


Abstract
Apart from the common causes of thyrotoxicosis, such as Graves' disease and functioning nodular goiters, there are more than 20 less common causes of elevated free thyroid hormones that produce the symptoms and signs of thyrotoxicosis. This review describes these rarer conditions and includes 14 illustrative patients. Thyrotropin and free thyroxine should be measured and, when the latter is normal, the free triiodothyronine level should be obtained. Measurement of the uptake of 123I is recommended for most patients.
Thyrotoxicosis is the syndrome caused by an excess of free thyroid hormones. Any or all systems of the body can be affected. The symptoms and signs depend on the degree of elevation of the hormones, the length of time that they have been elevated, the rate at which the hormone levels rose, and individual variations of patients. For example, a patient with ischemic heart disease is more likely to exhibit cardiac manifestations. The terms “hyperthyroidism” and “thyrotoxicosis” are often used interchangeably; however, hyperthyroidism means that the thyroid gland is functioning more than normal. Therefore, a hyperthyroid patient is thyrotoxic, but a thyrotoxic patient need not have an overactive thyroid and is therefore not actually hyperthyroid. Iagaru and McDougall discussed the treatment of thyrotoxicosis, focusing on common diseases, such as Graves' disease and toxic nodular disorders (1). In this article, we describe rare causes of thyrotoxicosis. Nuclear medicine physicians will not encounter these often; however, knowledge of the disorders, including how to diagnose and manage them, is important. Several of the conditions are self-limiting and do not need prolonged treatment.
When a patient is thought to be thyrotoxic, a convenient algorithm is to measure free thyroxine (free T4) and thyrotropin (TSH). When the former is higher than normal but the latter is suppressed, thyrotoxicosis is diagnosed. When the former is normal but TSH is low, it is valuable to measure free triiodothyronine (free T3); when the latter is abnormally high, the diagnosis is T3 toxicosis (2–4). When both free hormones are normal but TSH is low, the term “subclinical thyrotoxicosis” can be applied (5). Once it has been determined that thyrotoxicosis is present, measurement of 123I uptake can differentiate among several disorders (Table 1). Some have high uptake and, paradoxically, some have low uptake. This distinction is important because most disorders in the latter group are self-limiting and do not require treatment with 131I or antithyroid medications. In contrast, those with high uptake usually do require therapy. It should be recognized that the site of high uptake might not be in the expected site of the thyroid.
Unusual Causes of Thyrotoxicosis
Conditions associated with elevated uptake of radioiodine are addressed first (6). Several disorders are illustrated by case reports. The description of each group of thyrotoxic conditions is followed by a discussion relevant to those specific disorders. At the end of the article, there is no repetition of the discussions, but there is a “Conclusion” section. Routine cases of Graves' disease and toxic nodular goiters are not discussed.
UNCOMMON CAUSES OF THYROTOXICOSIS WITH INCREASED UPTAKE OF RADIOIODINE
Thyrotoxicosis in Newborns
Examples.
Patient 1 was a newborn baby who was irritable and restless. He had sinus tachycardia. Although the mother had been a patient at Stanford University Medical Center, the obstetric care and delivery were provided at a different medical facility. Four days after delivery, the physicians noted that the mother had a thyroidectomy scar and determined that she had been treated for Graves' hyperthyroidism. She had a distant history of weight loss, shaking, palpitations, sweating, and irritation of her eyes. Free T4 was high, TSH was suppressed, and she had been treated with propylthiouracil. She developed severe thyroid orbitopathy, which was treated with high doses of prednisone and external beam radiation. She also had pretibial dermopathy. The patient elected to have a thyroidectomy so that she could conceive as early as possible because she was 35 y old. The baby was then diagnosed with neonatal Graves' disease, which was confirmed by thyroid function tests. Propylthiouracil and propranolol were administered for 4 wk. The baby then required no therapy for thyrotoxicosis. In retrospect, in utero the baby had been noted to have persistent tachycardia. This baby has neonatal Graves' disease.
Patient 2 had failure to thrive from birth. It was considered that the mother was not feeding him, but thyrotoxicosis was diagnosed when he was 8 wk of age. Antithyroid antibodies, including antithyroglobulin, antithyroperoxidase, and thyroid-stimulating immunoglobulin (TSI), were negative. His mother had an enlarged thyroid but normal thyroid function and no history of Graves' hyperthyroidism. The baby was treated with antithyroid medications but remained thyrotoxic for 3 y and had a thyroidectomy at that age. He continued to be thyrotoxic, with elevated free T4 and suppressed TSH, and was treated with methimazole. As a result of persistent fetal and neonatal thyrotoxicosis, the patient had premature closure of skull sutures and deafness. At 12 y of age, a decision was made to treat the patient with radioiodine. Methimazole was stopped for 5 d, and imaging of the neck and trunk with 123I demonstrated uptake only in the thyroid bed. He was treated with 460 MBq (12.5 mCi) of 131I and is now taking replacement l-thyroxine. This patient has constitutively activated TSH receptors.
Discussion.
Thyrotoxicosis in neonates is very uncommon (7). When a baby is exposed to high levels of free thyroid hormones in utero, it is at increased risk of being born prematurely or small, and fetal mortality is increased. Premature closure of cranial sutures and reduced intelligence are noted, and cardiac failure can occur. The most likely cause of hyperthyroidism in a newborn is neonatal Graves' disease attributable to passive transplacental transfer of thyroid-stimulating antibodies from mother to baby, as was the case in patient 1. In this siuation, the maternal level of TSI, an IgG antibody, is high and remains elevated during the pregnancy (8–10). In contrast, in most pregnant patients with Graves' disease, the levels of TSI decrease as the pregnancy progresses. Maternal antibodies, both good and bad, are passively transferred to the fetus. The mother can be euthyroid and, if so, usually has been treated for Graves' hyperthyroidism (11). Guidelines indicate that measurement of TSH receptor antibodies should be obtained in a patient who has had surgery or 131I for Graves' hyperthyroidism or who is taking antithyroid medications during pregnancy (12). Management of the baby in utero is beyond the scope of this article, but when the diagnosis is suggested, careful monitoring of the fetal size and heart rate and the size of the fetal thyroid by ultrasound is important (13).
Although the second patient was hyperthyroid from birth, he does not have neonatal Graves' disease. His mother did not have Graves' disease, there was no evidence of thyroid autoimmunity or abnormal thyroid function, and his disease persisted despite antithyroid medications and thyroidectomy. The cause is a mutation, usually substitution of one base in the DNA responsible for the production of the TSH receptor or the related G protein complex. This mutation results in activation of the TSH receptor without the presence of TSH or TSH-like stimulators, such as thyroid-stimulating antibodies. The patient now takes l-thyroxine after 131I therapy. Thyrotoxicosis in the case of an activated TSH receptor or G protein is permanent until all thyroid tissue has been removed (9,14,15).
