


Abstract
Carvedilol is a β-blocking agent with antioxidant properties that has been shown to improve survival in chronic heart failure (CHF). Previous open-label studies have suggested that its use may have positive effects on the abnormalities of cardiac sympathetic innervation integrity and functioning. The present study aimed to test the hypothesis that carvedilol exerts its beneficial effects on hemodynamics in parallel with an action on myocardial sympathetic activity and with its antioxidant property. Methods: A randomized, multicenter, double-blind, placebo-controlled study of carvedilol was conducted on 64 CHF patients. Patients underwent—before and after 6 mo of therapy with either carvedilol or placebo—measurements of cardiac sympathetic activity, circulating catecholamine level, and hemodynamic indices. Myocardial meta-123I-iodobenzylguanidine (123I-MIBG) uptake was used to assess the changes in myocardial sympathetic activity. The antioxidant properties of the plasma were assessed by measuring the percentage of nonhemolyzed erythrocytes and the volume of plasma capable of inhibiting 50% of hemolysis after an oxidative stress. Echographic left ventricular (LV) diameters, radionuclide LV ejection fraction (LVEF), and exercise cardiopulmonary capacity were measured to evaluate the hemodynamic response. Results: End-diastolic and end-systolic LV diameters decreased (both P < 0.05) and LVEF increased (P = 0.03) in the carvedilol group, whereas these parameters remained unchanged in the placebo group. Carvedilol did not alter the submaximal exercise cardiopulmonary capacity or the circulating catecholamine level. The beneficial hemodynamic effects in the carvedilol group were associated with an increase in myocardial 123I-MIBG uptake as assessed by both planar and tomographic imaging (P < 0.01). Carvedilol had no detectable effect on antioxidant properties of the plasma. Conclusion: The benefits of carvedilol on resting hemodynamics appear to be associated with a partial recovery of cardiac adrenergic innervation functioning without detectable antioxidant effect in the plasma.
Adrenergic drive is increased in the failing human heart, leading to elevated local release of adrenergic neurotransmitters. It is likely that it is this local increase in cardiac adrenergic activity, rather than an increase in circulating norepinephrine (NE), which is both initially adaptative, by modulating contractility and heart rate, and, ultimately, deleterious to the failing heart, by leading to cardiac hypertrophy, β-adrenergic subsensitivity, myocardial ischemia, cardiac arrhythmias, tissue necrosis, myocyte apoptosis, and, subsequently, by leading to ventricular dysfunction. β-Blockers reduce the progression of left ventricular (LV) dysfunction and improve the prognosis of patients with chronic heart failure (CHF) (1–3).
Carvedilol is a third-generation β-blocker, which combines nonselective β-blockade, α-blockade, and antioxidant effects (4). This pharmacologic profile of carvedilol may offer a particular advantage in comparison with other β-blockers (5–7). Nevertheless, the exact effect of carvedilol on the sympathetic pathway remains putative. Meta-123I-iodobenzylguanidine (123I-MIBG) scintigraphy provides the opportunity to explore noninvasively the adrenergic neuronal function in vivo, since MIBG shares the same reuptake and storage mechanisms as NE. A striking decrease in MIBG uptake or retention has been found in the failing heart, and this finding has been related to the prognosis of the disease (8,9). Interestingly, pharmacologic interventions that led to an improvement in LV function in CHF induced a concomitant recovery in NE reuptake function (10). Some previous data (11–13) have suggested that the open-label therapy with carvedilol is associated with an improved cardiac adrenergic innervation functioning. To confirm this hypothesis, this study, SYMPOXYDEX (SYMPathetic and OXYDative stress KredEX study), was conducted as a multicentric, randomized, double-blind, placebo-controlled trial. The study aimed at comparing the effects of carvedilol and placebo on 2 primary endpoints: myocardial 123I-MIBG uptake and antioxidant status of the plasma and erythrocytes in patients with CHF.
MATERIALS AND METHODS
This study was designed and conducted as a multicentric, randomized, double-blind, placebo-controlled trial. Patients were included from 1997 to the beginning of 1999, at a period during which β-blocker treatment was not yet considered standard medical care in our country for heart failure patients. The protocol was approved by a regional ethics committee and all institutional boards. We also obtained approvals from the “Direction Générale de la Santé” and of the “Agence Française du Médicament” (French Ministery of Health). All patients gave their written consent.
Inclusion Criteria
Patients with CHF, in New York Heart Association (NYHA) class II–III, with an LV ejection fraction (LVEF) lower than 40% in the previous 2 mo, treated with diuretics and angiotensin-converting enzyme (ACE) inhibitors, and eventually digoxin, were eligible for the study.
Study Design
The following parameters were assessed at inclusion: physical status, NYHA functional class, electrocardiography, echocardiographic LV diameters, radionuclide LVEF, plasma catecholamine concentration, determination of antioxidant status of the plasma, and scintigraphic measurement of cardiac 123I-MIBG uptake.
The exclusion criteria were the following: stenotic valvulopathy, hypertrophic or restrictive cardiomyopathy, postpartum heart failure, symptomatic cardiac arrhythmias not controlled by treatment or by a cardiac defibrillator; unstable angina; recent (<3 mo) myocardial infarction; myocarditis; sinus node dysfunction; pacemaker implanted; second or third degree atrioventricular block; bradycardia <60 min−1; sitting systolic arterial pressure <90 mm Hg; treatment by carvedilol in the previous 2 mo. The following drugs had to be stopped at least 4 wk before inclusion: verapamil, diltiazem, group IA or IC antiarrhythmic agents, α- or β-blockers, monoamine oxidase inhibitors or tricyclic antidepressors (known to interfere with cardiac MIBG uptake); asthma or severe chronic obstructive pulmonary disease; diabetes mellitus; hepatic insufficiency (aspartate aminotransferase and alanine aminotransferase more than twice the normal values); severe renal insufficiency (plasma creatinine >250 mmol/L); pregnancy.
If the inclusion criteria were fulfilled, patients were randomized to receive either carvedilol or a placebo. The initial dose of carvedilol was 3.25 mg twice a day (BID), increased, if tolerated, to 6.5 mg BID, 12.5 mg BID, and 25 mg BID every 15 d. The target dose was 50 mg/d for patients with a weight of <85 kg and 100 mg for patients with a weight of >85 kg. Thus, the titration period lasted 8–10 wk with an initial administration done at the hospital. In case of bradycardia <50 min−1, symptomatic hypotension, or severe heart failure after the first dose, the patient was excluded from the study. Poor tolerance of the treatment during the 3.25-mg-BID or 6.5-mg-BID titration phase also led to exclusion of the patient. After that stage, occurrence of any adverse effect led to interruption of the titration process and the patient remained in the study, with the dose received at the previous visit.
