


Abstract
Sincalide-stimulated cholescintigraphy is performed to quantify gallbladder contraction and emptying. However, different infusion methods are used for this study. Our purpose was to determine the infusion method with the least variability (smallest coefficient of variation [CV]) for calculation of the gallbladder ejection fraction (GBEF) in healthy subjects and to establish normal values. Methods: Sixty healthy volunteers at 4 medical centers were injected intravenously with 99mTc-mebrofenin. After gallbladder visualization had been confirmed at 60 min, 0.02 μg of sincalide per kilogram was administered using 3 different infusion durations, 15, 30, and 60 min, each performed on separate days. The CV, mean, SD, first to 99th percentile, and fifth to 95th percentile were calculated. GBEF normal values were determined for the different infusion durations. Results: The CV was smallest for the 60-min infusion at 60 min (19%; 95% confidence interval [CI], 16%−23%), compared with the 30-min infusion at 30 min (35%; 95% CI, 29.2%−42.1%) and the 15-min infusion at 15 min (52%; 95% CI, 44%−63%). These were all significantly different (P < 0.0007). For the 60-min infusion at 60 min, the lower limit of normal for the GBEF was 38% defined at the 1% CI. Conclusion: The GBEF at 60 min has the lowest CV in healthy subjects, compared with shorter infusions of 15 or 30 min. This multicenter trial establishes a GBEF lower limit of normal of 38% (first percentile) for a 60-min infusion of 0.02 μg of sincalide per kilogram, quantified at 60 min. Using this infusion method minimizes the variability in measured GBEFs. This sincalide infusion method should become the standard for routine clinical use.
Cholecystokinin-stimulated cholescintigraphy was first described 3 decades ago as a method to accurately quantify gallbladder emptying (1,2). Sincalide (Kinevac; Bracco Diagnostics, Inc.) is the only commercially available form of cholecystokinin in the United States. Patients are commonly referred for sincalide-stimulated cholescintigraphy for calculation of a gallbladder ejection fraction (GBEF) to confirm chronic gallbladder disease as the cause for recurrent upper abdominal pain.
Numerous investigations over the years have reported that a low GBEF is predictive of symptomatic relief from recurrent biliary colic after cholecystectomy in patients without cholelithiasis; however, some investigations have not found the GBEF predictive (3). Two literature reviews found insufficient evidence to confirm the diagnostic utility of sincalide cholescintigraphy to predict outcome after cholecystectomy for chronic acalculous gallbladder disease, precluding any definitive recommendation regarding its diagnostic use (4,5). They concluded that a well-designed sufficiently powered prospective study is needed. One concern the reviews mentioned was the lack of standardization of sincalide infusion methodology. This may be one explanation for the disparate published results.
Almost 30 investigations have now been published that have used different sincalide infusion methodologies, that is, different total doses, infusion times, dose rates, and normal values (3). The dose, duration of sincalide infusion, and normal values used in clinical practice also vary considerably among different imaging centers. Doses of 0.01–0.02 μg/kg are usually used with infusion times ranging from 1 to 60 min. Some of these methods have validated normal values; however, many have not been validated. Before a prospective clinical trial in patients can be initiated, a scientifically valid sincalide infusion methodology with well-established GBEF normal values must be determined and standardized.
The purpose of this investigation was to determine an optimal method for sincalide infusion by comparing 3 different sincalide infusion methods in clinical use, 0.02 μg/kg for 15, 30, and 60 min, to determine which has the least variability in healthy adults and to establish normal GBEF values for these methods.
MATERIALS AND METHODS
General
The study protocol was written by the investigators and was approved by the Institutional Review Boards at all 4 institutions. Bracco Diagnostics, Inc., Princeton, NJ, provided an unrestricted grant to the Gastrointestinal Council of the Society of Nuclear Medicine to underwrite the cost of this investigation. Both 99mTc-mebrofenin and sincalide were provided free of charge by Bracco Diagnostics, Inc. The company had no involvement in the development of the protocol or its analysis.