A third cause of thyrotoxicosis in a newborn is the transfer of thyroid-stimulating antibodies in the mother's milk. We have not encountered this situation in practice (16).
Excess TSH
Examples.
Patient 3 was 41 y old when she was found to be thyrotoxic during pregnancy. Free T4 and free T3 were high, and TSH was normal. She had a diffusely enlarged thyroid. She was treated with propylthiouracil. Fourteen months after delivery, she was still hyperthyroid, and because TSH was measurable, there was a concern that the condition was secondary to a pituitary tumor. An MRI of the pituitary showed a macroadenoma, and she underwent transsphenoidal surgery that turned out to be incomplete. She continued to be thyrotoxic clinically and had elevated free hormones, but there was evidence of persistent TSH secretion. This patient does not have Graves' disease, but the cause of the hyperthyroidism is persistent TSH secretion from a pituitary adenoma.
Patient 4 was 55 y old when he was treated for thyroid cancer with thyroidectomy and 131I. Thereafter, the goal was to administer a dose of l-thyroxine that would keep his TSH at the low end of the normal range. Over a decade, his thyroid tests have consistently shown high free T4 and normal or high TSH (Table 2 shows representative values over 10 y). The patient is clinically mildly thyrotoxic, and he developed atrial fibrillation that is permanent. He is nervous and has difficulty sleeping. He has elevated free T4 at times when his TSH is well within normal or even elevated. At these times, he has worsening of the thyrotoxic symptoms. Follow-up whole-body scintiscans and serum thyroglobulin measurements indicate that there has been no recurrence of the cancer. This patient has pituitary resistance to thyroid hormones.
Free T4 and TSH Values in Patient Taking Exogenous Thyroxine and Exhibiting Symptoms and Signs of Thyrotoxicosis
Discussion.
These cases highlight examples of high TSH (17–19). TSH-secreting pituitary tumors are rare, occurring at a rate of approximately 1 in 1,000,000 in the general population and representing 1% or less of all pituitary adenomas (19–21). Most secrete TSH alone, although mixed hormonal secretion (growth hormone, prolactin and, rarely, gonadotropins) occurs in approximately 30% (22,23). Men and women are affected nearly equally. TSH-secreting adenomas have been associated with both multiple endocrine neoplasia type I and McCune–Albright syndrome (19,20). Most patients have symptoms of thyrotoxicosis for years before the diagnosis of a TSH-secreting pituitary tumor (21). The thyroid gland is palpably enlarged and often multinodular because of sustained TSH stimulation. Visual field defects (classically bitemporal hemianopia) are present in approximately 40%–50% of cases because of compression of the optic chiasm by the pituitary tumor. The key to the diagnosis of hyperthyroidism attributable to a pituitary adenoma is elevated thyroid hormone levels and detectable TSH levels. The biologic activity of the secreted TSH varies considerably; thus, serum immunoreactive TSH concentrations may range from normal (although inappropriately high given the presence of high free hormone levels) to markedly elevated (>500 mU/L). α-Subunit hypersecretion is seen in 66% of patients, and the molar ratio of the α-subunit to TSH is elevated in 80% of patients (24,25). In conjunction with typical laboratory results, MRI of the pituitary showing a mass lesion is usually diagnostic. Rarely, inferior petrosal sinus sampling for TSH is indicated when the results of MRI of the pituitary are normal. The most effective therapy is transsphenoidal resection of the pituitary tumor, which results in cure, improvement, or no change each in about one third of patients (25,26). External radiation and long-acting somatostatin analogs have been used (27–29). Treatment focused on the thyroid results in continued growth of the pituitary tumor. Nevertheless, there are reports of ablation of the thyroid rather than therapy of the pituitary adenoma, but careful long-term monitoring of the pituitary is important (30).
A particularly rare case was reported by Cooper and Wenig (31). The evidence suggested a TSH-secreting tumor, but studies of the pituitary were normal. The TSH was secreted by an ectopic nasopharyngeal pituitary tumor that was identified when the patient developed nasal obstruction.
The major differential diagnosis is resistance to thyroid hormones, which may be generalized or, in rare cases, selective to the pituitary gland (32,33). If the results of MRI of the pituitary are equivocal, then the differential diagnosis between a TSH-secreting tumor and resistance to thyroid hormones is made by administering thyrotropin-releasing hormone (TRH) (note that TRH is not available in the United States). Patients with a pituitary adenoma that autonomously produces TSH will have a blunted or absent TSH response to TRH stimulation, most likely because of the lack of TRH receptors on the adenoma itself (32). In addition, serum sex hormone–binding globulin concentrations are typically high in patients with TSH-secreting pituitary adenomas but normal in the syndrome of resistance to thyroid hormones.
Patient 4 appeared to have resistance to thyroid hormones at the pituitary level (34). His free hormone levels are normal or high, he has symptoms and signs of thyrotoxicosis, and his TSH levels are also normal or high. This condition can be difficult to manage, especially in a case like this one, in which the optimal TSH level for treating the thyroid cancer would be at the low end of the normal range. Another cause of thyrotoxicosis and elevated TSH has been reported by Pishdad et al (35). Their patient had been treated with methimazole for 14 y. Three months after discontinuation of the medication, the patient became thyrotoxic, but TSH was high. The condition spontaneously returned to normal. Their explanation was that the pituitary was hyperplastic after years of excess antithyroid therapy (the TSH level was 140 mU/L) and there continued to be an outpouring of TSH that caused hyperthyroidism.
In the presence of elevation of thyroid hormones, typical features of Graves' disease, and inappropriately high TSH but no evidence of pituitary disease, laboratory misinformation should be considered. Such misinformation could include heterophile antibodies interfering with the TSH assay (17).
Excess TSH-Like Material and Gestational Trophoblastic Diseases
Human chorionic gonadotropin (hCG) is a glycoprotein hormone that shares a common α-subunit with TSH, follicle-stimulating hormone, and luteininzing hormone but that has a specific β-subunit. hCG is synthesized primarily by syncytiotrophoblastic tissue, maintaining the corpus luteum and progesterone production in pregnancy (36,37). Receptors for the structurally similar glycoprotein hormones share significant homology in their extracellular binding domains, and hCG has confirmed thyroid-stimulating activity when present at high concentrations in serum because of a direct interaction of hCG with the TSH receptor (37–42).
Hydatidiform moles secrete large amounts of hCG, and the levels are proportional to the mass of the tumor. The values are severalfold higher than normal and can stimulate thyroid function (43). hCG secreted by a mole can also have greater thyrotropic potency than hCG secreted in normal pregnancy. Increased thyroid function in patients with hydatidiform moles can occur in 25%–64% of cases, but only 5% of cases have clinically significant thyrotoxicosis (44–46). Hydatidiform moles are most common in Asian and Latin American patients. In the United States, they occur in 0.5–2.5 per 1,000 pregnancies. The clinical presentation is usually vaginal bleeding, and the uterus is large for the date of the pregnancy. The diagnosis is confirmed by ultrasound, showing a pathognomonic “snowstorm” pattern and the absence of a fetus. Definitive treatment requires uterine evacuation of molar material by suction curettage or hysterotomy; the rapid decline in serum hCG levels is accompanied by a parallel decline in serum thyroid hormone levels.
Choriocarcinoma is a malignant tumor that is pathologically characterized by sheets of syncytiotrophoblastic and cytotrophoblastic cells, necrosis, and the absence of hydropic villi. Choriocarcinoma can invade blood vessels and progress to hemorrhagic metastases in distant organs such as the lungs and vagina. Its prevalence is 1 in 20,000 to 1 in 40,000 pregnancies in the United States and Europe (47). Approximately one half of choriocarcinomas occur in women who have had previous hydatidiform moles; however, only 3%–5% of women with moles develop choriocarcinomas (48). Rare cases of hyperthyroidism have also been reported in men with testicular choriocarcinoma (49). The usual treatment is chemotherapy and, as with a hydatidiform mole, cure of the choriocarcinoma results in a decline in hCG levels, and cure resolves the thyrotoxicosis. It can be necessary to treat the symptoms and signs of thyrotoxicosis before considering surgery (50).
New-onset thyrotoxicosis in pregnancy is usually attributable to Graves' disease, but if the clinical features are atypical and evidence of autoimmune thyroid disease is lacking, measurement of hCG and pelvic ultrasound are recommended. For completeness, it should be recognized that there can be a transient drop in TSH in normal pregnancy or in a pregnancy complicated by hyperemesis gravidarum because of high levels of hCG (51–53). When the free hormone levels are normal, the TSH level is low, and the patient has no symptoms or signs of thyrotoxicosis, it is wise to wait 3–4 wk and repeat the tests. If the TSH level improves, then no antithyroid therapy is advised.
High Uptake in Ectopic Sites
Struma ovarii is a teratoma of the ovary that is composed primarily of thyroid epithelium which, by definition, comprises more than 50% of its structure (54). Struma ovarii was first described in 1889, and fewer than 500 cases have been reported in the literature (55). Between 15% and 20% of ovarian tumors are of germ cell origin, and approximately 10% of these contain thyroid cells. A smaller percentage contain sufficient thyroid cells to be classified as struma ovarii (56). The lesion represents 0.3%–1% of all ovarian neoplasms and 2%–4% of all ovarian teratomas (57). It is most common in the fifth or sixth decade and is seen more often in countries in which goiter is endemic (58). Most struma ovarii lesions are benign, and it has been estimated that fewer than 3% are malignant (56).
Kempers et al. described 3 clinical situations for struma ovarii, asymptomatic, ascitic, and thyrotoxic (59). Ascites is evident in one third of the cases. Approximately 5%–20% of strumae produce significant amounts of thyroid hormones (60,61). The diagnosis should be considered in a patient with thyrotoxicosis, low radioiodine uptake over the thyroid, and a pelvic mass. Suspicion should be also raised in a patient who is thought to have silent thyroiditis and who fails to experience a hypothyroid phase (61). Most benign strumae accumulate iodine and occasionally (5%–20%) may even produce significant amounts of thyroid hormones and cause thyrotoxicosis. The common scenario is nonvisualization of the cervical thyroid gland during radioiodine or pertechnetate scintigraphy. Thyroiditis is the most common cause; however, imaging of the pelvis may reveal a functional structure situated in the region of one of the ovaries. Care must be taken not to mistake the bladder for struma ovarii or vice versa (62). SPECT/CT would be the ideal instrument for this investigation. This disease is rare, but when cervical uptake is negative, radionuclide imaging of the pelvis should be performed (55,61).
Sonographically, low-resistance blood flow within the tumor and free fluid in the pelvis are associated with a mature cystic teratoma (63). Struma ovarii should be included in the differential diagnosis of ovarian tumors when MRI shows a multicystic tumor with a solid component, a multilobulated surface, and signal intensities that indicate the presence of viscid gelatinous material (64,65).
Treatment of struma ovarii causing thyrotoxicosis is surgical excision. Antithyroid drugs can be used preoperatively to ameliorate thyrotoxic symptoms and signs, and surgery should be scheduled as soon as safely possible because of the concern of malignant transformation. β-Adrenergic blocking agents combined with iodine, ipodate, or iopanoic acid to block the T4-to-T3 conversion may be used in addition to thionamides to permit early surgery (61).
Thyrotoxicosis from Functioning Thyroid Cancer.
Thyroid cancer can cause thyrotoxicosis through 3 mechanisms: first, when there is a large volume of functioning cancer (usually of the follicular type); second, when there are activated receptors on the cancer cells; and third, when the cancer grows rapidly within the thyroid, invading and destroying thyroid follicles and releasing thyroid hormones (66). The first 2 mechanisms are discussed in this section, and the third is discussed along with pseudothyroiditis later in the article. In the first situation, there is almost always a large volume of functioning cancer. This might be a large primary lesion, and the cancer and thyrotoxicois might be cured by surgery. In the case described by Pont et al., the cancer weighed 900 g and produced only T3 (67). It is clear that such a primary cancer must be functioning, and this notion argues against the dogma that hot nodules are not thyroid cancers (68,69). Therefore, when a hot nodule has certain clinical characteristics, we recommend fine-needle aspiration, and when cytologic results are positive, thyroidectomy is recommended. More commonly, the patient has extensive functioning pulmonary or skeletal metastases or both (66,70–76). There are rare reports of metastastic cancer being stimulated by antibodies to the TSH receptor (77).
In patients with functioning metastases, 131I is the treatment of choice. However, care must be taken regarding the choice of dose because the cancer will produce large quantities of radiolabeled thyroid hormones that will result in prolonged radiation to the marrow and whole body. This is a situation in which dosimetry is recommended. The simple principles described by Sisson and Carey (78) and Sisson (79), taking into consideration the percentage of therapy retained and the level of free T4, have much merit. When a patient is clinically thyrotoxic, it is prudent to treat with antithyroid medications first, because 131I can cause a thyroid storm from an outpouring of thyroid hormones (80).
Thyrotoxicosis from Ectopic Thyroid.
Thyroid function in patients with ectopic thyroid is usually not elevated. However, there have been a few reports of elevated thyroid function. Sites of ectopic thyroid include the tongue, neck, and abdomen (81–83). The diagnosis is established by abnormal thyroid function test results and images demonstrating functioning thyroid tissue outside the cervical region. The treatment is surgical. It is important to prove that the ectopic tissue is not a metastasis by careful pathologic examination of the excised tissue.
Thyrotoxicosis with Low Uptake of Radioiodine
Examples.
Patient 5 was 62 y old when she developed pain in the front of her neck. The pain radiated to her jaw and ear and she consulted with an otolaryngeal consultant. She had fever and lost 2.25 kg in weight. Two months before she was seen at Stanford University Medical Center, her free T4 was 1.4 ng/dL, and her TSH was 0.55 mU/L. At the time of her evaluation, her free T4 was 3.0 ng/dL, and her TSH was 0.02 mU/L. The erythrocyte sedimentation rate was 105 mm/h. The 24-h uptake of 123I was 0.2%. Two months after that, her symptoms improved, and her free T4 and TSH were 0.69 ng/dL and 1.71 mU/L, respectively. Two weeks later, the values were 0.86 ng/dL and 11.7 mU/L, respectively. Subsequently, both tests returned to normal. This patient has subacute thyroiditis.
Patient 6 presented at age 27 with a 10-d history of feeling unwell; she had palpitations, difficulty breathing, and lightheadedness. She had no prior medical history, viral prodrome, or neck pain. There was no tenderness over the thyroid. Laboratory results and scintigraphic findings showed the typical pattern of high free T4 (2.6 ng/dL), low TSH (0.008 mU/L), and a 24-h radioactive iodine uptake of 2.5%. She was treated with β-blockers. This patient has silent thyroiditis.
Patient 7 was a 48-y-old man. He had classic symptoms and signs of Graves' hyperthyroidism. He was treated in another facility with 555 MBq (15 mCi) of 131I. The uptake was not measured. Three days later, he developed severe pain in the neck, and the skin over the thyroid became red and blistered and subsequently desquamated. He felt more symptomatic. Three months later, he required thyroid hormones, which he takes permanently. This patient has radiation thyroiditis attributable to internal radiation from 131I treatment.
Patient 8 was a 37-y-old woman who received a total of 44 Gy (4,400 rad) to the mantle, including the thyroid, for Hodgkin's disease. Fourteen months after the radiation, she developed symptoms of hot flashes, amenorrhea, irritability, and weight loss despite eating well. Her free T4 was 5.0 ng/dL, and her TSH was 0.05 U/L. The 24-h uptake of 123I was 1%. She was treated with propranolol and, several weeks later, became clinically and biochemically hypothyroid; she is now on long-term replacement l-thyroxine. This patient has a syndrome like silent thyroiditis that occurs rarely after external radiotherapy over the thyroid region. Permanent hypothyroidism occurs in almost all patients who have this syndrome.
Discussion.
Thyroiditis, or inflammation of the thyroid gland, encompasses several variants, including Hashimoto's or subacute, martial arts, drug-induced, postpartum, radiation-related, and silent thyroiditis (66,84–89). Hashimoto's thyroiditis (also known as autoimmune or chronic lymphocytic thyroiditis) is the most common form of thyroiditis and therefore is not discussed in detail here. There is some debate as to whether Hashimoto's thyroiditis causing thyrotoxicosis is actually a form of Graves' disease or a destructive form of thyroiditis. Some authorities use the term “hashitoxicosis” to cover these possibilities. Thyroiditis from drug ingestion is covered in the next section on exogenous causes of thyrotoxicosis. This section focuses on the remaining types of thyroiditis.
Subacute thyroiditis is also known as De Quervain's or granulomatous thyroiditis. The hallmark of this variant is a painful and tender thyroid after a viral prodrome of myalgias, pharyngitis, low-grade fever, and fatigue (90–92). The most accepted etiology of subacute thyroiditis is a viral illness. Whether the destructive thyroiditis is caused by direct viral infection of the gland or by the host's response to the viral infection is unclear. Subacute thyroiditis is associated with several viruses, including influenza virus, adenovirus, mumps virus, and coxsackievirus.
Biochemically and clinically, there is an initial period of thyrotoxicosis secondary to the release of thyroid hormones from the inflamed gland. This can last approximately 3–6 wk and is seen in one half of affected individuals. As the inflammation decreases, there is a return to euthyroidism within 6–12 mo. Usually, this is a self-limited disease requiring no specific treatment of the thyroid, and recurrences are uncommon. Symptomatic relief and a reduction of inflammation may be achieved with antiinflammatory medications. Steroids produce a dramatic response but are usually not recommended because there is recurrence of symptoms as the dose is tapered and the course of the disease is prolonged. β-Blockers may be used to control symptoms of tachycardia and tremor. Approximately 10% of patients will require long-term l-thyroxine treatment for persistent hypothyroidism.
The diagnosis is often clear from the history but can be confused with Graves' disease during the hyperthyroid phase, although the symptoms in Graves' disease are usually more severe and pain is lacking. More definitely, the 24-h radioiodine uptake will be low in subacute thyroiditis and high in Graves' disease.
Acute thyroiditis (abscess) is attributable to bacterial or fungal infection of the thyroid. It is rare. The symptoms and signs are similar to those of severe subacute thyroiditis with thyrotoxicosis in a severely ill patient. There is usually little time to obtain and review thyroid function tests. Drainage, culturing, and appropriate antibiotics should be expedited (93–96).
Silent thyroiditis is relatively uncommon and was, in fact, not recognized as a separate entity until the 1970s (97–100). This is not surprising, as it encompasses an overlap of traits similar to Hashimoto's thyroiditis, painless subacute thyroiditis, and Graves' disease (101). Clinically, patients experience symptoms of thyrotoxicosis with no or only mild enlargement of the thyroid and no infiltrative orbitopathy. During the thyrotoxic phase, circulating thyroid hormones are elevated and TSH is suppressed. On the basis of these findings, silent thyroiditis resembles a mild form of Graves' disease or subacute thyroiditis. In fact, Graves' disease and silent thyroiditis are not mutually exclusive, as patients can develop one after having had the other (102–104), and in one report, the patient had both simultaneously (105). Silent thyroiditis is principally differentiated from Graves' disease on the basis of a low radioiodine uptake (similar to subacute thyroiditis) and from subacute thyroiditis in that patients experience no pain and there is no viral prodrome. Pathologically, silent thyroiditis is more similar to Hashimoto's thyroiditis. There is a diffuse infiltrate of lymphocytes, but the germinal centers typical of Hashimoto's thyroiditis are absent. About 80%–90% of patients with silent thyroiditis show complete recovery and return of the thyroid gland to normal after 3 mo. Treatment of the thyrotoxic phase is usually symptomatic, with β-blockers being used to control tachycardia and palpitations. The patients then often experience a period of hypothyroidism during the recovery phase before ultimately returning to normal. A few patients become permanently hypothyroid and need replacement thyroid hormones. Recurrent silent thyroiditis has been reported but is rare (102,106–109). Familial silent thyroiditis has been described, and a history of this condition in a relative would strengthen the diagnosis (110).
