


Abstract
We reviewed our experience of 18F-FDG PET/CT in noncentral nervous system (CNS) pediatric malignancies and evaluated if PET/CT provided additional information to conventional imaging (CI) examinations to determine the efficacy of this new imaging modality in the clinical setting. Methods: One-hundred fifty-one consecutive FDG PET/CT examinations in 55 pediatric patients with non-CNS malignant tumors were reviewed. Among them, 108 PET/CT examinations were accompanied by CI, such as contrast CT or MRI, performed within a month of PET/CT in our hospital. Two radiologists reviewed the indication, purpose, and PET/CT findings and compared the findings with those of CI, if available, on the representative lesion in each of the 6 separate body regions. Positive findings included abnormal findings related to malignant lesions (suspected) as well as equivocal findings, in which the presence of malignancy could not be denied, but excluded findings considered to relate to past treatment. Accuracy of the findings was determined on the basis of the reference standard comprising histopathologic findings or informative follow-up of >1 y. An examination-based analysis was also performed in terms of additional information of PET/CT to CI. Results: There were 56 PET/CT-positive–CI-positive, 26 PET/CT-positive–CI-negative, and 54 PET/CT-negative–CI-positive lesions in 108 PET/CT examinations accompanied by CI, of which 54, 20, and 52 exhibited accurate PET/CT findings, respectively. Seventeen of the 20 PET/CT true-positive–CI false-negative lesions represented small lymph nodes diagnosed as negative on CI. All 52 PET/CT true-negative–CI false-positive findings were observed in lesions in a posttreatment status including 30 mediastinal masses in lymphoma. Examination-based analysis revealed that additional information of PET/CT to CI was found in 37 (34%) of the 108 examinations: 23 (21%) as negative and 14 (13%) as positive PET/CT findings. Conclusion: PET/CT exhibited better diagnostic performance than CI and showed accurate findings in 90% (72/80) of lesions with discordant findings between them. Additional information of PET/CT to CI was observed in more than one third of examinations compared. PET/CT was demonstrated to be an accurate imaging modality in evaluating pediatric patients with non-CNS malignancies.
PET with the glucose analog, 18F-FDG PET, is increasingly recognized as a powerful tool in evaluating patients with various malignant tumors (1–3). However, only a limited number of reports have been available to date on noncentral nervous system (CNS) body malignancies in pediatric patients with FDG PET (4–8), likely due to the relative infrequency of pediatric malignancies and limited insurance coverage. Thallium (201Tl), gallium (67Ga), metaiodobenzylguanidine, and bone scintigaphies are often used to evaluate pediatric body malignancies, in addition to CT, ultrasound, radiography, and MRI. PET has been long used on pediatric brain tumors (9–11), but the number of reports dealing solely with them is quite limited.
Recently, combined PET and CT systems (PET/CT) have emerged as promising imaging modalities and are being more routinely used in clinical situations (12–14). PET/CT offers routine precise fusion of metabolic PET images with high-quality CT images. Definite localization of FDG uptake is possible with fused PET/CT images. As PET/CT provides PET and CT images in a single examination, it is expected to be advantageous in evaluating pediatric patients, in whom reduced numbers of examinations are preferred.
Despite growing numbers of reports on imaging adult malignancies with PET/CT, little data have been reported so far about the clinical relevance of this modality in comparison with conventional imaging examinations in pediatric patients. Thus, we retrospectively reviewed our initial clinical experience with FDG PET/CT in pediatric malignancies to evaluate the efficacy of this new imaging system and to determine if PET/CT provided additional diagnostic information on disease status as compared with conventional imaging (CI) methods.
MATERIALS AND METHODS
Patients
Fifty-five pediatric patients (31 male, 24 female) had 151 PET/CT examinations in our PET center from July 2001 to January 2004. The patients were from 3 to 19 y old with a median age of 15 y at their first PET/CT examination. The indication, purpose, and findings of each PET/CT examination were reviewed, in addition to other imaging findings as well as clinical information including follow-up results for >1 y from their last PET/CT examination. Our institutional review board allowed an exempt retrospective review of our cancer PET database for this study, and informed consent was waived.
FDG PET/CT Examination
Whole-body FDG PET/CT was performed with a combined PET/CT scanner (Discovery LS; GE Healthcare). This scanner allows the simultaneous acquisition of 35 transaxial images with an interslice spacing of 4.25 mm in one bed position for PET images. This scanner also allows multidetector row helical CT. Technical parameters used for the CT portion of PET/CT were as follows: a detector row configuration of 4 × 5 mm, pitch of 6:1 (high-speed mode), gantry rotation speed of 0.8 s, table speed of 30 mm per gantry rotation, and 120 kVp. The tube current of CT was determined by patient weight: 40 mA for <45.3 kg and 60 mA for <68 kg.
After at least 4 h of fasting, patients received an intravenous injection of 5.55 MBq/kg (0.15 mCi/kg) body-weight dose of 18F-FDG (minimum dose, 74 MBq [2 mCi]; maximum dose, 555 MBq [15 mCi]). About 60 min later, CT images were acquired from the midthigh to the meatus of the ear without intravenous contrast media. A whole-body emission PET scan for the same axial coverage was performed with a 5-min acquisition per each bed position. Attenuation-corrected PET images were reconstructed with an ordered-subset expectation maximization iterative reconstruction algorithm. The 5-mm-thick transaxial CT images were reconstructed at 4.25-mm intervals to fuse with the PET images. PET, CT, and fused PET/CT images were generated for review on a computer workstation.
Review of PET/CT and Other Imaging Examinations
In each examination, all PET/CT image sets were reviewed by 2 radiologists in a consensus manner, referring to the official PET/CT reports from our PET center. PET images were reviewed first, followed by the CT portion of PET/CT and the fused PET/CT images on a computer workstation. Locations of abnormal FDG uptake were recorded. Abnormal FDG uptake was defined as the increased FDG uptake caused by other than physiologic process, and positive FDG uptake was defined as abnormal uptake related to malignant lesions (suspected). Equivocal findings, in which the presence of malignancy could not be denied, were regarded as positive in this study, but FDG uptake obviously considered to relate to past treatment (operation, radiotherapy, or others) was classified into negative findings. The location of abnormal FDG uptake was classified into 1 of the following 6 anatomic regions: head, neck, chest, abdomen, pelvis, and extremities.
Reports of contrast-enhanced CT or other imaging examinations performed in our institution were then reviewed by the same 2 radiologists, and locations of abnormal findings were also recorded. We defined a corresponding imaging (CI) examination to PET/CT as the conventional examination performed within a month of the PET/CT examination. Positive and equivocal findings on CI were dealt with similarly to those on PET/CT. As this study included many patients in posttreatment status, scarlike soft-tissue shadows were often observed. They were regarded as negative for the presence of malignancy if “no interval change” findings were obtained repeatedly, twice or more in a row, without interval therapy.
Lesion-Based Analysis
Findings were compared between PET/CT and CI examinations in terms of the presence of malignancy on the representative largest lesion in each region and were classified as true-positive (presence of malignancy), true-negative (absence of malignancy), false-positive (abnormal FDG uptake unrelated to malignancy), or false-negative (missed diagnosis of proved malignancy) according to the reference standard. The reference standard included histopathologic findings (obtained from operation or biopsy) or informative follow-up (clinical, laboratory, PET/CT, CI, or other imaging findings). The follow-up duration was >1 y from the last PET/CT examination for each patient. In most clinical situations it was impossible to obtain histopathologic proof for all suspected lesions, especially in patients with recurrence or systemic disease spread. Thus, we set our reference standard according to the published method adopted in the study comparing PET/CT and contrast-enhanced CT findings similar to ours (15).
Examination-Based Analysis
Each PET/CT examination was classified into a positive or negative examination, on the basis of the presence of positive PET/CT finding at the lesion-based analysis described. A positive PET/CT examination was defined as the examination having at least one PET/CT-positive lesion.
PET/CT examinations accompanied by CI were further classified into the following 4 categories according to the type of additional information of PET/CT to CI: type A, no additional information; type B, detection of additional lesion(s) without upstaging or possible influence of treatment strategy; type C, detection of additional lesion(s) with upstaging or possible influence of treatment strategy; type D, downstaging or exclusion of residual disease (possible influence of treatment strategy as negative findings). In cases in which PET/CT examinations consisted only of lesions with false PET/CT findings, they were categorized as type E examinations. The PET/CT examination not accompanied by CI was classified into type F, positive examination; type G, negative examination; or type H, examination that consisted only of lesion(s) with false PET/CT finding(s).
Statistics
The sensitivity, specificity, and accuracy were calculated for the lesion-based analysis. Differences in these indices between PET/CT and CI were evaluated with the McNemar test. P values < 0.05 were considered significant.
RESULTS
The 55 patients evaluated in this study included 30 with lymphoma (55% of the 55: 26 Hodgkin's and 4 non-Hodgkin's), 13 with bone/soft-tissue tumors (24%), and 12 with other tumors (22%). Patient characteristics are listed on Table 1. Thirty-six (65%) of the patients had repeated PET/CT examinations: 14 patients twice, 10 patients three times, and 12 patients four or more times.
Characteristics of 55 Patients and 151 PET/CT Examinations
A total of 151 PET/CT examinations were performed on these patients, and 107 (71%) were to evaluate lymphoma. Only 16 of the 151 examinations were performed for initial tumor staging or diagnosis, and the remaining 135 were performed in a posttreatment status. One hundred eight (71%) of the 151 PET/CT examinations were accompanied by CI, which was performed within a month of each PET/CT examination. PET/CT and CI findings were compared in these 108 examinations. Contrast-enhanced CT accounted for 97 (90%) of these 108 CI examinations.
Lesion-Based Analysis
There were 56 PET/CT-positive–CI-positive, 26 PET/CT-positive–CI-negative, and 54 PET/CT-negative–CI-positive lesions (1 representative lesion per region) observed in 108 PET/CT and CI examinations compared (648 regions in total). Table 2 summarizes the distribution and proofs for these lesions. Table 3 describes the details of lesions with discordant findings between PET/CT and CI. The remaining 512 regions showed PET/CT-negative–CI-negative findings, and no lesions that were both false-negative were found in this study.
Distribution of PET/CT and CI Findings on Suspected Malignant Lesions
Details of Lesions with Discordant PET/CT and CI Findings
Among 56 PET/CT and CI lesions that were both positive, 54 were considered to be true-positive on the basis of the reference standard. The remaining 2 lesions that were both positive showed false-positive findings: one for hypertrophic thymus and the other for postoperative inflammatory change in the chest wall.
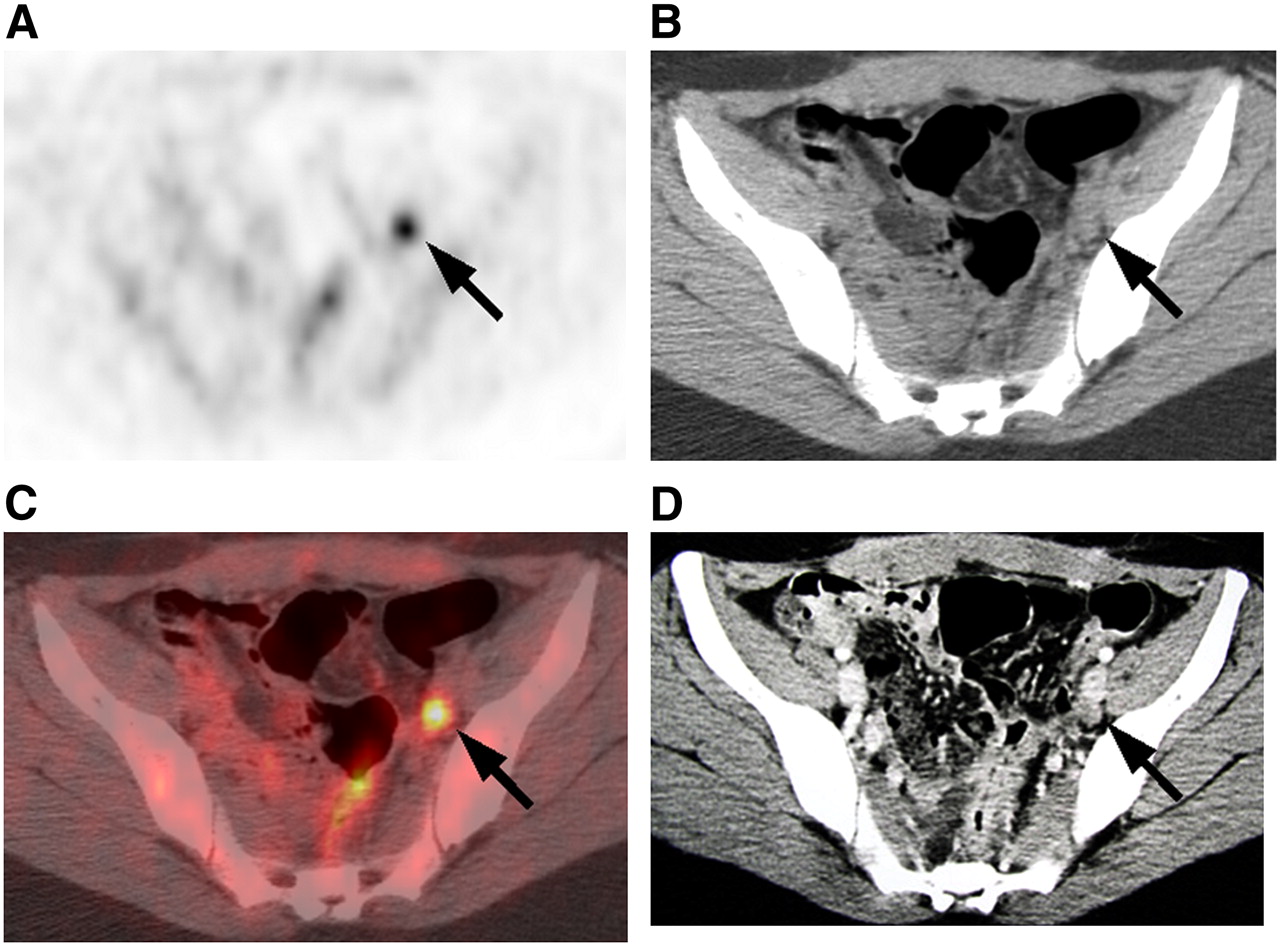
The 26 PET/CT-positive–CI-negative lesions included 20 PET/CT true-positive–CI false-negative lesions (77%). Seventeen of the 20 lesions represented small lymph nodes diagnosed as not clinically significant by the size criterion on CI (Table 3). Their locations were variable (Tables 2 and 3). The remaining 3 lesions with PET/CT true-positive–CI false-negative findings were observed as spleen and bone involvement in lymphoma (1 and 2 lesions, respectively). Figure 1 shows a patient with left pelvic lymph node metastasis from the gonadal stromal tumor. PET/CT clearly demonstrated a positive focus of FDG uptake in the small lymph node, whereas contrast-enhanced CT diagnosed the lesion as negative (not clinically significant) due to the size criterion. Figure 2 represents a patient with splenic involvement in lymphoma. The diffuse splenic involvement was clearly depicted on PET/CT but was regarded as negative, slight splenomegaly, on CI. Six PET/CT-positive–CI-negative lesions exhibited PET/CT false-positive–CI true-negative findings, which were observed in the neck (2 inflammatory lymph nodes), liver (inhomogeneous physiologic uptake), ovary (functional cyst), and leg (2 foci of inhomogeneous uptake probably due to slight inflammation).

