


Abstract
Prestimulation with recombinant human thyroid-stimulating hormone (rhTSH) augments radioiodine 131I therapy for benign nontoxic multinodular goiter. The purpose of this study was to determine the optimal time interval between rhTSH and 131I administration to enhance thyroid radioactive iodine uptake (RAIU). Methods: Patients were randomized, in a 2-factorial design, to receive either a 0.1-mg dose of rhTSH (n = 60) or placebo (n = 30) and to a time interval of 24, 48, or 72 h before 131I administration. The rhTSH- or placebo-stimulated RAIU study was performed at 4 wk after a baseline RAIU assessment in a tertiary referral center at a university hospital. A total of 90 patients (78 women; median age, 52 y; range, 22–83 y) referred to 131I therapy for symptomatic nontoxic goiter (median goiter volume, 63 mL; range, 25–464 mL) were included in the study. Change in thyroid RAIU was determined at 24 and 96 h after 131I tracer administration. Results: In the placebo subgroups, RAIU did not change significantly from baseline. The mean (±SE) 24-h RAIU increased from 33.8% ± 2.3% to 66.0% ± 1.8% (111.2% increase) with a 24-h interval, from 36.8% ± 2.1% to 64.6% ± 2.7% (83.3% increase) with a 48-h interval, and from 33.0% ± 2.7% to 49.6% ± 2.5% (62.4% increase) with a 72-h interval. All within-group changes were highly significant (P < 0.001). The effect was negatively correlated with initial RAIU (r = −0.703, P < 0.001). The increase in 24- and 96-h RAIU was significantly higher in the rhTSH/24-h group than it was in the rhTSH/72-h group (P = 0.023 and 0.012, respectively) and insignificantly higher than in the rhTSH/48-h group (P = 0.37 and 0.26, respectively). Conclusion: The effect of rhTSH on thyroid RAIU is most pronounced when administered 24 h before 131I administration and declines with longer time intervals. Whether there is a similar time dependency for goiter reduction after rhTSH-stimulated 131I-therapy remains to be clarified.
- endocrinology
- radionuclide therapy
- radiotracer tissue kinetics
- goiter
- radioiodine therapy
- recombinant thyrotropin
- rhTSH
Although 131I therapy has been used in patients with benign nontoxic multinodular goiter (NMG) for 2 decades, many physicians are reluctant to use this therapeutic option (1,2). An NMG often is large, and frequently the radioactive iodine uptake (RAIU) is low. Consequently, to treat NMG, compared with treating hyperthyroidism, higher 131I activities are needed, resulting in significantly higher extrathyroidal irradiation. However, 131I therapy has a role as a nonsurgical alternative in these patients since levothyroxine suppressive therapy has low efficacy (3) and most NMG patients are ineligible for this therapy (4), when international guidelines are followed (5,6).
Recombinant human thyroid-stimulating hormone (rhTSH) increases the thyroid RAIU by approximately 100% in both healthy individuals (7,8) and goiter patients (9–13). In 3 randomized controlled trials (13–15), rhTSH has been documented to enhance the goiter volume reduction by 35%−56% when standard 131I activities are used. An alternative strategy is to reduce the administered 131I activity with a factor corresponding to the rhTSH-induced increase in RAIU. Thus, the extrathyroidal irradiation can be reduced without compromising efficacy (11). Furthermore, rhTSH-augmented 131I therapy results in a greater improvement in inspiratory function than does conventional (without rhTSH) 131I therapy (16). However, the use of rhTSH in combination with 131I therapy is challenged by potential side effects such as the induction of transient thyrotoxicosis (10) and acute swelling of thyroid tissue (17,18). To minimize the side effects and still maintain the optimal benefit from rhTSH stimulation, it is paramount to establish the optimal dose of rhTSH and the ideal timing for rhTSH injection in relation to 131I administration.