Study Subjects
Sixty healthy volunteers were investigated between July 2008 and June 2009. Four medical institutions each recruited, performed, and completed studies on 15 research volunteer subjects, who had 3 studies each. The institutions included Johns Hopkins University, Baltimore, MD; Pennsylvania State University, Hershey, PA; Memorial Health University Medical Center, Savannah, GA; and Temple University, Philadelphia, PA. Before this investigation, the 4 institutions used different sincalide infusion durations, including 15 min (1 institution), 30 min (2 institutions), and 60 min (1 institution).
To be included, the subjects had to be healthy men or women 18–65 y old, with no gastrointestinal disease as confirmed by initial screening using a modified Mayo Clinic Research Gastrointestinal Disease Screening Questionnaire. They also had to have a high probability for compliance and completion of the study. In addition, they had to have normal results for complete blood count, metabolic profile (including liver, renal, and thyroid function tests), serum amylase, and gallbladder ultrasonography. Women had to have a negative pregnancy test.
Subjects were excluded from participation in the study if they had prior gastrointestinal surgery (excluding appendectomy); any surgery within the past 6 mo; cardiovascular, endocrine, renal, gastrointestinal, or other chronic disease likely to affect motility (including diabetes, renal insufficiency, gastroesophageal reflux disease, gastroparesis, irritable bowel syndrome, or peptic ulcer disease); gastrointestinal symptoms (e.g., heartburn, chest pain, dysphagia, abdominal pain, nausea, vomiting, constipation, or diarrhea); or a history of allergic reaction to sincalide. In addition, any subject was excluded if taking chronic opiate pain medications, atropine, nifedipine (calcium channel blockers), indomethacin, progesterone oral contraceptives, octreotide, theophylline, benzodiazepine, or phentolamine. Women were excluded if they were pregnant or lactating or if they were not practicing birth control.
Study Protocol
Each of the 60 subjects had 3 infusion studies at least 2 d apart, and all studies were completed within 3 wk. The order in which the 3 different sincalide infusions were performed was determined by randomization at the time of enrollment.
Subjects reported to the test facility fasting; 45 subjects at 3 institutions fasted overnight and the morning before the examination, 15 subjects at 1 institution fasted for 4 h before the study. All subjects were injected intravenously with 74–111 MBq of 99mTc-mebrofenin (Choletec; Bracco Diagnostics, Inc.). Images were acquired using a wide-field-of-view γ-camera and a low-energy collimator. A 20% window was set over the 140-keV 99mTc photopeak. After gallbladder visualization at 60 min had been confirmed, 0.02 μg of sincalide per kilogram was administered via a constant infusion pump for either 15, 30, or 60 min. A 0.02 μg/kg total dose was used because, first, this dose is approved by the Food and Drug Administration and recommended in the sincalide package insert and, second, the 0.02 μg/kg dose infused over 45 min has been shown to result in a higher GBEF than 0.01 μg/kg but no significant difference compared with 0.04 μg/kg (6).
The sincalide vial was reconstituted with 5 mL of sterile water. Then, 0.02 μg of sincalide per kilogram was withdrawn from the vial using a 1- to 3-mL syringe, transferred into a 30- or 50-mL syringe, and then diluted with sterile normal saline to the 30- to 50-mL syringe volume. The syringe was connected to infusion tubing, which was primed before placing it in the infusion pump. The pump was programmed to infuse the entire volume over 15, 30, or 60 min.
Image acquisition began at the start of the sincalide infusion. Images were acquired dynamically as 1-min frames. At 3 institutions, images were acquired for 60 min regardless of the infusion duration in 45 subjects. In 15 subjects at one institution, imaging was discontinued at the end of the infusion duration, that is, at 15, 30, or 60 min.
For GBEF quantification, regions of interest were drawn for the gallbladder and background (adjacent normal liver) on computer workstations. Time–activity curves were generated. The percentage GBEF was calculated using the formula [(maximum counts − minimum counts)/maximum counts] × 100, corrected for background and radioactive decay. The GBEF was determined at 15, 30, 45, and 60 min for all 3 infusion methods in 45 subjects; 15 subjects at 1 site had the GBEF calculated at the same time intervals but only until the end of the sincalide infusion. To determine the incidence of side effects associated which each infusion method, the subjects were asked about any adverse symptoms. Each institution processed the studies performed at its center.