A 17-y-old female with gonadal stromal tumor. (A) FDG PET, (B) CT, (C) fused PET/CT, and (D) contrast CT (performed on a different day from PET/CT) (all transaxial images). FDG PET clearly showed a focus of intense FDG uptake in left pelvic region (arrow), where CT and fused PET/CT depicted a small lymph node (arrow). Contrast-enhanced CT diagnosed the lymph node as negative (not clinically significant) for malignancy due to the size criterion (arrow). Progression of disease was observed from this lymph node lesion during the follow-up period in this study.

A 15-y-old male with Hodgkin's lymphoma. (A) FDG PET, (B) CT, and (C) fused PET/CT (all transaxial images). Diffuse and intense FDG uptake was observed in enlarged spleen on PET/CT, which corresponded to involvement. Splenic involvement was not detected on contrast-enhanced CT (not shown) but was diagnosed as mild splenomegaly.
There were 52 PET/CT true-negative–CI false-positive and 2 PET/CT false-negative–CI true-positive lesions. Thirty (58%) of the 52 PET/CT true-negative–CI false-positive lesions were observed as mediastinal soft-tissue masses in patients with lymphoma after treatment. Ten of the remaining 22 PET/CT true-negative–CI false-positive lesions were also observed in patients in a posttreatment status (8 in lymphoma). Both of the 2 PET/CT false-negative–CI true-positive lesions were located in the liver as small metastases.
Sixteen lesions represented scar-like soft tissue without FDG uptake, but they were classified into the category of PET/CT true-negative–CI true-negative finding because of “no interval change” on CI examinations repeatedly.
Taken together, of 80 lesions with discordant PET/CT and CI findings, 72 (90%) were considered to represent accurate PET/CT findings, 20 as PET/CT true-positive and 52 as PET/CT true-negative findings. Of all 74 lesions with PET/CT true-positive findings, 20 (27%) showed CI false-negative findings. The sensitivity, specificity, and accuracy on a per-region basis were 97%, 99%, and 98% on PET/CT and 74%, 91%, and 89% on CI, respectively. The former were significantly higher than the latter for each index (P < 0.01 for all). These high values are driven in part by the large number of true-negative regions for both PET/CT and CI studies.
Examination-Based Analysis
Of 108 PET/CT examinations with CI, 68 (66%) examinations gave no additional information to CI, which were categorized as type A examinations. The 68 examinations included 2 examinations comprised only of lesions with concordant PET/CT and CI false-positive findings. Fifteen of the 71 examinations exhibited residual soft tissue without FDG uptake after treatment, which were regarded as negative due to no interval change findings on repeat CI examinations.
Thirty-seven PET/CT examinations (34% of all 108) showed additional information to CI: 32 in lymphoma, 5 in others. In 2 and 12 examinations (2% and 11% of all 108, respectively), PET/CT detected more lesions than CI without and with upstaging (or possible influence of treatment strategy), respectively, representing type B and type C examinations. Positive PET/CT findings observed in normal-sized lymph nodes, which were diagnosed as negative on CI, accounted for 50% (1 lesion) of type B and 92% (11 lesions) of type C examinations.
Twenty-three PET/CT examinations (21% of all 108) were categorized as type D for their findings of downstaging or exclusion of residual viable lesions as compared with CI findings. The 23 type D examinations included 19 examinations in patients with lymphoma in a posttreatment status.
Three PET/CT examinations were regarded as type E, consisting only of lesions with false PET/CT findings: PET/CT false-positive–CI true-negative findings in 2 examinations and PET/CT false-negative–CI true-positive findings in 1 examination.
Of 43 PET/CT examinations without CI, 8 (19%) and 35 (81% of the 43) showed positive and negative findings, respectively, representing type F and type G examinations. Ten patients were followed up exclusively with PET/CT without CI. No examinations comprised only lesions with false PET/CT findings.
Figure 3 shows a patient with Hodgkin's lymphoma with right mediastinal soft-tissue mass. In the first PET/CT examination for this patient after chemotherapy, a focus of FDG uptake was observed in the peripheral area of the mass, which was considered to be a residual active portion. This mass was also diagnosed as positive on contrast-enhanced CT. In the next series, the mediastinal mass still existed, but PET/CT exhibited a negative finding for the lesion. PET/CT was thought to be useful in denying an active portion in the mass. The same findings were observed in the third PET/CT and CI examinations, indicating that the mediastinal mass was posttreatment scar.
