


Abstract
131I treatment in thyroid cancer patients may induce side effects, including extrathyroidal cancer and leukemia. There are still some uncertainties concerning parameters that may influence the effective half-life of 131I and the absorbed doses by extrathyroidal organs. Methods: Whole-body retention of radioiodine was measured in 254 patients, and repeated quantitative whole-body scans and measurements of the urinary excretion of 131I were performed on 30 of these patients. Results: The mean effective half-life (10.5 h) was shorter by 31%, with little difference between patients, in the 36 patients who received recombinant human thyroid-stimulating hormone than in the 218 patients who underwent thyroid hormone withdrawal (15.7 h). The residence times in the stomach and in the rest of the body were significantly shorter in patients who received recombinant human thyroid-stimulating hormone than in patients who underwent withdrawal, but the residence times were similar in the colon and bladder. Conclusion: In patients who undergo thyroid hormone withdrawal, the longer mean effective half-life is mainly due to delayed renal excretion of 131I and results in dose estimates higher than the data in report 53 of the International Commission on Radiological Protection, which were obtained from healthy, euthyroid subjects.
Radioiodine (131I) is used in thyroid cancer patients to ablate normal thyroid remnants after total thyroidectomy and to treat patients with persistent or recurrent disease (1–3). In these patients, the efficacy of radioiodine treatment has been related to the radiation dose delivered to normal and neoplastic thyroid tissues (4–6). However, the significant radiation doses delivered to extrathyroidal tissues may induce side effects such as nausea and vomiting, sialadenitis and xerostomia, loss of taste, bone marrow insufficiency, and late occurrence of extrathyroidal cancer and leukemia (7–10). Thus, treatment conditions should optimize the radiation dose delivered to normal and neoplastic thyroid tissues and should minimize the radiation dose delivered to extrathyroidal tissues.
In the absence of excess iodine, uptake of iodine in thyroid cells is mainly related to thyroid cell differentiation and the intensity of stimulation with thyroid-stimulating hormone (TSH) (6,11). In low-risk patients, normal thyroid remnants are ablated with radioiodine either after thyroid hormone withdrawal under hypothyroid conditions or after injections of recombinant human TSH (rhTSH) under euthyroid conditions (12–14). In patients with known persistent neoplastic foci, radioiodine treatment is preferably administered after thyroid hormone withdrawal, because no data have yet shown that the same range of radiation dose can be delivered to neoplastic foci with rhTSH (15).
The radiation doses delivered to normal and neoplastic thyroid tissue are frequently estimated in clinical practice (4–6,15–18). Also, the radiation dose to the blood is estimated when dosimetry is performed to estimate the optimal activity to be administered (16,17), but often, little attention is paid to radiation doses to extrathyroidal tissues. Thus, except for a single recent paper (19), only scarce and incomplete data are available.
To calculate doses absorbed by extrathyroidal tissues (i.e., organs), the MIRD formalism (20) is well adapted for protection evaluation purposes. To implement this method, 2 types of data are needed: S factors, which are related to the geometric modeling of the body and to radioactive decay, and residence time (τ), which reflects the biologic behavior of a radiopharmaceutical compound. Residence time is equal to the total cumulated activity in the organ divided by the total administered activity. There is no need for discussion of S factors, but residence times must be carefully considered. For instance, data published in report 53 of the International Commission on Radiological Protection (ICRP) (21) can be used for dose estimates in healthy subjects. However, these data may be irrelevant in thyroid cancer patients, for the following reasons: during hypothyroidism after thyroid hormone withdrawal, renal clearance of radioiodine is decreased, potentially prolonging its retention in the body; when used in a high activity for therapy, radioiodine may have a biodistribution different from that when used in a much lower activity for diagnosis; morphology may be different among patients; uptake may be present in metastases; and finally, data on the stomach and colon are missing from the ICRP 53 report for patients with no thyroid uptake.
This study was performed on thyroid cancer patients who were treated with radioiodine after either thyroid hormone withdrawal or rhTSH injections. Three types of measurements were performed: whole-body counting, in 254 patients, and quantitative whole-body scans and total urinary excretion of radioiodine, in 30 patients. We studied differences in 131I whole-body retention between rhTSH patients and withdrawal patients and the potential relationships with patient characteristics. Then, we provided dosimetry data on organs clearly identified as both source and target, that is, stomach, large intestine, bladder, and whole body (remainder of the body).
MATERIALS AND METHODS
Patients
Between December 2004 and June 2007, 254 thyroid cancer patients who were treated with radioiodine at Institut Gustave Roussy were prospectively enrolled in the study. Among them, 218 patients were treated after thyroid hormone withdrawal and 36 after injections of rhTSH.