On the basis of clinical, biochemical, scintigraphic, and pathologic similarities, silent thyroiditis is often grouped together with postpartum thyroiditis, and some authorities accept that they are the same disease (100,111–117). In fact, postpartum thyroiditis is clinically identical to silent thyroiditis, except that it occurs after pregnancy and, as such, is more prone to recurrences. Approximately 5%–7% of women experience this after birth (118). Most present with a painless, small, nontender goiters within 2–6 mo after delivery. The course of the disease follows that of silent thyroiditis, with a period of hyperthyroidism, then hypothyroidism, and ultimately a return to a euthyroid state. A total of 80% of patients return to normal by 1 y, although some have residual hypothyroidism. It is important to distinguish between postpartum thyroiditis and Graves' disease, although the degree of hyperthyroidism and its clinical symptoms are not as pronounced. Doppler ultrasound can help by demonstrating extreme vascular flow in Graves' disease. Treatment is symptomatic, with β-blockers being used for hyperthyroidism and l-thyroxine being used for hypothyroidism.
On occasion, a patient with one of these syndromes will be referred for treatment with 131I. This will not work when the uptake is low and should not be attempted. We have treated patients with recurrent silent thyroiditis but waited until the recovery phase, when the uptake was elevated (106,119).
There are 2 forms of radiation thyroiditis (120). One occurs after internal radiation therapy, such as that used to treat Graves' disease; the second occurs after external radiation for lymphoma or head and neck cancers. In the former, fewer than 1% of patients experience thyroiditis between 1 and 10 d after therapy. There is rapid destruction of the thyroid parenchyma and release of thyroid hormones. The neck is tender, and the overlying skin can be red. The pain radiates to the jaw and ear. A 7- to 10-d course of antiinflammatory medications, β-blockers, or steroids (rarely) can be used. In this situation, when the corticosteroids are stopped, there is no flare of symptoms because the thyroid is usually destroyed by the radiation. The thyroiditis resolves as the gland fibroses.
Hypothyroidism is a relatively frequent consequence of exposure of the thyroid gland to therapeutic doses of external ionizing irradiation. Paradoxically, we have described both Graves' disease and transient thyroiditis after external radiation (120–122). The best explanation for the development of Graves' disease is that the radiation causes a change in the structure of the TSH receptor, resulting in the formation of TSH-stimulating antibodies. In contrast, transient thyroiditis is most likely attributable to the destruction of follicles and the release of thyroid hormones. This is almost inevitably followed by permanent hypothyroidism.
Direct blunt or surgical trauma can cause transient hyperthyroidism (traumatic thyroiditis). This has been described after laryngectomy, needle aspiration of the thyroid, and parathyroidectomy (123). Martial arts thyroiditis has been described after a karate blow to the thyroid (124). There is pain and tenderness over the thyroid. Radioiodine uptake is low, free T4 is high, and TSH is suppressed. Because the history is clear, extensive work-up is usually not necessary. The process is self-limited and resolves in approximately 2 wk as the inflammation subsides. Palpation thyroiditis is a mild form of traumatic thyroiditis and is not associated with thyrotoxicosis. It results from vigorous palpation of the thyroid and can be seen pathologically in the excised thyroid of patients whose necks have been examined (vigorously) by several physicians (125).
Pseudothyroiditis or carcinomatous pseudothyroiditis occurs when there is very rapid growth of a cancer in the thyroid that disrupts the follicles and releases large amounts of thyroid hormones into the circulation (126–129). The onset can be rapid (130). Differential diagnoses are subacute thyroiditis and Riedel's thyroiditis. Usually the cancer is rapidly growing and clinically presents as a large hard fixed mass that is nontender. The last feature can differentiate this from subacute thyroiditis. The uptake of 123I is low. Because the type of cancer that produces this syndrome is aggressive, the prognosis is guarded.
Thyrotoxicosis Attributable to Exogenous Thyroid Hormones
Examples.
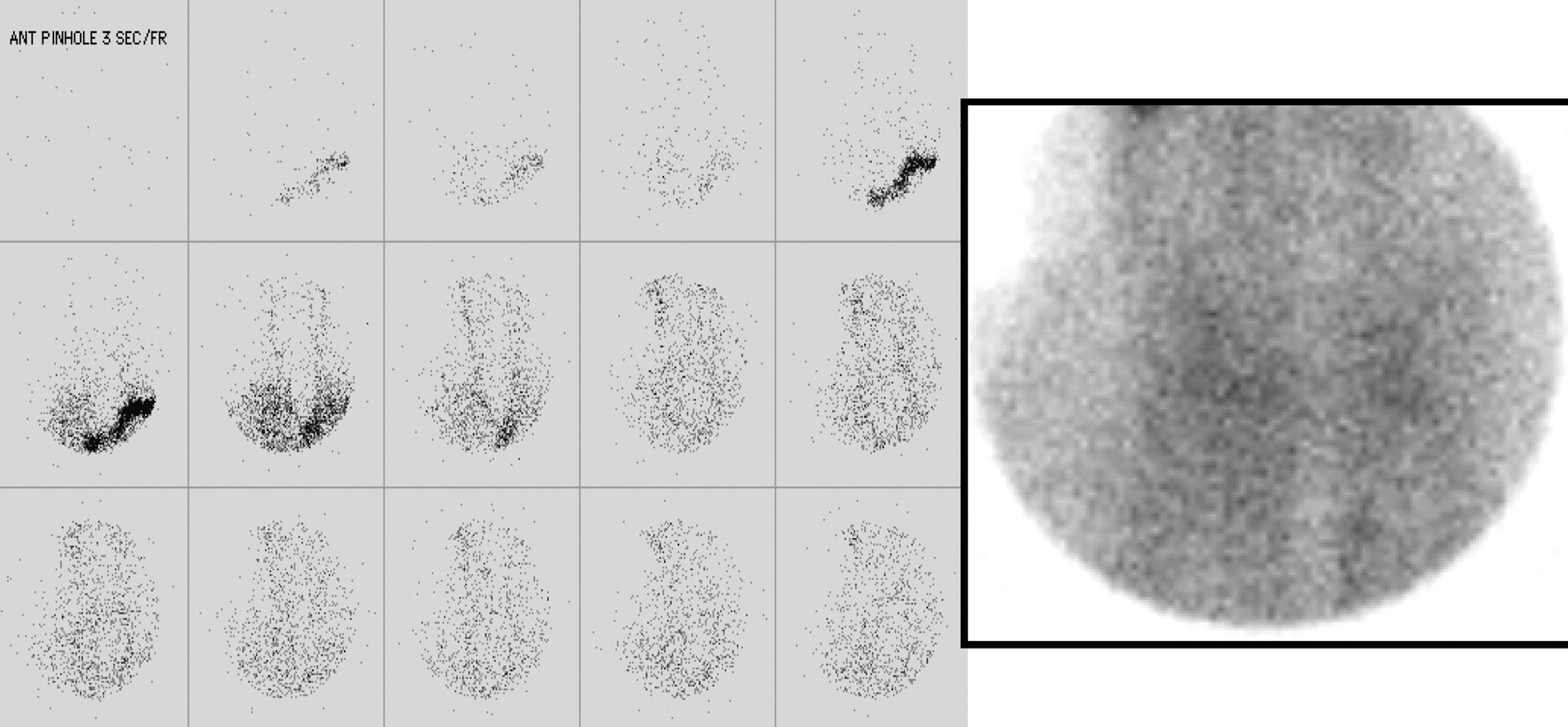
Patient 9, a 19-y-old woman, was seen because of a concern that she was thyrotoxic. She had a history of mild hypothyroidism attributable to autoimmune thyroiditis and she had been taking 100 μg of l-thyroxine daily. Clinically, she was extremely thyrotoxic, weepy, combative, and tremulous, with a pulse of 180 beats per minute. The thyroid was not palpable. Her free T4 was >6.0 ng/dL, her total T3 was 2,519 ng/dL, and her TSH was suppressed. A technetium scintiscan is shown in Figure 1. The patient was admitted to a cardiology unit because of the extreme tachycardia. She was seen by an endocrinologist, a cardiologist, and a psychiatrist. Eventually, she admitted to getting thyroid hormones, both l-thyroxine and liothyronine, from various sources, including ordering them over the Internet. She was taking the hormones to keep her weight down and to give herself more energy. This patient has thyrotoxicosis factitia (factitious thyrotoxicosis) (131).

