


Article Figures & Data
Figures
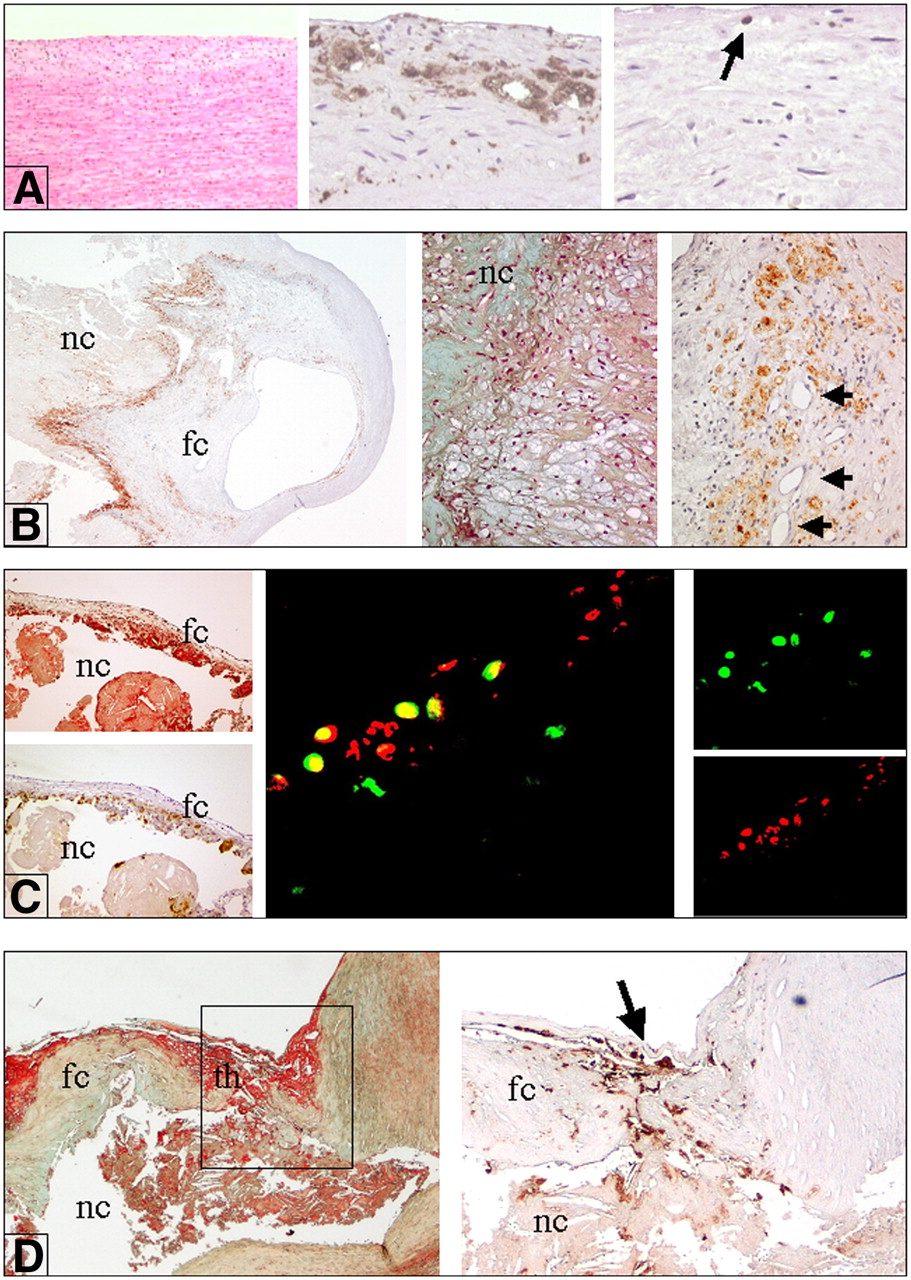
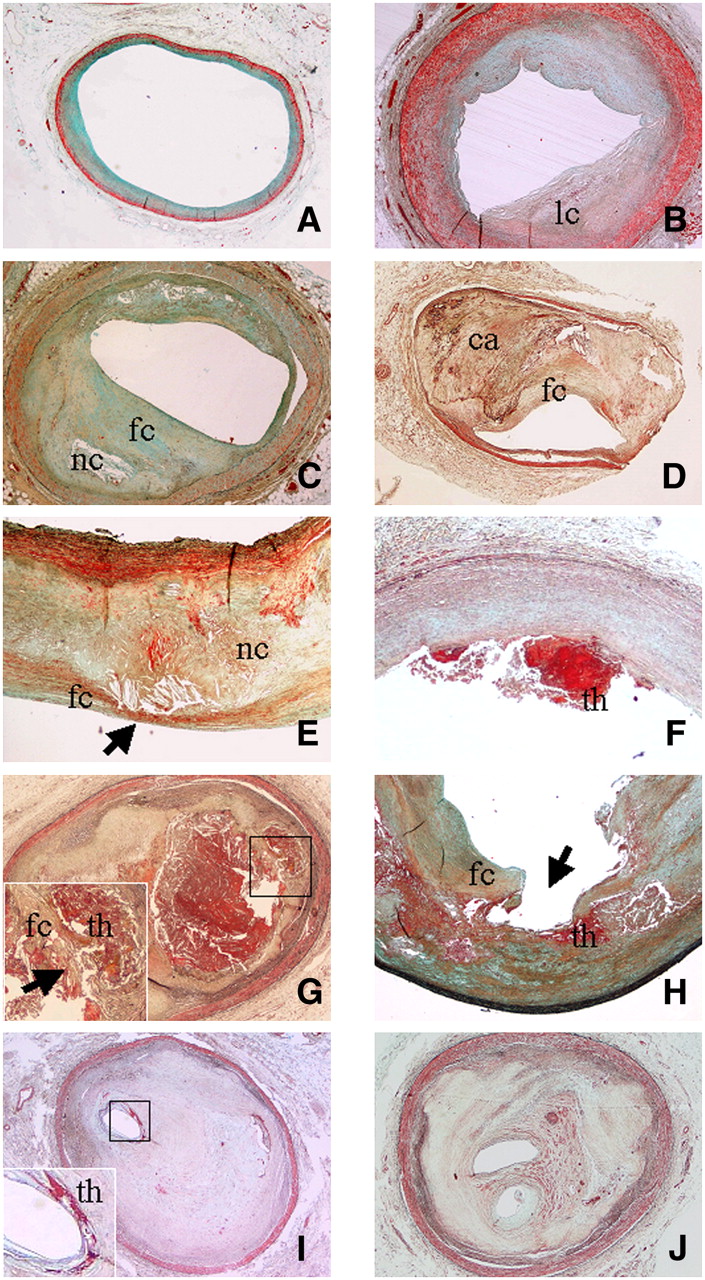
- FIGURE 1.
Various types of atherosclerotic lesions. (A) Diffuse intimal thickening consisting mainly of smooth muscle cells in proteoglycan-rich matrix (Movat stain; magnification, ×2). (B) Pathologic intimal thickening associated with some deep lipid core (lc) without necrosis (Movat stain; magnification, ×2). (C) Fibrous cap atheroma characterized by presence of large lipidic–necrotic core (nc) consisting of extracellular lipid, cholesterol crystals, and necrotic debris, covered by thick fibrous cap (fc), with various degrees of infiltration by macrophages and T lymphocytes (Movat stain; magnification, ×2). (D) Fibrocalcific plaque characterized by small lipid-laden necrotic core and thick fibrous cap (fc) overlying extensive accumulation of calcium (ca) in intima (Movat stain; magnification, ×2). (E) Vulnerable plaque (thin fibrous cap atheroma) characterized by large lipidic–necrotic core (nc) associated with thin inflamed fibrous cap (fc; arrow) (Movat stain; magnification, ×2). (F) Plaque erosion showing area of acute thrombosis (th) associated with superficial erosion of endothelium without fibrous cap rupture (Movat stain; magnification, ×2). (G) Fibrous cap (fc) rupture with lumen-occluding thrombus (th) (Movat stain; magnification, ×2). Inset shows site of cap rupture. Arrow indicates acute thrombosis. (H) Plaque rupture with ulceration (arrow), characterized by excavated necrotic core with discontinuation of fibrous cap (fc) (Movat stain; magnification, ×2). Acute thrombus is indicated by th. (I) Thrombotically active plaque characterized by stratified organizing thrombus (dense collagen interspersed with proteoglycan matrix) associated with area of acute thrombosis (th; inset) near residual lumen (Movat stain; magnification, ×2). (J) Healed lesion with lumen almost totally occluded, characterized by distinct layers of dense collagen interspersed with proteoglycan matrix (Movat stain; magnification, ×2).
