


Abstract
Radiolabeled chemotactic peptides have been studied for their applicability to the visualization of infectious and inflammatory foci. Because a radiolabeled leukotriene B4 (LTB4) antagonist allowed visualization of intramuscular E. coli abscesses in rabbits within a few hours after injection, we decided to test the imaging characteristics of this agent in a more clinically relevant model of pulmonary aspergillosis. The pharmacokinetics and imaging characteristics of the 111In-labeled LTB4 antagonist DPC11870 were studied in New Zealand White rabbits with experimental pulmonary aspergillosis infection. The imaging characteristics of 111In-DPC11870 were compared with those of 67Ga-citrate, a radiopharmaceutical commonly used to detect pulmonary infections in patients. Methods: Pulmonary aspergillosis was induced in the left lung of rabbits by intratracheal inoculation of 1 × 108 conidia of Aspergillus fumigatus. Three days after the inoculation, the rabbits received 111In-DPC11870 or 67Ga-citrate intravenously. Images were acquired at several time points up to 24 h after injection. Results: Pulmonary aspergillosis was visualized with both agents. Images acquired after injection of 111In-DPC11870 showed uptake in the pulmonary lesions from 6 h after injection. Because of accumulation at the site of infection and clearance from the background, the images improved with time. Region-of-interest analysis at 24 h after injection revealed infected lung–to–normal lung ratios of 5.0 ± 1.5 for 111In-DPC11870 and 2.9 ± 0.6 for 67Ga-citrate. Conclusion: The radiolabeled LTB4 antagonist DPC11870 clearly delineated experimentally induced pulmonary aspergillosis in rabbits. Images acquired at 24 h after injection of 111In-DPC11870 were superior to those obtained after injection of 67Ga-citrate.
Invasive pulmonary aspergillosis (IPA) is a common fungal infection that may affect morbidity and mortality in immunocompromised patients (1). Detection of aspergillosis infection at an early stage is of great importance because of the resulting improvement in the therapeutic outcome of patients (2). For the diagnosis of IPA, high-resolution chest CT is most often performed. Besides CT, other diagnostic methods, such as fungal culturing and non–culture-based methods such as serodiagnosis or polymerase chain reaction, may be applied (3). Scintigraphic imaging techniques may have an additional value in the diagnosis of IPA. They are based on physiologic changes, in contrast to radiologic techniques, which are based on morphologic alterations. 67Ga-Citrate is a radiopharmaceutical commonly used to visualize pulmonary and mediastinal infection, especially for immunocompromised patients in whom low white blood cell (WBC) counts hamper the use of radiolabeled leukocytes (3). Several other radiolabeled agents have been studied for applicability to the imaging of infection and inflammation. In particular, radiolabeled chemotactic peptides are promising imaging agents because of their favorable pharmacokinetic characteristics (4,5). In this study, we investigated the ability of the 111In-labeled leukotriene B4 (LTB4) antagonist DPC11870 to image experimentally induced aspergillosis in New Zealand White (NZW) rabbits.
LTB4 receptors (BLT1 and BLT2) are expressed mainly on leukocytes (6). In vitro binding of LTB4 to the BLT receptors results in intracellular signal transduction and subsequent chemotaxis (7). LTB4 expression and receptor targeting play an important role in the response of the immune system against infection and inflammation. Furthermore, overproduction of LTB4 contributes to inflammatory diseases, and LTB4 antagonists have been developed to exploit their antiinflammatory effect (8). LTB4 targets LTB4 receptors expressed on neutrophilic granulocytes that migrate toward and infiltrate the inflammatory and infectious lesion (9). This mechanism of receptor targeting may also be applicable to the visualization of inflammatory and infectious processes by using radiolabeled LTB4 antagonists. In this study, a bivalent LTB4 antagonist was labeled with 111In, and its ability to allow visualization of pulmonary aspergillosis in NZW rabbits was compared with that of 67Ga-citrate.
MATERIALS AND METHODS
DPC11870
Synthesis of the compound was based on the polyethylene glycol–tethered LTB4 antagonist SG385 described in a previous report (10). Boc-cysteic acid and Boc-Glu(OTfp)-OTfp were prepared as previously described (11,12). All other reagents were purchased from Aldrich Chemical Corp. or Fluka Chemical Corp.