Statistical Analysis
The primary statistical endpoint of the study was calculation of the coefficient of variation (CV) as a measure of variability for the GBEF for each infusion method at the different intervals to determine which sincalide infusion method had the lowest variation. The CV is the SD divided by the mean and expressed as a percentage. It reflects the variability of the values. Thus, the method considered best would have the lowest CV.
Healthy subjects were recruited to provide an appropriate mixture of both men and women and a wide, evenly distributed age range. The number of subjects required was estimated on the basis of different possible CVs: for a CV of 41%, 95% confidence interval (CI) is 30.4%−65.3% for n = 20, 33.0%−55.6% for n = 40, 34.2%−52.2% for n = 60, and 35.0%−50.4% for n = 80. For a CV of 24%, 95% CI is 18.0%−36.0% for n = 20, 19.4%−31.2% for n = 40, 20.1%−29.5% for n = 60, and 20.3%−28.2% for n = 80. For a CV of 14%, 95% CI is 10.7%−20.9% for n = 20, 11.6%−18.3% for n = 40, 12.0%−17.3% for n = 60, and 12.2%−16.9% for n = 80.
A substantial increase in precision of the CV was found in going from 20 to 40 subjects and from 40 to 60 subjects, with little additional improvement in going higher than 60 subjects (from 60 to 80).
Normal GBEF values were determined for each method using the mean ± 2 and 3 SDs, as well as the fifth and 95th percentiles and first and 99th percentiles. Further analysis was done to determine whether there were significant differences based on age, order, or sex. Statistical analysis was performed using version 9.1.3 SAS software (SAS Institute).
RESULTS
Sixty healthy subjects (32 women and 28 men; age range, 20–62 y; mean ± SD, 38 ± 12 y) met the inclusion and exclusion criteria and were included in the study.
All subjects had confirmed gallbladder filling by 60 min for all 3 studies. Only 2 subjects complained of adverse symptoms during the sincalide infusion, that is, mild nausea and abdominal cramping, and these were reported only for the 15-min-infusion method.
Table 1 shows the results for the 3 different infusions in the 60 healthy subjects, including the infusion duration (min), the time of GBEF calculation after the start of the sincalide infusion, the number of subjects studied, the mean percentage GBEF, the SD, the lower limits using the mean and 2 and 3 SDs, the CV, and the 95% upper and lower confidence limits.
GBEF, SD, Lower Limits of Normal for 2 and 3 SDs, CV, and 95% CIs for 3 Different Infusion Methods at 4 Intervals in Healthy Subjects
The CV was lowest for the 60-min infusion at 60 min (19%), which was significantly different from the CV for the 30-min infusion at 30 min (35%) and for the 15-min infusion at 15 min (52%) (P < 0.0007). The lack of overlap of the CIs shown in Table 1 also confirms statistical significance. The second lowest CV was the 60-min infusion at 45 min (24%), the third and fourth lowest were the 30-min infusions at 60 min (29%) and at 45 min (31%).