The timing of rhTSH administration has until now been scarcely investigated. In goiter patients, one trial demonstrated that an interval of 24 h (median increase of 90%) was more effective than an interval of 2 h (median increase of 50%) (10). So far, intervals longer than 24 h have been studied only in healthy individuals without goiter and that study points at 24 h being the optimal interval (7). These findings do not necessarily apply in NMG patients, because the morphologic changes in NMG may well result in an altered physiologic response. Thus, the aim of the present study was to investigate the effect of 0.1 mg of rhTSH on the thyroid RAIU when administered at various time points before 131I tracer administration.
MATERIALS AND METHODS
Patients
A total of 90 patients (78 women; median age, 52 y; range, 22–83 y) referred for 131I therapy of symptomatic NMG (median goiter volume, 63 mL; range, 25–464 mL) were enrolled in the study after an initial evaluation in our outpatient clinic. Inclusion criteria were benign NMG and the presence of either pressure complaints or subclinical hyperthyroidism (i.e., serum TSH below the reference range and normal levels of thyroid hormones). A multinodular goiter was defined as a thyroid gland with 2 or more nodules larger than 1 cm, determined by ultrasound. The patients' indication and eligibility for 131I therapy were evaluated by a consultant physician before the final inclusion in the study. The routine diagnostic setup included a thorough clinical evaluation, thyroid function tests, thyroid scintigraphy, and thyroid ultrasound. Because ultrasound is inaccurate in estimating goiter volume in patients with a large goiter and/or retroclavicular extension, MRI was used in such patients. An ultrasound-guided fine-needle aspiration biopsy of any scintigraphically dominant hypoactive nodule was performed to exclude malignancy. Exclusion criteria were age below 18 y, women of childbearing potential without appropriate contraceptive regimen, previous 131I therapy, ongoing levothyroxine or antithyroid drug therapy, history of ischemic heart disease within the last 3 mo, a fine-needle aspiration biopsy that was inconclusive or suggestive of thyroid malignancy, clinical suggestion of malignancy (family history of medullary thyroid cancer or multiple endocrine neoplasia, rapid goiter growth, firm nodules or fixation to adjacent structures, vocal cord paralysis, regional lymphadenopathy, or an elevated serum calcitonin), urinary incontinence, alcohol or drug abuse, and physical or psychiatric disabilities suggesting a patient's difficulty in adhering to the protocol.
The study was approved by the local ethics committee of the county of Funen, Denmark, and registered at http://www.clinicaltrials.gov. All patients provided signed informed consent, and the study was monitored by the good clinical practice unit at Odense University Hospital.
Study Design
The study was randomized, placebo-controlled, and double-blind. In a 2-factorial design, patients were randomized to receive either a 0.1-mg dose of rhTSH (n = 60) or a placebo (n = 30) and to a time interval of 24, 48, or 72 h before 131I tracer administration. Initially a baseline RAIU scan was obtained at 24 and 96 h. Four weeks later, RAIU at 24 and 96 h was repeated after prior rhTSH or placebo stimulation. Randomization was performed by an independent pharmacist at the hospital. A vial containing 0.9 mg of rhTSH (Thyrogen; Genzyme Transgenics Corp.) was reconstituted by a certified study nurse to a concentration of 0.1 mg/mL. The placebo injection constituted 1 mL of isotonic saline. Injections were administered intramuscularly in the gluteal region by the study nurse. For practical reasons, the study nurse was aware of randomization.
Thyroid Function Tests and Thyroid Imaging
Thyroid function tests were performed before screening and enrollment. Blood tests included serum total thyroxinec (T4) (reference range, 65–135 nmol/L) determined by radioimmunoassay (Diagnostic Products Corp.), serum total triiodothyronine (T3) (reference range, 1.00–2.10 nmol/L) determined by radioimmunoassay (Johnson & Johnson, Clinical Diagnostics td.), serum calcitonin (reference range, 0–0.10 μg/L) determined by radioimmunoassay (Medilab, Copenhagen), and serum TSH (reference range, 0.30–4.0 mIU/L) determined by dissociation-enhanced lanthanide fluorescent immunoassay (Wallac Oy). The serum-free T4 index (FT4I) and serum-free T3 index (FT3I) were calculated by multiplying the total values by the percentage of T3 resin uptake (reference interval, 0.77–1.33 arbitrary units). Characteristics of these routine assays have previously been reported (18). Thyroid 99mTc scintigraphy was performed with high-resolution γ-camera equipment. The thyroid volume assessment was based on planimetric measurements made by ultrasound or MRI, respectively, as previously described (19,20).