The maintenance phase lasted 4 mo at the maximal tolerated dose. Patients had monthly clinical evaluations. Study drug dosage was maintained constant throughout the trial. Associated medications for heart failure could be modified during the study. The final evaluation was made 6 mo after having initiated the treatment, while the patient was still receiving the allocated study drug.
The primary endpoint was the effect of treatment on cardiac 123I-MIBG uptake and retention and on the antioxidant status of the plasma 6 mo after the beginning of therapy. The following secondary endpoints were analyzed: functional status, echographic indices of LV enlargement, radionuclide LVEF, and plasma catecholamine level. Analyses of the echographic and scintigraphic data were performed in core laboratories by physicians who were unaware of the therapeutic and the clinical status of the patients.
123I-MIBG Scintigraphy
After a 30-min resting period, patients were injected intravenously with 111–148 MBq of 123I-MIBG. Twenty minutes (early acquisition) and 4 h (late acquisition) after MIBG administration, a 10-min planar acquisition was performed in the anterior view of the chest. Cardiac 123I-MIBG uptake was measured as the heart (H)-to-mediastinum (M) activity ratio (H × 100/M, in %) on the image (8) by 2 independent observers. For each patient, the H/M ratio was taken as the average of measurements performed over his or her scintigraphic image by each observer. The interobserver variability was 2.3%, whereas the intraobserver variability was 1.8% (P = not significant [NS]). A H/M value of 195% ± 31% (range, 175%–260%) was found in 20 healthy subjects (age, 49 ± 14 y) in our laboratory. The washout rate of 123I-MIBG within the myocardium was measured as the percentage change in cardiac activity from early to delayed images within the LV regions of interest as follows: ([H early − H delayed]/H early) × 100, H values being corrected for 123I physical decay.
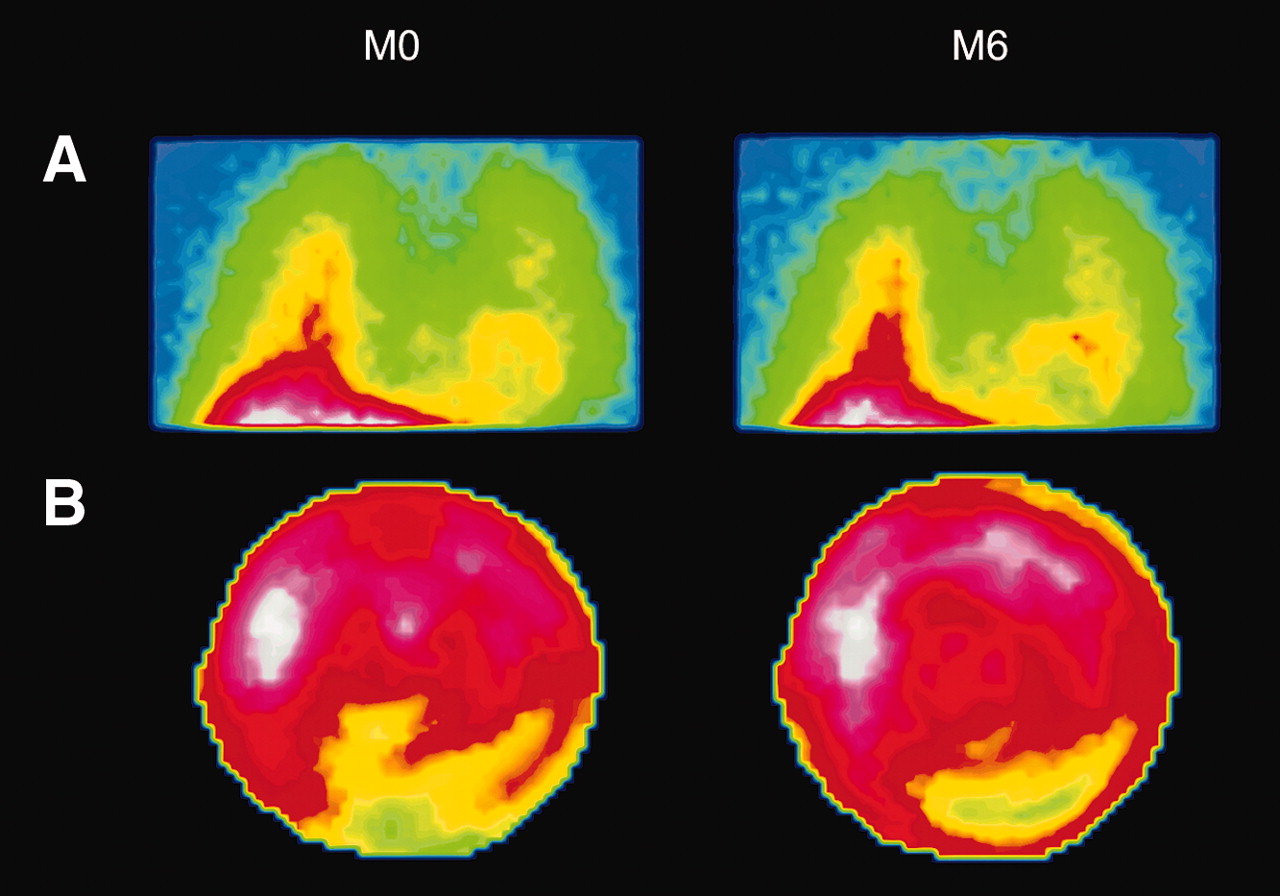
To evaluate the effect of therapy on the regional 123I-MIBG distribution, myocardial SPECT images were acquired after the delayed planar imaging acquisition, on a dual-head imaging system (Fig. 1). The tracer uptake on the myocardial SPECT images was analyzed visually using a 5-level scoring scale (0 = normal, 1 = mildly reduced, 2 = moderately reduced, 3 = severely reduced, 4 = no uptake), applied on 17 segments. The total severity score index (SSI) (9) was computed by summing the scores of individual segments. The tracer uptake on the myocardial SPECT images was analyzed semiquantitatively by measuring on a “bull’s eye” image both the extent (DE) of the defect (expressed as number of pixels of the defect/total number of pixels, in %) and the severity (DS) of the defect (expressed as mean counts/pixel in the defect over mean counts/pixel in the region with maximal uptake, in %).