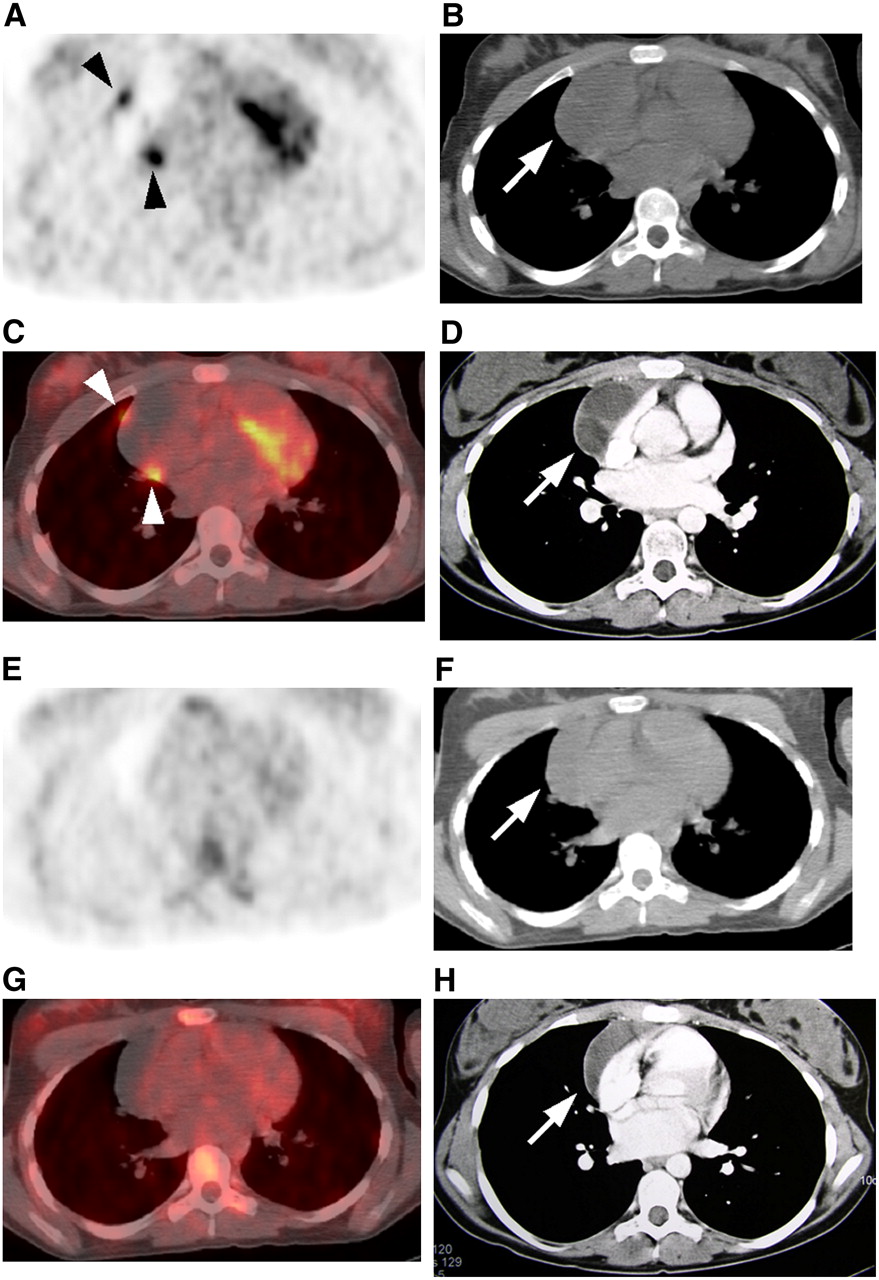
A 13-y-old female with Hodgkin's lymphoma. (A and E) FDG PET, (B and F) CT, (C and G) fused PET/CT, and (D and H) contrast CT (performed on different day from PET/CT) (all transaxial images). Patient presented with right mediastinal soft-tissue mass. In first PET/CT examination for this patient after chemotherapy (A–D), a focus of FDG uptake was observed in peripheral area of the mass (arrowhead), which was considered to be a residual active portion. Mass was also diagnosed as positive on contrast-enhanced CT (arrow). In next examination session after further treatment (E–H), the mediastinal mass still existed (arrow), although PET/CT showed a negative finding for this lesion. The same findings were observed in the follow-up PET/CT and CI examinations, indicating the PET/CT finding in second examination was correct and the mediastinal mass was posttreatment scar.
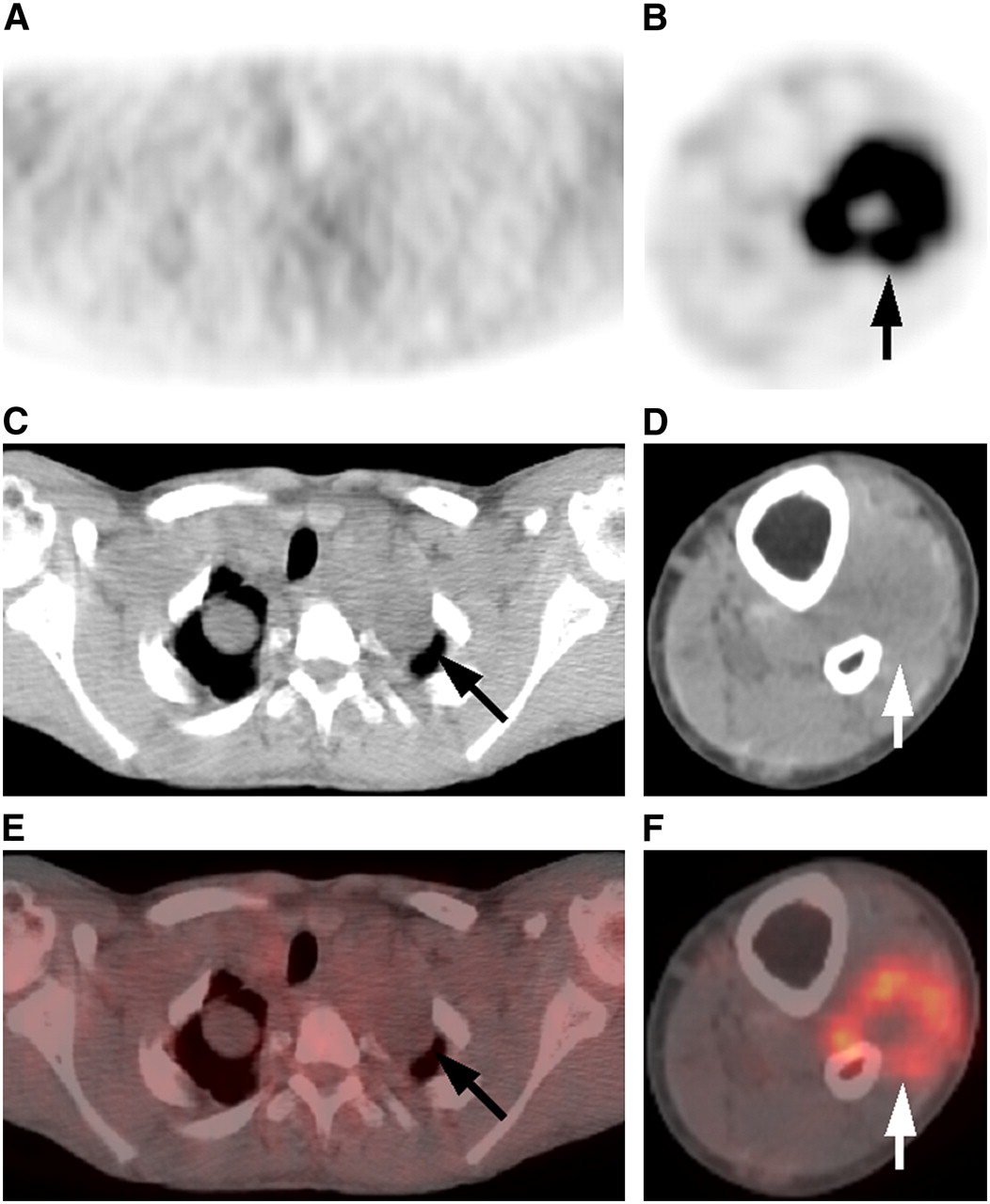
