


Abstract
Early experience is described in implementing a new multimodality stress test for accurate correlation of complementary functional and perfusion information from real-time 3-dimensional (3D) echocardiography and SPECT, respectively. The proposed new multimodality stress test has the potential for simultaneously improving sensitivity and specificity in the detection of early coronary artery disease (CAD). Methods: Pre- and poststress real-time 3D echocardiography and SPECT images were acquired in 20 patients referred for CAD evaluation and processed using previously developed algorithms for automatic fusion and quantitative analysis of myocardial function and perfusion. All cases of CAD were diagnosed by reviewing quantitatively analyzed fused images, using newly developed software. Results: Real-time 3D echocardiography, SPECT, advance processing, and image review were successfully performed in all 20 patients. Compared with the angiographic findings in 12 patients, diagnosis based on fused images correctly identified 13 of 13 diseased arteries, compared with 11 of 13 identified by SPECT and 6 of 13 identified by echocardiography-based analysis. Conclusion: The results suggest the feasibility and potential effectiveness of novel multimodality stress testing.
- 3D echocardiography
- myocardial perfusion SPECT
- image registration
- image segmentation
- multimodality
- image fusion
- coronary artery disease
Stress echocardiography and stress SPECT are the 2 most commonly prescribed first-step noninvasive diagnostic procedures for detection of coronary artery disease (CAD) (1) in patients with left ventricular (LV) dysfunction. However, both modalities suffer from low sensitivity and specificity (2,3), often necessitating costly and invasive follow-up procedures. Simultaneous improvement in sensitivity and specificity for detecting CAD may be achieved with multimodality stress testing, wherein diagnosis is based on accurately correlated (temporally and spatially) complementary functional and perfusion information available from echocardiography and SPECT, respectively. Previous studies reporting the combined use of echocardiography and SPECT for diagnosing CAD (4–6) adopted the inherently flawed approach of analyzing echocardiography and SPECT images separately and combining the independent diagnoses of both tests to arrive at a final diagnosis. The result was an inability to simultaneously improve both sensitivity and specificity.
We propose a true multimodality stress-testing approach, wherein diagnosis is based on fused real-time 3-dimensional (3D) echocardiography and SPECT images. This approach allows direct correlation of myocardial perfusion with underlying anatomy during diagnosis, thus eliminating the confounding effects of suspected artifactual defects commonly encountered during diagnosis based on echocardiography and SPECT individually.
This article summarizes our early experience in implementing the proposed multimodality stress-testing approach in a small cohort of patients and presents preliminary results indicating the potential clinical feasibility and effectiveness of the proposed methodology.
MATERIALS AND METHODS
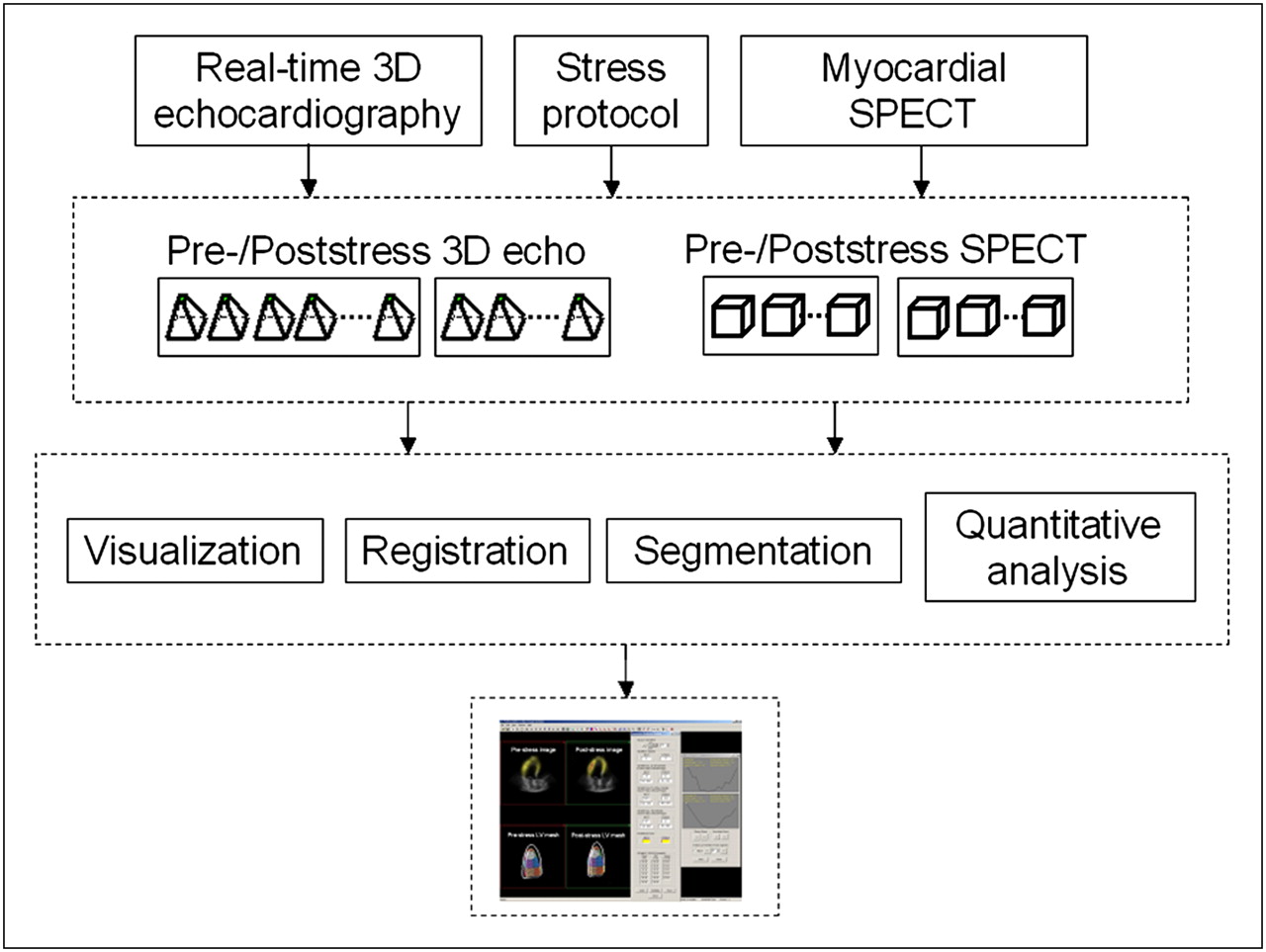
Figure 1 is a schematic of the proposed interactive, quantitative, multimodality stress-testing procedure involving advanced processing of images, quantitative analysis, and new software for image review and diagnostic interpretation.