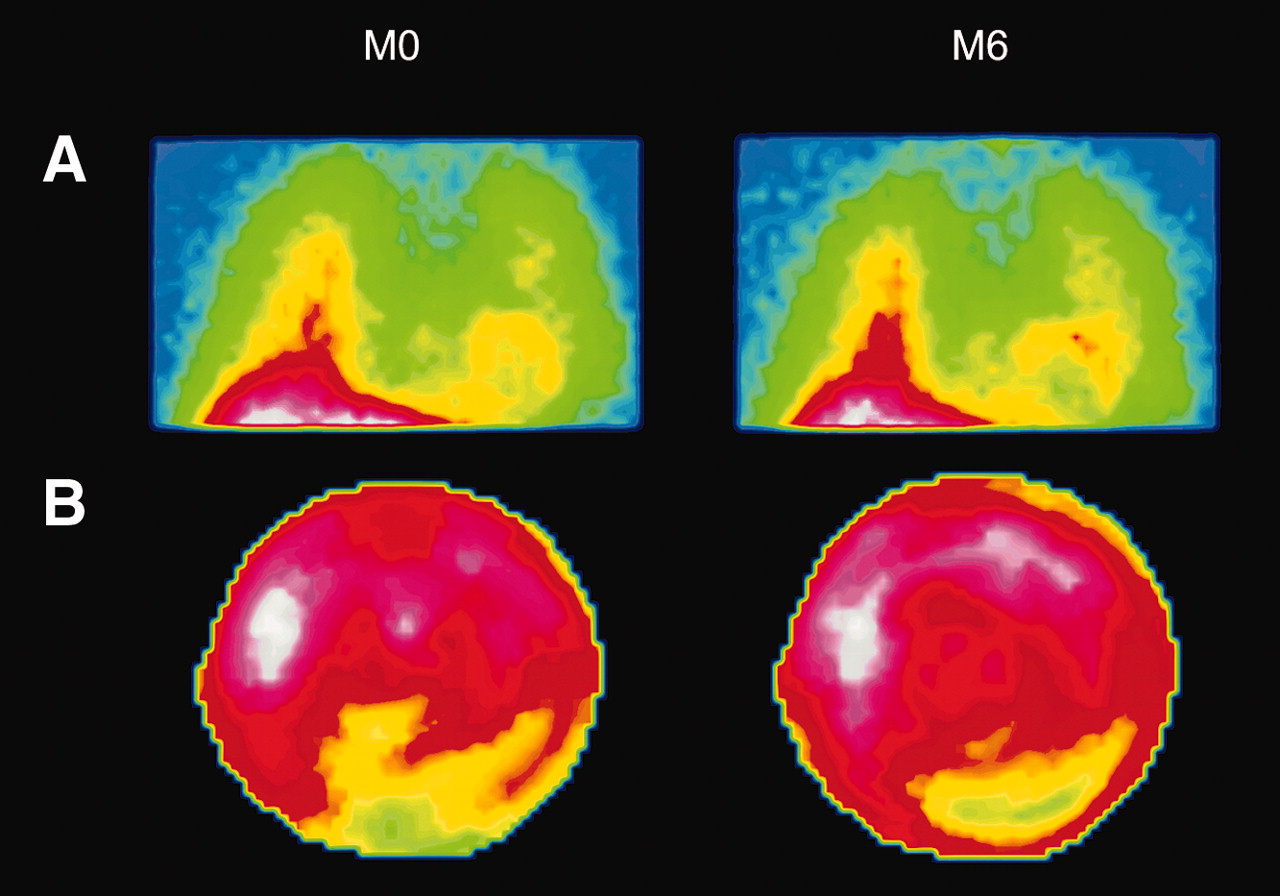
123I-MIBG planar imaging and SPECT obtained in patient with dilated cardiomyopathy randomized to the carvedilol group. (A) Clear increase in cardiac 123I-MIBG uptake is seen when comparing delayed 123I-MIBG image obtained before (M0) and after 6-mo β-blocking therapy (M6), especially in the anterolateral wall, whereas level of background activity seems comparable in these 2 images. (B) When comparing bull’s eye images of delayed 123I-MIBG SPECT before (M0) and after therapy (M6), a decrease in the extent of defect is observed in the inferolateral myocardial wall.
Plasma Antioxidant Status
Plasma and erythrocyte antioxidant status of the patients was determined simultaneously before and 6 mo after having initiated the therapy with either carvedilol or placebo. For this purpose, 5 mL of blood were drawn on ethylenediaminetetraacetic acid and put in ice at +4°C and then centrifuged 5 min at 100g at +4°C. The test had to be performed within 8 h after blood sampling. This test was based on the addition at 37°C of a fixed concentration of an oxygen free radical donor (2,2′-azobis(2-amidinopropane)dihydrochloride [AAPH]) into a suspension of patients’ erythrocytes, leading to membrane alteration and, ultimately, to hemolysis measured by the lactate dehydrogenase activity. This test permits evaluation of the ability of erythrocytes to resist the AAPH-induced oxidative stress defined by the percentage of hemolyzed erythrocytes (PHE, an arbitrary value of 100% being given for total hemolysis) and to determine by successive dilutions the volume of plasma capable of inhibiting 50% of AAPH-induced hemolysis (IPV50). In control subjects, this volume of plasma was 3.0 ± 0.1 μL. It was previously shown that the intraassay variation coefficients were 1.9% and 3.4% for PHE and IPV50, respectively, and the interassay variability was 4% for both tests (14).
Radionuclide LVEF
All patients had equilibrium radionuclide angiography after in vivo labeling of red blood cells using 740 MBq of 99mTc. A 500-kilocount acquisition was performed in the anterior and left anterior oblique views that best separated the right and left ventricles in the plane of the interventricular septum. The processing of the LVEF was performed from the left anterior oblique view using a standard commercially supplied semiautomated edge-detection program. The normal range of LVEF is 55%–70%.
Submaximal Cardiopulmonary Exercise Testing
All patients initially performed a maximal cardiopulmonary bicycle exercise test before randomization and peak oxygen consumption (peak Vo2) were determined. A submaximal constant work rate bicycle exercise test was done 3–5 d thereafter. However, there is no consensus on the methodology for a submaximal test in heart failure patients (15). We used 85% of the previously determined peak work rate as the constant work rate, progressively attained in 1 min. This level was supposed to be greater than the one at which the anaerobic threshold occurred. Exercise duration was the parameter measured. Patients exercised until exhaustion or a maximal preestablished time of 20 min.
Circulating Catecholamine Levels
Catecholamine (epinephrine and NE) plasma concentrations were assayed by liquid chromatography with electrochemical detection.
Data Analysis
Calculation of the number of subjects of the study was made as follows. According to previous data (8,9), assuming a mean value of 123I-MIBG H/M in the heart failure population of 135% and a variance of (0.17)2, with an expected absolute difference between carvedilol and placebo of 12%, the number of subjects required was 24 per group (α = 0.05 and β = 0.20 in an unilateral situation). Regarding the antioxidant variables, given that normal values in our laboratory for IPV50 were 3.35 ± 0.50 μL and 71.5% ± 3.8% for PHE and that decreases of these parameters by 29% and 18%, respectively, were observed after administration of vitamin E (500 mg/d for 15 d) in healthy volunteers (14), 18 subjects were required in each group (α = 0.05; β = 0.10 in unilateral analysis). Therefore, taking into account a 30% dropout rate, we planned to include 65 patients in the study. We used the intention to treat analysis, on patients receiving at least 2 mo of treatment. In this analysis, missing data at the final visit were replaced by the baseline values. A per-treatment analysis was also performed, which yielded similar results and, therefore, is not reported here.