Pertechnetate flow and static images over cervical region after intravenous injection of 185 MBq (5 mCi) of 99mTc. Flow images (left) were obtained every 3 s, and static image (right) was obtained after delay of 10 min. There was no thyroid trapping of 99mTcO4.
Patient 10, a 66-y-old woman, was diagnosed with metastatic follicular cancer in her mandible. A thyroidectomy had been conducted several years before for a benign nodular goiter. Whole-body scintigraphy with 123I and a posttherapy scan showed widespread functioning metastases. l-Thyroxine was administered at a dose designed to keep TSH as low as possible in an effort to prevent TSH-stimulated growth of the cancer. She developed atrial fibrillation. This patient has thyrotoxicosis medicamentosa.
Patient 11 was a 27-y-old woman when she was treated by surgery for thyroid cancer. The cancer was small and fully excised. Serum thyroglobulin values were always undetectable. The physician's goal was to keep the TSH value close to the lower end of the normal range (0.4 IU/L). The patient's tests always showed high free T4 and suppressed TSH (free T4 and TSH values over 5 y were 2.01, 2.64, 1.71, 1.98, and 2.37 ng/dL and <0.002, 0.004, 0.004, 0.033, and 0.043 mU/L, respectively). No matter what discussions were held about the potential risks of prolonged excess of thyroid hormones or what strength of thyroid hormones was prescribed, that pattern of tests was found.
This “syndrome” is not uncommon. The patient has more energy, can maintain or lose weight more easily, and needs less sleep. It is not factitious thyrotoxicosis because the physician and patient know that it is happening, and both know that the other knows it is happening. It is not truly iatrogenic because the physician is advising against too much hormone. This condition has been labeled “thyrotoxicosis insistiates” (132).
Patient 12, a 71-y-old man, was admitted with atrial fibrillation and cardiac failure. It became apparent that he had been advised to ingest thyroid hormone as liothyronine for the treatment of Wilson's syndrome. This involved monitoring of temperature and increasing the dose of liothyronine by increments of 7.5 μg every third day if his temperature remained “low,” defined as 98.4°F. He weighed 47.25 kg and was very frail. He was taking 120 μg of liothyronine daily at the time of his admission. His TSH was <0.004 IU/L. Because the history of Wilson's syndrome and ingestion of liothyronine was not volunteered, serum T3 was not measured. The medical team was not aware of this “syndrome.” One of us first met with the patient several days after his admission. The patient was armed with a volume of the Wilson textbook and instructions on how to take liothyronine based on his body temperature. Over several weeks, we had several conversations about thyroid physiology, pathophysiology, and thyroid testing; as a result, he agreed to stop liothyronine and to monitor thyroid function for several months to determine whether he did need thyroid hormone. In fact, he did, but 50 μg of l-thyroxine was sufficient (120 μg of liothyronine is equivalent to about 480 μg of l-thyroxine).
Discussion.
Each of the conditions discussed earlier is the result of ingestion of excess thyroid hormones (133). Apart from medicamentosa (iatrogenic) thyrotoxicosis insistiates, and Wilson's syndrome, the physician is unaware the patient is ingesting thyroid hormones. Iatrogenic thyrotoxicosis is the commonest of this category. Sometimes there is a clinical justification for this as in the case of progressive functioning thyroid cancer that is responsive to the level of TSH. In many patients the physician prescribes l-thyroxine to suppress TSH when there is no evidence that this has any benefit for the thyroid disorder (134). Treatment for weight loss, depression, infertility, menstrual abnormalities and attempted shrinkage of colloid goiter in patients with normal thyroid function are some of the reasons given. In one study, the odds ratio of a woman receiving too much thyroid hormone was 2.88 (135). The importance of measurement of TSH annually in patients taking l-thyroxine is stressed.
The danger of excess liothyronine is demonstrated by the development of uncontrolled atrial fibrillation in patient 13 who carries the nondiagnosis of Wilson's syndrome. This should not be confused with Wilson's disease, a disorder of copper metabolism. There are reports of sustained released tri-iodothyronine being used in this syndrome, a recent one in the Puerto Rico health science journal (136). Patients with Wilson's syndrome are usually educated and knowledgeable about thyroid. They have no difficulty obtaining the medication and can order over the Internet. There is no evidence-based data for prescribing this therapy for “low temperature” and it can be dangerous, as demonstrated earlier.
