


Article Figures & Data
Figures
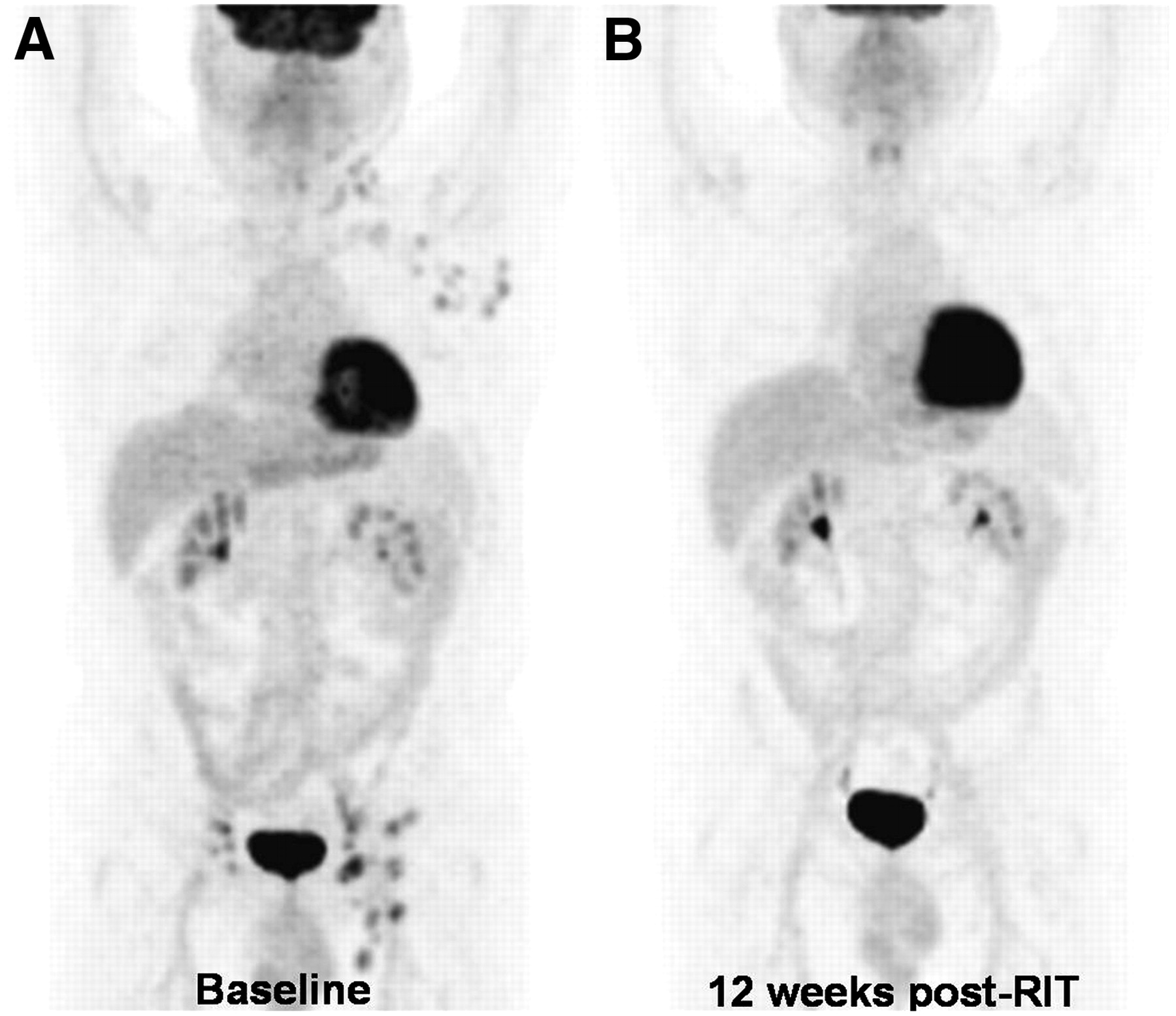
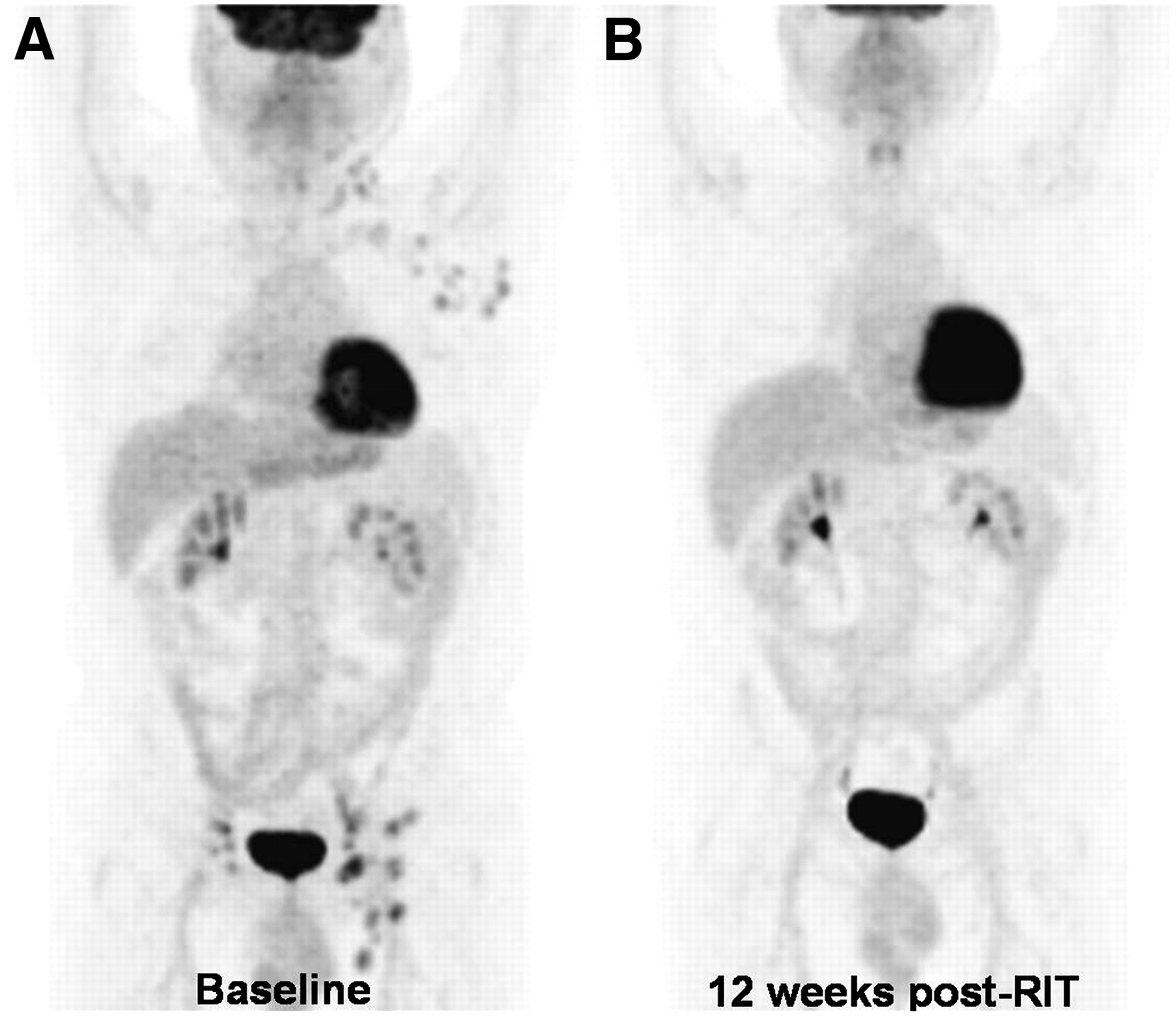
- FIGURE 1.
Homogeneous response to radioimmunotherapy. A 67-y-old man with grade 2, follicular NHL presented with progressive disease after rituximab and chemotherapy. Baseline 18F-FDG PET scan (A) revealed 18F-FDG–avid adenopathy in left neck, left axilla, and bilateral inguinal regions, which suggested active NHL. Patient received 65-cGy total-body radiation dose of 131I-tositumomab. 18F-FDG PET scan at 12 wk after therapy (B) revealed complete resolution of abnormal metabolic activity, and he remained in complete remission for 15.5 mo after radioimmunotherapy.