131I Uptake Measurements
The thyroid RAIU was determined at 24 and 96 h after the oral administration of 131I (0.5 MBq [14 μCi]). Before administration, the 131I tracer dose was placed in a neck phantom, and the counting rate was measured at a fixed distance (30.0 cm from the detector) using a collimated 2-in thalium-doped sodium iodide scintillation probe (Atom-Lab 950; Biodex Medical Systems), with dead-time correction.
Statistical Analysis
All statistical analyses were performed using a statistical software program (SPSS, version 15.0; SPSS Inc.). Kruskal–Wallis, ANOVA, or χ2 tests were used to assess differences in baseline characteristics. The Wilcoxon signed rank test was used to detect within-group changes in RAIU. One-way ANOVA was used to determine changes in thyroid RAIU over time by treatment group. Linear regression analysis was performed to test for a relationship between variables. Data are presented as frequencies and medians (range) or means (±SD/SE), depending on the normality of the data. The level of statistical significance was chosen as P less than 0.05.
RESULTS
Baseline Characteristics
All patients completed the protocol. After randomization, no statistically significant differences in age, sex, smoking status, goiter size, number of previously hemithyroidectomized patients, serum TSH level, FT4I, or baseline RAIU were observed (Table 1).
Baseline Characteristics of Patients in Different Groups
Effect of rhTSH Administration on Thyroid RAIU