Scintigraphic data (123I-MIBG and radionuclide LVEF) and echocardiographic data were analyzed in core laboratories by trained physicians who were unaware of the patients’ clinical and therapeutic status.
Variables were described by their mean, median, and SD (16) and quartiles. Statistics were done with the SAS program. A Student t test was used for continuous variables in the case of normality of the distribution and equality of the variances. Otherwise, a Wilcoxon nonparametric test was used. A χ2 test was used for categoric variables. A Hölm correction was made in the case of multiple comparisons of results for the same test. The statistical significance level was set at P < 0.05.
RESULTS
Except for plasma NE concentration, there was no significant difference in the clinical and the laboratory investigation results at the time of inclusion when comparing the placebo and carvedilol groups (Table 1).
Patient Characteristics at Time of Inclusion
Clinical Outcome
Sixty-four patients were selected. Seven of them were included but not randomized. Among the 54 randomized patients, 7 dropped out before the end of the study: 4 did not finish the titration process because of a serious adverse event; 2 were lost to follow-up, and 1 did not tolerate the treatment. Two of these 7 patients died. Eleven patients had a major deviation in the protocol (mainly poor compliance or administration of a drug prohibited by the protocol). Therefore, 43 patients entered the per-protocol analysis but the results are presented according to the intention-to-treat method (50 patients randomized and having entered the maintenance phase).
They were 42 men and 8 women with a mean age of 59 ± 10 y. The etiology of heart failure was an idiopathic dilated cardiomyopathy in 29 patients, an ischemic cardiomyopathy in 20 patients, and multiple causes of heart failure in the remaining patient. Thirty-nine patients were in NYHA class II and 11 were in class III. Ninety-six percent of the patients were in sinus rhythm. There was no significant difference between the 2 groups with regard to any of these variables. Sixty-four percent of the patients in the carvedilol group and 62% in the placebo group reached the target dose of the study drug. Seventeen patients reported a serious adverse effect during the study: 5 in the carvedilol group and 12 in the placebo group (P = 0.025). There was 1 sudden death in each group; 4 heart failure episodes occurred in the placebo group, but none occurred in