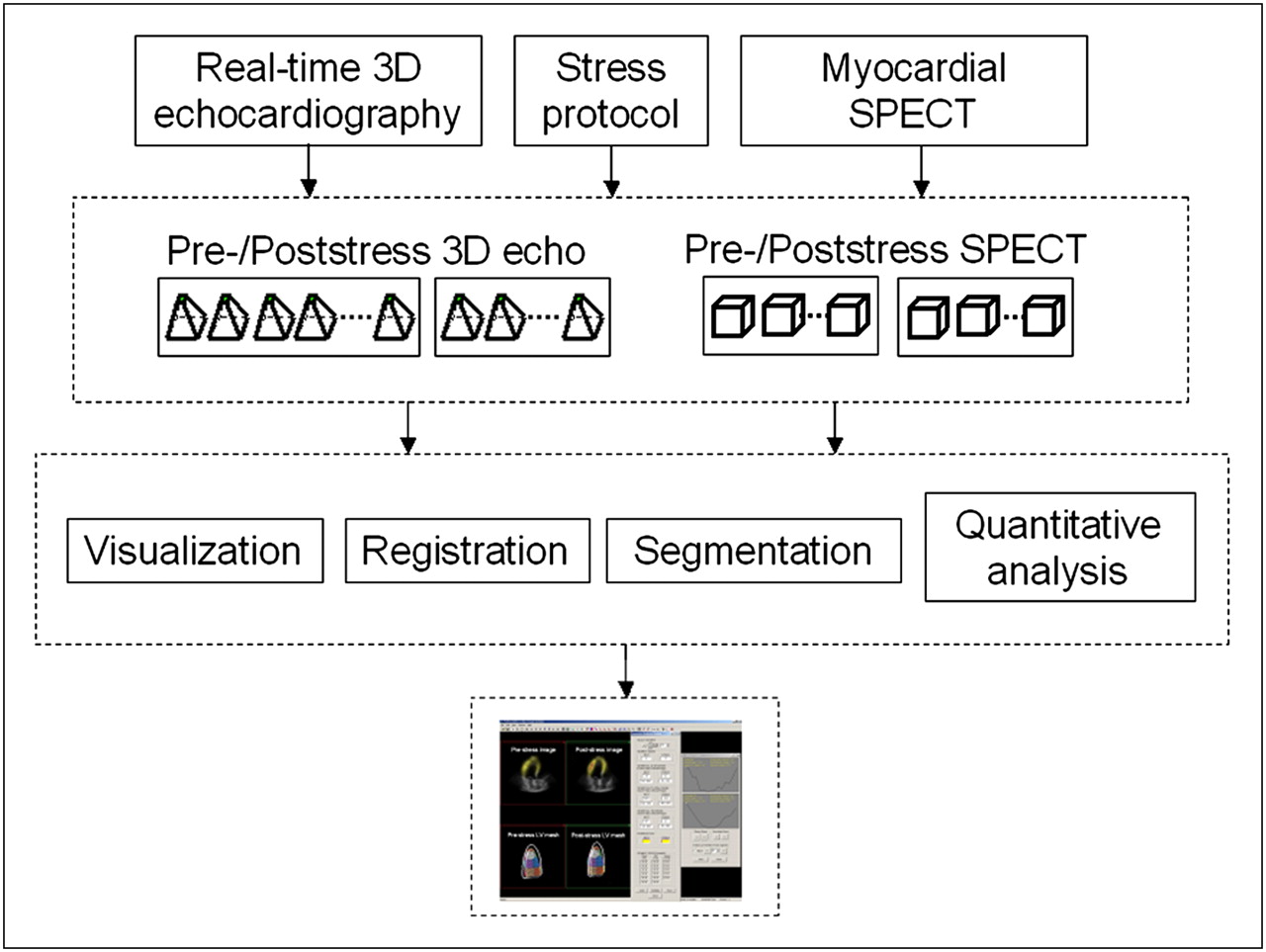
Flowchart of proposed multimodality stress-testing procedure.