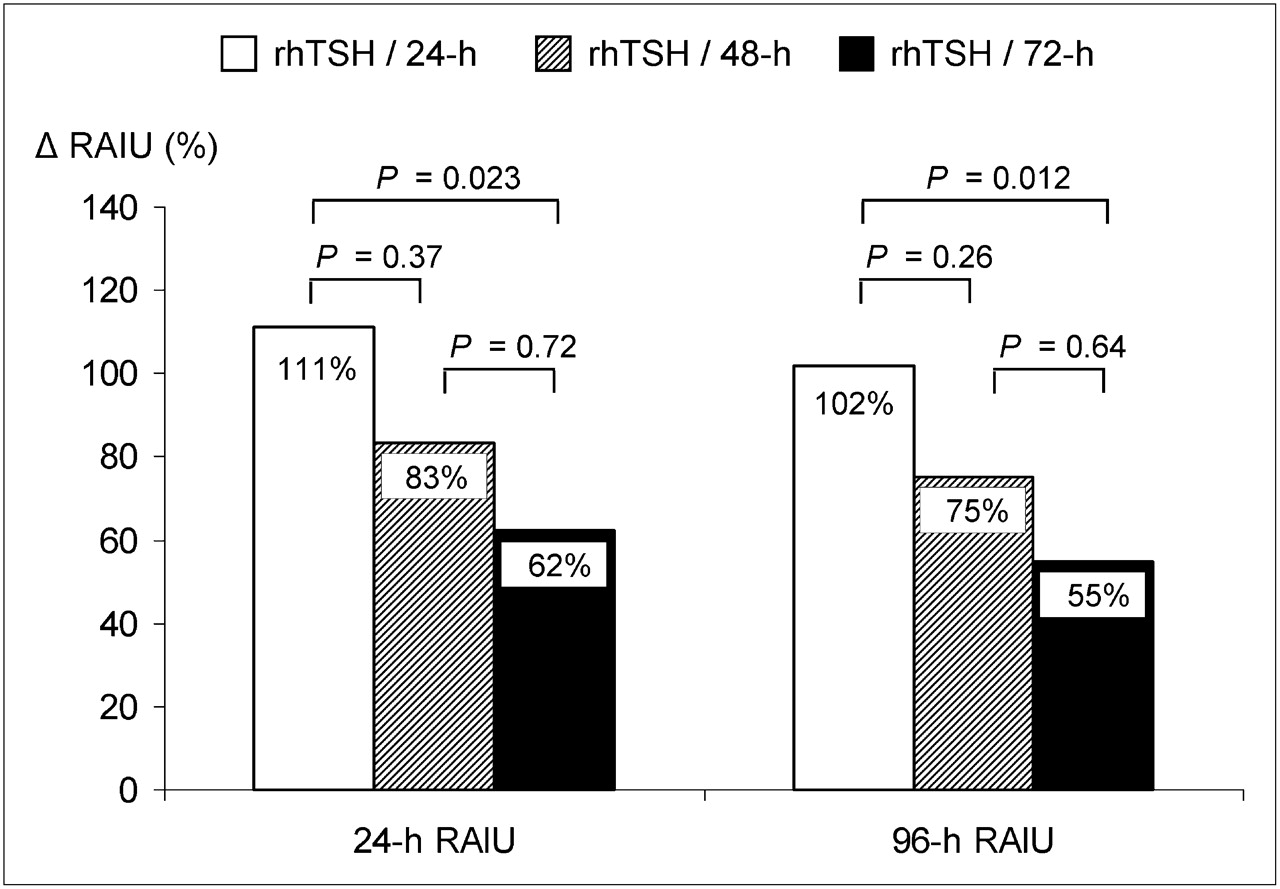
The absolute changes in thyroid RAIU are shown in Figure 1. In the 3 placebo subgroups, thyroid RAIU did not change significantly from baseline. In the rhTSH/24-h group, the mean (±SD) 24-h RAIU increased from 33.8% ± 9.8% to 66.0% ± 7.7% (mean relative increase, 111.2% ± 15.5% [SEM]), and the 96-h RAIU increased from 33.5% ± 10.5% to 62.5% ± 9.3% (mean relative increase, 102.5% ± 13.9% [SEM]). In the rhTSH/48-h group, the mean 24-h RAIU increased from 36.8% ± 9.3% to 64.6% ± 12.0% (mean relative increase, 83.3% ± 11.0% [SEM]), and the 96-h RAIU increased from 37.5% ± 9.8% to 63.7% ± 13.6% (mean relative increase, 74.9% ± 8.7% [SEM]). In the rhTSH/72-h group, the mean 24-h RAIU increased from 33.0% ± 11.9% to 49.6% ± 11.3% (mean relative increase, 62.4% ± 10.5% [SEM]), and the 96-h RAIU increased from 33.9% ± 11.% to 49.0% ± 11.6% (mean relative increase, 55.0% ± 10.3% [SEM]). All changes in RAIU in the rhTSH subgroups were highly significant (P < 0.001). A variance analysis revealed statistically significant differences between the rhTSH subgroups (P = 0.027). Post hoc (Bonferroni) analysis of these differences revealed that the mean relative increase in 24- and 96-h RAIU in the rhTSH/24-h group was significantly higher than the increase in the rhTSH/72-h group (P = 0.023 and 0.012, respectively) and insignificantly higher than the increase in the rhTSH/48-h group (P = 0.37 and P = 0.26, respectively) (Fig. 2).