the carvedilol group (P < 0.05). The other adverse events were cancer (n = 2), acute myocardial infarction (n = 1), atrial fibrillation (n = 2), atrial flutter (n = 1), orthostatic hypotension (n = 1), decompensated diabetes mellitus (n = 1), hemoptysis (n = 1), unilateral deafness (n = 1), arthritis (n = 1). No patient underwent a revascularization procedure during the 6-mo follow-up period.
Primary Endpoints
Cardiac 123I-MIBG Uptake.
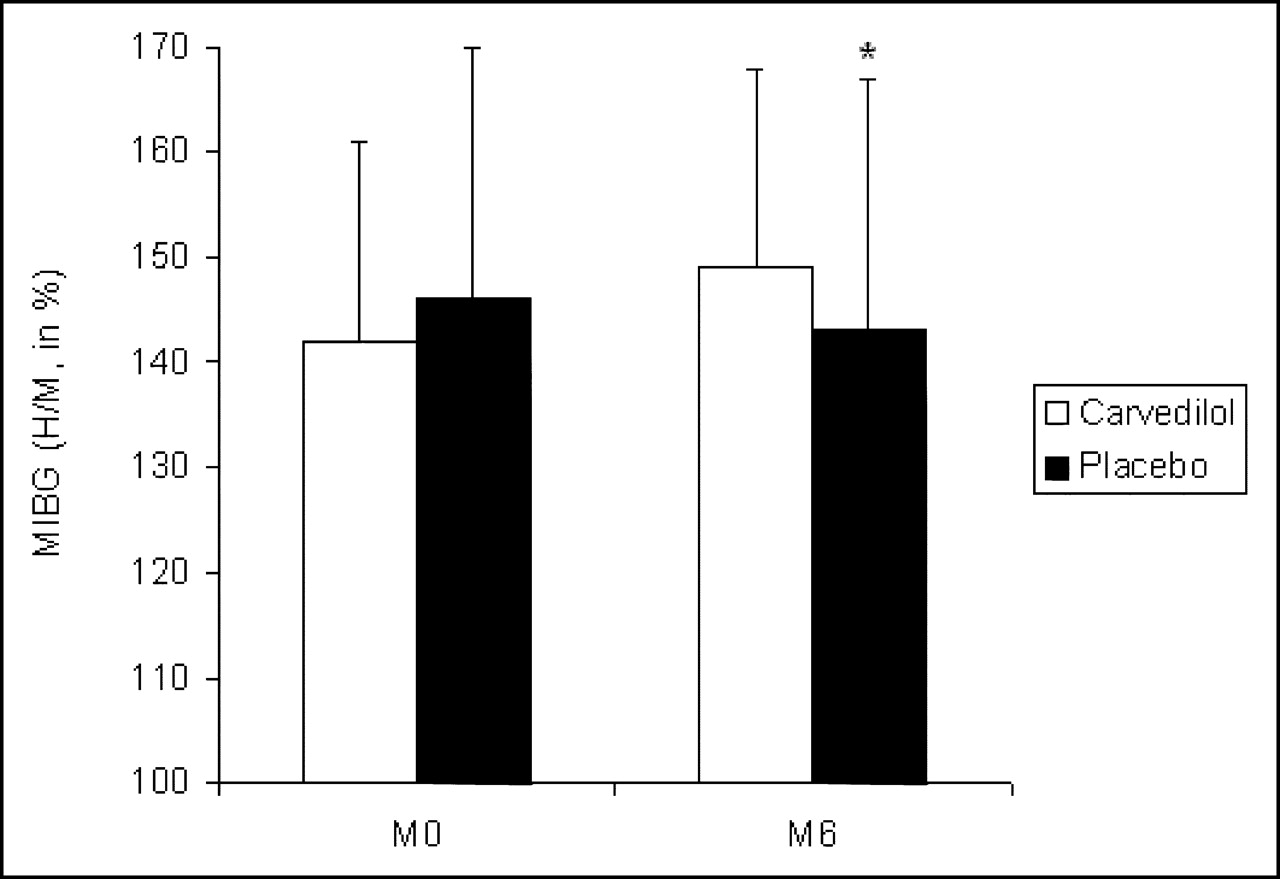
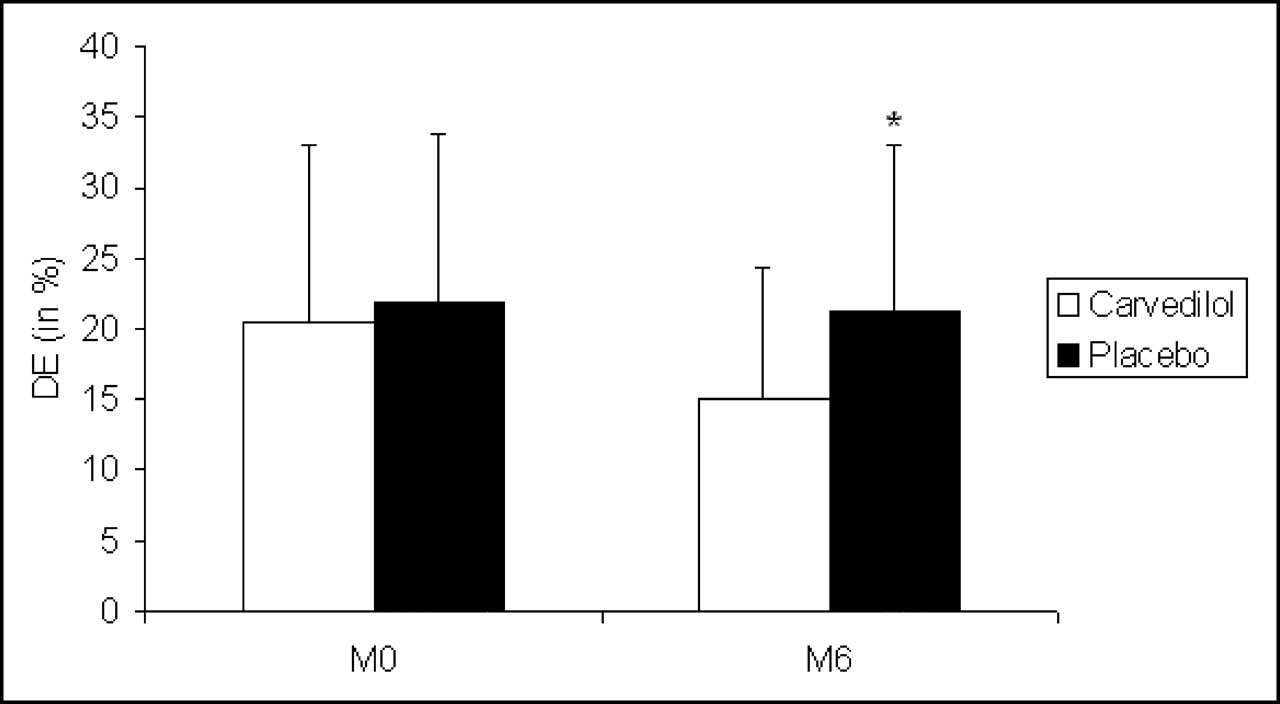
At the time of inclusion, 123I-MIBG H/M uptake 4 h after injection was 142% ± 18% and 146% ± 24% in the carvedilol group and the placebo group, respectively (P = NS). 123I-MIBG H/M uptake increased to 149% ± 21% in the carvedilol group, whereas it tended to decrease to 143% ± 24% in the placebo group (P = 0.003) (Fig. 2). A similar increase was seen in the ischemic and the nonischemic groups. The difference observed between the 2 study arms was significantly higher than the intra- and interobserver variability. When using the H/M ratio, 36% of the patients had improvement in their cardiac 123I-MIBG uptake in the placebo group, whereas 63% of the patients in the carvedilol group did so. Washout rates were 22% ± 14% and 23% ± 12%, respectively (P = NS). There was no difference with regard to the washout rate between the 2 groups at 6 mo. The index of regional 123I-MIBG uptake (SSI) was not significantly different in the carvedilol and the placebo groups at the initial examination (25.9 ± 17.9 and 23.6 ± 12.0, respectively; P = NS). The SSI tended to decrease to 21.6 ± 12.5 in the carvedilol group (P = 0.056), whereas no change was observed in the placebo group (SSI = 23.5 ± 12.4 at 6 mo; P = 0.9). The DE on the bull’s eye image decreased (Fig. 3) at 6 mo in the carvedilol group (20.4% ± 11.2% vs.15.0% ± 12.2%; P = 0.03), whereas no change was observed in the placebo group (21.8% ± 12.9% vs. 21.3% ± 10.6%; P = 0.8). The DS estimated on the bull’s eye image decreased at 6 mo in the carvedilol group (52.6% ± 5.6% vs. 55.9% ± 6.0%; P = 0.014), whereas no change was observed in the placebo group (52.7% ± 4.2% vs. 52.6% ± 7.6%; P = 0.9).
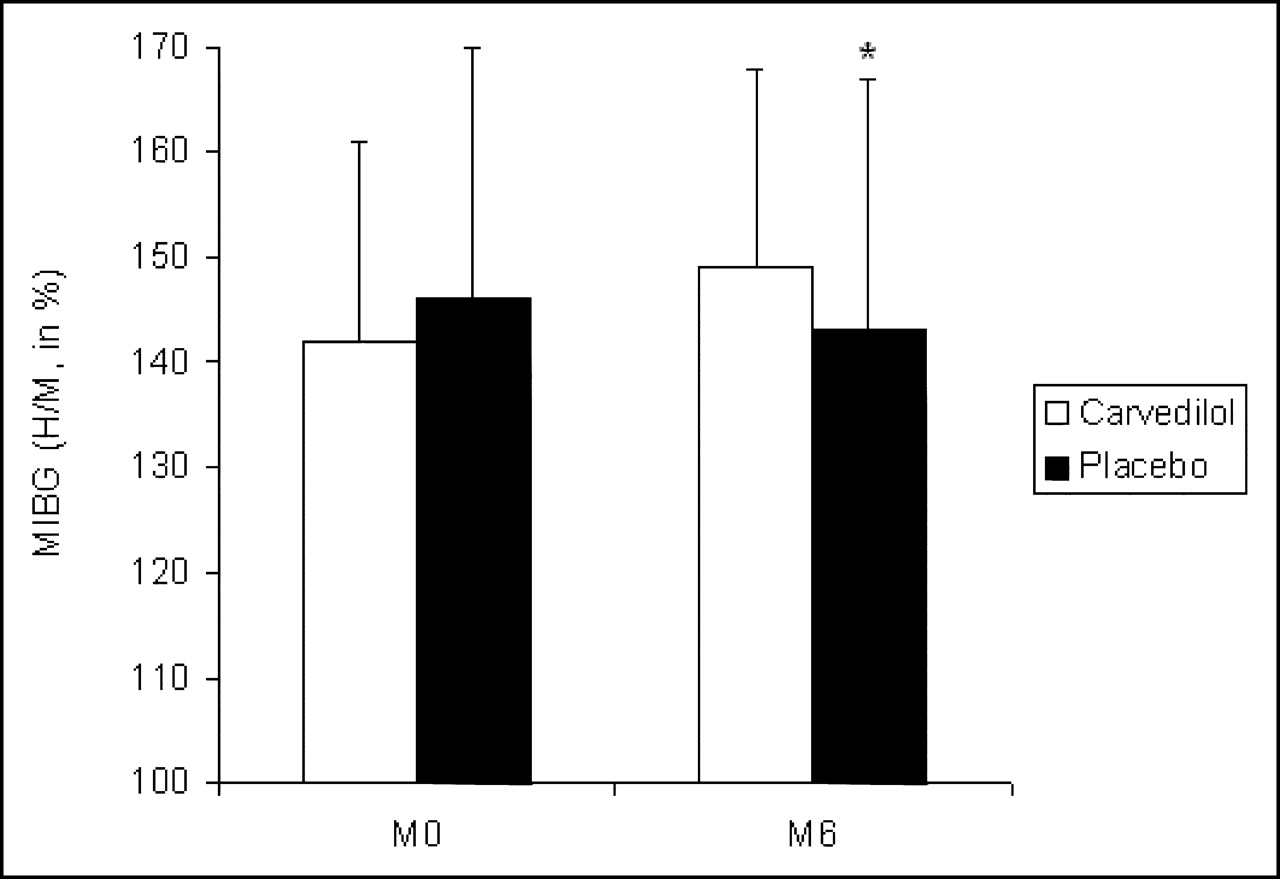
Therapeutic effect of carvedilol on late 123I-MIBG uptake. After 6-mo therapy, 123I-MIBG uptake, as assessed by late H/M ratio, increased from 142% ± 18% to 149% ± 21% in the carvedilol group, whereas it decreased from 146% ± 24% to 143% ± 24% in the placebo group. *P = 0.003.