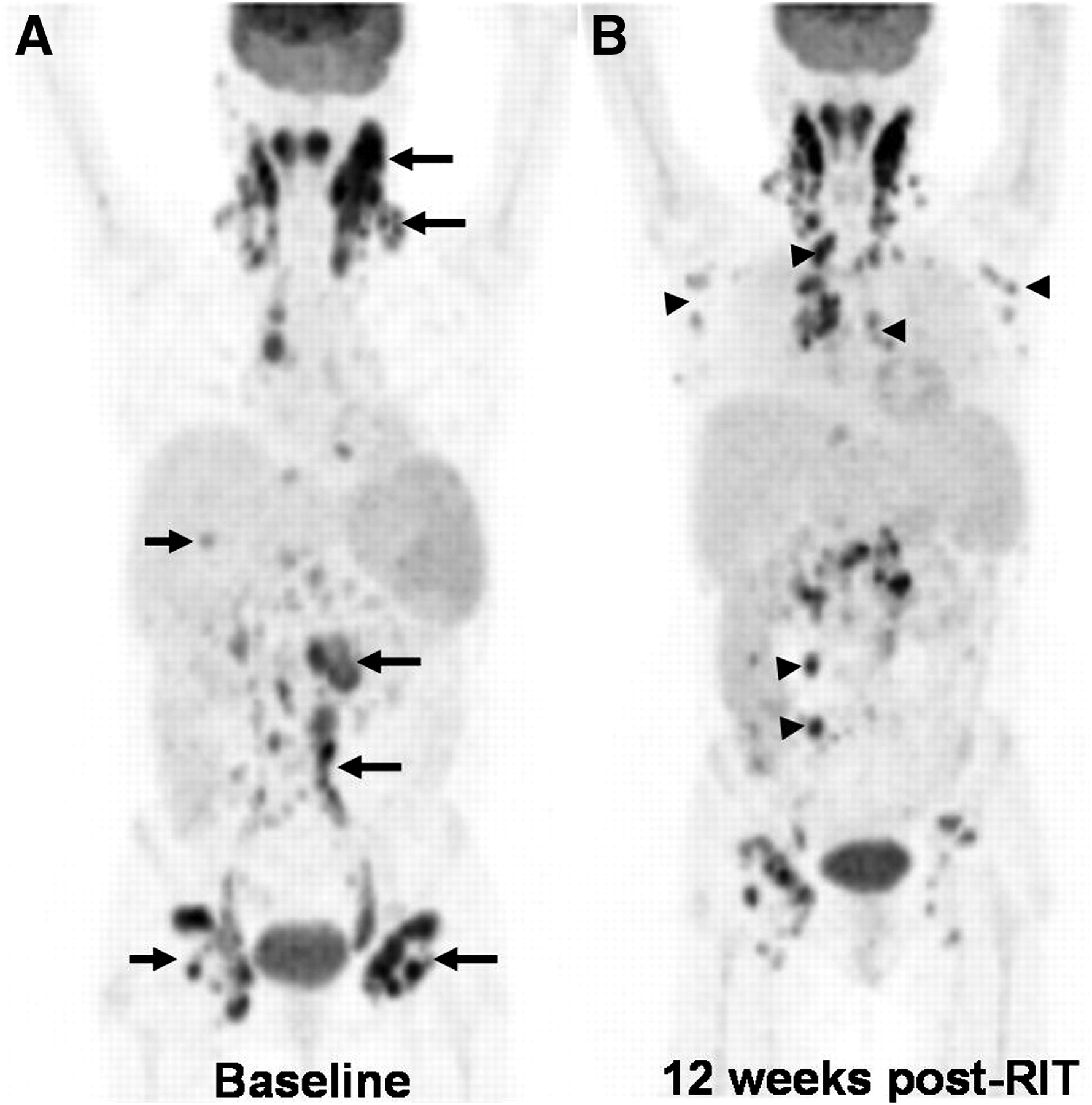
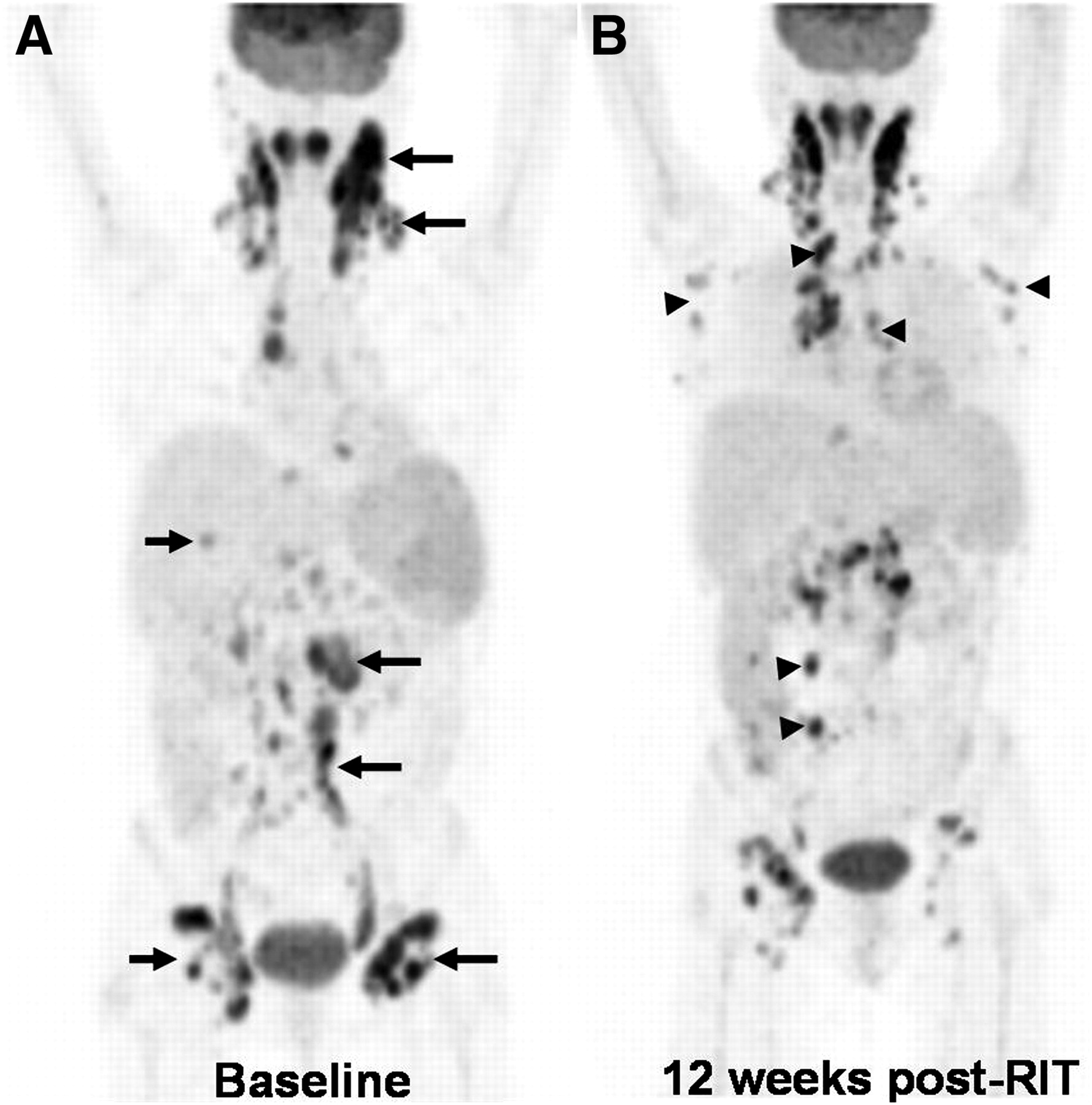
- FIGURE 2.
Heterogeneous response to radioimmunotherapy. A 58-y-old woman with grade 3, follicular NHL status after first-line chemotherapy, rituximab alone, and salvage chemotherapy presented with progressive NHL. Baseline 18F-FDG PET scan (A) revealed 18F-FDG–avid adenopathy in mediastinum, bilateral tonsillar, cervical, paraaortic, and inguinal regions (arrows), indicating active NHL. Spleen was also enlarged, with moderately increased 18F-FDG activity suggestive of lymphomatous involvement. Patient received 65-cGy total-body radiation dose of 131I-tositumomab. 18F-FDG PET scan at 12 wk after therapy (B) revealed decreased 18F-FDG activity in some target lesions (A, arrows), but others increased and new lesions developed (B, arrowheads).
- FIGURE 3.
OS vs. 12-wk response. (A) Response (CR/PR) at 12 wk after radioimmunotherapy is associated with significantly longer OS, compared with no response (SD/PD), by both IWC and IWC-PET. (B) OS was not significantly longer for patients with CR by IWC-PET vs. no CR. PFS tended to be longer for CR group.