Patient Recruitment and Data Acquisition
We recruited 20 consecutive patients (age range, 45–75 y; average age, 62 y; male-to-female ratio, 70:30) with known or suspected CAD referred for clinically indicated stress SPECT studies, without regard to sex or race, as part of a study approved by the Institutional Review Board of the Cleveland Clinic. On the basis of available information, 5 patients had a known prior history of myocardial infarction and 7 patients had known prior coronary intervention or cardiovascular surgery. The only exclusion criterion was known atrial fibrillation (either on medical history or detected at the time of recruitment).
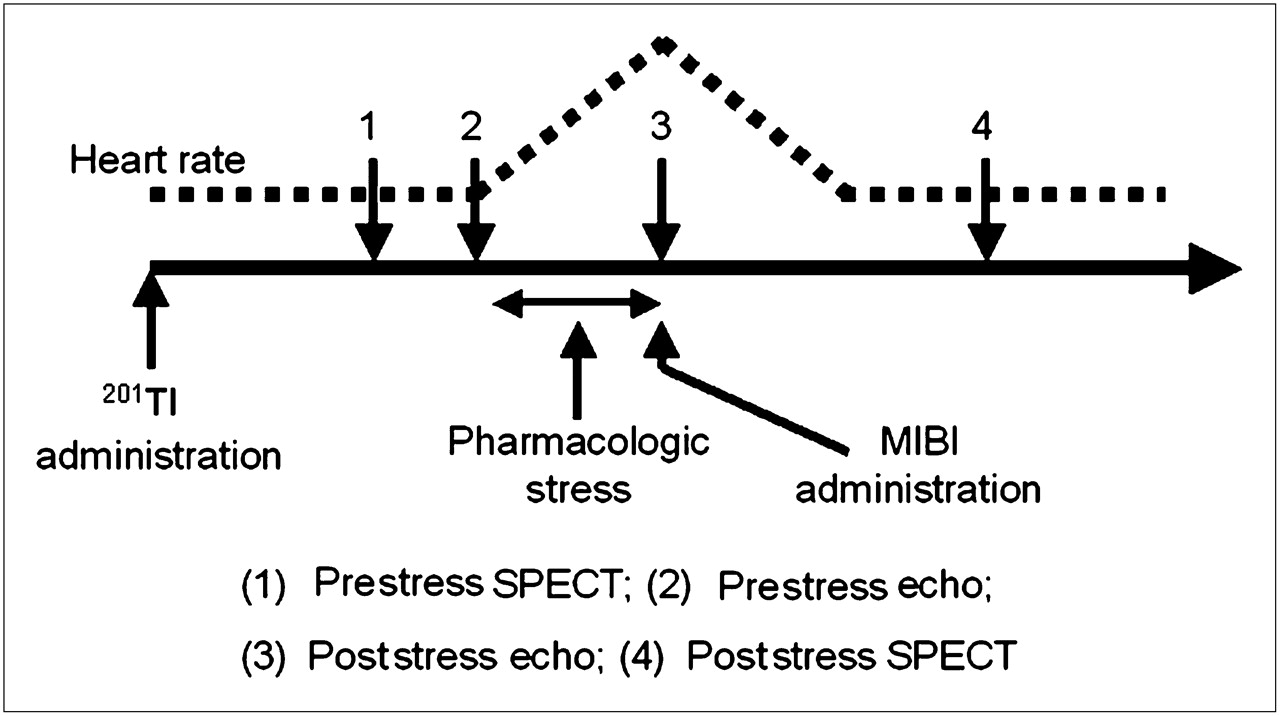
Figure 2 shows the sequence of clinical image acquisition for this study. Electrocardiograph-gated pre- and poststress SPECT image sequences consisting of 8 frames each were acquired using a dual-head γ-camera (Siemens). LV real-time 3D echocardiography images (15–20 frames, depending on patient heart rate) were acquired by a trained sonographer using an iE33 scanner (Philips).