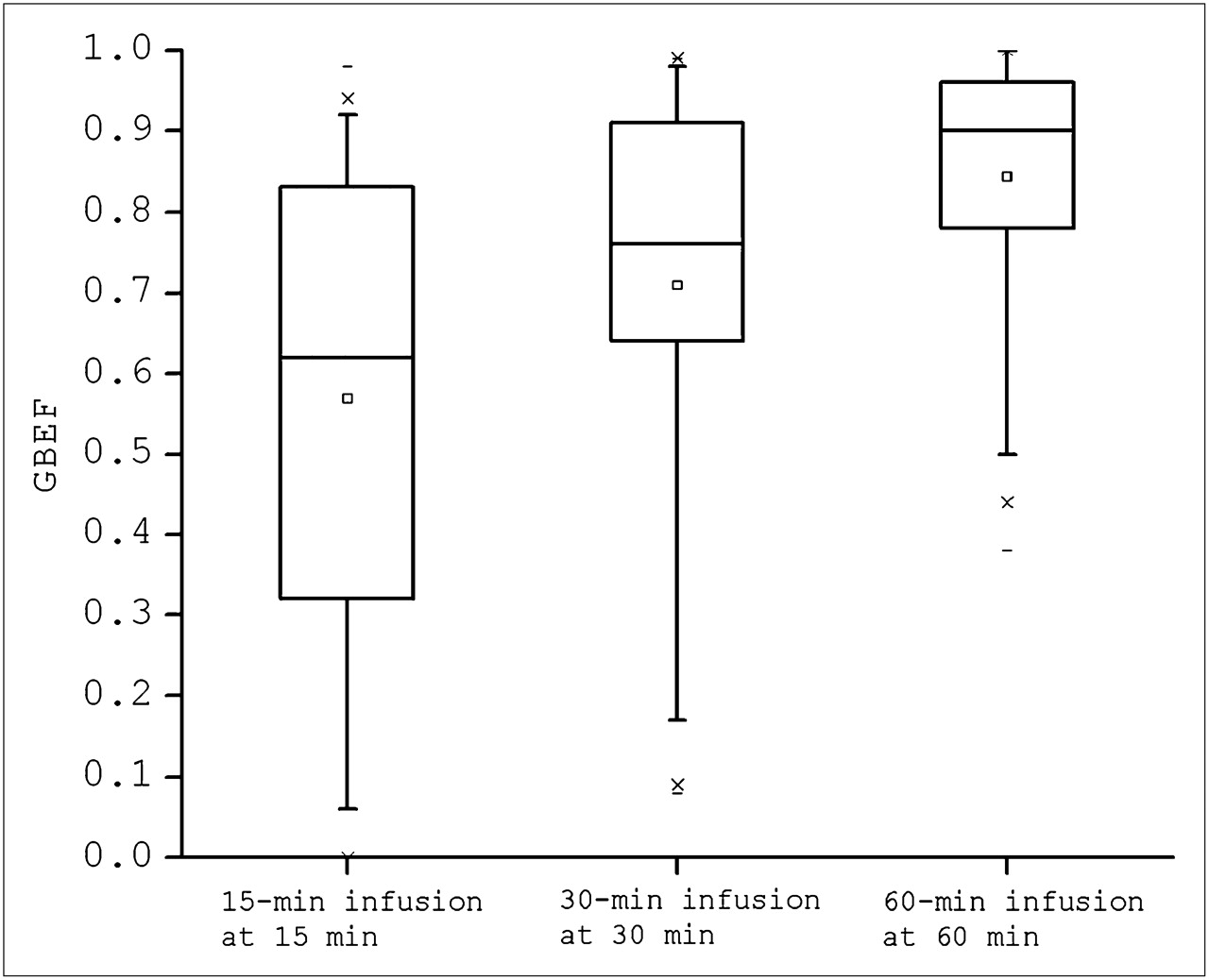
The mean ± 2 and 3 SDs was initially used to calculate normal values for the GBEF. For the 60-min infusion at 60 min, the lower limits of normal for the GBEF were 52% (mean ± 2 SDs) and 36% (mean ± 3 SDs). However, because the data did not have a gaussian distribution and were skewed somewhat to the left, the first, fifth, 95th, and 99th percentiles were considered more appropriate for defining normal values (Table 2; Fig. 1). For the 60-min infusion at 60 min, the lower limits of normal for the GBEF were 49% (fifth percentile) and 38% (first percentile). For the 60-min infusion at 45 min, the lower limits of normal for the GBEF were 38% (fifth percentile) and 20% (first percentile). For the 15- and 30-min infusions, the lower limits of normal for all infusion lengths were all less than 25% and 19% (fifth percentile), respectively, and less than 17% and 13% (first percentile), respectively (Table 2).
