bleb formation, vesicle formation, and cytoskeletal disruption, with subsequent cytoplasmic contraction, nuclear chromatin condensation, and DNA fragmentation (107). Animal models of acute and chronic doxorubicin cardiotoxicity have been used, and a significant increase in 99mTc-annexin V uptake was observed in the myocardium of doxorubicin-treated animals. Higher uptake was seen in animals treated with multiple doxorubicin doses over a longer time, and this finding correlated well with toxicity scored on histopathology and immunohistochemistry (10,108) and with other indices of toxicity, such as staining with terminal deoxynucleotidyl transferase biotin–deoxyuridine triphosphate nick end labeling in myocardium and expression of left ventricular atrial natriuretic factor messenger RNA (107).
FATTY ACID USE
Taxanes are important agents in the treatment of lung, breast, and ovarian cancer. However, they can cause adverse cardiac effects such as ischemia, arrhythmias, and heart failure. Taxane impairs the normal microtubular transport system in cardiomyocytes, resulting in a failure to store free fatty acids in the lipid pool of the cytosol. As a result, uptake of free fatty acids by the mitochondria may be reduced. This process can be reflected by 123I-15-(p-iodophenyl)-3-(R,S)-methylpentadecanoic acid (BMIPP) scintigraphy or 123I-paraphenyl pentadecanoic acid scintigraphy (106,109).
Saito et al. performed a comparative study of myocardial perfusion scintigraphy and 123I-BMIPP SPECT. They demonstrated that combination therapy with taxane and carboplatin did not affect myocardial perfusion but could impair fatty acid metabolism (109). A decrease of myocardial 123I-BMIPP uptake took place in 56% of patients after treatment. 123I-BMIPP myocardial dynamic SPECT was also useful in the early identification of patients who were at risk for doxorubicin cardiotoxicity, when cardiac function was still preserved (110). Taxanes combined with carboplatin, however, appeared to exert a more toxic effect on myocardial fatty acid metabolism than doxorubicin alone. A significant positive correlation was found between 123I-BMIPP SPECT parameter impairment and LVEF decrement. These findings suggest that combination therapy with taxane and carboplatin causes a decline in myocardial fatty acid metabolism and myocardial contractile dysfunction.
111IN-TRASTUZUMAB
Behr et al. (111) hypothesized that trastuzumab-induced cardiotoxicity is based on a direct effect of trastuzumab on HER2 expressed in the myocardium and suggested that pretreatment scanning with a tracer dose of radiolabeled trastuzumab could predict trastuzumab-induced cardiotoxicity. In a preliminary report, they observed uptake of 111In-labeled trastuzumab in the myocardium in 7 of 20 patients. Six of these patients developed New York Heart Association functional class II–IV heart failure after treatment with trastuzumab, and the seventh patient had episodes of cardiac arrhythmia during trastuzumab administration. In the 13 patients without myocardial 111In-trastuzumab uptake, no adverse cardiac effects occurred. These results, however, could not be confirmed by the study of Perik et al. (112). They observed myocardial uptake at the start of trastuzumab treatment in only 1 of 15 patients. This patient had received extensive anthracycline pretreatment and had cardiac ventricular arrhythmias before trastuzumab treatment. No myocardial uptake was observed in the 3 patients who developed severe symptomatic left ventricular dysfunction during trastuzumab treatment.
Because trastuzumab can induce cardiotoxicity, particularly when combined with anthracyclines, de Korte et al. (113) investigated whether myocardial HER2 expression is upregulated by anthracycline-induced cardiac stress. They obtained 111In-trastuzumab scans in 10 patients shortly after anthracyclines and in 10 patients with nonanthracycline-related heart failure. They observed myocardial 111In-trastuzumab uptake in 5 of the anthracycline-treated patients, who were all without symptomatic cardiac dysfunction. None of 10 heart failure patients showed myocardial uptake. On the basis of these data, trastuzumab-related cardiotoxicity, occurring after anthracyclines, is a 2-step process. The first step, cardiac stress induced by anthracyclines, causes an increase in myocardial HER2 expression. The second step, represented by trastuzumab treatment, subsequently results in cardiac dysfunction through inhibition of HER2-mediated signaling. On the basis of these results, de Korte et al. initiated a new study, of which the results are awaited, exploring the time of occurrence and duration of myocardial HER2 expression in relation to anthracycline chemotherapy.
SUMMARY AND FUTURE PERSPECTIVES
Despite the huge number of currently available options, serial LVEF monitoring using MUGA continues to be the gold standard for assessing LVEF to identify subclinical left ventricular dysfunction in patients treated with cardiotoxic agents, because of its high reproducibility and low interobserver and intraindividual variability and because it is a simple and effective approach not only from a medical but also from an economic point of view.