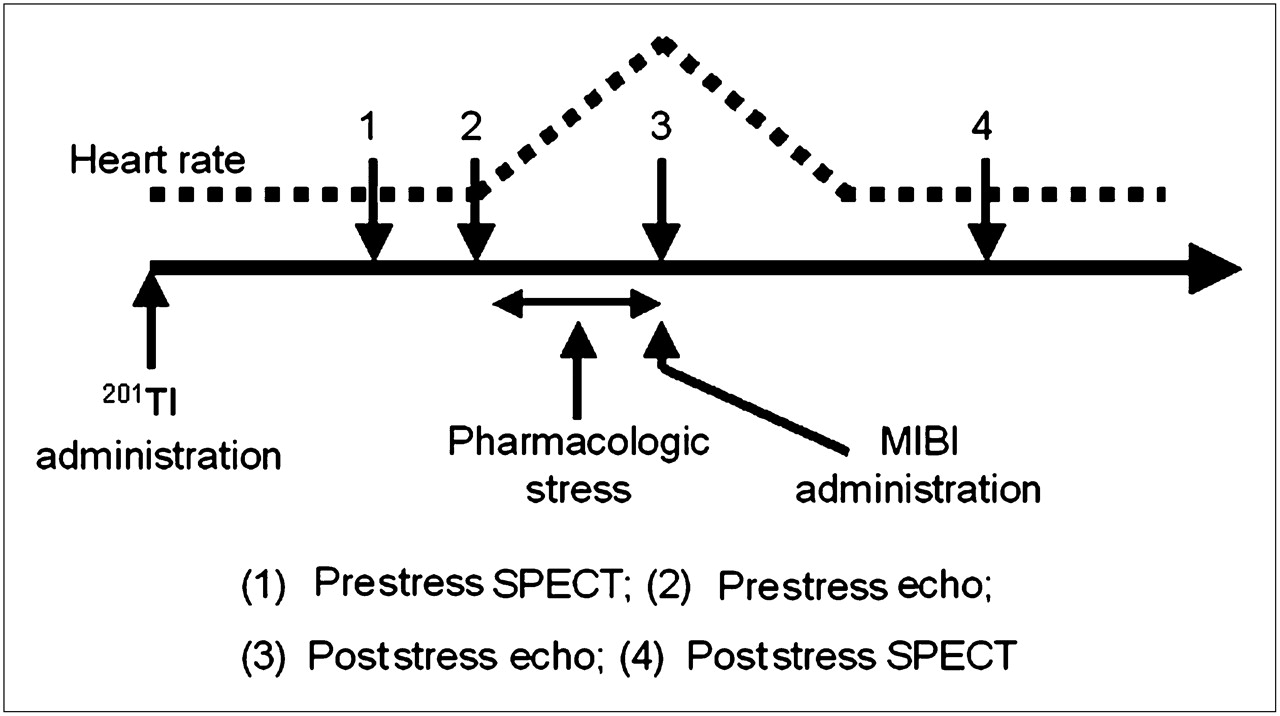
Timeline of clinical image acquisition and corresponding variation of patient heart rate. MIBI = methoxyisobutylisonitrile.
Automatic Image Fusion and Quantitative Analysis
Pre- and poststress image registration, segmentation, and quantitative analysis for all frames of the cardiac sequence were performed automatically for all real-time 3D echocardiography and SPECT images, with no manual intervention. The processed images and results of quantitative analysis were stored for expert review.
Image Registration
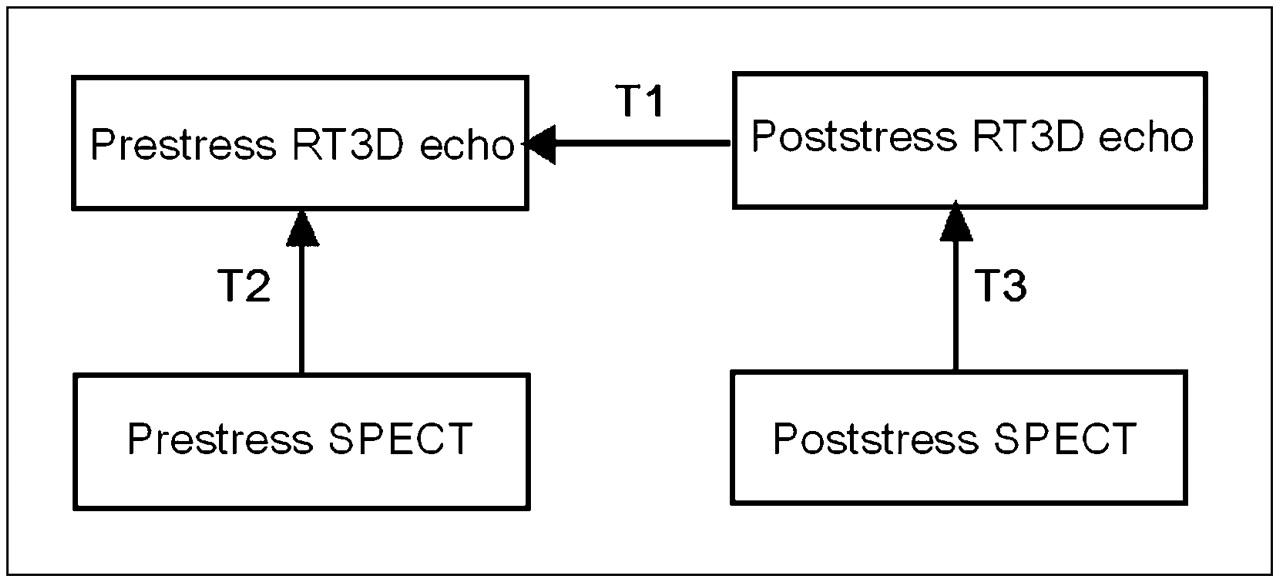
Figure 3 shows the 3 registration tasks required for successful pre- and poststress echocardiography–SPECT image fusion.