- FIGURE 2.
Inflammation in various types of atherosclerotic plaques. (A) Intimal thickening, characterized by smooth muscle cells (left; hematoxylin–eosin stain; magnification, ×10), a few fat-laden macrophages (foam cells) (middle; immunostaining with anti-CD68; magnification, ×10), and scattered T lymphocytes (arrow) (right; immunostaining with anti-CD3; magnification, ×10). (B) Stable plaque (fibrous cap atheroma). Immunohistochemical stain for CD68 (anti-human monocytes and macrophages) shows diffuse positive reaction near lipidic–necrotic core (nc) and large numbers of macrophage foam cells (left; anti-CD68; magnification, ×2) (middle; Movat stain; magnification, ×10). In contrast, only a few macrophages are present in fibrous cap (fc). Numerous macrophage foam cells, positive for CD68, are present near newly formed vessels (arrows) (right; anti-CD68; magnification, ×10). (C) (Left) Vulnerable plaque, characterized by large lipidic–necrotic core (nc) associated with thin fibrous cap (fc) (top; Movat stain; magnification, ×4) rich in inflammatory macrophage foam cells (bottom; immunostaining for CD68; magnification, ×4). (Middle) CXCR3 (fractalkine receptor) expression in activated T lymphocytes. Double fluorescence immunostain studied by 2-dimensional confocal analysis clearly shows diffuse positive reaction for CXCR3 in activated T lymphocytes (concordant double positivity appears as yellow stain) (magnification, ×800). (Right Top) CXCR3 reaction revealed by streptavidin–fluorescein conjugate (green stain). (Right Bottom) CD25 (IL-2 receptor antigen) antibody revealed by streptavidin–Texas Red fluorescent conjugate (red stain). (D) Unstable thrombotic plaque. nc = lipidic–necrotic core. (Left) Site of rupture of thin cap (fc) associated with acute thrombus (th) (Movat stain; magnification, ×4). (Right) Fibrous cap at site of rupture (arrow) showing many CD68-positive macrophages.