Figure 4 exhibits a patient with neurofibromatosis. There were many soft-tissue masses in the body with mild-to-moderate FDG uptake, suggesting that they were benign lesions. However, in his left lower leg, a mass with intense FDG uptake was observed, which proved to be a lesion of malignant transformation by histopathologic evaluation. PET/CT for this case was valuable in discriminating malignant lesions from other benign soft-tissue masses, which was not possible on CI.
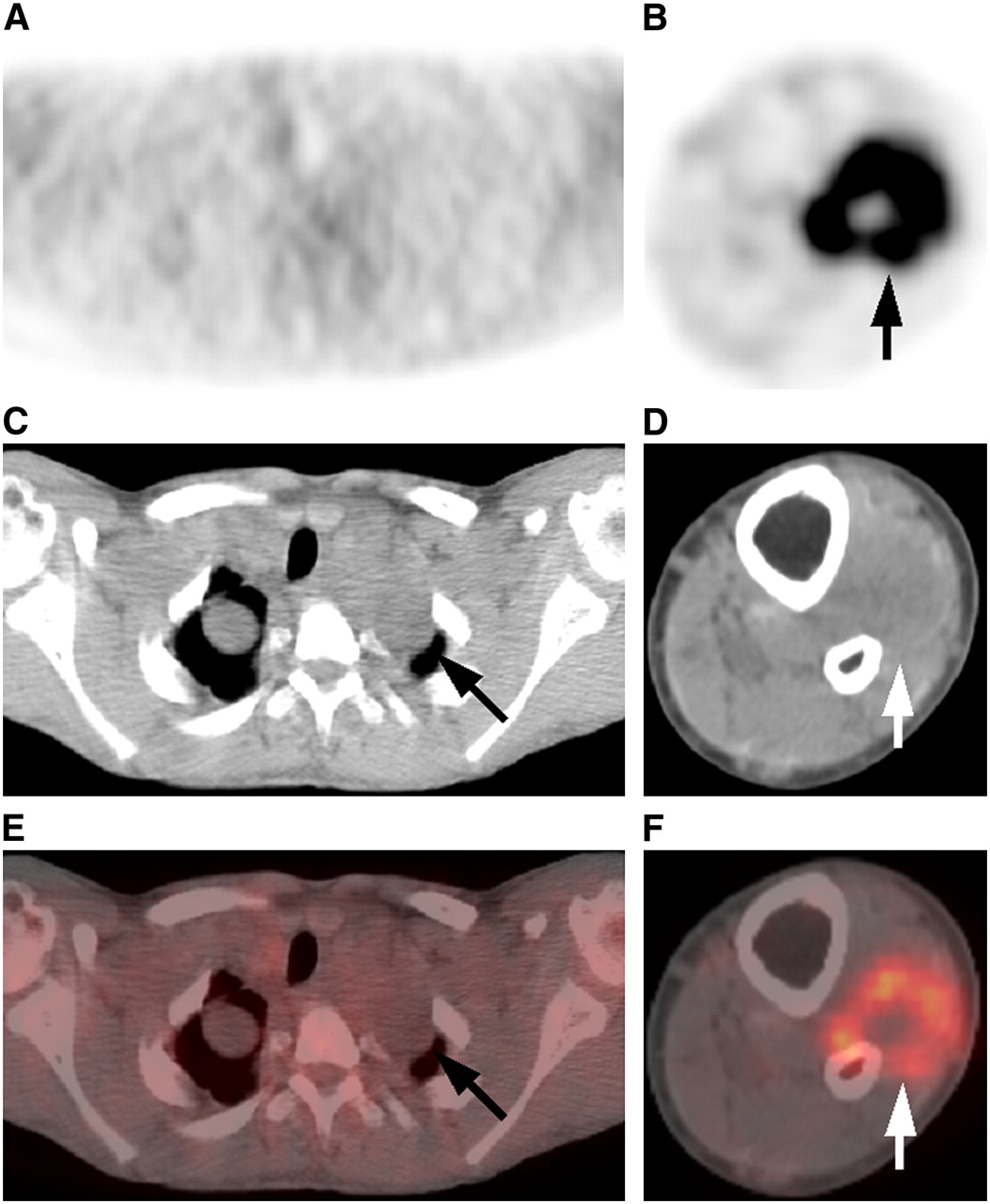
A 15-y-old male with neurofibromatosis. (A and B) FDG PET, (C and D) CT, and (E and F) fused PET/CT (all transaxial images). There were many soft-tissue masses in the body (A, C, and E) with mild-to-moderate FDG uptake, consistent with benign lesions of neurofibromatosis (arrow). However, in his left lower leg (B, D, and F), masses with intense FDG uptake were observed (arrow), which proved to be lesions of malignant transformation by histopathologic evaluation. PET/CT was valuable in discriminating malignant lesions from other benign soft-tissue masses in this patient.