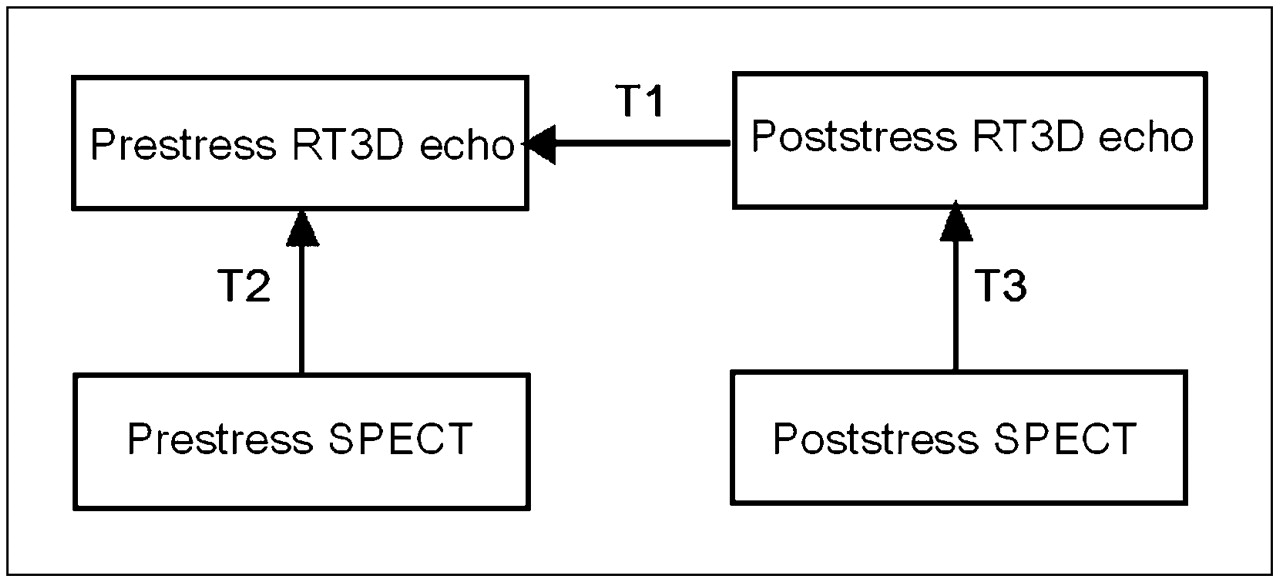
Transformations between pairs of real-time 3D (RT3D) echocardiography and SPECT image sequences: T1, rest–stress echocardiography registration (mutual information–based, rigid-body transformation model); T2, registration of rest echocardiography–rest SPECT (mutual information–based, rigid-body transformation model); and T3, stress echocardiography–stress SPECT registration (mutual information–based, non–rigid-body transformation model).
To account for the varying heart rates between different image sequences, we performed temporal registration by regarding rest echocardiography (with the highest number of frames) as a reference and generated an equal number of phase-matched frames for all other sequences through a piecewise linear interpolation (to account for disproportionate shortening of systole with increasing heart rate) between neighboring frames. Phase-matched frames were subsequently used for spatial registration.
On the basis of our prior successful studies, which involved registration of rest–stress echocardiography and echocardiography–SPECT images (7,8), we used mutual information–based similarity measures for spatial registration. In principle, mutual information is currently the most robust, accurate, and flexible approach for multimodality medical image registration (9), because it is based on correlation between intensity histograms and not directly on anatomic structures.
The aim of rest–stress echocardiography registration (T1) is to recover coordinate system mismatch (resulting from patient position and probe-placement variations) based only on the healthy myocardium while retaining clinically relevant misalignment caused by diseased myocardium. Registration was performed per the technique described previously (8) to recover coordinate system mismatch. For registration of rest echocardiography–rest SPECT (T2), we used a mutual information–based approach with a rigid-body transformation model. The use of mutual information for echocardiography–SPECT registration was successfully demonstrated by our prior feasibility work (7). For the current study, the same mutual information–based approach was used, but all the steps involved in the registration were fully automated, without the need for any manual intervention.
During stress echocardiography–SPECT registration (T3), it is important to note that although stress SPECT represents perfusion information locked in the myocardium at peak stress, the underlying anatomy corresponds to the resting state, because the actual imaging is performed about 40–50 min after reaching peak stress. We used a nonrigid registration algorithm to recover the nonlinear mismatch between the stress perfusion with underlying rest anatomy from SPECT and actual stress anatomy from echocardiography. Details of the algorithm have been described (10). For a pair of reference and floating images, the registration algorithm initially recovers the global mismatch, followed by hierarchical (based on an octree subdivision scheme) refinement of the localized matching between the globally registered images. Because the objective of the current registration is to superimpose matching perfusion information from SPECT over anatomic information from echocardiography, the echocardiography image was treated as a reference image and the SPECT image as the floating image that was morphed to match the reference image. Both global and local registration use a mutual information–based optimization scheme. As described in Walimbe and Shekhar (10), use of the 6-parameter rigid-body transformation model for localized image registration and quaternion-based direct interpolation of the localized transformations for the generation of a smooth global nonrigid transformation field are unique features of this registration algorithm. We used the nonrigid transformation field to superimpose the perfusion data from the floating SPECT image on the corresponding higher-spatial-resolution reference echocardiography image.