Thyroid hormone withdrawal consisted of the withdrawal of levothyroxine for 5 wk, the administration of triiodothyronine for 3 wk, and the total withdrawal of thyroid hormone treatment for 2 wk, with the aim of obtaining a serum TSH level above 30 mU/L on the day of 131I administration. rhTSH (0.9 mg of rhTSH [Thyrogen]; Genzyme Therapeutics) was injected intramuscularly for 2 consecutive days, and radioiodine was administered on the day after the second injection of rhTSH, levothyroxine treatment being maintained during the procedure.
The patients received oral and written information concerning 131I treatment and radioprotection. 131I was administered as capsules (Capsion; Schering Cis-Bio). For 234 patients, the administered activity was 3,700 MBq (100 mCi); and for 20 patients with low-risk cancer, the administered activity was 1,110 MBq (30 mCi). The patients were hospitalized for 2.5–3 d in protected rooms in the Department of Nuclear Medicine. Abundant hydration and laxative treatment were given during hospitalization.
Measurement of Whole-Body Retention
The whole-body retention of 131I was measured by a probe fixed on the ceiling of each protected room. The probe (ARIES; Ludlum Measurements) is made of a scintillator, NaI(Tl), coupled to a photomultiplier tube and connected to a computer for data acquisition and management. An adapted collimator defines a rectangular field of view over the patient's bed. For each patient, all measurements were performed by the same probe and with the same distance between the ceiling and the bed. An alarm advised the patient when the measurement was going to start and stop. At least 7 measurements were performed per patient after 131I administration: at 0.5 h (before any urinary elimination), at 2 h, and then every 12 h (i.e., at 14, 26, 38, 50, and 62 h). Results were corrected for counting losses due to the high initial activity.
Urine Samples and Biodistribution of Radioiodine
Additional investigations were performed on 19 withdrawal patients and 11 rhTSH patients and consisted of collection of urine samples and repeated whole-body scans.
For urine collection, a urine sample was collected after each miction, with the patient recording the day and hour of sampling and the urination volume. The radioactivity of each sample was measured with a calibrated γ-counter (LKB 1282 CompuGamma; Wallac).
Repeated whole-body scans were obtained using a calibrated dual-head γ-camera (AXIS; Philips, 19-mm-thick crystal) on days 1, 2, and 3 after radioiodine administration. The camera was calibrated using activities comparable to those encountered in patients on day 1 after radioiodine administration. From a practical point of view, a phantom mimicking the abdominal area was used to quantify the saturation of the detector. During the calibration procedure, regions of interest were drawn on the geometric mean of the anterior and posterior views to determine the relationship between the activity present in the region of interest and the total number of counts. To provide unbiased results, the raw clinical data were corrected using this relationship.
Dosimetry Analysis
When a particular organ is considered, residence time can be used to evaluate the “dosimetry status” of a radiopharmaceutical compound.
From the 3 sets of available data (whole-body retention, whole-body scans, and urinary excretion), it was possible to extract dosimetry data on the organs of interest. Data on whole-body retention were obtained from total-body counting; data on stomach and large intestine were obtained from quantitative whole-body scans; data on bladder were derived from urinary measurements; and data on remainder of body were calculated by combining all these data. To fit experimental measurements, we used a conventional least-squares algorithm (KaleidaGraph; Synergy Software). Depending on the organ, a mono-, bi-, or multiexponential model was implemented. OLINDA software (Vanderbilt University) provided dosimetry calculations when necessary.
Regarding the reproducibility of the results, we mainly had to consider the region-of-interest determination, because geometry has been defined from standard woman and man models. Two operators performed masked calculations using 6 patients, and the results for the two were similar, showing that the results were reproducible.
After 2.5 d (60 h), the patients were discharged from the hospital because about 90% of the total administered activity had been eliminated. Data that were missing due to the absence of subsequent measurements were then extrapolated from the mathematic fits.
Statistics
Quantitative data were expressed as means and SDs, and qualitative data were expressed as percentages. Significant differences between groups were sought with a χ2 test. A univariate linear regression analysis using the individual characteristics of patients was performed to identify variables influencing the effective half-life of radioiodine. The influence of parameters such as age, sex, serum creatinine, serum thyroglobulin level, serum TSH level, number of previous radioiodine treatments, histology, and TNM classification was studied. A nonparametric test (Kruskal–Wallis) was used when fewer than 30 patients were involved, and no hypothesis on the distribution of our data had been made. All statistical analyses were performed with SAS software, version 9.1.