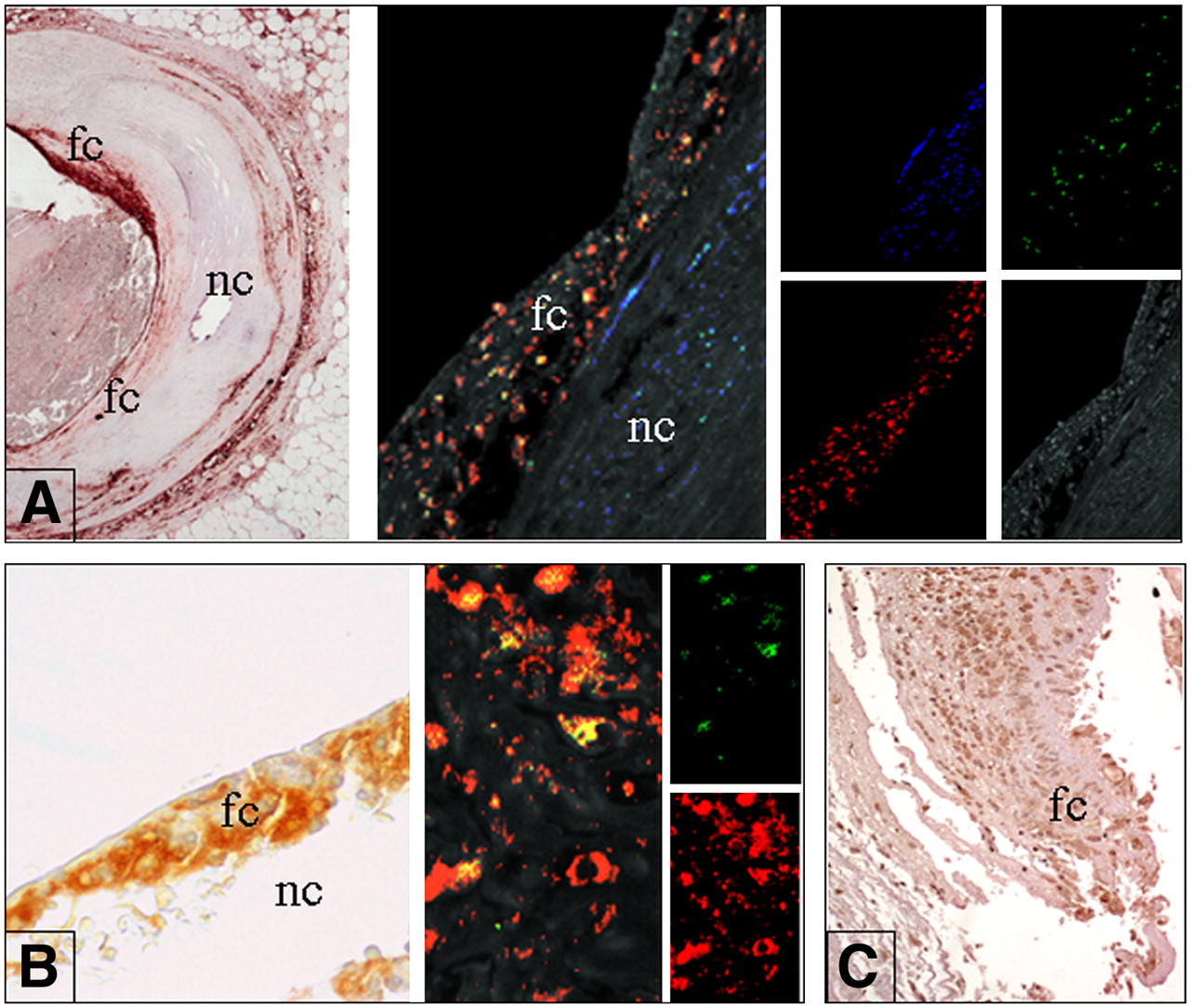
- FIGURE 3.
In situ expression of molecular factors. (A) In situ expression of PTX-3. (Left) Cross section of coronary artery (low-power field; magnification, ×4). Shoulder area of eroded plaque shows strong positivity for PTX-3 (conventional immunohistochemistry; 3,3′-diaminobenzidine [DAB] revealed). (Middle) Triple fluorescence immunostain studied by 2-dimensional confocal analysis demonstrates that PTX is mainly expressed by macrophages (concordant double positivity appears as yellow stain). (Right) Confocal analysis showing smooth muscle actin (smooth muscle cell antigen) reaction revealed by streptavidin–Alexa fluor 430 (Molecular Probes/Invitrogen) conjugate (blue stain), CD68 (macrophage antigen) reaction revealed by streptavidin–Texas Red fluorescent conjugate (red stain), and PTX3 reaction revealed by streptavidin–fluorescein conjugate (green stain). Plaque background is shown at bottom right (medium wave excitation UV filter). fc = fibrous cap; nc = necrotic core. (B) Expression of PAPP-A. (Left) Thin cap of ruptured plaque is rich in foam cells (fc) expressing PAPP-A at high levels and covering large necrotic core (nc) (magnification, ×40; conventional immunohistochemistry; DAB revealed). (Middle) Double fluorescent immunostain studied by 2-dimensional confocal analysis clearly shows strong and diffuse positive reaction for PAPP-A in macrophages (concordant double positivity appears as yellow stain) (magnification, ×800). (Right Top) PAPP-A reaction revealed by streptavidin–fluorescein conjugate (green stain). (Right Bottom) CD68 antibody revealed by streptavidin–Texas Red fluorescent conjugate (red stain). (C) Foam cells (fc) at site of plaque rupture strongly express IL-6 (magnification, ×20; conventional immunohistochemistry; DAB revealed).
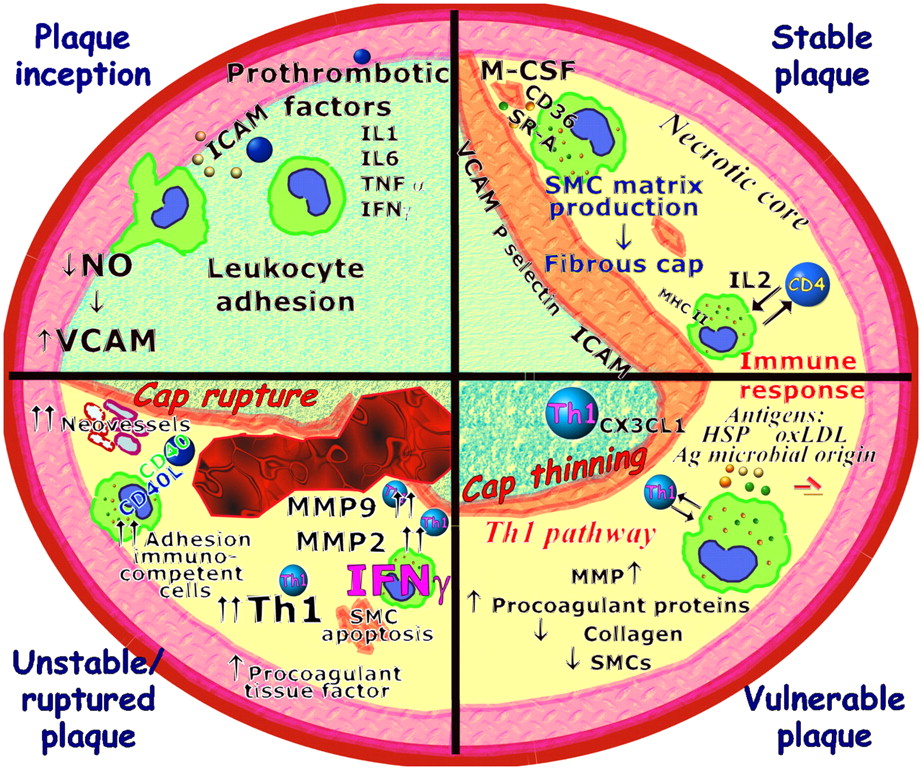
- FIGURE 4.
Molecular factors involved in plaque evolution. In plaque inception, activated endothelial cells increase expression of adhesion molecules and inflammatory genes. Circulating monocytes migrate into subendothelial space and differentiate into macrophages. Macrophages take up lipid deposited in intima via several receptors, including scavenger receptor A (SR-A) and CD36. Lipid-laden macrophages forming fatty streak secrete MMPs, tissue factor, and proinflammatory cytokines that amplify local inflammatory response in lesion. Repeated cycles of inflammation lead to accumulation of macrophages, some of which can die in this location, producing so-called necrotic core, and induce smooth muscle cell (SMC) proliferation and migration in lesion to form fibrous cap of advanced complicated stable atherosclerotic lesion (stable plaque). T cells may encounter antigens (Ag), such as OxLDL and heat shock proteins (HSP) of endogenous or microbial origins. Several different effector mechanisms can be elicited by immune response. Combination of IFN-γ and TNF-α upregulates expression of fractalkine (CX3CL1). This cytokine network promotes development of Th1 pathway, which is strongly proinflammatory and induces macrophage activation, superoxide production, and protease activity. Selective recruitment and activation of Th1 T cells determine potent inflammatory cascade favoring transition from stable plaque to unstable or ruptured plaque. During this transition, existence of theoretic plaque structure known as vulnerable plaque, which is very similar to unstable plaque except for plaque erosion or rupture, has been postulated.


Tables
Standard American Heart Association classification* Revised morphologic classification† Type I: initial lesion Nonatherosclerotic intimal lesions Type IIa: progression-prone type II lesion Intimal thickening Type IIb: progression-resistant type II lesion Fatty streak Type III: intermediate lesion (preatheroma) Progressive atherosclerotic lesions Type IV: atheroma Stable plaques Type Va: fibroatheroma (type V lesion) Pathologic intimal thickening Type Vb: calcific lesion (type VII lesion) Fibrous cap atheromas Type Vc: fibrotic lesion (type VIII lesion) Fibrocalcific lesions Type VI: complicated lesion Vulnerable plaques VIa: with surface defect Thin fibrous cap atheromas VIb: with hematoma–hemorrhage Calcified nodule VIc: with thrombotic deposit Unstable thrombotic plaques Plaque rupture with luminal thrombus Plaque rupture with ulceration Plaque erosion Calcified nodule Healed lesions Metabolic and immune disorders Hypercoagulability Complex atherosclerotic plaque Abnormal lipoprotein profile [e.g., high LDL, low HDL, and Lp(a)] Markers of blood hypercoagulability (e.g., fibrinogen, d-dimer, and factor V of Leiden) Morphology and structure Nonspecific markers of inflammation (e.g., hs-CRP, CD40L, ICAM-1, and VCAM-1), leukocytosis, and other immunologic and serologic markers that may not be specific for atherosclerosis and plaque inflammation Increased platelet activation and aggregation (e.g., gene polymorphisms of platelet glycoproteins IIb/IIIa, Ia/IIa, and Ib/IX) Cap thickness Serum markers of metabolic syndrome (diabetes or hypertriglyceridemia) Increased coagulation factors (e.g., clotting factors V, VII, VIII, and XIII and von Willebrand factor) Lipid core size Specific markers of immune system activation (e.g., anti-LDL antibody and anti–heat shock protein antibody) Decreased anticoagulation factors (e.g., proteins S and C, thrombomodulin, and