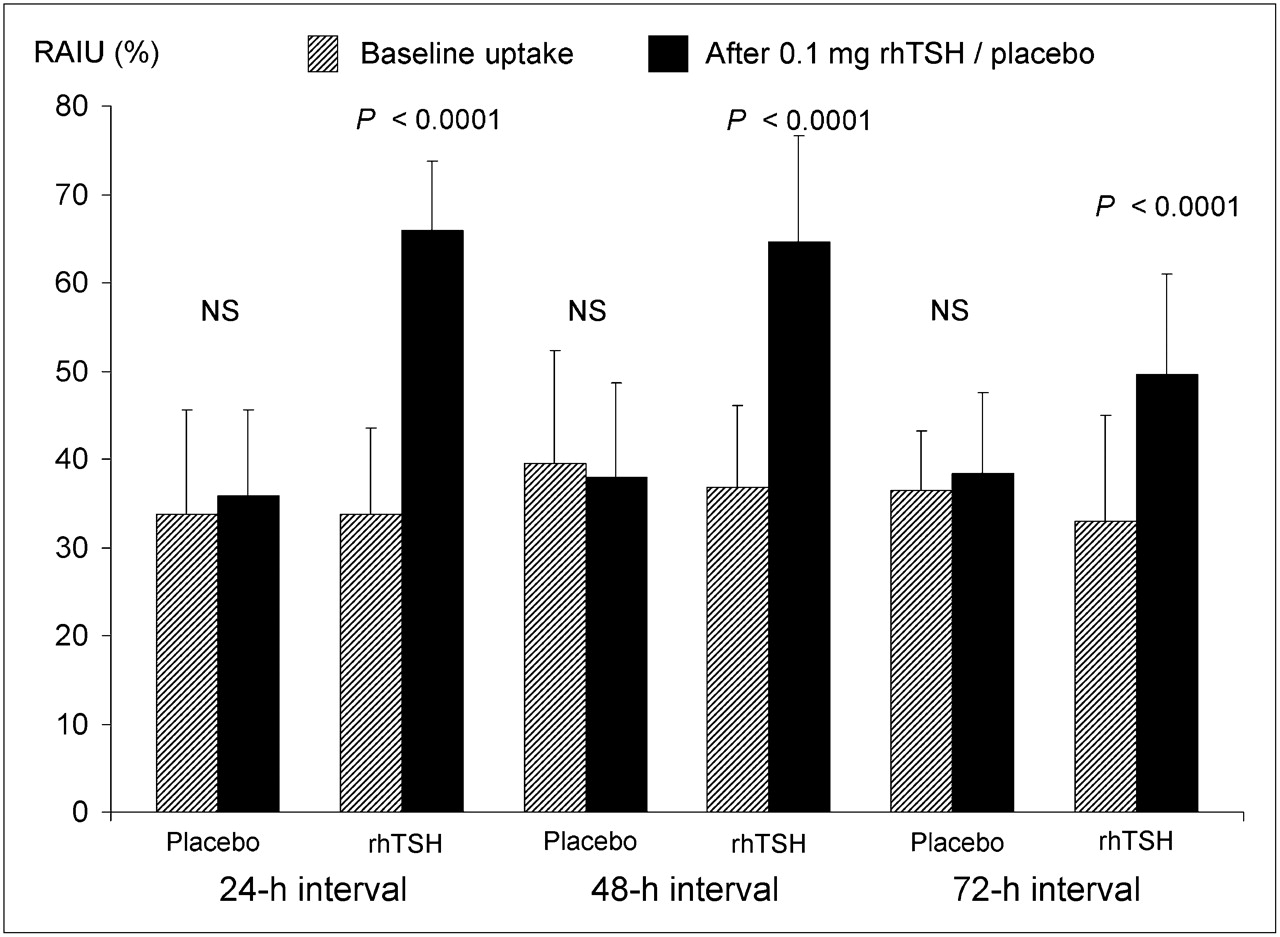
Absolute changes in mean 24-h RAIU (+SD) in all subgroups. NS = not significant.
