


Abstract
Angina pectoris is a major symptom associated with myocardial ischemia. The aim of this study was to find whether stress myocardial perfusion imaging can independently predict mortality in patients with angina. Methods: We studied 455 patients with stable angina pectoris by exercise or dobutamine stress 99mTc-tetrofosmin myocardial perfusion tomographic imaging. An abnormal finding was defined as a reversible or fixed perfusion abnormality. The endpoint during follow-up was death from any cause. Results: Mean age was 60 ± 10 y. There were 266 men (58% of the patients). Myocardial perfusion was normal in 137 patients (30%). Perfusion abnormalities were reversible in 167 patients and fixed in 151 patients. During a mean follow-up of 6 ± 1.7 y, 93 patients (20%) died. The annual mortality rate was 1.5% in patients with normal perfusion and 4.5% in patients with abnormal perfusion. Patients with a multivessel distribution of perfusion abnormalities had a higher annual death rate than patients with abnormalities in a single-vessel distribution (5.1% vs. 3.7%). In a multivariate analysis model, independent predictors of death were age (risk ratio, 1.05; 95% confidence interval [CI], 1.03–1.08), the male sex (risk ratio, 2.1; CI, 1.3–3.4), diabetes (risk ratio, 2.2; CI, 1.4–3.5), heart failure (risk ratio, 2.7; CI, 1.6–4.5), smoking (risk ratio, 1.7; CI, 1.1–2.6), reversible perfusion abnormalities (risk ratio, 1.9; CI, 1.1–2.8), and fixed perfusion abnormalities (risk ratio, 2; CI, 1.2–3.1). Conclusion: Stress 99mTc-tetrofosmin myocardial perfusion imaging provides independent information for predicting mortality in patients with stable angina pectoris. Both reversible and fixed defects are associated with an increased risk of death. The extent of stress perfusion abnormalities is a major determinant of mortality. Patients with normal perfusion have a low mortality rate during long-term follow-up.
Evaluation of patients’ clinical and symptomatic status provides the physician with important data on the probability that coronary artery disease (CAD) is present (1,2). Angina pectoris is a cardinal symptom that alerts the physician to a high probability of the presence of myocardial ischemia. However, because of the relatively low specificity of anginal symptoms in predicting underlying obstructive CAD, it may not be justifiable to submit all patients with angina to invasive procedures in the absence of more specific signs of myocardial ischemia (3,4). According to the Bayesian theory, the probability of CAD does not change substantially in patients with a high pretest probability of CAD if they had negative results on stress testing (1). It is not known whether these patients remain at high risk for mortality at long-term follow-up irrespective of their stress test results.
Stress myocardial perfusion imaging is a valuable tool for the diagnosis and risk stratification of CAD (5–12). Although many previous studies have shown that the technique identifies patients at high risk of future cardiac events, its independent clinical value in predicting long-term mortality in patients with angina has not been well established. The clinical value of various stress-testing modalities has been recognized mainly in patients with an intermediate pretest probability of CAD (4,9,10). Because patients with angina have a high probability of myocardial ischemia, they are expected to have a high rate of future cardiac events. It is not known whether stress myocardial perfusion imaging can permit further classification of these patients into high- and low-risk categories and thereby guide the physician in the selection of patients who require invasive procedures. The aim of this study was to assess the independent value of stress 99mTc-tetrofosmin SPECT in predicting mortality and hard cardiac events in patients with stable angina pectoris.
MATERIALS AND METHODS
Patients
The initial study population consisted of 458 consecutive patients referred to our laboratory between January 1996 and December 2002 for exercise or dobutamine stress 99mTc-tetrofosmin SPECT to evaluate typical anginal complaints. Contraindications for stress testing were unstable angina, uncontrolled heart failure, and severe valvular heart disease. The choice of stress test was based on ability to exercise. Follow-up was successful in 455 patients (99%). The data of these patients are reported. All patients gave informed consent before the test. The Ethics Committee of the University Hospital Rotterdam approved the protocol. A structured interview and clinical history were acquired and cardiac risk factors were assessed before nuclear testing. Diabetes mellitus was defined as a fasting glucose level ≥ 140 mg/dL or the need for insulin or oral hypoglycemic agents. Hypercholesterolemia was defined as a total cholesterol level ≥ 200 mg/dL or treatment with lipid-lowering medications. Hypertension was defined as blood pressure ≥ 140/90 mm Hg or the use of antihypertensive medication.
Stress Test Protocols
Patients were instructed to discontinue β-blockers at least 24 h before the stress test, whenever applicable. Other medications were not routinely discontinued. For 165 patients, an exercise stress test was performed, using symptom-limited upright bicycle ergometry with a stepwise increment of 20 W every minute. For 290 patients, dobutamine-atropine stress testing was performed. Dobutamine was infused intravenously, starting at a dose of 10 μg/kg/min for 3 min, and increasing by 10 μg/kg/min every 3 min to a maximum of 40 μg/kg/min (11,12). If the test endpoint was not reached at a dobutamine dose of 40 μg/kg/min, atropine (up to 1 mg) was given intravenously. Blood pressure, heart rate, and electrocardiography were continuously monitored. Test endpoints were achievement of target heart rate (85% of maximum age-predicted heart rate); horizontal or downsloping ST-segment depression > 2 mm at an interval of 80 ms after the J point, compared with baseline; severe angina; a systolic blood pressure fall of >40 mm Hg; blood pressure > 240/120 mm Hg; and significant cardiac arrhythmia. Metoprolol was available to reverse the side effects of dobutamine/atropine if these did not revert spontaneously.
Three electrocardiographic leads were continuously monitored. Cuff blood pressure measurements and the 12-lead electrocardiogram were recorded at rest and every minute during stress and recovery. Computer averaging of the electrocardiographic complexes was performed with both stress tests. Significant ST-segment depression was defined as a >1-mm horizontal or downsloping ST-segment depression occurring at 80 ms after the J point.
99mTc-Tetrofosmin SPECT Imaging
An intravenous dose of 370 MBq of 99mTc-tetrofosmin (Myoview; Amersham) was administered approximately 1 min before termination of the dobutamine or exercise test (9,12). For resting studies, 370 MBq of tetrofosmin were injected at least 24 h after the exercise study. Images were acquired with a Gammasonics single-head Rota camera (Orbiter; Siemens) without attenuation or scatter correction, using a low-energy all-purpose collimator. Thirty-two projections were obtained over a 180° arc from left posterior oblique to right anterior oblique, with an acquisition time of 45 s per projection. Data were collected in a 64 × 64 matrix (word mode), and images were reconstructed using a filtered backprojection algorithm and a ramp reconstruction filter. Transverse images were reconstructed using a software package (SPETS; Nuclear Diagnostics). From the 3-dimensional data, oblique (short-axis) and sagittal (vertical long-axis) images obtained perpendicular and parallel to the long axis, respectively, were reconstructed. For each study, 6 oblique (short-axis) slices from the apex to the base and 3 sagittal (vertical long-axis) slices were defined. Each of the 6 short-axis slices was divided into 8 equal segments. The septal part of the 2 basal slices was excluded from analysis because this region corresponds to the fibrous portion of the interventricular septum and normally exhibits reduced uptake. Consequently, a total of 47 segments were identified (3 long-axis and 44 short-axis). The scan was semiquantitatively interpreted by visual analysis. Stress and rest tomographic views were reviewed side by side by an experienced observer who was unaware of the patients’ clinical data. A reversible perfusion defect was defined as a perfusion defect on stress images that partially or completely resolved at rest in ≥2 contiguous segments or slices in the 47-segment model. This was considered diagnostic of myocardial ischemia. A fixed perfusion defect was defined as a perfusion defect on stress images in 2 or more contiguous segments or slices, which persisted on rest images in the 47-segment model. An abnormal study was considered to be one showing a fixed or reversible perfusion defect.
The impact of the extent of perfusion abnormalities on outcome was evaluated by estimating the number of coronary arterial territories with perfusion abnormalities on the stress images, as previously described (12). Myocardial segments were assigned to corresponding coronary arteries as follows: the anterior wall and anterior septum to the left anterior descending coronary artery, the posterolateral wall to the left circumflex coronary artery, and the basal posterior septum and the inferior wall to the right coronary artery. The apex was assigned to the arterial distribution with concomitant perfusion abnormalities. Isolated apical abnormalities were considered indicative of single-vessel CAD.
Follow-up
Follow-up data were collected by contacting the patient’s general practitioner and reviewing hospital records. In addition, vital status was verified through the civil data registry. Two endpoints were considered: death from any cause and hard cardiac events (cardiac death and nonfatal myocardial infarction, defined by cardiac enzyme levels and electrocardiographic changes). Death was considered cardiac if it was caused by acute myocardial infarction, significant arrhythmias, or refractory heart failure. Sudden unexpected death occurring without another explanation was included as cardiac death. Myocardial revascularization procedures were also noted. Patients who underwent revascularization within 3 mo of the stress test were censored at the time of revascularization. The annual event rate was calculated by dividing the number of events by the number of patients followed in each year, during the 7 y after the stress test. A mean was obtained by adding these rates and dividing by 7.
Statistical Analysis
Continuous data were expressed as mean value ± SD. The Student t test was used to analyze continuous data. Differences between proportions were compared using the χ2 test. Univariate and multivariate Cox proportional hazard regression models (BMDP Statistical Software Inc.) were used to identify independent predictors of events. Parameters considered for multivariate analysis were those with P < 0.05 in the univariate analysis. Variables were selected in a stepwise forward manner, with entry and retention set at a significance level of 0.05. The probability of survival was calculated using the Kaplan–Meier method, and survival curves were compared using the log-rank test.
RESULTS
Clinical Data
Mean age was 60 ± 10 y. There were 226 men (58% of the patients). Risk factors for CAD were hypertension in 211 patients (46%), diabetes mellitus in 87 patients (19%), hypercholesterolemia in 213 patients (47%), and smoking in 152 patients (33%). One hundred twenty patients (26%) had a history of previous myocardial infarction, 135 patients (30%) underwent previous myocardial revascularization procedures, and 45 patients (10%) had a history of congestive heart failure. Medications included β-blockers in 273 patients (60%), angiotensin-converting enzyme inhibitors in 141 patients (31%), and calcium channel blockers in 236 patients (52%).
Stress Test Data
There was a significant increase of heart rate (71 ± 15 vs. 131 ± 22 beats/min) and systolic blood pressure (138 ± 24 vs. 164 ± 31 mm Hg) from rest to peak stress, respectively. With stress, ST-segment depression occurred in 100 patients (22%) and angina occurred in 191 patients (42%). The mean achieved workload with exercise was 137 ± 45 W. The mean maximal dobutamine dose was 34 ± 10 μg/kg/min. Atropine was administered to 140 patients. The target heart rate was achieved in 387 patients (85%).
SPECT and Follow-up Results
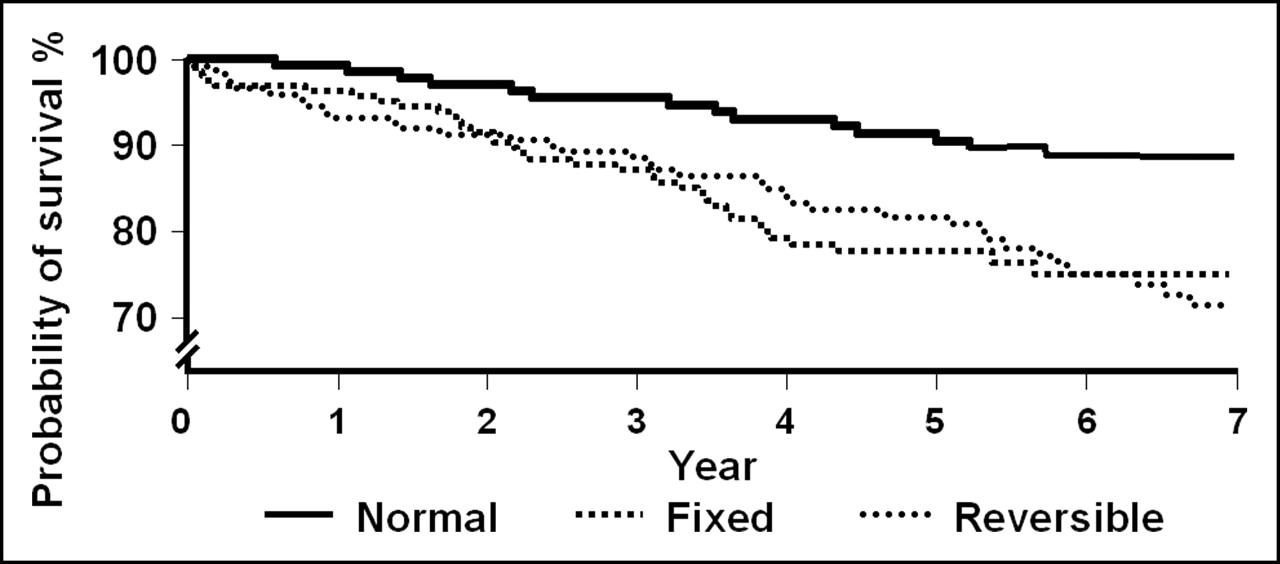
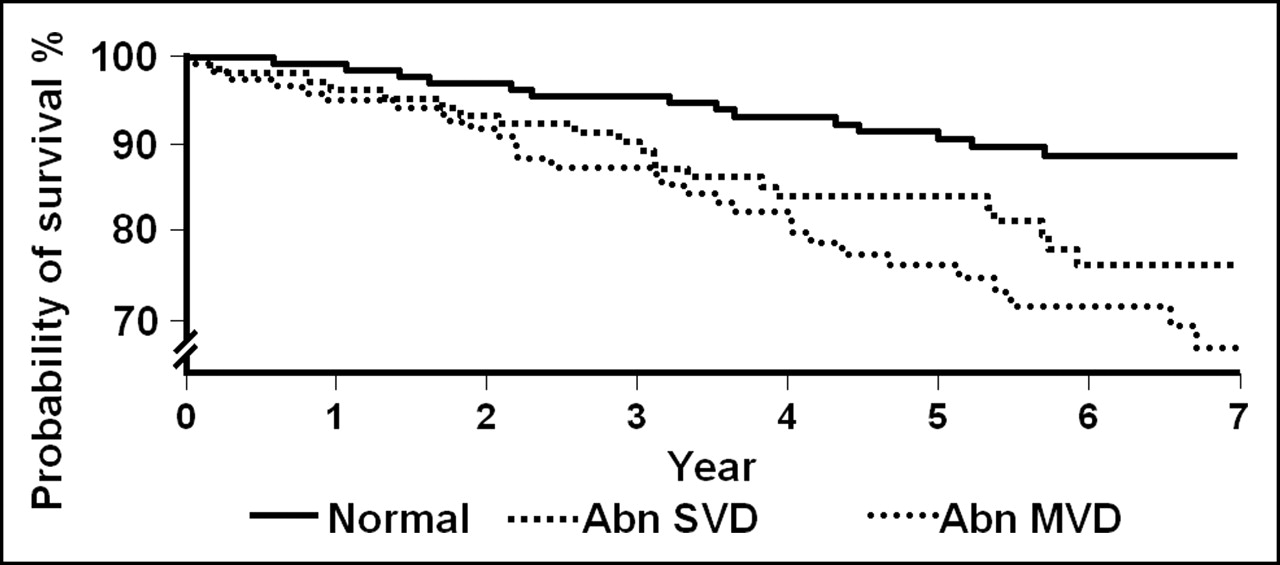
Myocardial perfusion was normal in 137 patients (30%). Myocardial perfusion abnormalities were fixed in 151 patients (33%) and reversible in 167 patients (37%). Among patients with reversible defects, 47 had completely reversible defects and 120 had resting perfusion defects as well. Perfusion abnormalities were observed in a single-vessel distribution in 145 patients and in a multivessel distribution in 173 patients. During a mean follow-up period of 6 ± 1.7 y, 93 patients (20%) died. Death was considered cardiac in 46 patients (10%). Nonfatal myocardial infarction occurred in 40 patients (9%), and 152 patients (33%) underwent coronary revascularization. This was performed early (within 90 d) in 35 and late in 117 patients. The annual mortality rate was 1.5% in patients with normal perfusion and 4.5% in patients with abnormal perfusion. Both reversible and fixed abnormalities were associated with increased risk of death (Fig. 1). The annual death rate was 5.1% in patients with a multivessel distribution of perfusion abnormalities and 3.7% in patients with a single-vessel distribution (P < 0.05). Survival curves based on extent of perfusion abnormalities are presented in Figure 2. The annual hard cardiac event rate was 1.2% in patients with normal perfusion and 3.9% in patients with abnormal perfusion (Fig. 3). Patients with a multivessel distribution of abnormalities had a higher hard cardiac event rate than patients with a single-vessel distribution of abnormalities (4.8% vs. 3.1%, P < 0.05) (Fig. 4). Univariate and multivariate predictors of events are presented in Table 1. Cumulative survival and event-free survival rates at 1, 3, 5, and 7 y based on presence and extent of perfusion abnormalities are presented in Table 2.
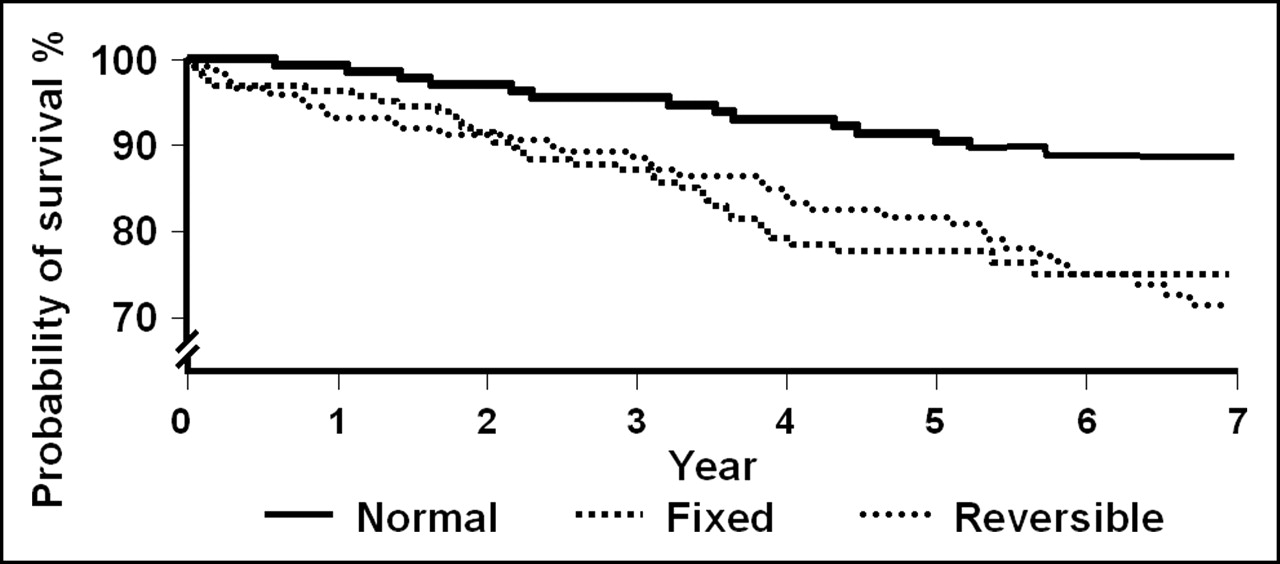
Unadjusted Kaplan–Meier survival curves (all-cause mortality) according to presence and type of perfusion abnormality.
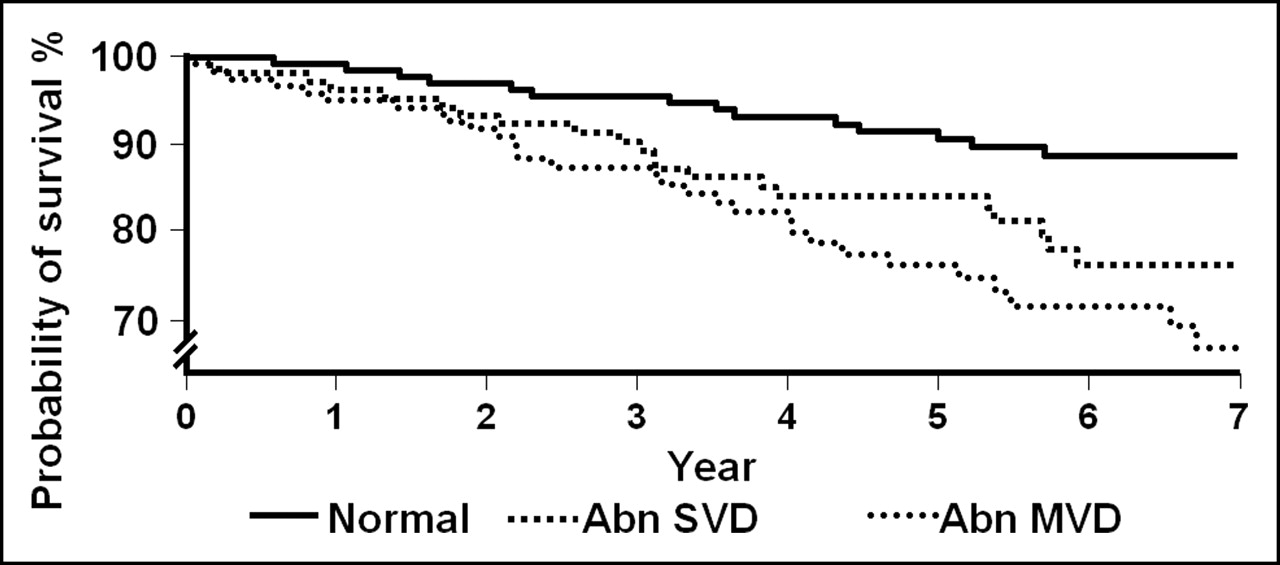
Unadjusted Kaplan–Meier survival curves (all-cause mortality) according to presence and extent of perfusion abnormality. Abn = abnormal; MVD = multivessel distribution; SVD = single-vessel distribution.

Unadjusted Kaplan–Meier survival curves (hard cardiac events) according to presence and type of perfusion abnormality.

Unadjusted Kaplan–Meier survival curves (hard cardiac events) according to presence and extent of perfusion abnormality. Abn = abnormal; MVD = multivessel distribution; SVD = single-vessel distribution.
Predictors of Hard Cardiac Events by Cox Models
Survival and Event-Free Survival Rates According to Presence and Extent of Perfusion Abnormalities
DISCUSSION
In this study, stress 99mTc-tetrofosmin SPECT provided independent prognostic information for predicting all-cause mortality as well as hard cardiac events in patients with stable angina pectoris. Patients with normal perfusion had a lower risk of death and hard cardiac events, whereas in patients with abnormal perfusion, the mortality and hard cardiac event rates were substantially higher. Patients with a multivessel distribution of perfusion abnormalities were at greatest risk, with an annual death rate of 5.1% and an annual hard cardiac event rate of 4.8%. Both fixed and reversible perfusion abnormalities were predictive of mortality. Older age, the male sex, diabetes mellitus, and a history of congestive heart failure were independent clinical predictors of outcome. The risk associated with abnormal perfusion persisted after adjustment to other clinical parameters.
Myocardial perfusion was normal in 30% of the population. The results of our study indicate that patients with normal results on stress 99mTc-tetrofosmin myocardial perfusion imaging have a low event rate during long-term follow-up. The findings have important clinical implications because these patients can be exempted from invasive studies unless clinical status changes. A policy of proceeding directly with coronary angiography in these patients without performing a stress test would have resulted in subjecting 30% of patients to expensive and invasive procedures, despite an expected good outcome without interventions, because of the presence of normal perfusion.
One interesting finding of this study is that one third of patients with angina had fixed perfusion abnormalities. These abnormalities predicted mortality as reversible abnormalities did. The reason for the presence of fixed, rather than reversible, abnormalities in patients with angina is not entirely clear. It is possible that some of these abnormalities represent a consequence of myocardial hibernation/stunning due to chronic/repetitive ischemia. We have recently shown that a significant number of patients without a history of CAD exhibit fixed perfusion abnormalities on stress sestamibi imaging. In that particular population, these abnormalities were associated with an incidence of hard cardiac events similar to that for reversible abnormalities (13). Another explanation would be the presence of minimal residual ischemia, in an infarct zone, that does not yield itself as a significant reversible perfusion defect. Previous studies have shown that the magnitude of ischemia is not related to the presence or absence of symptoms (14), and therefore, angina in some patients may be due to trivial ischemia in an infarct zone.
Impact of Extent of Perfusion Abnormalities
The scintigraphic extent of CAD was a powerful determinant of prognosis. Patients with a multivessel distribution of perfusion abnormalities had the highest event rate when the endpoints of all-cause mortality, as well as hard cardiac events, were considered. Revascularization should be considered for these patients. Patients with normal results on stress perfusion imaging had a low event rate up to 6 y after the test and therefore can be exempted from invasive studies during that period. Patients with a single-vessel distribution of abnormalities had a risk that was intermediate between the other groups. The decision to perform coronary angiography and subsequent revascularization in these patients should be individualized. These data indicate that the results of stress myocardial perfusion imaging in patients with angina can provide the physician with valuable information on the risk status of the patients and, therefore, assist in the decision on the next management strategy in patients with angina.
Previous Studies
To our knowledge, this was the first study to assess the long-term prognostic value of stress myocardial perfusion imaging in a well-defined group of patients with stable angina. Hachamovitch et al. studied 1,270 patients with a high pretest likelihood (>0.85) of CAD who underwent exercise or adenosine stress dual-isotope imaging (15). Most of the patients had angina. Follow-up was complete for 94%. During 2.2 ± 1.2 y of follow-up, 60 hard events occurred. Patients with normal perfusion had an annual hard-event rate of 1.3%. The addition of perfusion data in the Cox model resulted in incremental prognostic value over clinical data for predicting hard cardiac events. Independent predictors of mortality were not reported. Our study demonstrated that patients with normal perfusion had a low event rate, which was sustained over a longer mean follow-up period of 6 y. The number of deaths in our study was large enough to demonstrate an independent association of perfusion abnormalities with mortality.
Some studies have suggested an independent prognostic value for stress myocardial perfusion imaging after stabilization of patients with unstable angina (16–19). These studies have generally included a small number of patients with a shorter-term follow-up. An association of perfusion abnormalities with composite endpoint (but not mortality) was reported. Dakik et al. studied 136 patients who were hospitalized for unstable angina and subsequently underwent stress myocardial perfusion imaging before discharge (17). During a mean follow-up of 31 ± 17 mo, 20 patients (15%) sustained either cardiac death (n = 12) or nonfatal myocardial infarction (n = 8). The significant multivariate predictors of cardiac events were the total perfusion defect size, the presence of reversible perfusion defects, and the presence of multiple perfusion defects. Brown studied 52 patients admitted with the diagnosis of unstable angina within 1 wk of discharge after stabilization of symptoms by stress 201Tl imaging (18). Patients were followed up for 39 ± 11 mo. Cardiac events included cardiac death (n = 3), nonfatal myocardial infarction (n = 4), and admission for unstable angina or revascularization (n = 17). 201Tl redistribution was the only significant predictor of cardiac death or nonfatal myocardial infarction (P < 0.05). Studies of long-term outcome after a normal stress radionuclide study are scarce. Gibbons et al. determined the long-term risk of subsequent cardiovascular events in 4,649 patients with an intermediate-risk treadmill score who did not have myocardial perfusion defects on radionuclide imaging. Follow-up was 95% complete. Cardiovascular survival was 99.8% at 1 y, 99.0% at 5 y, and 98.5% at 7 y. Cardiac survival free of myocardial infarction was 96.6% at 7 y (20).