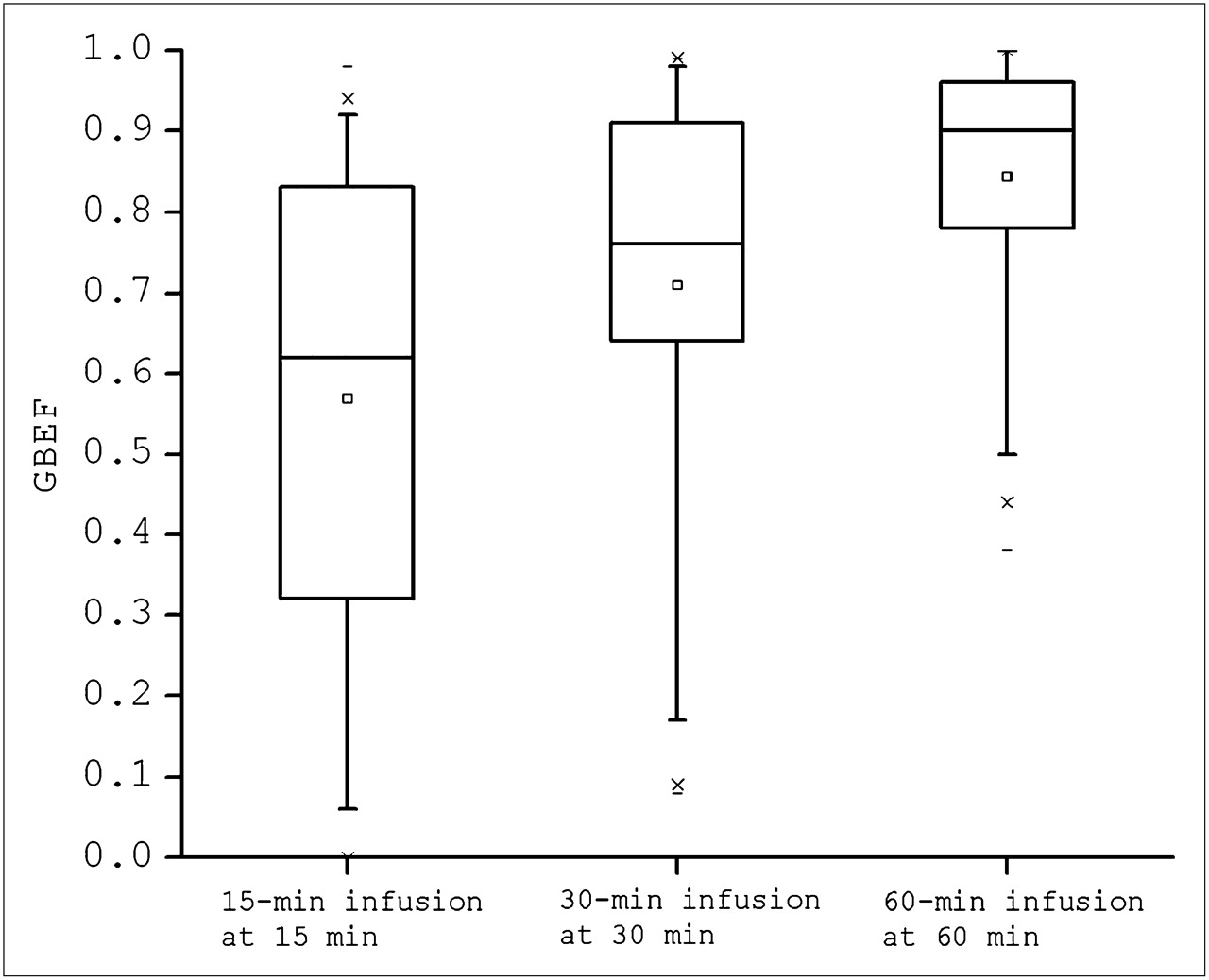
Box plots showing distribution of GBEF values for 3 different infusion groups at different times. Boxes represent interquartile range (25th−75th percentiles, median line in center, mean is a square). Bars represent fifth and 95th percentiles, Xs represent first and 95th percentiles, and dash is minimum and maximum.
GBEF Percentiles for 3 Infusion Methods at 4 Intervals Each
Secondary analysis of the GBEF at the end of the 60-min infusion, grouped by sex and age (20–40 y vs. >40 y) showed no significant differences. The mean GBEF for men and women 20–40 y old was 89.0% ± 14.7% and 81.9% ± 14.5%, respectively. The GBEF for men and women older than 40 y was 88.1% ± 15.7% and 80.5% ± 17.5%, respectively.
DISCUSSION
Sincalide-stimulated cholescintigraphy has been used for over 3 decades for calculation of a GBEF to evaluate patients for recurrent upper abdominal pain suggestive of chronic gallbladder disease. This disorder has been called by various names, including chronic acalculous gallbladder disease, chronic acalculous cholecystitis, gallbladder dyskinesia, cystic duct syndrome, gallbladder spasm, and functional gallbladder disease. Although there are some differences, what they all have in common are symptoms of recurrent biliary colic, poor gallbladder contraction, and relief of symptoms after cholecystectomy.
At least 22 published investigations have reported that a low GBEF is predictive of symptomatic relief after cholecystectomy in patients referred with clinically suspected chronic acalculous gallbladder disease; however, approximately 6 other publications have not found sincalide cholescintigraphy predictive of symptomatic relief after cholecystectomy (3). The reasons for this discrepancy are uncertain, but there could be several factors, including referral bias, small sample size, or the retrospective nature of the investigations. Alternatively, the discrepancy may be due to the many different methodologies and normal values used for sincalide-stimulated cholescintigraphy, many of which have not been well validated. In published reports, administered sincalide doses have varied from 0.01 to 0.5 μg/kg; the infusion duration has varied from that of a bolus to 1, 2, 3, 5, 10, 15, 30, 45, or 60 min; and many different values have been used to define abnormal, including GBEFs less than 30%, 35%, 40%, 50%, and 65% (3).
This multicenter investigation was designed to determine the optimal methodology for infusion of sincalide and to establish normal values. Our approach was to compare 3 different sincalide infusion methods in clinical use, that is, 0.02 μg/kg as a 15-min, 30-min, and 60-min infusion. This approach allowed us to also look at additional intervals and dose rates during and after sincalide infusion; for example, a 60-min infusion at 30 min represents a total dose of 0.01 μg/kg infused over 30 min. The optimal method was defined in this study as the one with the least variation in the healthy subjects, that is, the lowest CV.
There is another method that is used clinically, a 3-min infusion of 0.01 or 0.02 μg of sincalide per kilogram (7,8) with image acquisition for approximately 20 min. However, multiple investigations have shown that this relatively short infusion method has such a variable intersubject contraction response that GBEF normal values cannot be established, and the method results in poor gallbladder contraction in at least a third of healthy subjects who show good gallbladder contraction with slower and longer infusions, and importantly, causes abdominal cramps and nausea in up to 50% of healthy subjects (9–12). The slower infusions, that is, 30–60 min, almost never produce adverse symptoms; the 15-min infusion occasionally causes adverse symptoms, as seen in this study.
In the era of oral cholecystography, bolus infusions of sincalide were reported to sometimes cause nausea and abdominal cramping and spasm of the neck of the gallbladder, with ineffective contraction (13,14). As a result, the sincalide package insert recommends 30- to 60-s infusions. However, the adverse symptoms and ineffective gallbladder contraction seen with a 3-min infusion of sincalide are similar to what is reported with bolus infusions. The symptoms of nausea and abdominal discomfort are due to intestinal cramping caused by the nonphysiologic rapid method of infusion (15). Because of the considerable published data reporting that a 3-min infusion method is unsatisfactory, it was not included in this trial.
The results of this investigation show that the CV is lowest for the 60-min infusion measured at 60 min (19%), significantly lower than the CV for the 30-min infusion at 30 min (35%) and the 15-min infusion at 15 min (52%). The next lowest CV is the 60-min infusion at 45 min (24%), followed by the 30-min infusion at 60 min (29%). The latter intervals offer no clinical advantage over the 60-min infusion at 60 min.