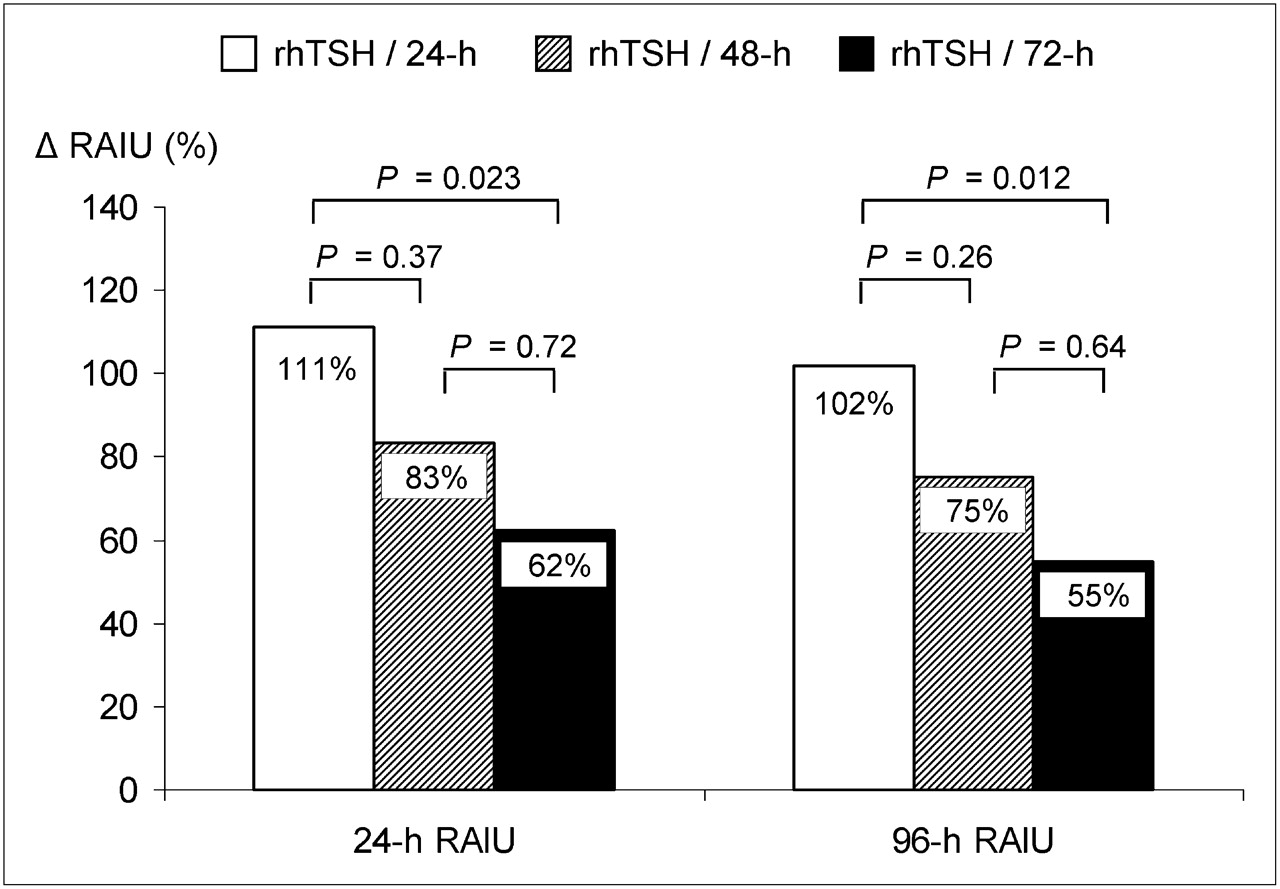
Comparison of mean relative increase in 24-h and 96-h RAIU among rhTSH subgroups. ΔRAIU = change in RAIU.
The mean (±SD) effective 131I half-life at baseline (estimated from the 24- and 96-h RAIU) was 7.3 ± 1.0 d and 7.1 ± 1.2 d in the rhTSH and placebo groups, respectively (P = 0.64). At the second (stimulated) RAIU measurement, a slight decrease to 6.9 ± 1.2 d was seen in the rhTSH group (all 3 groups pooled) (P = 0.07, compared with baseline), whereas the effective 131I half-life in the placebo group was slightly longer (7.4 ± 0.9 d) (P = 0.25, compared with baseline; P = 0.11, compared with the rhTSH group).
In patients with subclinical hyperthyroidism (serum TSH < 0.3 mU/L), the mean relative increase in 24-h RAIU was 104.9% ± 17.4% (SEM), compared with 77.7% ± 7.9% (SEM) in patients with euthyroidism (serum TSH ≥ 0.3 mU/L). This difference was not statistically significant (P = 0.11). However, the randomization resulted in a slightly skewed distribution of the baseline serum TSH between groups (Table 1). To detect any possible independent effect of this variable, a multiple-regression analysis, including the following factors, was performed: rhTSH prestimulation interval, age, sex, smoking status, initial goiter size, baseline serum TSH level, baseline FT4I, and initial 24-h RAIU, which revealed that serum TSH at baseline was inversely correlated to the relative increase in the 24-h RAIU obtained by rhTSH stimulation (r = −0.17, P = 0.040). In addition, the effect of rhTSH on 24-h RAIU was strongly inversely dependent on the initial 24-h RAIU (r = −0.7, P < 0.001), illustrated in Figure 3.