Myocardial Segmentation and Quantitative Analysis
Segmentation of the LV myocardium is the prerequisite for performing quantitative analysis of LV function and perfusion. Because of the superior spatial resolution of real-time 3D echocardiography, segmentation of the LV wall was performed in the pre- and poststress echocardiography images using our previously reported algorithm (11,12). Endo- and epicardial surfaces from the real-time 3D echocardiography image were then transferred to the corresponding temporally and spatially registered SPECT image.
After segmentation, the LV wall was automatically divided into 17 segments according to the standard American Society of Echocardiography–defined scheme (13) in both real-time 3D echocardiography and SPECT images (14). LV functional measures (volume curves, ejection fractions, segmental wall thickening, and fractional area change) were evaluated directly from the segmented LV myocardium obtained from the real-time 3D echocardiography images. Per-segment myocardial perfusion was computed as the average normalized SPECT image intensity within the segment, averaged over the cardiac cycle.
Interactive, Quantitative Image-Analysis Software
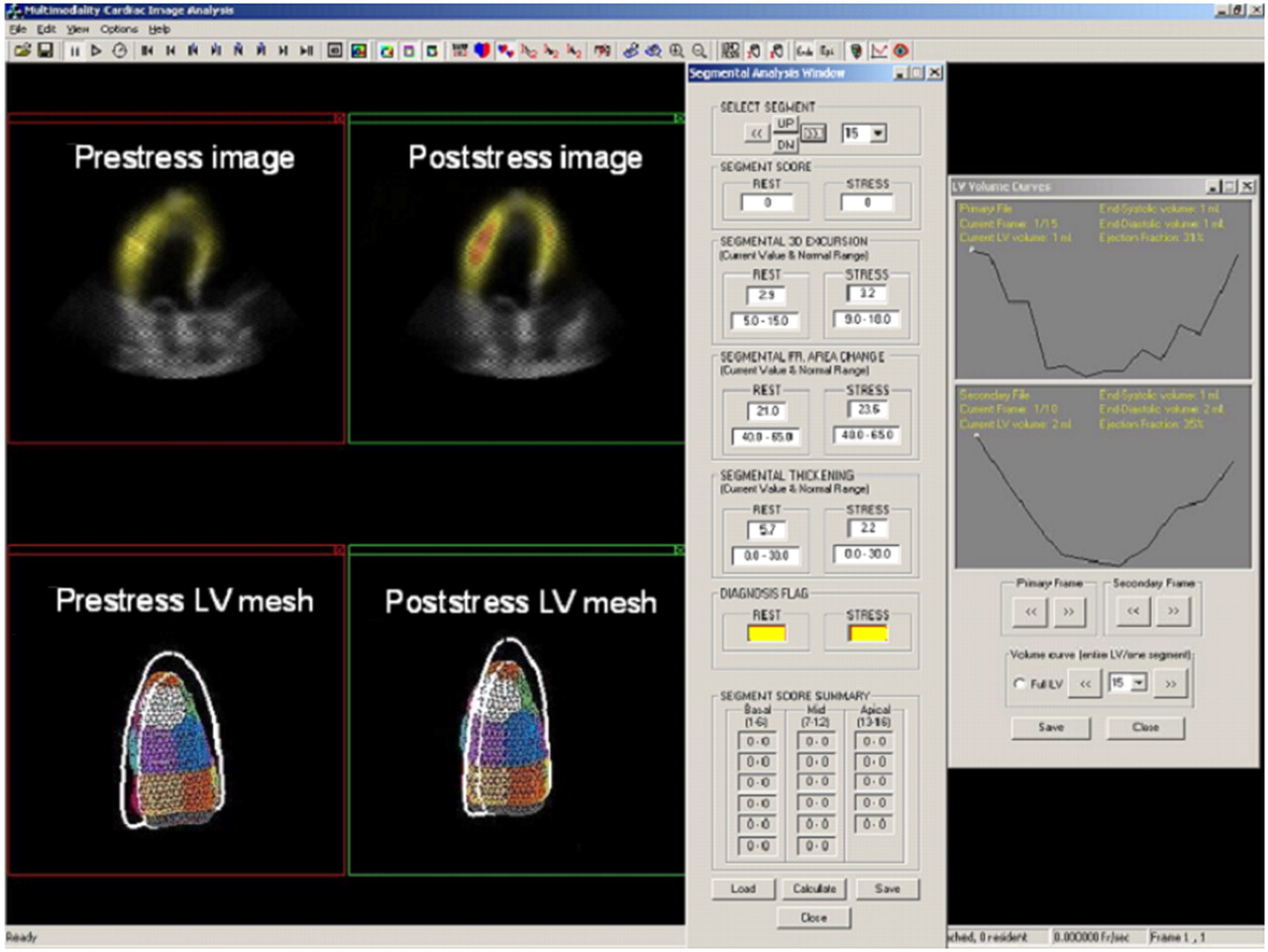
Figure 4 is a snapshot of the quantitative multimodality image-analysis software that was developed for reviewing the temporally and spatially registered echocardiography–SPECT images and the results of the automatic segmentation and quantitative analysis.