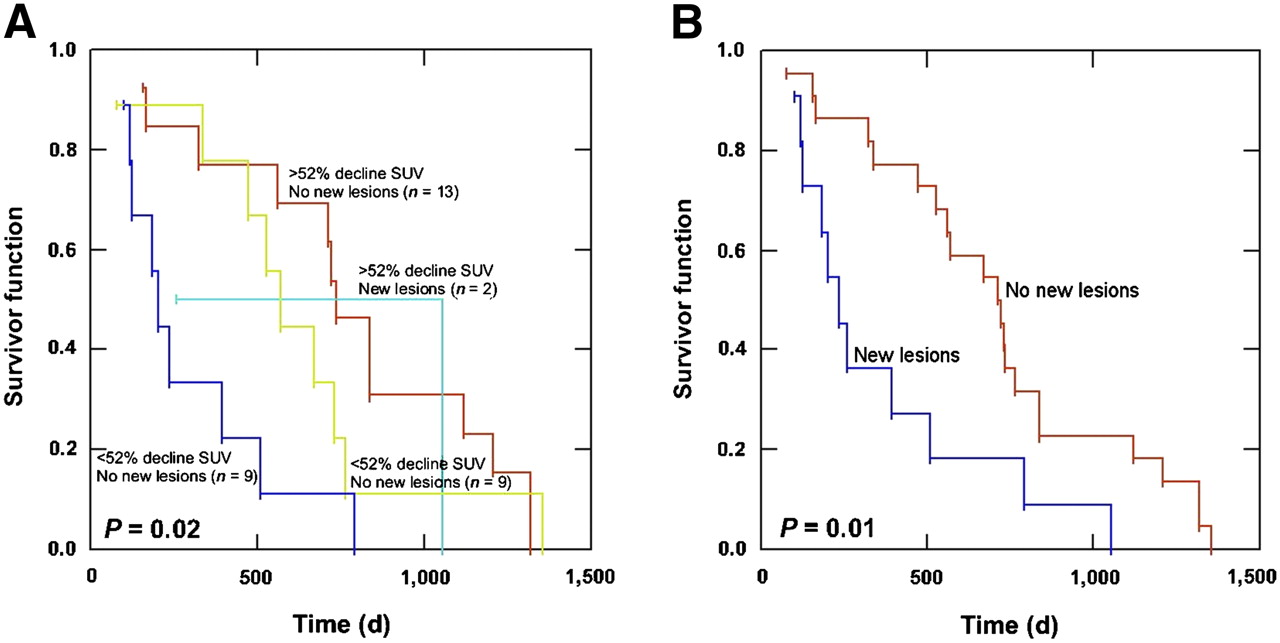
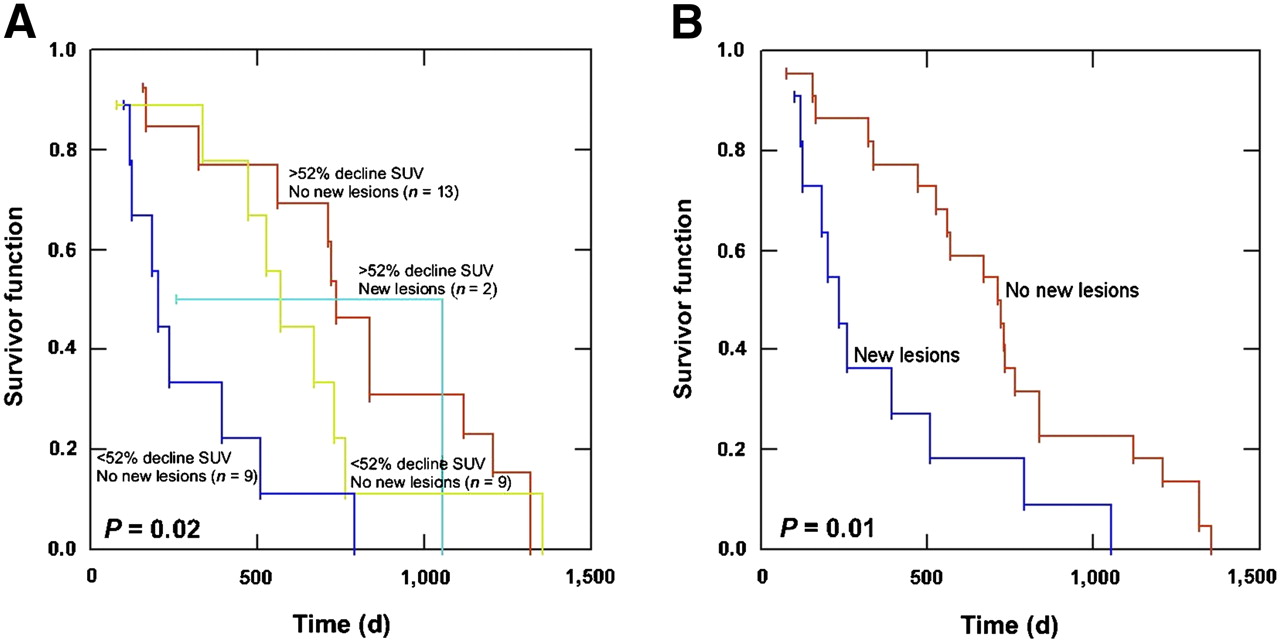
- FIGURE 4.