Therapeutic effect of carvedilol on regional late SPECT 123I-MIBG imaging. After 6-mo therapy, DE on the bull’s eye image decreased from 20.4% ± 11.2% to 15.0% ± 12.2% (P = 0.03) in the carvedilol group, whereas it remained unaltered in the placebo group (from 21.8% ± 12.9% to 21.3% ± 10.6%; P = NS). *P = 0.004.
Plasma Antioxidant Status.
At initial examination, PHE was 64% ± 9% and 64% ± 6% in the carvedilol and the placebo groups, respectively (P = NS). IPV50 was 4.3 ± 1.5 μL and 4.2 ± 1.7 μL in the carvedilol and the placebo groups, respectively (P = NS). At the end of the study, PHE was 66% ± 8% in the carvedilol group and 64% ± 8% in the placebo group (P = NS). IPV50 also did not differ between the 2 groups at the end of the study (4.0 ± 1.6 μL in the carvedilol group and 4.2 ± 1.7 μL in the placebo group, respectively). The effect of carvedilol varied, however, when patients with a normal IPV50 at initial examination (i.e., ≤3.4 μL) were distinguished from those with an abnormal IPV50 (i.e., >3.4 μL). Carvedilol permitted maintaining a normal range value for patients with an initially normal IPV50 (P < 0.05), whereas this index became abnormal in the placebo group (P < 0.05). Conversely, carvedilol had no effect in the group of patients with an IPV50 of >3.4 μL.
Secondary Endpoints
Functional Status.
Carvedilol induced a beneficial effect with regard to the functional status reported by patients: Only 15% of the patients did not report any improvement in the carvedilol group compared with 67% in the placebo group (P = 0.003). Nevertheless, there was no difference with regard to the NYHA functional class as assessed by the physician. No change in systolic arterial pressure was found in both the carvedilol group (from 123 ± 16 to 131 ± 20 mm Hg; P = NS) and the placebo group (from 120 ± 20 to 128 ± 21 mm Hg; P = NS) during the follow-up period. No change in heart rate was found in both the carvedilol group (from 76 ± 11 to 75 ± 9 beats/min; P = NS) and the placebo group (from 82 ± 13 to 78 ± 14 beats/min; P = NS) during the follow-up period.
Radionuclide LVEF.
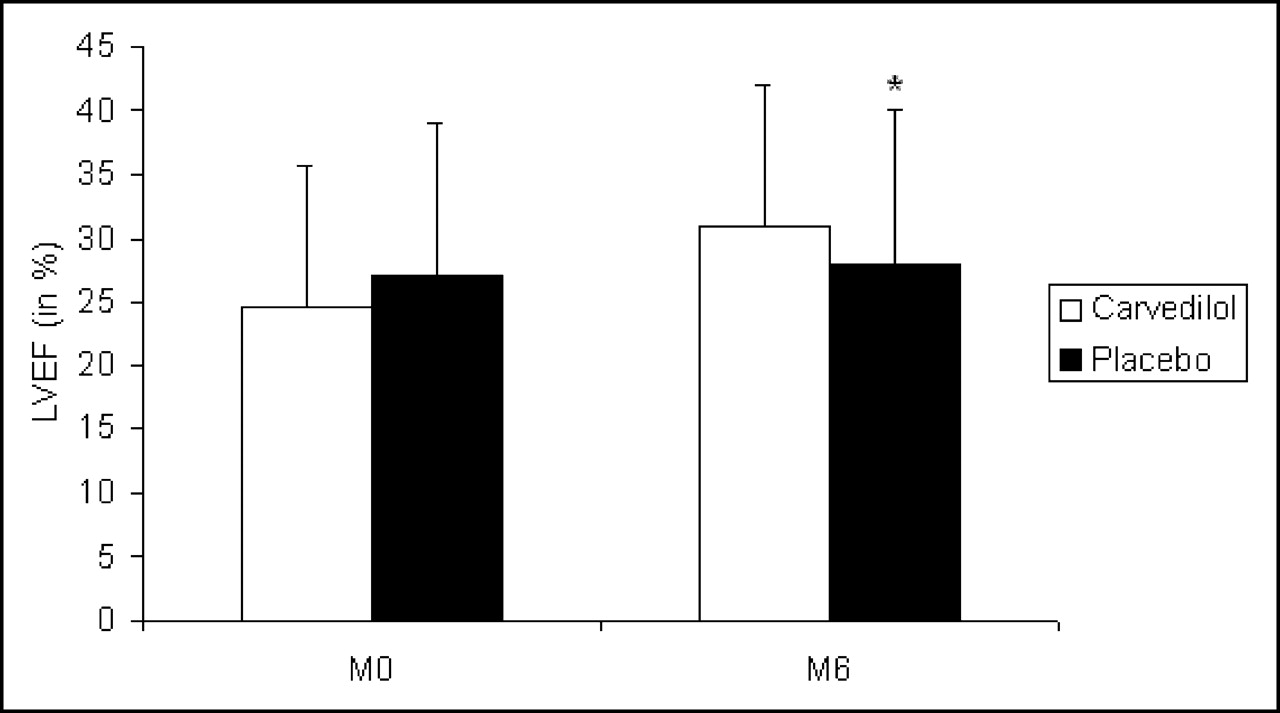
Patients treated with carvedilol showed a significant improvement in radionuclide LVEF when compared with those treated with placebo (Table 2; Fig. 4).