Because the data are not gaussian in distribution, normal values are more appropriately determined using percentiles rather than the mean ± 2 or 3 SDs, although we report both. Using the fifth to 95th and first to 99th percentiles to calculate normal values, we found that the 60-min time-point of the 60-min infusion resulted in a lower limit of normal for GBEF of 38% (first percentile). This value is similar to that obtained in a prior report of 40 healthy subjects using a similar but not identical protocol (0.02 μg/kg/h infused for 45 min and quantified at 60 min) that found the lower limits of normal for the GBEF to be 40% (mean ± 3 SDs) (16). Another study of 20 healthy subjects (12) reported a GBEF lower level of normal of 40% (mean ± 2 SDs) for an infusion method similar but not identical to our investigation (0.01 μg/kg infused over 60 min and quantified at 60 min).
Because of the wide CV, the lower limits of normal calculated for the 15- and 30-min infusions at any time point were determined at best to be equal to or less than 25% (fifth percentile) and 17% (first percentile) (Table 2). This is lower than reported in any previous publication (3), probably because of the small numbers of healthy subjects previously studied. The only 2 previous studies of 30-min infusions showed widely different results, with the lower limit of normal being less than 30% (23 healthy subjects) (11) and less than 65% (15 female subjects) (17). The only prior investigation using a 15-min infusion reported normal values of less than 35% but studied only 15 healthy subjects (18). This result demonstrates the importance of studying a statistically valid number of subjects to establish normal values. We believe that these methods should no longer be used.
Standardization of sincalide infusion methodology and use of statistically valid normal GBEF values determined for that methodology are necessary to gain the confidence of clinicians and surgeons who refer patients for this study. Standardization is also needed to provide uniform evidence-based advice to imaging clinics on the optimal infusion methodology and its appropriate normal values. Finally, standardization of sincalide infusion methodology will make it possible to develop a well-designed clinical multicenter prospective trial that can confirm the utility of a GBEF for predicting outcome after cholecystectomy in patients having recurrent upper abdominal pain possibly due to gallbladder disease.
In summary, our data have determined that the optimal methodology for sincalide cholescintigraphy using a 0.02 μg/kg total dose is infusion over 60 min with quantification of the GBEF at 60 min. Using this method, the lower limit of normal is 38%. The large number of healthy subjects studied and the direct comparison of the 3 methodologies in the same subjects make the results of this multicenter investigation compelling.
CONCLUSION
This multicenter investigation of 60 healthy subjects compared 3 different sincalide infusion durations for a 0.02 μg/kg total dose and found that that a 60-min infusion duration with calculation of the GBEF at 60 min is the optimal method; it has the lowest CV and the best-defined normal values. The lower range of normal for this method is 38% (first percentile). We believe that this infusion method for sincalide-stimulated GBEF should become the standard.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 14, 2009.
- Accepted for publication October 7, 2009.





{kind=link}
Jump to section
Related Articles
Cited By...
- Hepatobiliary Imaging
- Sincalide: A Review of Clinical Utility, Proper Infusion Methodology, and Alternative Cholecystogogues
- Regarding Pharmacology, Part 3A
- Liquid Gastric Emptying as an Adjunct to Hepatobiliary Scintigraphy When Oral Corn Oil Is Used as a Cholecystagogue for Determining Gallbladder Emptying
- Hepatobiliary Scintigraphy in 2014
- Hepatobiliary Scintigraphy in 2014
- Whole-Body Biodistribution Kinetics, Metabolism, and Radiation Dosimetry Estimates of 18F-PEG6-IPQA in Nonhuman Primates
- SNM Practice Guideline for Hepatobiliary Scintigraphy 4.0
- Sincalide-Stimulated Cholescintigraphy: What Is the Standard?
- Reply: Sincalide-Stimulated Cholescintigraphy: What Is the Standard?