In the case of factitious thyrotoxicosis the diagnosis depends on clinical suspicion and biochemical thyrotoxicosis with high free T4 and suppressed TSH plus a low uptake of radioiodine. Pearce et al. have recommended the ratio of T4 to T3 to help make the diagnosis. However, some patients with factitious thyrotoxicosis take excess liothyronine and in this situation have low free T4 values but very high free T3 and suppressed TSH. The source of thyroid might even be unrecognized by the patient as in the case of diet pills that contain thyroid hormones (137,138). Patients who take an excess of thyroid hormones but deny taking it have a reason such as to lose weight, increase energy or reduce the need for sleep. Alternative names for this syndrome are thyroxine addict or metabolic malingerer (139,140). To aid in the diagnosis, serum thyroglobulin is usually low or undetectable (141). However, when the patient has underlying autoimmune thyroid disease, antibodies against thyroglobulin make this measurement less reliable. One group has demonstrated that thyroid hormone levels are higher in the feces when the cause of thyrotoxicosis is attributable to ingestion of the hormone (142). Color flow Doppler is also a valuable investigation because it shows almost absent blood flow to the thyroid (143). Patient 10 described in this section was extremely ill and was admitted to a cardiac unit. Thyroid storm and myocardial infarction attributable to factitious thyrotoxicosis have been reported (144,145).
We have no patient histories to describe “hamburger thyrotoxicosis”; however, there have been several outbreaks of thyrotoxicosis attributable to thyroid gland being included with neck trimmings that were used to make ground beef (146,147). This practice is now prohibited in the United States. A more recent report of recurrent “silent” thyroiditis turned out to be attributable to hamburger thyroiditis in a woman whose husband slaughtered a cow every year or so and included the thyroid with gullet muscles (148). One of us has heard that this syndrome can be identified in deer hunters who unknowingly include the thyroid in their ground venison.
Feit and Feit described a 50-y-old woman who was clinically and biochemically thyrotoxic (149). This was attributable to her mistakenly taking her dog's l-thyroxine rather than her own. Most physicians would not know that a replacement dose of l-thyroxine for a 31.5- to 36-kg dog is about 0.6 mg 4 times per day. The authors called this “thyrotoxicosis factitia veterinarius.” They did not discuss whether the dog was given the patient's l-thyroxine and was hypothyroid.
In patients with high levels of free thyroid hormones and a low level of TSH and who are known to be ingesting thyroid hormones, there is no need for additional tests. When it is thought they are not taking thyroid hormones an 123I uptake would be ordered and a low result would allow this possibility to be considered (150). Sensitive enquiry would be in order and if that is not a helpful measurement of thyroglobulin. In cases of factitious thyrotoxicosis consultation with a psychiatrist is generally required.
Thyrotoxicosis Attributable to Excess Iodine
Example.
Patient 13 was a 68-y-old man who had been taking amiodarone for paroxysmal atrial fibrillation for 2 y. Paradoxically there was an increase in the number of arrhythmias. He underwent a coronary arteriogram that was normal. His free T4 was >6 ng/dL, and his TSH was <0.04 IU/L. Because of the recent radiographic contrast, a thyroid uptake and scan were not obtained. He was treated with methimazole and prednisone. His clinical condition and the thyroid function tests improved and the prednisone dose was tapered over a few weeks. Eight weeks later, his free T4 was nearly normal (1.94 ng/dL).
Discussion.
Iodine-induced thyrotoxicosis is also called Jod Basedow disease. Jod Basedow is derived from jod, the German for iodine, and Basedow from Von Basedow who described in German what the English-speaking medical world knows as Graves' disease (151). Iodine-induced thyrotoxicosis is usually not Graves' or Basedow's disease but toxic nodular goiter. It is more likely to occur in regions of iodine deficiency in people with nodular goiters who are then exposed to an excess of iodine (152,153). The autoregulatory controls of the thyroid must fail for this to occur. Usually an increase in plasma inorganic iodine causes reduced trapping of iodine, organification (Wolff–Chaikoff effect) and reduced release of preformed thyroid hormones. Thus, an autonomously functioning nodular goiter is at most risk.
The source of iodine is usually apparent, such as the addition of iodine to salt. There are many reports of this occurring in regions of low iodine intake soon after iodine is added to the diet. The extensive review by Stanbury et al. discusses the history, etiology and epidemiology of this (154). This is rare in the population born and raised in the United States but is found in immigrants from regions of low dietary iodine who come to the United States (155). The source might be obvious but the outcome not predicted, such as development of thyrotoxicosis after iodine given to block uptake of radioiodine in the thyroid (156,157). In contrast the source of iodine might not be obvious. For example, a patient developed thyrotoxicosis after drinking herbal tea with added kelp (158).
Radiographic contrast is a rare cause of Jod Basedow disease in the United States (159). These compounds contain between 300 and 400 mg of iodine per milliliter, and 100–200 mL are administered for many procedures, such as CT with contrast material and coronary arteriography. Therefore, up to 80 g (80,000,000 μg) of iodine are rapidly administered. The daily requirement is 150–200 μg. We have demonstrated that excess iodine can be identified in the nail clippings of patients for months after the procedure (160).
Amiodarone is an effective antiarrhythmic medication but it has several side effects, including effects on thyroid function. There are 2 atoms of iodine in amiodarone that contribute 38% of its weight. Deiodination of amiodarone produces about 12 mg of free iodine daily when a patient ingests 400 mg. This is a large quantity compared with the recommended daily intake of 150 μg (4,161–164). Amiodarone is fat soluble and has a half-life of many months because of the slow release of stored drug from that site. The effect on thyroid function is somewhat dependent on the quantity of iodine ingested. In regions of iodine deficiency amiodarone is more likely to cause thyrotoxicosis, and in iodine-sufficient regions hypothyroidism is more likely. This difference is attributed to nodular goiter being more prevalent in iodine-deficient regions. The excess iodine from amiodarone provides the raw material for the nodules to produce excess thyroid hormones. This has been designated type 1 amiodarone–induced thyrotoxicosis. It contrasts with type 2, which is attributable to destruction of follicles producing a thyroiditis-like picture. Type 2 is more common in the United States. Some patients have an overlap of these patterns. In the United States, most patients have a low uptake of 123I. In contrast in regions of low iodine intake the uptake values in type 1 amiodarone–induced thyrotoxicosis can be normal or high. Some investigators have reported that interleukin 6 levels are elevated in type 2 amiodarone–induced thyrotoxicosis; however, the results do not provide a clear separation. Ultrasound with color flow Doppler shows increased vascularity in type 1 and reduced vascularity in type 2 AIT. Treatment is difficult because amiodarone is often the most effective antiarrhythmic in the patient and there is reluctance to stop it. In addition, because of the long half-life its effects persist for months to years. The low uptake of radioiodine makes 131I useless. Antithyroid medication such as methimazole 30–40 mg daily has been effective and the patient should be educated about side effects, including skin rash and agranulocytosis. Potassium perchlorate has been used as a competitive inhibitor of trapping iodine by the sodium–iodide symporter. Reports from Europe indicate a combination of methimazole and potassium perchlorate is successful. Potassium perchlorate is not available in the United States. Corticosteroids such as prednisone at 30–60 mg/d are effective in the destructive type 2 syndrome. Thyroidectomy can be undertaken when antithyroid therapy is ineffective, but these patients are often poor operative candidates because of the underlying cardiac disease.