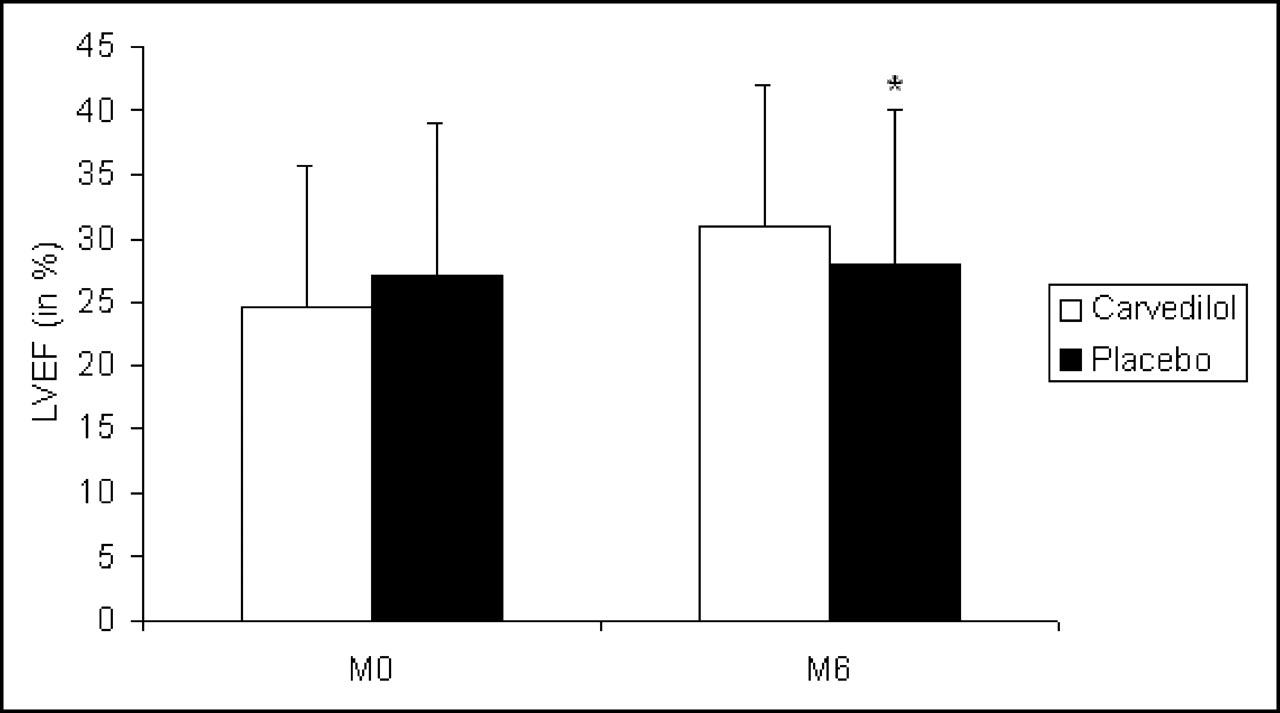
Therapeutic effect of carvedilol on LVEF. After 6-mo therapy, LVEF increased from 25% ± 11% to 31% ± 12% in the carvedilol group, whereas it remained unaltered in the placebo group (from 27% ± 12% to 28% ± 12%, respectively; P = NS). *P = 0.03.
Therapeutic Effects on Primary and Secondary Endpoints
Echocardiographic Indices of Ventricular Enlargement.
End-diastolic and end-systolic LV diameters decreased in the carvedilol group (both P < 0.05), whereas they remained unchanged in the placebo group.
Cardiopulmonary Exercise Testing.
There was no change in submaximal exercise test duration in both therapeutic groups when comparing the initial values with those obtained after the 6-mo follow-up period (from 552 ± 373 s to 532 ± 324 s, respectively, in the carvedilol group; from 631 ± 327 s to 679 ± 362 s, respectively, in the placebo group; P = NS).
Plasma Catecholamine Level.
There was no significant difference with regard to the changes of any of the catecholamine levels within the 2 therapeutic groups during the follow-up period.
DISCUSSION
The present study shows that, in CHF patients, the beneficial effects of carvedilol on resting hemodynamics are associated with improvement of cardiac adrenergic innervation functioning.
In the normal heart, adrenergic drive is low at rest. Conversely, in heart failure, adrenergic hyperactivity occurs and plays a critical role in the evolution of the disease. As heart failure progresses, circulating NE levels are increased in relation to the degree of LV dysfunction and to the risk of death (17). Even though the plasma levels of NE are elevated in response to heart failure, myocardial NE reuptake and inotropic responsiveness to catecholamines are abnormal and have been found to be inversely correlated with duration of life (8).
This is attributed to the fact that catecholamines, and specifically NE, exert cytotoxic actions on both myocytes and the myocardial adrenergic pathway. Myocardial hemorrhage, necrosis, and heart failure have been shown to occur in animals after high doses of catecholamines (18), with these effects being a result of an imbalance between oxygen supply and demand. However, at concentration levels such as those achieved in heart failure, NE does not produce prominent myocardial necrosis but induces progressive cardiac muscle damage (19). This phenomenon has been related to apoptosis in cultured rat cardiomyocytes (20) via the formation of reactive oxygen species (16). Evidence that the sympathetic nerve endings are damaged by NE-derived free radicals has been provided by measurements of increased hydroxyl free radical generation by nonenzymatic autooxidation of NE in the heart after NE administration (21) and after cardiac sympathetic nerve stimulation (22). Some reports in animal models have demonstrated that chronic infusion of NE at doses achieving myocardial interstitial NE levels comparable to those observed in heart failure produces β-adrenoceptor downregulation and desensitization, and reduction of noradrenergic nerve terminal profiles due to uptake-1 carrier site downregulation, associated with an increase in oxidative stress as demonstrated by increased tissue oxidized glutathione and a decreased ratio of reduced to oxidized glutathione (23).
Because neuronal reuptake of NE is the major mechanism for terminating action of NE on the myocardial β-receptors, its impairment can further accentuate myocyte hyperstimulation to the neurotransmitter (24). The subsequent amplification of postsynaptic changes—especially, β-1 adrenergic receptor downregulation, β-2 adrenergic receptor uncoupling, and intracellular calcium overload—contributes to the worsening of cardiac function and to the rise of neurohormonal activation.