Correlation between initial 24-h RAIU and relative increase in 24-h RAIU after rhTSH stimulation in all 3 rhTSH subgroups.
DISCUSSION
The present study is the first, to our knowledge, randomized, placebo-controlled trial to evaluate the effect of different intervals (24, 48, or 72 h) between rhTSH and 131I administration on the subsequent increase in the thyroid RAIU in NMG patients. Our study underlines that 0.1 mg of rhTSH is a potent stimulator of the thyroid RAIU. We found a 111% increase in 24-h RAIU in the 24-h interval group. Because the effect of rhTSH is highly dependent on the stable iodine load (21) and, especially, the baseline RAIU—but also to some extent on rhTSH dose—comparing this result with previous studies of NMG patients is difficult. In previous studies (9–13,22), an increase in 24-h RAIU between 68% and 335% was found using rhTSH doses from 0.01 to 0.45 mg. This considerable variation can mainly be attributed to differences in baseline RAIU (12%−33%) and to the dose of rhTSH used. Although low doses of rhTSH cause considerable increase in thyroid RAIU, a positive dose–response relationship may exist in the lower range. Thus, in a comparative trial in NMG patients (11), a relative increase in mean RAIU of 87% was observed using 0.01 mg of rhTSH, compared with the significantly higher 145% with 0.03 mg of rhTSH. Another trial (23) demonstrated that the effect of 0.03 mg of rhTSH (increase of 132%) was comparable to that of 0.1 mg (increase of 116%).
Our study clearly demonstrates that the effect of rhTSH on the thyroid RAIU is time-dependent, with a declining effect with an increasing time interval. The lack of a statistically significant difference between the effect observed in the 24- and 48-h subgroups is probably due to the lack of power. rhTSH retained its impact on the 96-h RAIU, showing a pattern similar to that seen with the 24-h RAIU measurements. In an uncontrolled trial including 25 healthy individuals (7)—also using 0.1 mg of rhTSH—the same intervals (24, 48, and 72 h) between rhTSH and 131I tracer administration were investigated. In that study (7), the relative increase in 24-h RAIU was 88%, 36%, and 0%, respectively, in the 24-, 48-, and 72-h rhTSH groups. Our results indicate that the response to rhTSH in goiter patients, compared with healthy individuals, may differ. Although we observed a similar trend (the effect of rhTSH decreased with intervals longer than 24 h), we found that the RAIU was still significantly increased (by 62%) in the rhTSH/72-h group, in contrast to no response seen in healthy individuals (7). Apparently the morphologic or physiologic changes in goiter tissue cause a prolonged effect of rhTSH on RAIU. A possible explanation could be that the inactive tissue in a goiter reacts more slowly to rhTSH stimulation than does normal thyroid tissue. Furthermore, the response to a 0.1-mg dose of rhTSH was much more pronounced in our goiter patients, even though the baseline RAIU was lower in the healthy individuals. However, comparative studies in individuals from the same area have not been performed.
We demonstrated a strong negative correlation between baseline 24-h RAIU and the increase in 24-h RAIU after rhTSH stimulation. This observation is in line with previous studies (9,10,12). Consequently, patients with a low RAIU benefit the most from rhTSH stimulation. In support of this strategy, 1 uncontrolled study (9) in 18 NMG patients with a baseline RAIU of 12% showed an increase in RAIU of 335% after 2 injections of rhTSH (0.1 mg). In these patients, the mean goiter reduction was 39% after 6 mo and 53% after 2 y (9,24). Because many patients with goiter show a low thyroid RAIU, particularly after the introduction of iodization programs, it is promising that considerable goiter reduction can be attained in such patients when rhTSH is used. Previously, the only effective treatment option in such patients was surgery.