Thyrotoxicosis Attributable to Nonthyroid Medications
Example.
Patient 14 had a history of hepatitis C. She acquired hepatitis C during childhood. At age 25 she was treated with pegylated interferon and ribavirin. After 1 y, her free T4 was elevated, and her TSH was suppressed. The antiviral regimen was stopped because of a lack of benefit. One year later, her free T4 was 1.4 ng/dL, and her TSH was 1.16 IU/L. Most likely, she had thyrotoxicosis attributable to interferon.
Discussion.
Thyrotoxicosis has been identified in patients treated with interferon-α interleukin, lithium, denileukin diftitox, and leuprolide acetate (108,109,165–169). Usually these medications cannot be stopped; therefore, the key is to determine whether the thyroid has high or low uptake of 123I. The former group can be treated in conventional fashion, including 131I. The latter are likely to be self-limiting. With regard to interferon-α, most of the information relating to this topic is in patients with hepatitis C (170–174). Some are treated with a combination of interferon-α and ribavirin. About 10% of patients produce antithyroid antibodies, and a proportion develop Graves' hyperthyroidism. Thyroid function tests and levels of antithyroid antibodies should be measured and 123I uptake obtained. The treatment is that of Graves' disease and is usually 131I or antithyroid medications (175). There is also a destructive form of thyroiditis with thyrotoxicosis that occurs in patients treated with type II interferons. The key is to obtain an uptake measurement, and when the value is low the course is similar to that of silent thyroiditis (165,176). Eight patients with mycosis fungoides became thyrotoxic during treatment with denileukin diftitox (167). Denileukin diftitox is a recombinant fusion protein consisting of the ligand binding region of interleukin 2 and diphtheria toxin. The course of the disease with sudden onset of thyrotoxicosis plus evidence of low uptake of radioiodine in 2 patients and subsequent hypothyroidism implies an inflammatory thyroiditis.
It is paradoxical that lithium is associated with development of thyrotoxicosis because it is used to treat Graves' hyperthyroidism and it can cause hypothyroidism (177–179). Thyrotoxicosis can be the result of a syndrome like silent thyroiditis or Graves' disease (180–182). Barclay et al. identified 14 patients, 3 times the expected number (180). Thirteen had scans: 8 had Graves' disease, 3 toxic nodular glands, and 2 silent thyroiditis.
Thyrotoxicosis After Bone Marrow Transplantation
The immune system of the donor is transferred to the recipient of a bone marrow transplant. It is therefore expected that autoimmune disorders in the former can appear in the latter. Thyrotoxicosis is one rare example (183–185). Treatment is standard for Graves' hyperthyroidism. As would be expected, hypothyroidism has also been described (186).
CONCLUSION
Thyrotoxicosis in the United States is usually the result of Graves' hyperthyroidism and less often single and multiple hyperfunctioning nodules. There are, however, many other causes of high values of free thyroid hormones associated with symptoms and signs of thyrotoxicosis. This review discusses the majority of these. General physicians, endocrinologists and nuclear medicine consultants will encounter these patients periodically. The key to management is to establish the correct diagnosis because the therapy differs depending on the specific diagnosis. We acknowledge that many physicians order only TSH as a screening test to rule out thyroid dysfunction. We recommend that free T4 and TSH be measured at the first visit to ensure rare disorders such as a TSH-secreting pituitary tumor or resistance to thyroid hormones are not misdiagnosed as Graves' disease. We also recommend that patients who have elevated free hormone levels and a suppressed TSH have an 123I uptake (or 99mTc-pertechnetate scintiscan) to differentiate patients with low uptakes. Figure 2 shows an algorithm for differentiating the various causes of low-uptake thyrotoxicosis. First, technical factors, including whether the patient ingested the tracer of radioiodine and the correct settings for uptake, should be confirmed. Exogenous thyroid and high doses of iodine, such as in contrast material, would be excluded as causes. Next, patients with painful thyroids would be separated from those with no pain or tenderness. Figure 2B demonstrates the differentiation of thyrotoxicosis with low uptake and a painful thyroid. Figure 2C does the same for painless glands. In general, thyrotoxicosis with low uptake is self-limiting and the patient seldom benefits from standard antithyroid treatments. That information is very reassuring to them.

Algorithm for diagnosing different forms of thyrotoxicosis with low uptake. (A) Importance of measuring uptake and checking technical factors that could cause false-positive outcome. (B) Painful thyroid glands with low uptake. ESR = erythrocyte sedimentation rate. (C) Painless thyroid glands.
When the uptake over the cervical region cannot be identified and the course of thyrotoxicosis persists, 123I scintigraphy of the remainder of the body is recommended to diagnose ectopic sites of formation of thyroid hormones.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH FEBRUARY 2009.
-
No potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.
- 39.
- 40.
- 41.
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.
- 83.↵
- 84.↵
- 85.
- 86.
- 87.
- 88.
- 89.↵
- 90.↵
- 91.
- 92.↵
- 93.↵
- 94.
- 95.
- 96.↵
- 97.↵
- 98.
- 99.
- 100.↵
- 101.↵
- 102.↵
- 103.
- 104.↵
- 105.↵
- 106.↵
- 107.
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.
- 128.
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.
- 163.
- 164.↵
- 165.↵
- 166.
- 167.↵
- 168.
- 169.↵
- 170.↵
- 171.
- 172.
- 173.
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.
- 179.↵
- 180.↵
- 181.
- 182.↵
- 183.↵
- 184.
- 185.↵
- 186.↵
- Received for publication February 26, 2007.
- Accepted for publication September 10, 2007.





{kind=link}
{kind=link}