Myocardial fixation of 123I-MIBG depends on the integrity of the sympathetic innervation. The reduction in myocardial 123I-MIBG uptake in heart failure can be due to a downregulation of the uptake-1 carrier protein induced by an overexposure to the neurotransmitter at the synaptic level. In a prior experimental study, we found that a chronic intravenous infusion of NE in the rat induced a decrease in myocardial 123I-MIBG uptake that paralleled a downregulation of uptake-1 carrier protein density (25).
The deleterious role of the adrenergic hyperactivity in CHF has been indirectly confirmed by data from numerous clinical trials that have demonstrated multiple benefits of β-blocker therapy (1–3). Similarly, in the present study, carvedilol markedly increased LVEF (by 25%) and reduced LV volumes, in accordance with prior data that demonstrated a favorable effect of β-blockers on LV remodeling (26,27).
To our knowledge, the present study is the first double-blind, multicenter, placebo-controlled study to assess the effect of carvedilol by 123I-MIBG imaging in heart failure patients. It shows that, 6 mo after having initiated a therapy with carvedilol, an improvement in NE reuptake function occurs in parallel with the improvement of cardiac function. The finding that carvedilol exerts cardioprotective properties on myocardial adrenergic innervation is in accordance with previous data. An increase in either global (H/M) or regional (SPECT) 123I-MIBG uptake was reported in either ischemic or nonischemic heart failure after open-label therapy with metoprolol (28,29), carvedilol (11–13), and other agents improving LV function (30,31). In a placebo-controlled study, a 6-mo therapy with metoprolol led to both an improvement in NE uptake function and a decrease in LV diameter, but no significant effect on systolic function was found (10).
The antioxidant effect may be a potential mechanism of the better hemodynamic response observed with carvedilol than that found with other β-blockers. Indeed, congestive heart failure is associated with an increased oxidative stress that may alter cardiac function in part by its toxic effect on NE, and subsequent interventions with antioxidant effects have shown beneficial effects. Carvedilol, but not metoprolol, partially prevented oxygen radical–induced contractile dysfunction in isolated human cardiomyocytes (32). Lipid peroxides and 8-iso-prostaglandin F2a, which are the major biochemical products of reactive oxygen species generation, are elevated in plasma and pericardial fluid of patients with heart failure (33,34). Recently, direct evidence of elevated oxidative stress in the myocardium of patients with heart failure was provided by immunohistochemical assays of endomyocardial biopsy samples for the expression of 4-hydroxy-2-nonenal–modified protein, which is a major lipid peroxidation product (35). Moreover, in the same study, the open-label administration of carvedilol resulted in a decrease in the oxidative stress level together with amelioration of cardiac function (35). In the present study, the antioxidant status in CHF patients was evaluated using a global method (14). The lack of a detectable antioxidant effect in the whole group treated with carvedilol could be due to the fact that the responses of plasma and erythrocytes do not necessarily reflect the antioxidant defenses of specific tissues such as the heart. However, in the subgroup of patients with normal oxidative status at baseline, carvedilol prevented the increase in oxidative stress observed with time in the placebo group (P < 0.05). This may suggest that the antioxidant effect of carvedilol is dependent on the baseline oxidative status and is not observed when oxidative stress is already elevated, which requires further confirmation.
The present findings may have some clinical implications. It is likely that in patients with heart failure attributed to dilated cardiomyopathy, but untreated by β-blockers, MIBG imaging and radionuclide LVEF are challenged in assessing the prognosis by the measurement of exercise capacity (9). Nevertheless, the value of exercise capacity measurements to monitor the therapeutic response of β-blockers appears limited. In the present study as well as in other controlled studies (36–38), although patients reported an improvement in functional status, carvedilol did not exhibit any significant effect on submaximal exercise capacity assessed by treadmill exercise. This observation may be due to the use of an exercise protocol that is not sensitive enough to detect a change in exercise capacity (39). Recent studies, however, have confirmed that this limited impact of β-blockers on exercise tolerance has led to a decrease in the predictive prognostic value of peak exercise Vo2 in patients receiving β-blockers (15,40), suggesting the need for reassessing the comparative prognostic values of 123I-MIBG imaging and exercise testing in patients treated with β-blockers (9).
CONCLUSION
This study shows that carvedilol improves the function of adrenergic innervation as assessed by 123I-MIBG scintigraphy in parallel with the hemodynamic improvement as assessed by radionuclide LVEF.
Acknowledgments
This study was supported by grants from Carveteam and Produits Roche groups. We thank Bernard Caviezel, Amin Kadi, Angela Moryussef, and Laurent Joubert for their help in designing the protocol; and Cecile Jourdan and François Montestruc (Produits Roche) for their help in performing the statistical analysis of the data.
The SYMPOXYDEX Study included Main Investigators: Alain Cohen-Solal (Hopital Beaujon, Clichy) and Alain Berdeaux (Pharmacology Department, Hopital Bicetre, Le Kremlin Bicêtre); Investigators: Damien Logeart (Hopital Beaujon, Clichy); Eric Pussard, Serge Witchitz, Christine Richer-Giudicelli, and Jean François Giudicelli (Faculté de Médecine du Kremlin-Bicêtre); Marie Claude Aumont and Philippe Duc (Hôpital Bichat, Paris); Richard Isnard and Kristina Chafirovskaia (Hopital de la Pitié-Salpêtrière, Paris); Patrice Colin, Michel Slama, Sylvie Dinanian, and Yvan Carel (Hôpital Antoine Béclère, Clamart); Florence Beauvais, Guillaume Jondeau, and Olivier Dubourg (Hôpital Ambroise Paré, Boulogne); and Core Laboratories: Nuclear Medicine (Pascal Merlet, Centre Hospitalier Frederic Joliot, Orsay; Dominique Le Guludec and Nicolas Delahaye, Service de Médecine nucléaire, Hopital Bichat, Paris); Echocardiography: Eric Abergel (Hopital Europeen Georges Pompidou, Paris).
Footnotes
Received Mar. 11, 2005; revision accepted Aug. 1, 2005.
For correspondence or reprints contact: Pascal Merlet, MD, PhD, Service de Médecine Nucléaire, Centre Hospitalo-Universitaire Bichat et EA 3512, 46 rue Henri Huchard, 75877 Paris Cedex 18, France.
E-mail: pascal.merlet{at}bch.ap-hop-paris.fr
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nuclear Cardiology Surrogate Biomarkers in Clinical Trials
- Nuclear Imaging of the Cardiac Sympathetic Nervous System: A Disease-Specific Interpretation in Heart Failure
- {beta}-Adrenoceptor Blockers Increase Cardiac Sympathetic Innervation by Inhibiting Autoreceptor Suppression of Axon Growth
- Decreased Myocardial {beta}-Adrenergic Receptor Density in Relation to Increased Sympathetic Tone in Patients with Nonischemic Cardiomyopathy