OS vs. percentage change in SUVlean max and new lesions. (A) OS is longer for patients with decline in SUVlean max greater than 52% and no new lesions (n = 13) than for those with decline in SUVlean max less than 52% and new lesions (n = 9). In patients without new lesions at 12 wk after radioimmunotherapy, there was no significant difference in OS based on percentage change in SUVlean max greater or less than 52% (P = 0.89). (B) OS was better for patients without new lesions on 12-wk PET scan than for those with new lesions (P = 0.01).
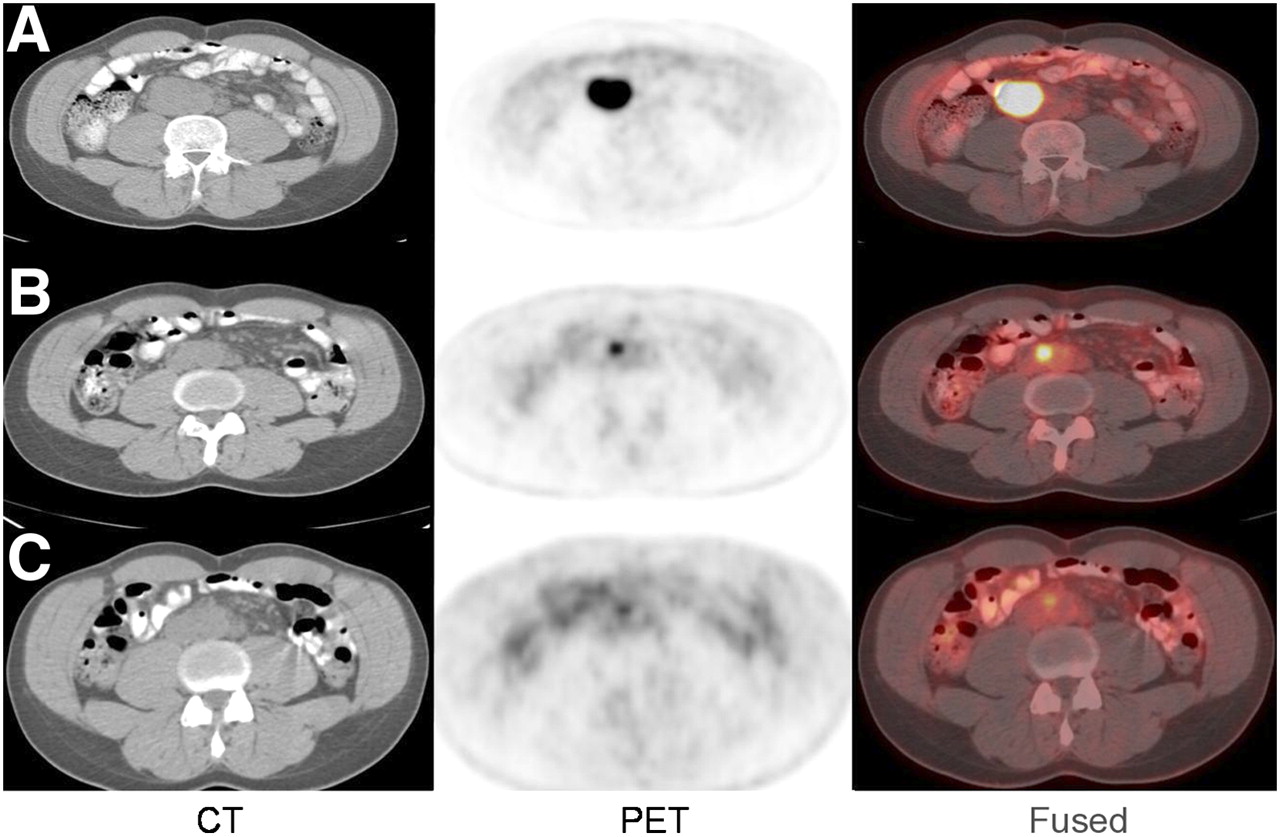
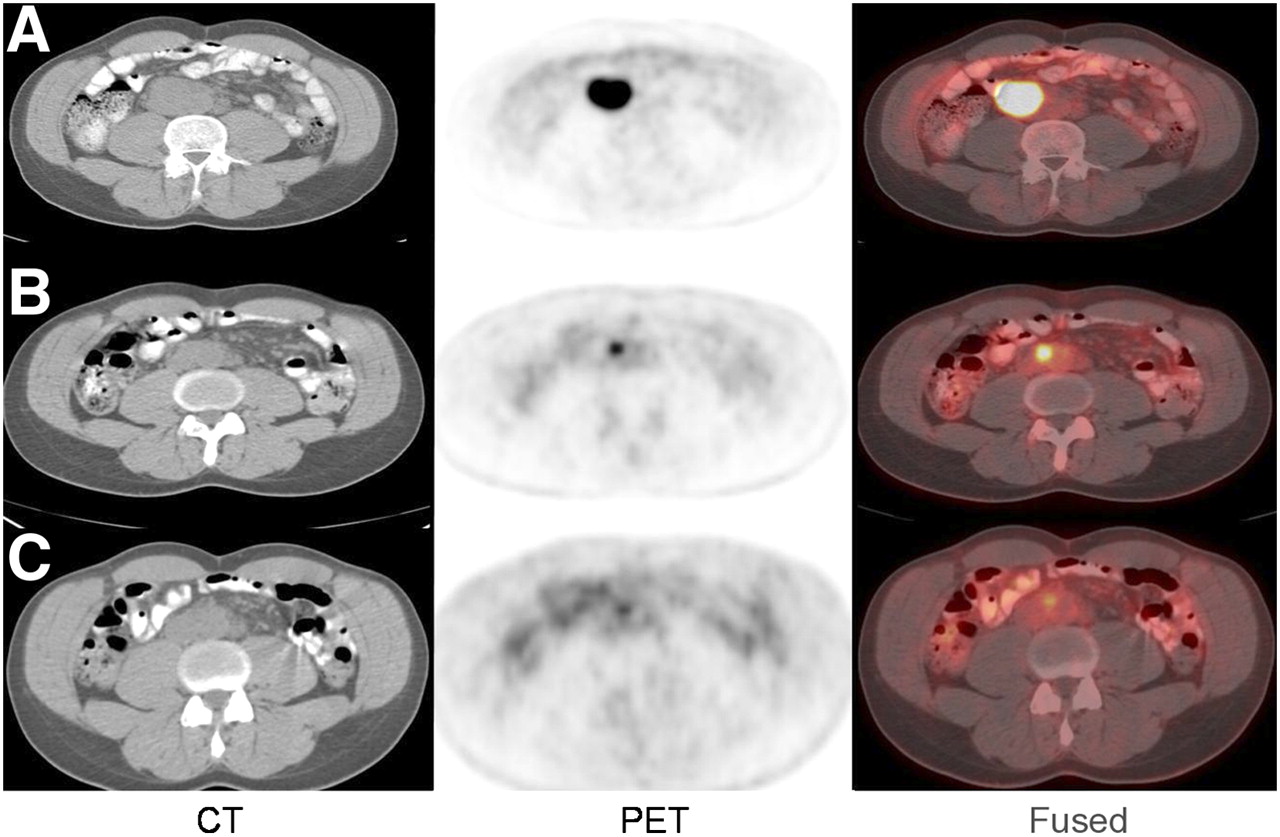
- FIGURE 5.