RESULTS
Patients
The effective half-life in the body—that is, the time required for the amount of a radioactive element deposited in a living organism to be divided by a factor of 2, from the combined action of physical decay and biologic disappearance—was not dependent on the administered activity (3.7 or 1.1 GBq), and the 254 patients were pooled for the analysis.
Because the stimulation method (thyroid hormone withdrawal or rhTSH) may have an important effect on whole-body retention of radioiodine, the 254 patients were studied according to the stimulation method used (Table 1) (4,12,22).
Effective Half-Life: Comparison Between Withdrawal Patients and rhTSH Patients
In the 218 withdrawal patients (Table 2), the mean effective half-life was 15.7 h and was not related to age at the time of the study (P = 0.2), serum TSH level (P = 0.8), or number of previous treatments with 131I (P = 0.9). A longer mean effective half-life was associated with the male sex (P = 0.02), a higher serum creatinine level (P = 0.0001), a follicular histology of thyroid cancer (P = 0.016), a higher serum thyroglobulin level (P = 0.018), and the presence of metastases (P = 0.03).
Univariate Analysis: Relationship Between Patient Characteristics and Effective Half-Life After Either Thyroid Hormone Withdrawal or rhTSH Injections
Because rhTSH is used for ablation only in low-risk patients and because the presence of metastases was associated with a longer effective half-life, we individualized the 167 withdrawal patients who had no distant metastases and who had a T1–T3 tumor. In these 167 patients, the mean effective half-life was longer by 31% than in the 36 comparable patients who received rhTSH, at 15.2 and 10.5 h, respectively (P = 0.0001). Of interest, the SD of the mean effective half-life was smaller in patients who received rhTSH than in those who underwent thyroid hormone withdrawal, at 1.5 and 4.7 h, respectively (P = 0.0001). Among these 167 withdrawal patients, a higher serum creatinine level was associated with a longer effective half-life (P = 0.0002); indeed, the mean creatinine clearance was lower in withdrawal patients than in rhTSH patients.
Dosimetry Analysis
Dosimetry was analyzed for the 30 patients who underwent repeated whole-body scans. The mean effective half-life was 10.6 h for the 11 patients who received rhTSH and 16.0 h for the 19 patients who underwent withdrawal (P = 0.0006), similar to those for the corresponding patients in the entire series (Table 3).
Residence Time (Hours): Comparison Between Withdrawal Patients, rhTSH Patients, and ICRP 53 Reference
The whole-body residence time was 15.2 h in rhTSH patients—significantly shorter than the 23.0 h observed in withdrawal patients.
The residence time in the stomach was significantly shorter in rhTSH patients than in withdrawal patients (P = 0.01), whereas no difference appeared for colon (P = 0.07), bladder (P = 0.9), or breast (P = 0.53). Regarding the remainder of the body, the residence time was shorter in rhTSH patients (P = 0.04) (Table 3).
In rhTSH patients, dose estimates were lower for the stomach (P = 0.009), were of borderline significance for the upper large intestine (P = 0.05) and the bone marrow (P = 0.05), and were not different for the lower large intestine (P = 0.09) or ovaries (P = 0.26) (Table 4).
Dosimetry (mGy/MBq) Estimation: Comparison Between Withdrawal Patients, rhTSH Patients, and ICRP 53 Reference
As shown in Figure 1, iodine urinary excretion was slower in withdrawal patients than in rhTSH patients, with an excretion of 1,800 MBq being achieved at 15.6 and 10.3 h, respectively.
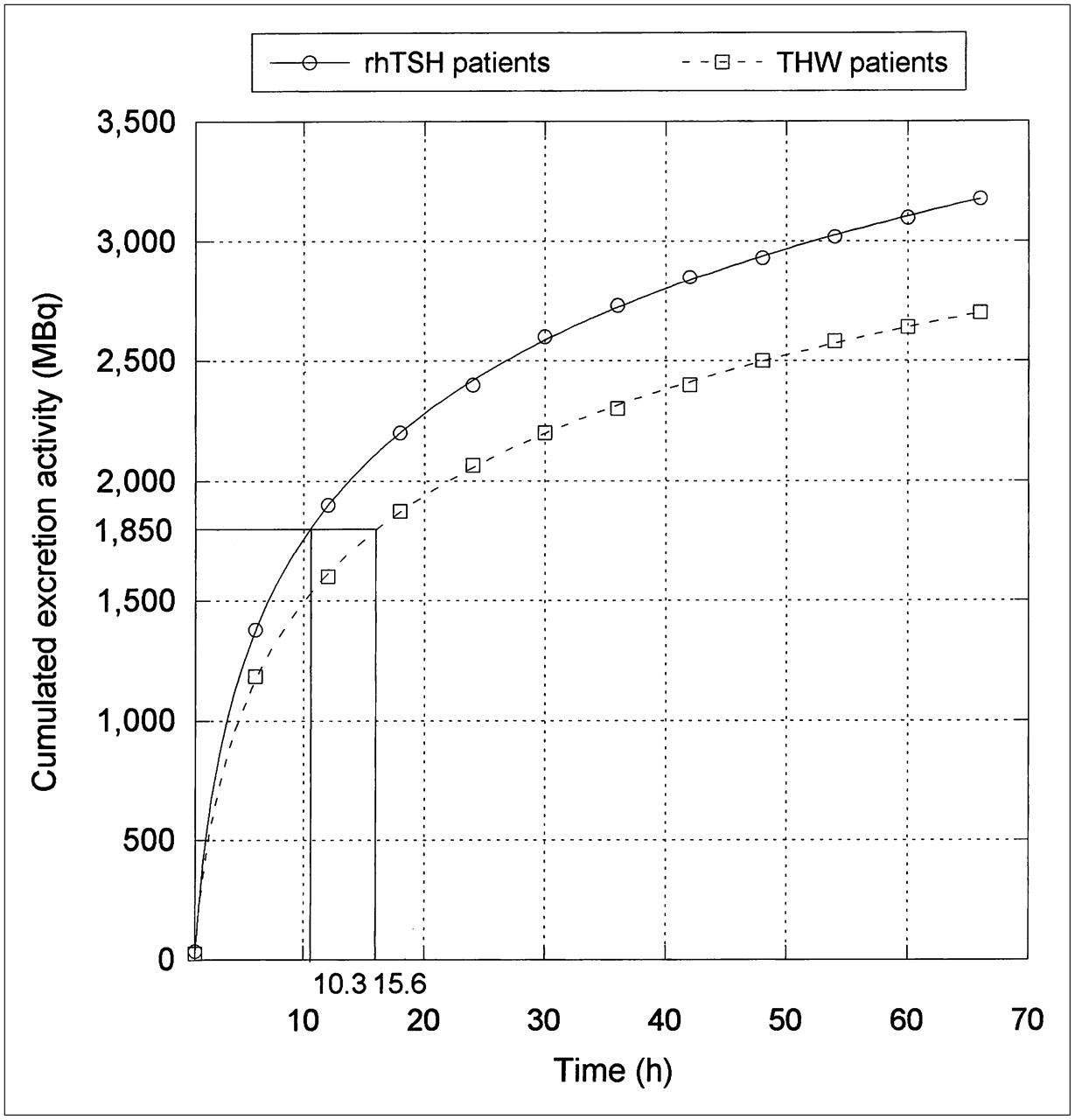
Cumulated urinary excretion activity: comparison between withdrawal patients (THW) and rhTSH patients.
DISCUSSION
ICRP data are usually considered the standard in the field of internal dosimetry but do not provide any powerful information when residence times are needed for calculations after therapeutic administration. The method based on whole-body retention, quantitative whole-body scanning, and urinary radioactive measurements was implemented to determine residence times and appeared reliable and easy to perform. In particular, the patient's contribution to urinary sampling was priceless and avoided the need to study urinary excretion from pooled volumes, as is usually done.
The effective half-life in the 218 patients who underwent withdrawal was 15.7 h, in accordance with previously reported data (22,23). Among this group of patients, the effective half-life was longer in those with distant metastases or a T4 tumor and in those with elevated serum thyroglobulin levels (that indicate the persistence of thyroid tissue), relative to the radioiodine uptake in normal or neoplastic thyroid tissue. Similarly, male patients and those with follicular carcinoma may also have more extensive disease than female patients and those with papillary carcinoma.
RhTSH is used in low-risk patients, and for comparison, we individualized among patients who underwent withdrawal a group of 167 low-risk patients who had no initial distant metastases and who had a T1–T3 tumor. The mean effective half-life was significantly longer, by 31%, in patients who underwent withdrawal than in those treated with rhTSH. This difference was mainly due to a delayed urinary excretion of 131I during hypothyroidism, as shown by urinary excretion measurements. In addition, a narrower distribution of individual effective half-lives was observed in patients who received rhTSH. From a practical point of view, in countries where regulations specify a maximal value of residual activity above which the patient must be hospitalized in a dedicated room, discharge from the hospital may occur earlier and can be more easily predicted, thus partially compensating for the rhTSH acquisition cost (24). In countries with no such restrictions, this narrow distribution eases patient management after radioiodine administration, through imposing fewer rules on the patient's daily life.
RhTSH has already proved its benefit in avoiding hypothyroidism and in maintaining quality of life (11,25–27). Our data confirm that a further advantage of using rhTSH is that it reduces by about one third the amount of radiation to which the body is exposed (12). The dosimetry study confirms previous reports on body retention (4) and on estimated doses to the blood and bone marrow and that the whole-body residence time is shorter in patients treated with rhTSH than in those who undergo withdrawal, in whom residence time was longer than the 11.1 h reported in the ICRP 53 report (21). In a study by Hänscheid et al. (4), patients without metastasis were randomized after thyroidectomy to either the withdrawal group or the rhTSH group, and residence time in the whole body and in thyroid remnants and absorbed dose to the blood were calculated. In the present study performed on consecutive patients, the aim of the dosimetry study during radioiodine treatment was to obtain residence time data in source or target healthy organs such as colon and thus to complete the ICRP 53 data. In both studies, the mean whole-body residence time was shorter in rhTSH patients (17.3 ± 3.9 h and 15.2 ± 3.1 h, respectively) than in withdrawal patients (24.1 ± 7.8 h and 23.0 ± 7.7 h, respectively). Thus, these 2 studies were complementary and provided similar results.
The present study revealed similar residence times in the bladder, because most radioiodine is eliminated in the urine under both euthyroid and hypothyroid conditions; doses to the ovaries, delivered mostly by activity in the bladder, were also similar under both conditions. In the stomach, the residence time was significantly shorter with rhTSH and may have been related to a lower bioavailability of radioiodine, because most radioiodine in the stomach is concentrated from the blood; residence time was not different in the colon, at least in part because the routine use of laxative treatment in all patients after withdrawal decreased radioiodine accumulation in the colon. Residence time was not different in the breast (P = 0.53), because the self–β-irradiation is low compared with that due to the γ-rays from external sources. Considering the geometry, this result is easily predictable because the sources of irradiation are large and not near the breast. Our dose estimates are higher than those in the ICRP 53 report, which were obtained in healthy, euthyroid patients with intravenous injection of a low activity of 131I (21). In fact, our patients received oral treatment with a large activity of 131I; thyroid uptake was either low or absent, and those treated after withdrawal were hypothyroid.
Our methodology is quite different from the one implemented by Kolbert et al. (19). In that robust and rigorous study, the authors dealt with absorbed doses to normal organs using a complementary imaging modality such as PET/CT or CT, and results were provided for organs in the investigated fields. In our study, data were derived from actual high-activity physiologic images to individualize the most significant source organs, to quantify global uptake for each organ, and finally to calculate the residence time. Another major difference is the way in which the absorbed dose was calculated, either through voxelized dedicated software (3D-ID; Memorial Sloan-Kettering Cancer Center) (19) or through OLINDA without any organ resizing. By doing that, we deliberately considered dosimetry for normal organs from a protection point of view rather than the clinical viewpoint of Kolbert's approach. Of course, findings from these 2 approaches cannot be directly compared, but both aimed to improve our knowledge of extrathyroidal organ dosimetry.
CONCLUSION
In euthyroid patients treated with rhTSH, mean 131I effective half-life is shorter by 31% than in hypothyroid patients who undergo withdrawal and is similar among patients. This treatment decreases the radiation doses delivered to extrathyroidal tissues and permits a shorter and more predictable length of hospitalization.
Acknowledgments
This study was supported by unrestricted grants from Genzyme Corporation and Electricité de France.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 6, 2008.
- Accepted for publication May 16, 2008.





{kind=link}
Jump to section
Related Articles
Cited By...
- Analysis of Radiometry on Patients Undergoing Radioactive Iodine Therapy
- Thyroid Uptake and Effective Half-Life of Radioiodine in Thyroid Cancer Patients at Radioiodine Therapy and Follow-Up Whole-Body Scintigraphy Either in Hypothyroidism or Under rhTSH
- Recombinant human thyrotropin preparation for adjuvant radioiodine treatment in children and adolescents with differentiated thyroid cancer
- Dosimetry and thyroid cancer: the individual dosage of radioiodine
- Influence of Vitamin C on Salivary Absorbed Dose of 131I in Thyroid Cancer Patients: A Prospective, Randomized, Single-Blind, Controlled Trial