DISCUSSION
Pediatric malignancies are regarded as distinct from adult malignancies in view of their low frequency, treatment strategy, and expected prognosis (8,16). Special attention should be required in interpreting images of pediatric patients, taking these conditions into consideration. As only a limited number of reports have been available to date regarding FDG PET or PET/CT in pediatric patients, we conducted this study to begin to assess the clinical utility of PET/CT as an imaging system in non-CNS pediatric malignancies. The present study demonstrated that PET/CT exhibited significantly higher sensitivity, specificity, and accuracy than CI and showed accurate findings in 90% (72/80) of lesions with discordant findings between them. Additional information of PET/CT relative to CI was observed in more than one third of examinations compared.
We first reviewed the indication or purpose of each PET/CT examination in our initial experience. PET/CT examinations for lymphoma were found to account for >50% (30/55) on a patient basis and >70% (107/151) on an examination basis in this study. Although lymphoma is also a common indication for PET/CT in adults, other major malignancies, such as lung or colorectal cancers, were rarely included in this pediatric study. Probably because pediatricians have already recognized the usefulness of PET/CT in pediatric lymphoma in our institution, PET/CT was commonly used to evaluate this disease, although its frequency is <15% of all pediatric malignancies (16,17). Because lymphoma requires repeat imaging examinations after treatment, PET/CT potentially can be a selected sole evaluation method, providing both metabolic and anatomic information in one examination. In other pediatric malignancies as well, PET/CT is expected to serve as a powerful imaging modality, especially in staging or in evaluating suspected recurrence, according to the results of this study.
Discrepant PET/CT and CI findings were frequently observed on a lesion-based analysis in this study. Ninety percent (72) of the 80 lesions with discrepant findings proved to exhibit accurate PET/CT findings. Many of them (30 of the 80 lesions with discrepant findings) were PET/CT true-negative–CI false-positive findings for mediastinal soft-tissue masses in lymphoma in a posttreatment status. The same finding was also observed for soft-tissue masses of other malignancies in a posttreatment status. The important point relevant to this finding is that residual viable portions are not necessarily excluded in these kinds of soft-tissue masses solely on CI without follow-up information. PET or PET/CT has clear advantage in evaluating these lesions and, thus, has been reported to be useful in patients with lymphoma or other malignancies after treatment (3,18,19). Schaefer et al. reported that PET/CT was particularly useful in demonstrating absence of residual active disease in adult lymphoma after treatment (15). As absence of FDG uptake on the residual soft tissue is known to be a strong indicator for better prognosis in adults (20,21), accurate interpretation with confidence is valuable in managing patients in a posttreatment status. PET/CT has an advantage over CI or PET alone in this regard as well.
Another major discrepant finding was observed in small lymph node lesions, in which PET/CT and CI showed true-positive and false-negative findings, respectively. A size criterion has long been used in discriminating metastatic lymph nodes from benign ones, but its limited sensitivity for small malignant nodes is already well recognized (22). Our group reported—using PET/CT—that 23% of all lesions with a true-positive PET finding were diagnosed as negative on CT in adult lymphoma (23). As PET/CT allowed evaluation of FDG uptake while viewing completely corresponding CT images, it is obviously superior to PET alone in detecting small lesions or in characterizing the FDG uptake.
Although PET/CT is generally useful in evaluating various types of malignant lesions, it is considered to have limited sensitivity to detect tiny lesions in the liver, where moderate-to-intermediate FDG uptake is observed as physiologic background on PET. The CT portion of PET/CT without intravenous contrast is insufficient to evaluate small liver lesions—even they represent low attenuation as they cannot be discriminated from cysts. Contrast CT or MRI appears to have better sensitivity for small metastatic liver lesions. Sahani et al. (24) or Ghanem et al. (25) reported that MRI detected significantly more and smaller liver metastatic lesions than did FDG PET. In this study, 2 liver metastatic lesions were detected only on CI. This phenomenon should be kept in mind as a possible reason for false-negative PET/CT findings. This also can occur in small lung lesions.