antithrombin III) Percentage of stenosis Markers of lipid peroxidation (e.g., OxLDL and oxidized HDL) Decreased endogenous fibrinolytic activity (e.g., decreased tissue plasminogen activator, increased type I plasminogen activator [PAI], and PAI polymorphisms) Remodeling (positive vs. negative) Homocysteine Prothrombin mutation (e.g., G20210A) Color (yellow or red) PAPP-A Thrombogenic factors (e.g., anticardiolipin antibodies, thrombocytosis, sickle cell disease, diabetes, and hypercholesterolemia) Collagen content vs. lipid content Circulating apoptosis markers (e.g., Fas and Fas ligand) Transient hypercoagulability (e.g., smoking, dehydration, and infection) Calcification burden and pattern ADMA and dimethylarginine dimethylaminohydrolase Shear stress Circulating nonesterified fatty acids Activity and function Plaque inflammation (macrophage density and rate of monocyte and activated T-cell infiltration) Endothelial denudation or dysfunction (local NO production and anti- or procoagulation properties of endothelium) Plaque oxidative stress Superficial platelet aggregation and fibrin deposition Rate of apoptosis (apoptosis protein markers and microsatellites) Angiogenesis, leaking vasa vasorum, and intraplaque hemorrhage MMPs (MMP-2, MMP-3, and MMP-9) Microbial antigens (Chlamydia pneumoniae) Temperature Global features Transcoronary gradient of vulnerability biomarkers Total calcium burden Total coronary vasoreactivity Total arterial plaque burden (intima–media thickness)





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- NATURAL HISTORY OF ATHEROSCLEROTIC PLAQUES
- MOLECULAR FACTORS ACTING ON NATURAL HISTORY OF ATHEROSCLEROSIS
- PATHOBIOLOGIC DETERMINANTS OF PLAQUE RUPTURE
- POTENTIAL FACTORS CONTRIBUTING TO PLAQUE INSTABILITY
- DIFFUSE INFLAMMATION AND VULNERABILITY
- SERUM MARKERS CORRELATED WITH PLAQUE INFLAMMATION
- FUTURE CHALLENGES IN TREATMENT OF VULNERABLE PLAQUES
- CONCLUSION
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Association between endostatin and mortality in patients with acute dyspnoea, with or without congestive heart failure: a single-centre, prospective, observational study
- A Prediction Tool for Plaque Progression Based on Patient-specific Multi-Physical Modeling
- High-Density Lipoprotein-Associated Apolipoprotein M Limits Endothelial Inflammation by Delivering Sphingosine-1-Phosphate to the Sphingosine-1-Phosphate Receptor 1
- Supraclavicular Brown Adipose Tissue 18F-FDG Uptake and Cardiovascular Disease
- Age- and Hypertension-Associated Protein Aggregates in Mouse Heart Have Similar Proteomic Profiles
- Relationship Between Measures of Adiposity, Arterial Inflammation, and Subsequent Cardiovascular Events
- Myocardin Regulates Vascular Smooth Muscle Cell Inflammatory Activation and Disease
- In Vivo Evaluation of Atherosclerotic Plaque Inflammation and of Anti-Inflammatory Effects of Statins by 18F-Fluorodeoxyglucose Positron Emission Tomography
- Interleukin-1 Mediates Neuroinflammatory Changes Associated With Diet-Induced Atherosclerosis
- Carotid Plaque Inflammation Is Associated With Cerebral Microembolism in Patients With Recent Transient Ischemic Attack or Stroke: A Pilot Study
- Watershed Infarcts in Transient Ischemic Attack/Minor Stroke With >=50% Carotid Stenosis: Hemodynamic or Embolic?
- Multimodality Cardiovascular Molecular Imaging Technology
- Insufficient Deactivation of the Protein Tyrosine Kinase Lck Amplifies T-Cell Responsiveness in Acute Coronary Syndrome
- One Step Closer to Imaging Vulnerable Plaque in the Coronary Arteries