Impact of Type of Stress Test
We used dobutamine and not vasodilator stress in patients unable to exercise. Preferring vasodilator stress to dobutamine for myocardial perfusion imaging was based on earlier studies demonstrating better flow heterogeneity with dipyridamole than dobutamine (21). These studies used a small dose of dobutamine without addition of atropine and did not represent the state-of-art protocol for dobutamine stress. Recent studies have shown that the flow heterogeneity obtained by high-dose dobutamine–atropine stress is equal to that obtained by dipyridamole (22). Bin et al. demonstrated that in coronary arterial beds with a noncritical stenosis, the increases in myocardial blood flow and velocity and capillary derecruitment are similar for both dobutamine and adenosine (23). Therefore, there is no literature-supported evidence to suggest a superiority of vasodilator over dobutamine stress. In our study, mortality was higher in patients who underwent dobutamine stress testing. However, the type of stress test was not predictive of events when adjusted to other data, suggesting that the standard dobutamine stress has no inherent limitations in the assessment of myocardial perfusion.
It is generally believed that patients with normal results on stress myocardial perfusion imaging have a hard cardiac event rate of <1%. In developing radionuclide imaging guidelines, the American College of Cardiology, American Heart Association, and American Society for Nuclear Cardiology reviewed 14 studies published between 1994 and 2003 that included more than 100 patients who did not have recent myocardial infarction (5). Event rates (cardiac death or nonfatal myocardial infarction) associated with normal perfusion scan findings ranged from 0% to 1.3% per year, compared with 2%–14.3% per year in patients with abnormal scan findings. The mean follow-up in these studies was 27.6 mo. A hard cardiac event rate of 1.2% in our study can be explained by the longer-term follow-up, which tends to show relatively higher rates. The annual event rate in the first year in our study was 0.8% after normal perfusion imaging findings. The annual event rate in patients with a high pretest probability was previously reported at 1.3% in patients undergoing sestamibi dual-isotope imaging (15). Finally, our study included a large number of patients with known CAD. We have previously reported that among patients with normal exercise sestamibi findings, those with a history of CAD had a slightly higher event rate after 2 y of follow-up than those without a history of CAD (24). One limitation of this study is that gated SPECT data were not available and, therefore, the prognostic information obtained from left ventricular function and transient left ventricular dilation could not be assessed.
CONCLUSION
Stress 99mTc-tetrofosmin myocardial perfusion imaging is a valuable tool for the risk stratification of patients with stable angina pectoris. The extent of stress perfusion abnormalities is a powerful predictor of cardiac events. Patients with normal perfusion have low event rates up to 6 y after the test and therefore can be exempted from invasive procedures during that period. Patients with a multivessel distribution of abnormalities had the highest risk of cardiac events. These patients should represent the major group in which invasive procedures should be considered. Patients with a single-vessel distribution of perfusion abnormalities have an intermediate risk of death. The decision to proceed with invasive procedures in these patients should be individualized.
Acknowledgments
This study was supported in part by a publication grant from GE Healthcare. We thank Sean Duffy for his help in preparing the manuscript
Footnotes
Received Jul. 18, 2005; revision accepted Sep. 6, 2005.
For correspondence or reprints contact: Abdou Elhendy, MD, PhD, 982265 Nebraska Medical Center, Omaha, NE 68198-2265.
E-mail: Aelhendy{at}unmc.edu





{kind=link}
{kind=link}
{kind=link}
{kind=link}