A decrease in LVEF is, however, a relatively late manifestation of progressive subclinical myocardial damage. A more desirable approach would be detection of myocardial injury before irreversible left ventricular dysfunction has occurred. This approach is important not only for the prevention of cardiac morbidity and mortality but also for the development of newer approaches to prevent cardiac injury, through new dosage schedules, less toxic analogs, or addition of ameliorating agents. Furthermore, these techniques help to provide more insight into the mechanisms and pathophysiology of cardiotoxicity induced by existing and newly developed anticancer agents. The increased survival of patients with several types of cancer, due to the introduction of new antitumor agents, calls for close prospective attention to the potential deleterious cardiac effects of all designer therapeutic agents in development for cancer.
Several nuclear cardiac imaging techniques that belong to third-order functional imaging (visualizing pathophysiologic and neurophysiologic processes at the tissue level) rather than to first-order functional imaging (visualizing mechanical [pump] function) are of interest and can provide such an approach. Some of these third-order functional imaging techniques, such as 99mTc-annexin V (which visualizes apoptosis and cell death), and several sympathetic neuronal PET agents have been used up to now in a preclinical setting only, whereas others have already been studied in a clinical setting. Both 111In-antimyosin and 123I-MIBG scintigraphy have been shown to be excellent early predictors of cancer treatment–induced cardiac dysfunction. These techniques, however, were investigated more than a decade ago, and it is therefore difficult to understand why, despite the promising preliminary results, these strategies have not gained extensive clinical use.
For several semiquantitative measures, such as the washout ratio, heart-to-mediastinum ratio, and heart-to-lung ratio, it would be efficacious to internationally standardize the acquisition protocols and quantitative methods to attain less variation between institutions and create suitable conditions to perform large-scale clinical studies with the aim of establishing evidence for the usefulness of 123I-MIBG scintigraphy.
Clinical experience with neuronal PET is still limited to a few tracers, which mainly target presynaptic sympathetic innervation. Because neuronal PET can add further detail to the biologic insights and this technique allows for a more detailed dissection of processes of neurotransmitter uptake, storage, release, metabolism, and receptor interaction, neuronal PET tracer development remains a worthwhile track of research to pursue. Future challenges for neuronal PET tracer development will include the introduction of neurotransmission tracers and receptor ligands with properties that allow for easier modeling. Such tracers will set the basis for future clinical application of this type of PET technology.
Footnotes
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the role of nuclear medicine imaging techniques in the assessment of cancer treatment–induced cardiotoxicity; (2) the mechanisms on which these scintigraphic techniques are based; and (3) the specific role the scintigraphic techniques could play in the future in the clinical work-up of patients at risk for cardiotoxicity.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNM is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNM designates each JNM continuing education article for a maximum of 1.0 AMA PRA Category 1 Credit. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For CE credit, participants can access this activity through the SNM Web site (http://www.snm.org/ce_online) through April 2012.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.
- 36.↵
- 37.↵
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.
- 63.↵
- 64.↵
- 65.↵
- 66.
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.
- 101.
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- Received for publication August 29, 2010.
- Accepted for publication December 8, 2010.





{kind=link}
Jump to section
- Article
- Abstract
- POTENTIAL MECHANISMS OF CARDIOTOXICITY
- ROLE OF SURVEILLANCE AND EARLY DETECTION OF CARDIOTOXICITY
- NONINVASIVE IMAGING OF CARDIOTOXICITY
- 99MTC MUGA
- 99MTC GATED BLOOD-POOL SPECT
- 123I-LABELED MIBG SCINTIGRAPHY
- CARDIAC SYMPATHETIC NEURONAL IMAGING USING PET
- 111IN-ANTIMYOSIN AND 99MTC-LABELED ANNEXIN V
- FATTY ACID USE
- 111IN-TRASTUZUMAB
- SUMMARY AND FUTURE PERSPECTIVES
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Molecular Imaging Biomarkers in Cardiooncology: A View on Established Technologies and Future Perspectives
- Imaging of Chemotherapy-Induced Acute Cardiotoxicity with 18F-Labeled Lipophilic Cations
- Insights into Doxorubicin-induced Cardiotoxicity: Molecular Mechanisms, Preventive Strategies, and Early Monitoring
- Prevention of Anthracycline-Induced Cardiotoxicity: Challenges and Opportunities
- Noninvasive Imaging of Cardiovascular Injury Related to the Treatment of Cancer
- Cancer Therapy-Induced Cardiac Toxicity in Early Breast Cancer: Addressing the Unresolved Issues