


Abstract
The reliability of sentinel node biopsy is dependent on the accurate visualization and identification of the sentinel node(s). It has been suggested that extensive metastatic involvement of a sentinel node can lead to blocked inflow and rerouting of lymph fluid to a “neo–sentinel node” that may not yet contain tumor cells, causing a false-negative result. However, there is little evidence to support this hypothesis. Recently introduced hybrid SPECT/CT scanners provide both tomographic lymphoscintigraphy and anatomic detail. Such a scanner enabled the present study of the concept of tumor blockage and rerouting of lymphatic drainage in patients with palpable groin metastases. Methods: Seventeen patients with unilateral palpable and cytologically proven metastases in the groin underwent bilateral conventional lymphoscintigraphy and SPECT/CT before sentinel node biopsy of the contralateral groin. The pattern of lymphatic drainage in the 17 palpable groin metastases was evaluated for signs of tumor blockage or rerouting. Results: On the CT images, the palpable node metastases could be identified in all 17 groins. Four of the 17 palpable node metastases (24%) showed uptake of radioactivity on the SPECT/CT images. In 10 groins, rerouting of lymphatic drainage to a neo–sentinel node was seen; one neo–sentinel node was located in the contralateral groin. A complete absence of lymphatic drainage was seen in the remaining 3 groins. Conclusion: The concept of tumor blockage and rerouting was visualized in 76% of the groins with palpable metastases. Precise physical examination and preoperative ultrasound with fine-needle aspiration cytology may identify nodes with considerable tumor invasion at an earlier stage and thereby reduce the incidence of false-negative results.
Sentinel node biopsy is used in a variety of malignancies with a lymphogenic dissemination pattern to assess the tumor status of the regional lymph nodes (1–3). This procedure selects patients who may benefit from early regional lymph node dissection and identifies others who can be spared such dissection in case of the absence of metastasis in the sentinel node.
Unfortunately, the sentinel node procedure is not 100% accurate, and lymph node metastases have been reported after sentinel node procedures with negative results (4). Such false-negative results have a potential impact on survival (5,6). Several hypotheses for why a tumor-positive sentinel node might be overlooked have been postulated (4). One of the proposed causes is the alteration of lymphatic drainage by a phenomenon called tumor blockage (6). In this situation, massive tumor invasion of the sentinel node completely obstructs the lymph flow, preventing tracers from accumulating in the sentinel node and thus preventing its identification. Tracers can be rerouted through other lymphatics to a “neo–sentinel node” that may not yet be involved. In this scenario, the original sentinel node harboring the tumor cells is overlooked and may become apparent later on when the disease progresses and the node becomes palpable (because of the presence of metastases). Although the concept of tumor blockage and rerouting of lymphatic drainage is widely accepted, there is little reported evidence to support this hypothesis.
Hybrid SPECT/CT scanners combine the physiologic information provided by lymphoscintigraphy with the anatomic landmarks provided by CT. This technique creates the opportunity to demonstrate the process of tumor blockage and rerouting in vivo.
At The Netherlands Cancer Institute, sentinel node biopsy is performed in penile carcinoma to assess the tumor status of groin nodes with clinically negative findings. More than 95% of penile malignancies are squamous cell carcinomas that typically metastasize to the inguinal lymph nodes (7–9). The present study concerns 17 patients who had unilateral palpable and cytologically confirmed inguinal metastases and who were scheduled for sentinel node biopsy of the contralateral groin node with clinically negative findings. The palpable groin metastases were evaluated for signs of tumor blockage and rerouting with SPECT/CT.
MATERIALS AND METHODS
Study Design and Inclusion Criteria
Since August 2006, all penile carcinoma patients scheduled for sentinel node biopsy at The Netherlands Cancer Institute undergo preoperative SPECT/CT in addition to conventional planar scintigraphy. Between August 2006 and September 2008, 105 consecutive patients with a penile tumor of at least stage T1 G2 underwent hybrid SPECT/CT before sentinel node biopsy (10,11). Included in the present study were all 17 patients with a unilateral palpable node in the groin that was confirmed to contain metastatic disease by fine-needle aspiration cytology. The median age of the patients was 67 y (range, 48–87 y). Six patients had T1 tumors, 9 patients had T2 tumors, and 2 patients had T3 tumors. Tumor differentiation was intermediate in 12 patients, poor in 1 patient, and unavailable in 4 patients.