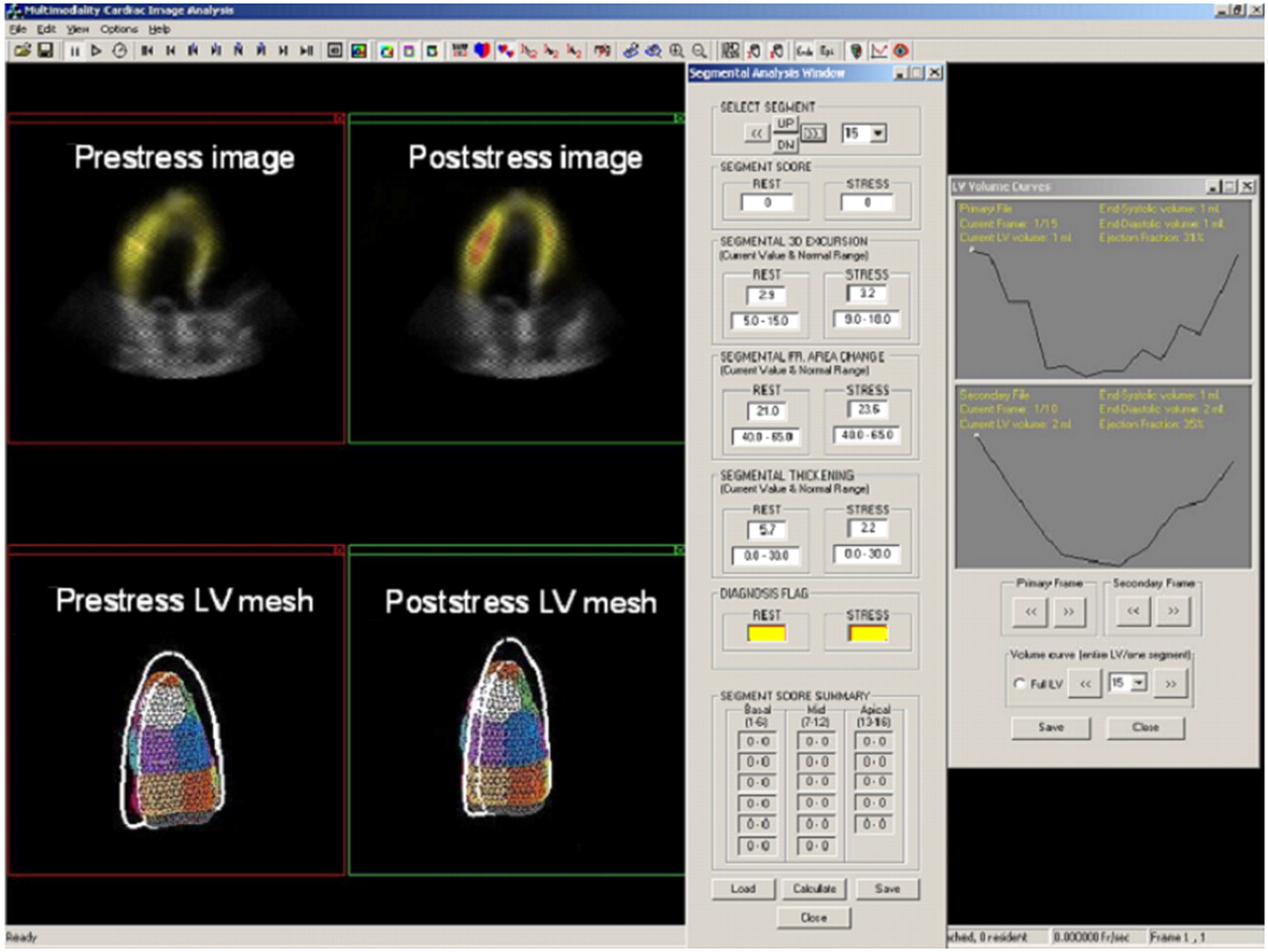
User interface of quantitative, multimodality image-analysis software. User-defined matching pre- and poststress fused images (echocardiography + SPECT) are available after alignment of images using registration techniques. Corresponding LV meshes are obtained using automatic segmentation technique. Results of quantitative analysis are displayed alongside.
During diagnostic review of the images, pre- and poststress cross-sectional views of fused images at identical anatomic locations were available by navigating through either of the images when viewed simultaneously. Using interactive controls, the physician could selectively highlight individual segments simultaneously on the cross-sectional image and the rendered wire meshes, thus gaining a precise understanding of the regional wall motion for accurate and focused regional wall motion analysis. During analysis of any segment, results of the quantitative evaluation of corresponding regional LV parameters were made available interactively, along with images in the form of numeric values and graphs and plots tracking variation over the entire cardiac cycle.
Clinical Evaluation
A nuclear cardiologist with expertise in reading both echocardiography and SPECT images reviewed all 20 cases, using the interactive and quantitative multimodality image-analysis software. A diagnostic rating was assigned for each of 17 LV segments, on a scale ranging from 1 to 5 (1. definitely normal or no disease; 2. suspected disease or inconclusive; 3. mild disease or lesion; 4. moderate disease; and 5. definitely or severely diseased). Segments with ratings of 3 or more were classified as diseased. Diagnosis for each individual segment was based on the assessment of the images by the expert, which was aided by the availability of novel visualization tools and automatically evaluated LV quantitative information. LV segmental ratings from each case were converted to per-vessel ratings using the standard American Society of Echocardiography–determined scheme (13).