Our finding of a negative correlation between the increase in 24-h RAIU and the baseline serum TSH concentration is novel and, potentially, clinically important. The only study so far (10) on this issue did not find such a correlation, but that study group was considerably smaller (n = 15) than ours. In theory, a relationship between serum TSH and the response to rhTSH is plausible. A decreased serum TSH indicates a certain degree of functional autonomy in the thyroid gland, often seen as hot regional areas on scintigraphy. In parallel, the autonomous nodules result in a downregulation of normal TSH–responsive thyrocytes, which may constitute a substantial part of the goiter. On rhTSH stimulation, these dormant or inactive thyrocytes become reactivated for 131I uptake (25), resulting in an increase in RAIU. This theory is well supported by the observation that rhTSH causes a more homogeneous distribution of 131I within the nodular goiter, as shown by Nieuwlaat et al. (25). Thus, through the use of rhTSH, the previous assumption that cold inactive nodules are inaccessible for 131I therapy may no longer be true. It remains unconfirmed whether patients with a low serum TSH (i.e., subclinical hyperthyroidism) attain the most pronounced goiter reduction after rhTSH-augmented 131I therapy.
The purpose of our study was to optimize the timing of the rhTSH injection, with a focus on the impact on the thyroid RAIU. However, the RAIU might not be the only factor of importance when it comes to improvement of the goiter volume reduction. Using conventional 131I therapy, the goiter volume reduction is to some extent related to the retained thyroid dose (26,27). This dose depends not only on the administered activity and RAIU but also on the residence time of 131I within the thyroid gland, reflected by the effective 131I half-life. Theoretically, because of an increased cell turnover, rhTSH stimulation might alter 131I half-life. Although we, in line with previous studies (10,28), observed a slight decrease in the effective 131I half-life in the rhTSH group, it is reassuring that effective half-life was not affected to any greater extent. However, estimation of the effective 131I half-life from a 2-point function is a simplification and does not necessarily describe the true iodine kinetics.
Interestingly, data from our previous randomized controlled trials (14,15) indicate that mechanisms beyond the increase in the retained thyroid dose may be partially responsible for the beneficial effect of rhTSH in combination with 131I therapy. In those studies, we found a positive correlation between the relative goiter volume reduction and the retained thyroid dose in the conventional (without rhTSH) 131I therapy group. However, no such correlation existed in the rhTSH group. A plausible explanation for this additional rhTSH effect could be an increased vulnerability to ionizing radiation of the rhTSH-stimulated thyrocytes. Studies of hyperthyroid patients support that TSH alone might act as a preconditioning factor, amplifying the effect of the 131I therapy (29,30).
CONCLUSION
Our observations indicate that 24 h is the optimal time interval for rhTSH administration to increase the RAIU. However, whether this time interval is also optimal for goiter reduction remains to be established. Patients with a low RAIU and those with low levels of serum TSH—reflecting thyroid autonomy—seem to benefit the most from rhTSH stimulation. Thus, these individuals would be the most obvious candidates for rhTSH-augmented 131I therapy. The optimal dose of rhTSH remains to be clarified.
Acknowledgments
We thank our study nurses, Marianne Reuter and Carina Rebsdorf, and our secretary, Dorrit Pahlke. We also thank Ulla Bindslev-Jensen for taking care of the randomization procedures. Finally, we acknowledge the important support of the staffs of the Departments of Endocrinology and Metabolism and Nuclear Medicine. This study was supported by research grants from the Novo Nordic Foundation, The Strategic Research Council at Odense University Hospital, The Agnes and Knut Mørk Foundation, The National Thyroid League, The Institute of Clinical Research at University of Southern Denmark, The Hans Skouby and wife Emma Skouby Foundation, Dagmar Marshall's Foundation, Oda Pedersens Research Foundation, The Ingemann O. Buck's Foundation, The Else Poulsen Memorial Foundation, and the Danish Agency for Science Technology and Innovation.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 14, 2008.
- Accepted for publication January 6, 2009.





{kind=link}
{kind=link}
{kind=link}