Acquisition of SPECT/CT Images
Conventional planar lymphoscintigraphic images were obtained after intradermal peritumoral injection of a 99mTc-nanocolloid (Nanocoll; GE Healthcare) for all patients 1 d before sentinel node surgery.
The tracer was administered at an average dosage of 70 MBq in a total volume of 0.3–0.4 mL at 3 or 4 sites around the tumor. SPECT/CT images were obtained immediately after 2-h conventional images. The SPECT/CT system (Symbia T; Siemens) consisted of a dual-head, variable-angle γ-camera equipped with low-energy, high-resolution collimators and spiral CT optimized for rapid rotation. SPECT acquisition (matrix, 128 × 128; 60 frames; 25 s per frame) was performed with 6°-angle steps. The CT settings were 130 kV and 17 mAs. After reconstruction, SPECT images were corrected for attenuation and scatter. Both SPECT and CT axial 5-mm slices were generated with the Esoft 2000 application package (Siemens). The slices were transferred to a PACS after generation of DICOM (Digital Imaging and Communications in Medicine) files. Fusion of images was performed with an OsiriX DICOM viewer in a Unix-based operating system (Mac OS X, Mac Pro; Apple Inc.).
Analysis of SPECT/CT Images
All scans were evaluated by 2 experienced nuclear medicine physicians. First, the CT images were separately analyzed to identify the palpable inguinal lymph node metastasis. The largest diameter of the node was measured. Second, the fused images were analyzed for the uptake of radioactivity in this node and for the identification of radioactive sentinel nodes and higher-tier nodes. A sentinel node was defined as a lymph node on a direct drainage pathway from the tumor (12). For facilitation of analysis of the lymphatic drainage patterns, the fused images were studied after orthogonal reslicing, when needed.
Surgery
All patients underwent inguinal lymph node dissection of the palpable groin node metastasis, and sentinel node biopsy of the contralateral node with clinically negative findings was performed.
RESULTS
The palpable node metastases were identified on the CT images of all 17 groins and had a median size of 29 mm (range, 19–90 mm). Four of the 17 palpable node metastases (24%) showed uptake of radioactivity on the SPECT/CT images. In 10 groins (59%), there was no uptake in the node metastasis, and rerouting of the lymph to a neo–sentinel node was observed (Fig. 1). Nine of these neo–sentinel nodes were located in the ipsilateral groins, and one was located in the contralateral groin (Fig. 2). A complete absence of lymphatic drainage to the groin nodes with clinically positive findings was observed in the remaining 3 patients (18%) (Fig. 3).

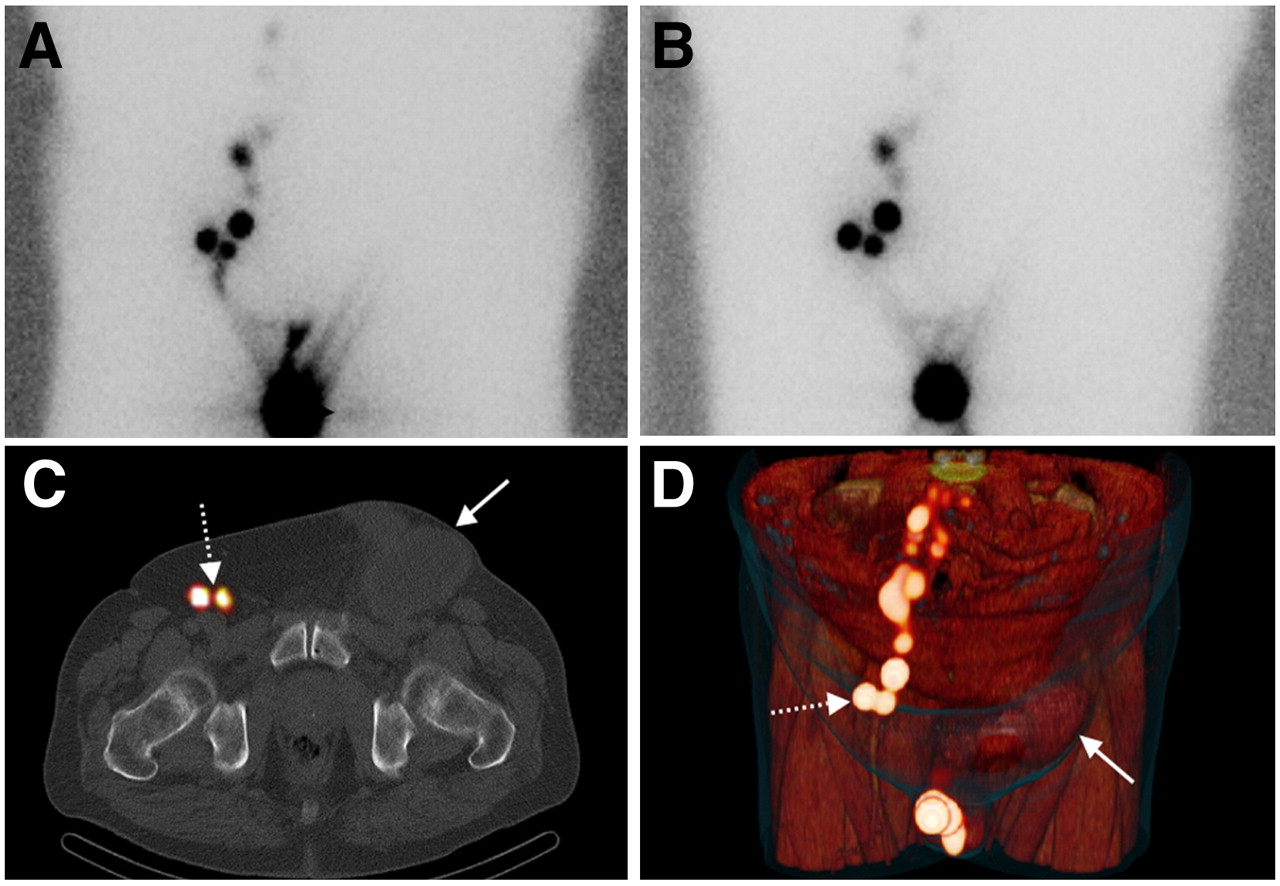
Right groin with palpable lymph nodes and left groin nodes with clinically negative findings in 74-y-old penile cancer patient. (A) Anterior conventional image shows lymphatic drainage to both groins. (C) Fused axial SPECT/CT image shows enlarged lymph node in right groin without uptake of radioactivity (solid arrow) and sentinel node in left groin (broken arrow). (B and D) Fused axial 2-dimensional SPECT/CT image with maximum intensity projection (B) and 3-dimensional SPECT/CT image displayed with volume rendering (D) show lymphatic drainage (small arrows) bypassing metastatic inguinal lymph node (large arrows). Note also uptake of tracer in other inguinal and iliac lymph nodes.

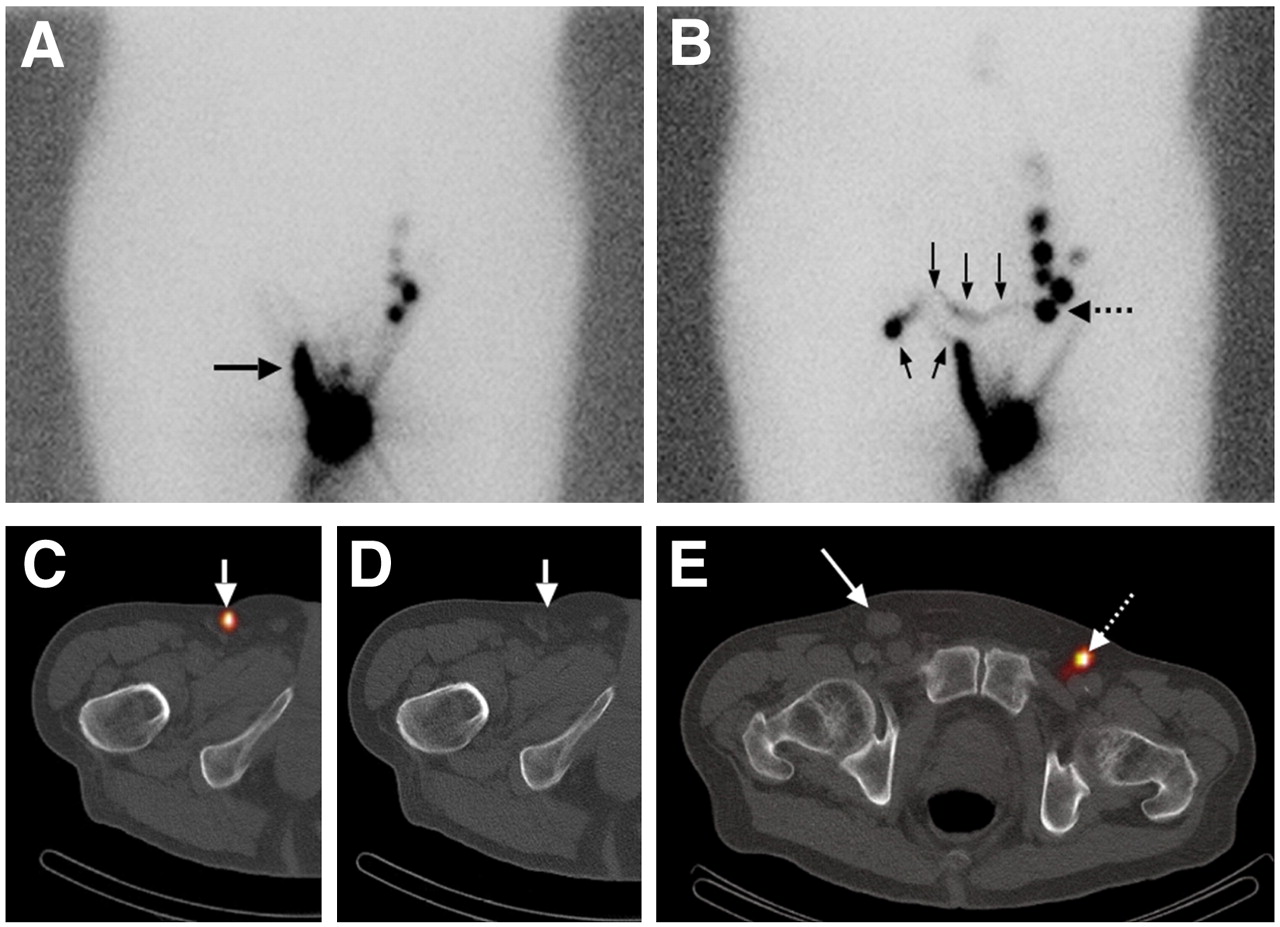
Right groin with palpable lymph node and left groin nodes with clinically negative findings in 84-y-old penile cancer patient. (A and B) Both early (A) and delayed (B) anterior planar images show lymph vessel draining to right groin (horizontal arrow in A). Delayed image shows lymphatic crossing over (vertical arrows) to left groin as well as neo–sentinel node (horizontal arrow in B). (C and D) Tracer accumulation in right groin is related not to lymph node but to tracer stasis in lymphatic vessel, as shown (arrows) on fused SPECT/CT image (C) and CT image (D), on which no lymph node is visible at location of hot spot. (E) Axial fused SPECT/CT image shows that this abnormal lymphatic drainage of right groin is caused by enlarged lymph node (solid arrow). Neo–sentinel node in left groin is shown in color (broken arrow).
Left groin with palpable lymph nodes and right groin nodes with clinically negative findings in 71-y-old patient. (A and B) Early (A) and delayed (B) conventional anterior images show no lymphatic drainage to left groin. (C and D) Two-dimensional axial (C) and 3-dimensional volume-rendered (D) fused SPECT/CT images show that this blockage is caused by enlarged lymph node in left groin (solid arrows). Two sentinel nodes with uptake of radioactivity are seen in right groin (broken arrows).
All patients underwent inguinal lymph node dissection of the groin node containing the palpable metastasis. The dissection specimens contained a median of 2 tumor-positive lymph nodes (range, 1–7 nodes). The median size of the metastatic nodes was 25 mm. Extracapsular growth was present in 5 of 17 specimens. Five of the 17 contralateral groin nodes with clinically negative findings contained a tumor-positive sentinel node.
DISCUSSION
The sentinel node procedure is based on the hypothesis that a lymph node on a direct drainage pathway from the primary tumor is the first to be involved in the case of dissemination. The present study proves that massive tumor invasion of this sentinel node can prevent the uptake of injected tracers and hinder its identification by nuclear medicine physicians and surgeons. In addition, the obstructed sentinel node can cause diversion of the lymph flow to a neo–sentinel node that may not yet be involved. Presuming that this node is the only sentinel node while overlooking the original one can cause false-negative results. In the present study, the total absence of lymphatic drainage to the palpable groin metastasis was seen in 18% of patients, and in 59% of patients, rerouting to a neo–sentinel node was observed. Tracer uptake was noted in only 24% of the lymph nodes with gross metastases.
Two studies have examined the reliability of sentinel node biopsy in penile carcinoma patients with clinically palpable inguinal nodes, with the rationale that metastases are found in only 50% of palpable nodes and that an inflammatory reaction is responsible for the remaining palpable nodes (13–15). Disappointing false-negative rates of 60% and 75% were found in these studies, and it was concluded that sentinel node biopsy is unreliable for groin nodes with clinically positive findings. These results are in concordance with our current findings and emphasize the importance of accurately selecting for sentinel node biopsy only patients who have nodes with clinically negative findings.
In the present study, the phenomenon of tumor blockage and rerouting of lymphatic drainage was demonstrated for lymph nodes with clinically palpable metastases. It seems plausible that this observation can be extrapolated, at least in part, to lymph nodes with nonpalpable metastases. Such nodes cannot be detected by physical examination either because of their small size or because the patient is obese. We speculate that the latter scenario especially could lead to false-negative results in sentinel node procedures. Although there are no data regarding the sizes of metastases in relation to the uptake of radioactivity, it seems likely that a lymph node will accumulate less radioactivity with an increasing tumor load. An enlarged lymph node (potentially not accumulating tracers) is more challenging to detect in an obese patient, thus increasing the likelihood of false-negative results in sentinel node procedures.
For optimal selection of patients suitable for sentinel node biopsy, preoperative staging of lymph nodes is essential. The most important and simplest tool for selecting only patients who have no suspected palpable lymph nodes probably is precise physical examination. An additional tool is preoperative ultrasound with fine-needle aspiration cytology. Ultrasound may be able to diminish the risks associated with tumor blockage by detecting sizable metastases that are not yet palpable (16–19). Another measure for reducing the chances of false-negative results is intraoperative palpation of the wound to identify unstained and nonradioactive lymph nodes that are suspected of containing metastases because of their consistency but that were not found during physical examination and ultrasound (6,20,21).
Rates of false-negative results for sentinel node biopsy vary among different malignancies. In a comprehensive review of 26 published series on sentinel node biopsy followed by routine axillary node dissection in breast cancer, rates of false-negative results varied from 0% to 40%, with a median of 7% (22). In a recent study of breast cancer patients at our institute, the rate of false-negative results without confirmatory node dissection was 1.4% (23). The recent favorable rates of false-negative results may be attributable to the adjuvant therapy that the majority of breast cancer patients receive. Postoperative radiotherapy is often applied to the breast and is likely to target some of the tumor-positive nodes that surgeons may overlook and leave behind in the adjacent axilla. The same can be said for the adjuvant systemic treatment that many of these patients receive.
Rates of false-negative results in melanoma presently are about 10% (24–26). The lack of standard adjuvant therapy for melanoma could explain the difference between this disease and breast cancer. Reported rates of false-negative results in penile cancer vary from 4.8% to 29% (3,27). At our institute, a decrease in the rates of false-negative results from 22% to 4.8% occurred after the introduction of several measures, including preoperative ultrasound and improved histopathologic analysis of the harvested sentinel node (3,28).
CONCLUSION
The present study showed that the scenario of tumor blockage and rerouting of lymphatic drainage does occur. Accurate selection of patients by precise physical examination and preoperative ultrasound may reduce the risks of false-negative results in sentinel node procedures.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 31, 2008.
- Accepted for publication December 5, 2008.





{kind=link}
{kind=link}
{kind=link}