Gradual decline in metabolic activity after radioimmunotherapy. A 41-y-old man with low-grade follicular NHL status after R-CHOP and ICE chemotherapy and myeloablative allotransplant presented with enlarging aortocaval lymph node. Baseline 18F-FDG PET/CT scan (A) before radioimmunotherapy demonstrated 4.8 × 3.6 cm aortocaval lymph node with SUVlean max of 13.3. A 55-cGy total-body radiation dose of 131I-tositumomab was administered because of patient's history of transplant. Follow-up 18F-FDG PET/CT scans at 12 (B) and 24 (C) wk after radioimmunotherapy demonstrated gradual decline in size (1.8 × 1.3 and 1.2 × 0.7 cm) and metabolic activity (SUVlean max, 4.42 and 2.72) of lymph node. Patient underwent additional 18F-FDG PET/CT scan that demonstrated no change in metabolic activity of aortocaval node from 24-wk scan. He remains without evidence of active NHL 28 mo after radioimmunotherapy.

Tables
Characteristic All patients (n = 33) 131I-tositumomab (n = 23) 90Y-ibritumomab tiuxetan (n = 10) P* Sex (M/F) 23/10 16/7 7/3 >0.99 Median age (y) 63 (31–79) 63 (31–79) 64.5 (40–73) 0.95† NHL histologies Grade I/II follicular 19 12 7 0.46 Grade III follicular 4 4 0 Small lymphocytic 2 2 0 Marginal zone 2 1 1 Mantle cell 1 1 0 Transformed large B cell 5 3 2 0.63 Median number of prior chemotherapies 3 (1–8) 3 (1–8) 2 (1–7) 0.40† Prior history of… Rituximab 32 22 10 >0.99 External-beam radiation 10 9 1 0.12 Transplantation 3 3 0 0.54 Stage at radioimmunotherapy >0.99 I/II 5 4 1 III/IV 28 19 9 Tumor size (mean SPD, mm2) 5,432 ± 4,843 4,375 ± 3,854 7,863 ± 6,138 0.06 Bone marrow involvement at time of radioimmunotherapy 6 5 1 0.64 Radioimmunotherapy dosage Full 23 15 8 Attenuated 10 8 2 0.68 Response to radioimmunotherapy Patient no. Histology Agent/dosage IWC IWC-PET Follow-up 1 Follicular, grade 3 131I-tositumomab (55 cGy) CRu PR Continued decline in 18F-FDG activity to CR on 24-wk PET without additional therapy. Nonmyeloablative allotransplant for myelodysplastic syndrome and remains in CR for NHL at 27.8 mo after radioimmunotherapy. 2 Mantle 131I-tositumomab (75 cGy) SD PD Progressive lymphoma at 5.3 mo after radioimmunotherapy. Expired 15.7 mo after radioimmunotherapy. No interval follow-up between date of progression and death. 3 Follicular, grade 2 90Y-ibritumomab tiuxetan (14.8 MBq/kg [0.4 mCi/kg]) CR PR Additional therapy unknown. Expired 24.2 mo after radioimmunotherapy; lymphoma status unknown. 4 Low-grade follicular 90Y-ibritumomab tiuxetan (14.8 MBq/kg [0.4 mCi/kg]) SD CR No additional therapy. PD by PET/CT 8.9 mo after radioimmunotherapy. Remains asymptomatic at 18.7 mo after radioimmunotherapy. 5 Follicular, grade 2 131I-tositumomab (75 cGy) PR CR No additional therapy and disease-free 15.5 mo after radioimmunotherapy. PD after retreatment with 131I-tositumomab; transplant with disease at 24.5 mo after initial radioimmunotherapy. 131I-tositumomab (n = 23) 90Y-ibritumomab tiuxetan (n = 10) P* SUVlean max Baseline 6.68 ± 4.42 6.16 ± 3.15 0.35 12 wk after radioimmunotherapy 4.14 ± 4.57† 3.54 ± 4.06† 0.32 SPD (mm2) Baseline 4,375 ± 3,854 7,863 ± 6,138 0.06 12 wk after radioimmunotherapy 2,669 ± 3,573† 2,983 ± 2,733† 0.81 Percentage change SUVlean max −31% ± 51% −47% ± 46% 0.38 SPD (mm2) −39% ± 43% −63% ± 32% 0.13





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prediction of Response to Immune Checkpoint Inhibitor Therapy Using Early-Time-Point 18F-FDG PET/CT Imaging in Patients with Advanced Melanoma
- End-Therapy Positron Emission Tomography for Treatment Response Assessment in Follicular Lymphoma: A Systematic Review and Meta-analysis
- Expert Opinions on Positron Emission Tomography and Computed Tomography Imaging in Lymphoma
- From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors