


Abstract
Cardiac sympathetic function plays an important role in the regulation of left ventricular (LV) function and the pathophysiology of LV dysfunction. 11C-CGP-12177 (11C-CGP) has been used to assess myocardial β-adrenergic receptor (β-AR) density in vivo using PET. The aim of this study is to measure myocardial β-AR density in patients with nonischemic cardiomyopathy and to compare the measurements with various standard parameters of heart failure (HF), particularly with presynaptic function assessed by 123I- metaiodobenzylguanidine (123I-MIBG) imaging. Methods: 11C-CGP PET was performed on 16 patients with nonischemic cardiomyopathy and 8 age-matched healthy volunteers using a double injection method. A 11C-CGP dynamic scan for 75 min was performed after the injection of 11C-CGP with a high specific activity. After 30 min, 11C-CGP with a low specific activity was injected. The β-AR density of the whole LV was calculated on the basis of the graphical analysis method. Additionally, β-AR density was compared with LV ejection fraction (LVEF), sympathetic presynaptic function assessed using 123I-MIBG kinetics, and neurohormonal parameters. Results: The β-AR density of patients was significantly lower than that of healthy volunteers (3.80 ± 0.96 vs. 7.70 ± 1.92 pmol/mL; P < 0.0001). In the patients, β-AR density correlated significantly with LVEF (r = 0.62, P < 0.05). Furthermore, β-AR density correlated significantly with the 123I-MIBG washout rate (r = −0.68, P < 0.01) and delayed heart-to-mediastinum ratio (H/M ratio) (r = 0.61, P < 0.05). On the other hand, the correlation between β-AR density and early H/M ratio was not significant (r = 0.40, P = 0.13). The β-AR density of patients with severe HF (New York Heart Association functional [NYHA] class III) was significantly lower than that of those with NYHA functional class I or class II HF (3.24 ± 0.96 vs. 4.24 ± 0.73 pmol/mL; P < 0.05). Conclusion: A reduction in β-AR density measured by 11C-CGP PET was observed in patients with nonischemic cardiomyopathy. This downregulation may be due to the increased presynaptic sympathetic tone as assessed by 123I-MIBG imaging.
Heart failure (HF) is a major cause of mortality and represents a growing health problem, despite major therapeutic advances (1–3). The severity of HF is evaluated primarily by symptoms, clinical findings, hemodynamic measurements, left ventricular ejection fraction (LVEF), or exercise tolerance (4–7). In addition, the assessment of neurohormonal system disorders related to HF has proven to be valuable for risk stratification (8–11). Despite these indices, the accurate evaluation of the risk of mortality remains difficult.
Cardiac sympathetic function plays an important role in the regulation of heart function and has been studied extensively in recent decades (12,13). In a failing heart, the myocardial responsiveness to β-agonist stimulation is suppressed, primarily because of the downregulation of β1-adrenergic receptor (AR) (14,15). This β-AR downregulation has been induced by an enhanced sympathetic activity to the heart and an enhanced release of endogenous cardiac-derived catecholamines (16). The degree of downregulation is related to the severity of HF (15). Furthermore, these patients have higher levels of circulating catecholamines, which are inversely related to prognosis (8). On the basis of these findings, a beneficial effect of β-adrenergic blocker therapy has been hypothesized. In fact, many trials have shown the beneficial effect of β-blocker therapy in heart failure patients (3).
However, this in vitro measurement is invasive and does not allow longitudinal and regional assessment in humans. PET is an excellent noninvasive tool for investigating the distribution of myocardial β-AR in vivo and provides the possibility of repeated measurements. Studies using PET and the radioligand 11C-CGP-12177 (11C-CGP) have shown promising results that are in agreement with those of in vitro studies (17). CGP appears to be the most suitable ligand because it is very potent and is a hydrophilic nonselective β-AR antagonist with low nonspecific binding on membranes and slight cellular uptake (18). CGP enables the investigation of plasma membrane receptors. However, CGP has not been studied extensively in vivo because of difficulty in the synthesis of 11C-CGP. We developed a method for producing 11C-CGP with very high yield and specific activity, which provides high-quality images and the clinical application for myocardial β-AR density (19,20).
Merlet et al. demonstrated the downregulation of β-AR in patients with HF caused by idiopathic dilated cardiomyopathy (17). We hypothesized that this downregulation may be related to the adrenergic presynaptic dysfunction. However, there is little information about the relationship between presynaptic function and β-AR density in HF. The aim of this study was to measure myocardial β-AR density in patients with nonischemic left ventricular (LV) dysfunction using 11C-CGP PET and to compare the measured values with various standard parameters of HF and presynaptic function. Adrenergic presynaptic function was assessed by 123I-metaiodobenzylguanidine (123I-MIBG) imaging. 123I-MIBG, a norepinephrine (NE) analog, is accumulated in sympathetic nerve endings through the uptake-1 mechanism and can be used to delineate cardiac sympathetic nerve distribution and function (21–23).
MATERIALS AND METHODS
Study Patients
In this study, we enrolled 16 patients diagnosed as having nonischemic cardiomyopathy (8 men, 8 women; mean age ± SD, 62.8 ± 11.1 y). All patients had LV dysfunction (LVEF < 45%) but showed normal coronary angiography. All patients underwent 11C-CGP PET and 123I-MIBG imaging within 1 mo (mean time, 15 d) during the stable stage of HF. No clinical events or changes in medication occurred during these 2 studies. Because treatment with a β-blocker is known to affect myocardial β-AR density, patients with a history of β-blocker treatment were excluded from the study.
Control Subjects
Eight age-matched healthy volunteers (6 men, 2 women; mean age ± SD, 57.6 ± 13.0 y; P = not significant vs. patients) served as control subjects for the measurements of β-AR density. They showed no sign of cardiac disease and each had a normal resting electrocardiogram. This study was approved by the Ethics Committee of Hokkaido University Hospital. All subjects gave their written informed consent for the study.
PET Data Acquisition
All PET scans were obtained using an ECAT EXACT HR+ (Siemens Medical Solutions, Inc.). A transmission scan was performed to correct photon attenuation for 8 min with a 68Ge source. 11C-CGP was prepared as reported previously (21,22). The measurement of myocardial β-AR density using 11C-CGP PET was performed according to a modified double-injection protocol reported previously (24,25). During a 75-min dynamic emission scan, the first dose of 11C-CGP with a high specific activity (169 ± 65 MBq, 0.19 ± 0.13 μg) was infused intravenously over a 2-min period. Thirty minutes later, the second dose of 11C-CGP with a low specific activity (312 ± 145 MBq, 22.0 ± 1.8 μg) was again infused over a 2-min period. A 54-frame dynamic emission scan was used for measurement of the sequential distributions of the tracer in vivo. During the 30-min period after the start of the first infusion, 24 time frames (8 × 15-s, 4 × 30-s, 2 × 60-s, 2 × 120-s, and 8 × 150-s frames) were acquired. After the second infusion, the scan was completed with 30 frames (8 × 15-s, 4 × 30-s, 2 × 60-s, 2 × 120-s, and 14 × 150-s frames).
PET Data Analysis
All emission sinograms were reconstructed with filtered backprojection using a Hann filter (cutoff frequency, 0.3 cycle/pixel). The in-plane resolution was 4.5-mm full width at half maximum in the images reconstructed into a 128 × 128 matrix. All data were corrected for dead time, decay, and measured photon attenuation. A whole-heart region of interest (ROI) was set manually in each transaxial view. Myocardial time–activity curves in the ROIs were corrected for radioactive decay and for vascular activity using the regional values of blood volume. The sections of the curve corresponding to the 2 slow clearance phases, which represent the dissociation of 11C-CGP bound to β-AR, were extrapolated back to the start of the infusions. β-AR density was then determined as the maximum number of available specific 11C-CGP−binding sites per gram of tissue (Bmax) in the ROIs using a modified equation described by Delforge et al. (24,25).
123I-MIBG Data Acquisition and Analysis
123I-MIBG (111 MBq) (Dai-ichi Radioisotope Laboratories, LTD.) was injected intravenously into the patients under resting and fasting conditions. Fifteen minutes and 4 h after the injection, static planar images were acquired in the anterior view using a dual-head γ-camera (ADAC Vertex Plus; Phillips) equipped with low-energy, general-purpose collimators. Static images on 512 × 512 matrices were collected for 5 min with a 20% window centered at 159 keV. Subsequently, SPECT of the heart was performed in 64 × 64 matrices using a filtered backprojection method for reconstruction. A ramp filter and a Butterworth filter with an order of 5.0 and a cutoff frequency of 0.50 cycle per pixel were used for reconstruction. No attenuation or scatter correction was performed. LV uptake was assessed by quantitative analysis performed manually drawing the ROI over the LV in the anterior view. The rectangular ROIs of 9 × 9 pixels were placed over the upper mediastinum. Counts per pixel were calculated from each ROI located in the heart and the mediastinum. The heart-to-mediastinum count ratios (H/M ratios) of early and delayed planar images were computed to quantify the cardiac uptake of 123I-MIBG. The washout rate (WR) was calculated using the following formula: where H = mean counts per pixel in the LV.
where H = mean counts per pixel in the LV.
Echocardiography
Echocardiography was performed in all patients at about the same time as 11C-CGP PET. LVEF was measured from apical 2-chamber and 4-chamber images using the biplane disk-summation method based on the standards of the American Society of Echocardiography (26).
Measurement of Neurohormonal Parameters
Before the PET study was started, venous blood samples were drawn after a 20-min resting period in the supine position. Plasma NE levels were measured using high-performance liquid chromatography. Plasma brain natriuretic peptide (BNP) levels were measured by chemiluminescent enzyme immunoassay.
Statistical Analysis
All data were expressed as mean ± SD. Regression analysis was performed using a linear regression method. A Student t test was performed to test differences between patients and control subjects. A P value < 0.05 was considered statistically significant. In addition, multivariate stepwise regression analyses were performed to investigate whether the β-AR density was associated independently with LVEF or NYHA class or whether it was dependent on presynaptic changes of plasma neurohumoral levels.
RESULTS
11C-CGP was produced with a very high yield (1,964 ± 1,105 MBq) and specific activity (485 ± 370 GBq/μmol). The characteristics of the patients are shown in Table 1. Four patients were classified as New York Heart Association (NYHA) functional class I, 5 patients as class II, and 7 patients as class III at the time of the PET scan. Although the BNP levels of the patients were significantly higher than those of the control subjects (183 ± 143 vs. 26 ± 24 pg/mL; P < 0.05), there was no significant difference in the NE levels between the 2 groups (367 ± 235 vs. 249 ± 116 pg/mL; P = 0.20).
Clinical Characteristics of 16 Patients
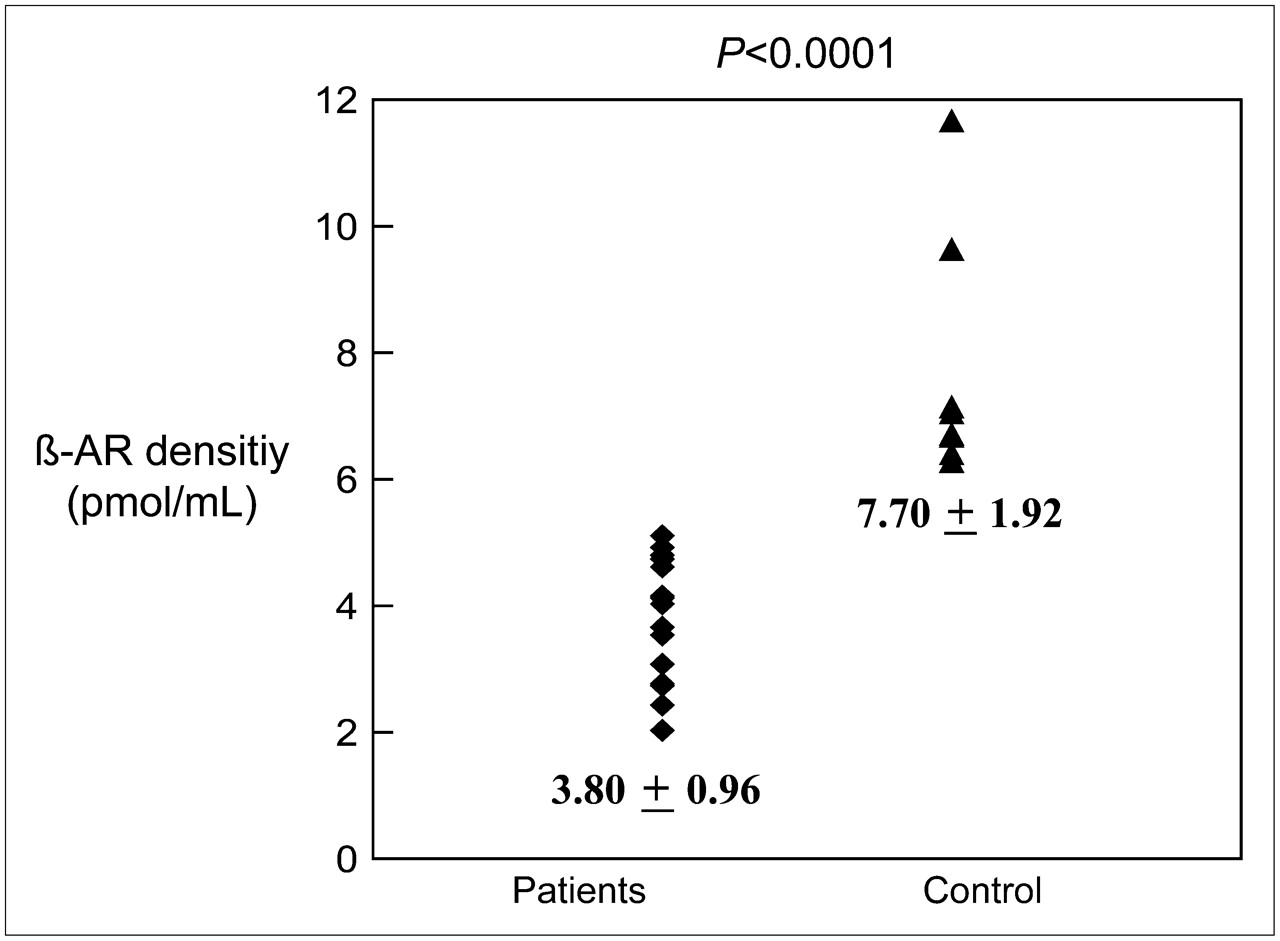
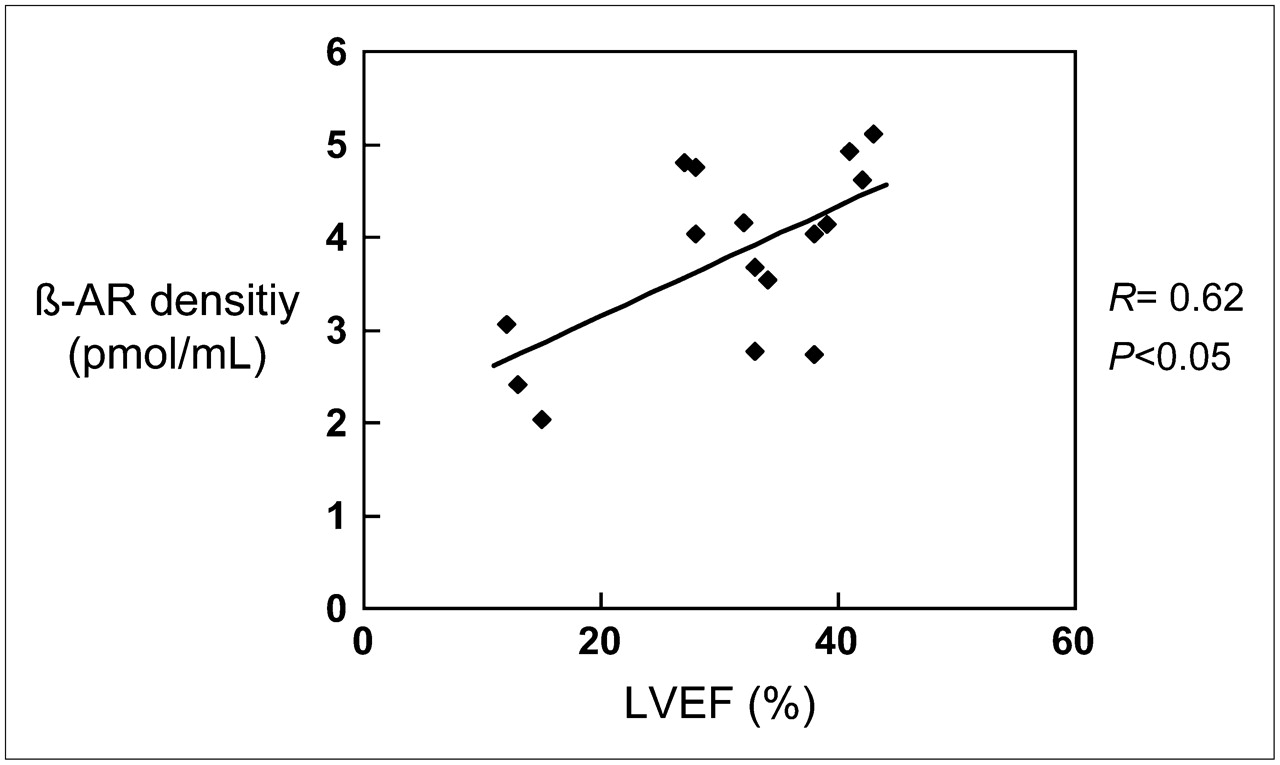
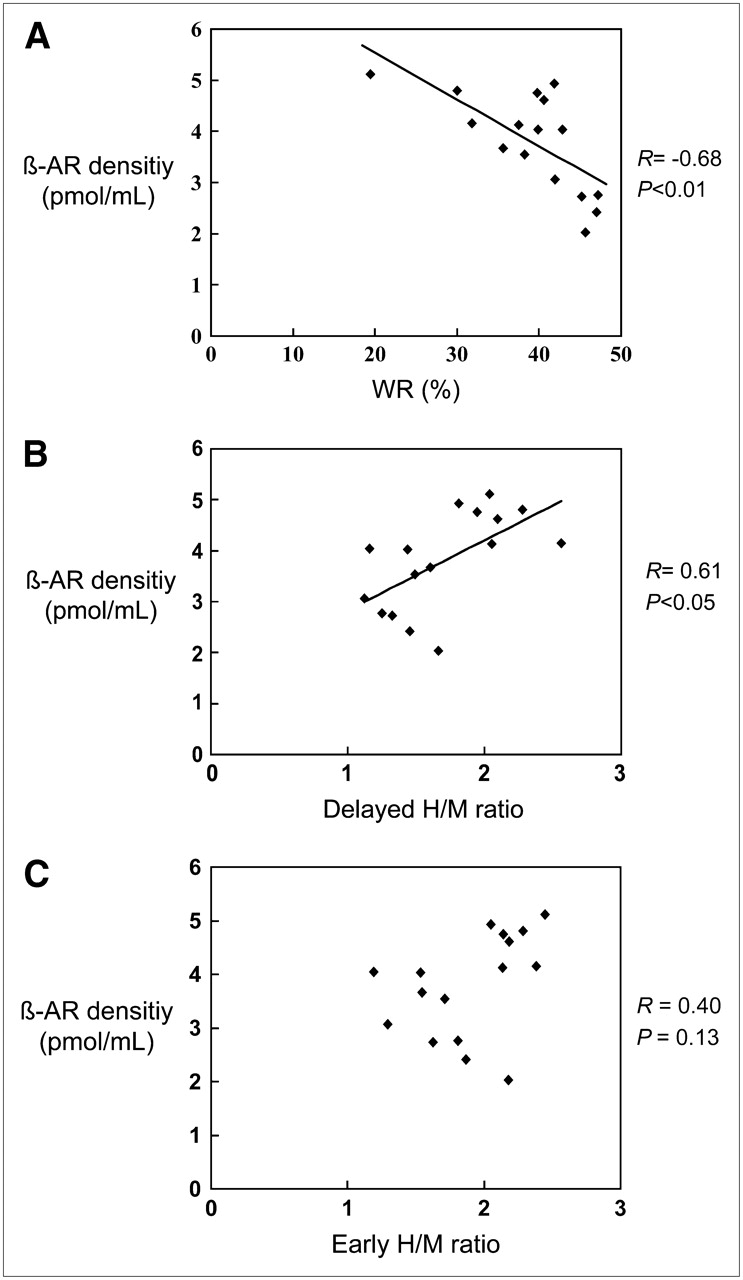
The calculated β-AR densities are shown in Figure 1. The β-AR density of the patients was significantly reduced by 51% in comparison with that of the control subjects (3.80 ± 0.96 vs. 7.70 ± 1.92 pmol/mL; P < 0.0001). In the patients, β-AR density correlated significantly with LVEF (r = 0.62, P < 0.05; Fig. 2). Furthermore, β-AR density showed good correlations with 123I-MIBG WR (r = −0.68, P < 0.01; Fig. 3A) and delayed H/M ratio (r = 0.61, P < 0.05; Fig. 3B). The correlation between β-AR density and early H/M ratio was not significant (r = 0.40, P = 0.13; Fig. 3C). β-AR density showed no correlation with BNP levels (r = −0.26, P = 0.33) or NE levels (r = −0.44, P = 0.09).

Comparison of β-AR density between patients with HF and control subjects.

Relationship between LVEF and β-AR density.

(A) Relationship between 123I-MIBG WR and β-AR density. (B) Relationship between delayed 123I-MIBG H/M ratio and β-AR density. (C) Relationship between early 123I-MIBG H/M ratio and β-AR density.
β-AR density of the patients with severe HF (NYHA class III) was significantly lower than that of those with mild HF (NYHA class I or II) (3.24 ± 0.96 vs. 4.24 ± 0.73 pmol/mL, P < 0.05; Table 2). There were no significant differences in early H/M ratios (1.76 ± 0.41 vs. 2.01 ± 0.35; P = 0.22) and delayed H/M ratios (1.49 ± 0.40 vs. 1.88 ± 0.38; P = 0.07), WR (41.4% ± 6.1% vs. 37.2% ± 7.7%; P = 0.26), and BNP levels (201 ± 129 vs. 169 ± 159 pg/mL; P = 0.66) between these 2 groups. The LVEF (24.6% ± 11.0% vs. 36.0% ± 5.9%; P < 0.05) and NE levels (584 ± 188 vs. 198 ± 60 pg/mL; P < 0.0001) of the severe HF group were significantly lower than those of the mild HF group (Table 2).
NYHA Classification and Parameters of HF
β-AR density significantly correlated with NYHA class (r = −0.61, P < 0.05), LVEF, 123I-MIBG WR, and delayed H/M ratio. In multivariate analysis, delayed H/M ratio was excluded, because there was a significant correlation between 123I-MIBG WR and delayed H/M ratio (r = −0.62, P < 0.05). 123I-MIBG WR (r = −0.70) and NYHA class (r = −0.50) were the determinants of myocardial β-AR density by multivariate stepwise analysis. By multivariate stepwise analysis, β-AR density was the only significant determinant of LVEF (r = 0.58) among β-AR density, 123I-MIBG WR, BNP level, and NE level. In contrast, NE level was the only determinant of NYHA class (r = 0.73).
DISCUSSION
This study showed that the myocardial β-AR density of the patients with nonischemic cardiomyopathy was significantly reduced by 51% in comparison with that of the age-matched control subjects. Myocardial β-AR density showed good correlations with LVEF, 123I-MIBG WR, and delayed H/M ratio but not with plasma BNP level or NE level.
β-AR density was reduced with decreasing LVEF. Severe HF patients showed a greater reduction in β-AR density than mild HF patients, indicating that a decrease in β-AR density reflects the severity of HF. On the other hand, β-AR density showed no correlation with plasma BNP level or NE level. These neurohormonal levels may change rapidly depending on the condition of HF. Because this study was performed at the stable stage of HF, these neurohormonal levels might have already returned to near-normal levels. In contrast, it is not clear whether β-AR density may change so rapidly. Therefore, such chronological differences might possibly cause little or no significant correlation between β-AR density and these neurohormonal parameters.
Bristow et al. showed a reduction in β-AR density in a failing human heart using an in vitro ligand-binding technique (14). They reported 50%–56% reductions in β-AR density. In 1993 Merlet et al. reported in vivo measurements of β-AR density using PET and 11C-CGP (17). They showed downregulation of β-AR by 53% with correlation with LVEF in the patients with idiopathic dilated cardiomyopathy. Our current results are in agreement with these previous reports.
Increased presynaptic activity in the failing human heart (8,16) and a decrease of postsynaptic β-AR density in failing heart (14,15,17) have been reported. In our study, the degree of β-AR downregulation corresponded to the increase in 123I-MIBG WR and a decrease in delayed H/M ratio. Because MIBG is a NE analog, WR and delayed H/M ratio may directly reflect NE release from the nerve terminal and its reuptake into the nerve terminal (uptake-1). In addition, the 123I-MIBG WR may reflect presynaptic sympathetic tone. The local NE concentration in the synaptic cleft increases when WR increases or delayed H/M ratio decreases (21–23). Our results may confirm the hypothesis that the increase in NE concentration in the synaptic cleft contributes to myocardial β-AR downregulation (27–29). Furthermore, the present study confirms pathophysiologic conditions of failing heart, which have been proven clinically over decades.
On the other hand, the correlation between β-AR density and early H/M ratio was not significant. It has been reported that an early MIBG uptake reflects only the integrity of presynaptic nerve terminals and their uptake-1 function, whereas a delayed MIBG uptake represents overall information with regard to neural function at the nerve terminal (30).
Schafers et al. reported β-AR downregulation and an impaired uptake-1 mechanism in patients with hypertrophic cardiomyopathy using 11C-CGP and 11C-hydroxyephedrin (11C-HED) PET (28). In their study, all patients had preserved LV systolic function and no evidence of HF. To our knowledge, there is no information with regard to the relationship between presynaptic and postsynaptic functions in HF in vivo. Our results show a precise correlation between β-AR density estimated by 11C-CGP PET and presynaptic function determined by 123I-MIBG imaging in HF patients.
123I-MIBG imaging has been widely used for the assessment of cardiac sympathetic function in HF (22,23,31–34). In many studies, it has been reported that impaired cardiac adrenergic innervation as assessed by 123I-MIBG imaging was closely associated with mortality in patients with HF (35–37). Some studies demonstrated that 123I-MIBG imaging was a good predictor of response to adrenergic β-blocker therapy (38,39). Spyrou et al. reported that β-AR downregulation can be used as a predictor of LV remodeling in patients after acute myocardial infarction (40). Further studies may be needed to evaluate the relationship between β-AR density, prognosis, and response to therapy in a larger patient population.
As a first limitation of this study, we used different methods for assessment of presynaptic and postsynaptic function. 11C-HED enables quantitative assessment of presynaptic function using PET. Because presynaptic function was assessed using 123I-MIBG imaging instead of 11C-HED, an accurate quantification of presynaptic function might be limited. The resolution of 123I-MIBG imaging is inferior to PET. Attenuation and scatter correction were not performed in this study. Myocardial 123I-MIBG imaging was analyzed semiquantitatively by using the H/M ratio on early and delayed planar images and the myocardial WR. However, we do not believe that attenuation and scatter may affect these parameters, because these parameters were relative values calculated from the counts in the anterior planar images. On the other hand, MIBG has advantages for estimating the integrity of presynaptic nerve terminals, their uptake-1 function, and sympathetic tone. Although we applied commonly used parameters from MIBG imaging, a better quantitative measurement may be needed for further analysis.
Because the number of patients in this study was small (n = 16) and the follow-up time was limited, cardiac events were not observed in the patients. Thus, we did not evaluate the prognostic value of β-AR density in this study. However, because this parameter was correlated with LVEF, NYHA, and MIBG parameters, β-AR may have the potential for risk stratification in patients with HF. Further study is warranted to confirm the prognostic value.
CONCLUSION
Decreased cardiac β-AR density measured by 11C-CGP PET was observed in patients with nonischemic cardiomyopathy. In addition, β-AR density correlated with 123I-MIBG WR and delayed H/M ratio. This downregulation may be due to an accelerated presynaptic sympathetic tone.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 30, 2007.
- Accepted for publication August 18, 2007.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Radiotracers to Address Unmet Clinical Needs in Cardiovascular Imaging, Part 1: Technical Considerations and Perfusion and Neuronal Imaging
- Assessment of cardiac sympathetic activity by MIBG imaging in patients with heart failure: a clinical appraisal
- Myocardial {beta}-Adrenergic Receptor Density Assessed by 11C-CGP12177 PET Predicts Improvement of Cardiac Function After Carvedilol Treatment in Patients with Idiopathic Dilated Cardiomyopathy