The examination-based analysis revealed that PET/CT provided no additional information (type A) to CI in 63% of all examinations compared (68/108). The 68 examinations included 15 having residual soft tissue after treatment, which exhibited the findings of negative PET/CT and no interval change repeatedly on CI. Depending on the criteria for discrepant PET/CT and CI findings, they might have been considered to be the examinations with additional information in other studies. The soft-tissue masses with negative PET/CT findings in a posttreatment status are highly suggestive of scar in most instances; thus, this discrepant PET/CT and CI finding is helpful in examinations without previous follow-up information.
Additional information of PET/CT to CI was observed in 37 (34%) of the 108 examinations: 23 (21%) as negative PET/CT findings (downstaging or exclusion of residual viable lesions [possible influence of treatment strategy as negative findings]) and 14 (13%) as positive PET/CT findings (2 < 2% > with identification of more lesions without upstaging or possible influence of treatment strategy and 12 < 11% > with upstaging or possible influence of treatment strategy). Except for the positive PET/CT findings without upstaging, additional information of PET/CT potentially affects treatment strategy or patient management. Thus, PET/CT appeared to provide more valuable information than CI with regard to treatment in about 30% of examinations compared in this study. This percentage was higher than the data by Antoch et al. (26) or by Bar-Shalom et al. (27) but was similar to the data by Israel et al. (28), who reported that PET/CT had an impact on adult patient management in 33% of patients with suspected recurrence. Most of the examinations included in this study were performed in a posttreatment status. The percentage of clinical impact of PET/CT appears to be influenced by the number of patients in a posttreatment status.
Forty-three of all 151 PET/CT examinations in this study were not accompanied by CI. All except one of them were performed in a posttreatment status, and many of them were parts of repeat PET/CT examinations. This suggests that the referring pediatricians selected PET/CT as a sole imaging modality to evaluate patient disease status during a certain period and relied on the PET/CT findings. Especially as a follow-up examination, PET/CT appears to be the best imaging modality currently, as it provides both PET and CT information simultaneously in pediatric patients, in whom fewer examinations are preferable. PET/CT with intravenous contrast may be more useful in detecting small lesions, but the feasibility of this method in a pediatric population should be adequately evaluated in view of a burden on the small body.
Radiation exposure should be fully considered in examinations of pediatric patients. In this study the injection dose of 18F-FDG was determined by patient weight (5.55 MBq/kg [0.15 mCi/kg] body weight), and the tube current of the CT portion of PET/CT was also dependent on the weight (40 mA for <45.3 kg and 60 mA for <68 kg). Thus, the total radiation dose per examination was lower in general than that in adult patients, while the image quality of the PET or CT portion in each examination was kept sufficient. However, further reduction of radiation dose per examination may be necessary, if applicable, in pediatric patients requiring repeat imaging evaluation, such as patients with lymphoma. MRI has a huge advantage in this regard. Recent advances in its high-quality images and a fast data-acquisition protocol have produced many opportunities in clinical situations. Although accurate evaluation of lesion viability, especially after treatment, seems to be a role for PET, roles for MRI in the management of pediatric malignancies should be adequately assessed in other studies.
This study dealt with many patients with various kinds of non-CNS malignant tumors. We did not evaluate lesion malignancy semiquantitatively using the standardized uptake value (SUV) because of this inhomogeneity. We believe the SUV is useful to assess changes of activity at the specific lesion before and after chemo- or radiation therapy. However, use of the SUV is questionable to differentiate benign and malignant lesions. In retrospect, most of our patients had lymphoma. The International Harmonization Project in Lymphoma has recently released its recommendation that visual assessment alone appears to be adequate for determining whether PET is positive or negative at the conclusion of therapy, and quantitative or semiquantitative approaches (e.g., using SUV) do not seem necessary (29).
There were some limitations in this study. As this was a retrospective study dealing with many patients with lymphoma or patients to evaluate recurrence, we had histologic proof for only a limited number of lesions. Thus, we assessed the accuracy of PET/CT and CI findings on the basis of the reference standard, which consisted primarily of follow-up results. Considering the situation that referring physicians do not obtain histopathologic verification for all suspected lesions, in part due to an ethical consideration, the lack of proof is a known limitation in general for this type of imaging study. However, many patients in this study had PET/CT and CI examinations repeatedly; thus, the information from the reference standard was thought to be very reliable. Inclusion of patients with soft-tissue masses in a posttreatment status, which proved to represent true-negative PET/CT and false-positive CI findings, might have been a selection bias, but was inevitable because pediatric patients having PET/CT examinations were consecutively involved in this study. Another limitation may be the heterogeneous patient population. This study was conducted to clarify the efficacy of PET/CT in pediatric malignancies and to determine if PET/CT provided additional diagnostic information on disease status as compared with CI methods. Now that PET/CT was demonstrated to be useful in evaluating pediatric malignancies as a whole in this study, further studies are warranted in specific pediatric malignancies.
CONCLUSION
PET/CT exhibited significantly higher sensitivity, specificity, and accuracy than CI and showed accurate findings in 90% (72/80) of lesions with discordant findings between them. PET/CT was useful to detect small lymph node lesions diagnosed as negative on CI and to deny the presence of active disease in soft-tissue masses in a posttreatment status. Additional information of PET/CT to CI was observed in more than one third of examinations compared. PET/CT is a promising imaging modality in evaluating pediatric malignancies.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 28, 2007.
- Accepted for publication August 18, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}