Similar diagnostic ratings were also assigned for all LV segments on the basis of review of wall motion only from real-time 3D echocardiography (using the image-analysis tools described in Walimbe et al. (14)) and myocardial perfusion only from SPECT images (using commercially available 4D-MSPECT software), in randomized order, by an echocardiologist and by the nuclear cardiologist (who also reviewed the fused images), respectively. Relative comparisons were performed among the 3 findings for each patient. In the 12 patients in whom angiographic findings were available, angiography was used as the reference standard.
RESULTS
During the clinical stress protocol, all study participants reached or exceeded the 85% maximum predicted heart rate considered necessary for inducing diagnosable myocardial ischemia in the setting of mild-to-significant CAD. Simultaneous pre- and poststress real-time 3D echocardiography and SPECT and all fully automatic preprocessing steps were performed successfully in all 20 patients. No images or patients had to be retrospectively excluded for reasons of inability to complete imaging, suboptimal image quality, or failure to implement any of the preprocessing steps. After the preprocessing steps, the expert physicians were able to successfully analyze all fused images and assign diagnostic ratings for all 17 segments for each case using the image-review software.
Table 1 summarizes the diagnoses for 12 patients for whom reference angiography data were available. For 13 coronary artery territories identified with mild (30%−50%) or severe (>50%) stenosis per angiography, diagnosis based on fused images correctly identified 13 of 13 diseased arteries, compared with 11 of 13 identified by clinical SPECT and 6 of 13 identified by echocardiography-based analysis.
Results of Diagnoses Based on Real-Time 3D Echocardiography, SPECT, and Fused Imaging, with Reference to Standard Angiography, in 36 Coronary Arteries
DISCUSSION
The current work demonstrates for the first time, to our knowledge, a procedure that combines complementary anatomic information (from volumetric real-time 3D echocardiography data) and perfusion information (from SPECT) for the entire cardiac cycle. The simultaneous quantitative analysis of correlated LV wall motion, thickening, and perfusion can minimize ambiguity of diagnosis and allow an improved diagnosis of CAD. The simultaneous analysis can reduce false-negatives from stress echocardiography–based diagnosis in cases of mild disease in which wall motion abnormalities may not be induced (in such patients, the perfusion abnormalities are visible in fused stress images and can help in making the correct diagnosis) and reduce false-positives from stress SPECT–based diagnosis, in which the intensity artifacts in stress SPECT are mistaken for true perfusion abnormalities (in such patients, normal rest and stress wall motion from real-time 3D echocardiography can be used to ascertain that the perfusion defect is, in fact, an image artifact). The multimodality approach is an improvement over gated SPECT, which allows evaluation of myocardial perfusion and only resting wall motion but not of stress-induced wall motion abnormalities. In contrast, fused images provide the potential for diagnosis to be based on the availability of complete pre- and poststress myocardial perfusion and wall motion information (perfusion data from SPECT, together with the spatially and temporally correlated wall motion data from real-time 3D echocardiography).
Successful data acquisition for all patients in the current study provides preliminary evidence of the feasibility of the implementation of dual echocardiography–SPECT in a clinical setting. Real-time 3D echocardiography imaging is noninvasive and adds no more than 5 min to the clinical stress SPECT protocol, making integration of the extra imaging step into the clinical workflow practical and convenient.
Image registration and segmentation algorithms previously developed by our group are important image-processing innovations that enable fusion and quantitative evaluation of real-time 3D echocardiography and SPECT images. Successful implementation of the image-processing steps during the current study provides preliminary evidence of the applicability of these algorithms for images acquired in an actual clinical setting. Moreover, processing of real-time 3D echocardiography and SPECT images using these algorithms is fully automatic and does not add any significant effort on the part of the physician in the interpretation process. The newly developed interactive image-review software allows the physician to interactively view any cross-section simultaneously in fused pre- and poststress images, which—with simultaneous knowledge of the exact quantitative regional wall motion, wall thickening, and perfusion information—makes the diagnosis more objective, potentially resulting in smaller interobserver variability.
The small sample size of the study makes it difficult to derive a statistically significant conclusion regarding the improved diagnosis of CAD using the multimodality stress-testing approach. However, these results indicate the potential for improving the diagnosis of CAD using a multimodality approach. A larger follow-up clinical trial would be necessary to more rigorously evaluate the hypothesis of improved diagnosis of CAD using the proposed multimodality approach.
CONCLUSION
A novel multimodality stress-testing approach, involving real-time 3D echocardiography and myocardial gated SPECT, is both feasible and promising for performing dual imaging tasks in a clinical setting and implementing novel visualization and advanced image processing for effective and efficient CAD evaluation. The results of this small-scale clinical evaluation study indicate that this combination of fused real-time 3D echocardiography and SPECT plus interactive, quantitative analysis has excellent potential for accurate detection of wall motion abnormalities and improved diagnosis of ischemia with underlying CAD.
Acknowledgments
Vivek Walimbe is currently with GE Healthcare and performed this work in full as part of doctoral dissertation research at the Ohio State University and the Cleveland Clinic. This work was funded in part by the American Heart Association (predoctoral fellowship grant 0415141B) and the Cleveland Clinic General Clinical Research Center.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 31, 2008.
- Accepted for publication November 12, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.