The tetra-cysteic acid derivative of SG385 was prepared by the sequential coupling of Boc-cysteic acid in dimethylformamide using benzotriazol-tetramethyluronium-hexafluorophosphate coupling reagent. Boc was removed by treatment with 50:50 trifluoroacetic acid:methylene chloride. Purifications were performed after the addition of the first cysteic acid (partitioning between CHCl3 and water) and after the addition of the second and fourth cysteic acids (high-performance liquid chromatography [HPLC] on C18 silica using 0.1% trifluoroacetic acid–modified acetonitrile/water mobile phases). Products were recovered from HPLC mobile phases by lyophilization. The tetra-cysteic acid derivative 11870 was checked with HPLC and high-resolution mass spectrometry. In addition, the dimerization was achieved by reaction of 11870 with the bis-trifluoropropanone ester of Boc-glutamic acid and hydroxyazabenzotriazole (HOAt) in dimethylformamide. The crude reaction product was treated with trifluoroacetic acid/methylene chloride/triethylsilane to remove the Boc protecting group. The product was purified with C18 HPLC in a 0.1 mol/L ammonium acetate–modified acetonitrile/water mobile phase. Conjugation with diethylenetriaminepentaacetic acid was accomplished by reaction with diethylenetriaminepentaacetic acid anhydride in dimethylformamide. Purification gave DPC11870 in 73% yield from intermediate DPC11870. HPLC analysis of the lyophilized product gave a single peak. Additional quality control was performed with 1H nuclear magnetic resonance, and performance of high-resolution mass spectrometry showed an (M + 2H) value of 1563.5056 for this C123H182N26O53S8 structure.
Radiolabeling of DPC11870
DPC11870 was labeled with 111InCl3 in metal-free 0.25 mol/L ammonium acetate buffer, pH 5.5, for 30 min at room temperature. Radiochemical purity was checked by instant thin-layer chromatography (Rf of 111In-DPC11870, 0–0.5; Rf of unbound 111In, 1.0) and by reversed-phase HPLC on a C18 column (Zorbax Rx-C18, 4.6 mm × 25 cm; Agilent Technologies) as described previously (13).
67Ga-Citrate
67Ga-Citrate was commercially obtained (DRN 3103; Tyco Healthcare). The activity concentration was 37 MBq/mL at calibration time.
Aspergillus fumigatus
A. fumigatus, used for the induction of the infection, was isolated from an immunocompromised patient diagnosed with an A. fumigatus infection. The inoculum was prepared from a frozen isolate that was subcultured 2 times onto Sabouraud dextrose agar slants, followed by an incubation period of 5 d at 30°C. Conidia were harvested with phosphate-buffered saline (Invitrogen BV; Gibco) containing 0.20% Tween 20 (Sigma-Chemical Co.). Conidia were washed 3 times in Hanks’ balanced salt solution without calcium and magnesium (BioWhittaker Europe) and transferred to a 50-mL conical tube and counted in a hemocytometer. The concentration was adjusted to give each rabbit a predetermined inoculum of 1 × 108 conidia of A. fumigatus in a volume of 250 μL.
Induction of Pulmonary Aspergillosis
Fourteen female NZW rabbits weighing 2.3–2.8 kg were used during the experiments. Animals were housed individually and fed standard laboratory chow and water ad libitum. All animal experiments were approved by the local animal welfare committee in accordance with the Dutch legislation and performed in accordance with their guidelines.
Twelve rabbits received cytarabine (cytosine arabinoside) injections to bring about immunosuppression, using a modification of a method to induce neutropenia in rabbits (14). Cytarabine injections were given on 4 consecutive days to lower the WBC counts and allow the aspergillosis infection to become established. The other 2 animals remained healthy and served as control animals (for comparison with the pharmacokinetics of 111In-DPC11870 in cytarabine-treated animals) (Table 1). Aspergillosis was induced essentially as described by Groll et al., with a few modifications for our application (14). Cytarabine (Onco-Tain; Faulding Pharmaceuticals nv) was administered intravenously (525 mg/m2) on days −4 through −1 before the injection of radiolabeled compound. On day −3, after the second dose of cytarabine, A. fumigatus conidia were inoculated in 10 animals. Two animals injected with cytarabine were not inoculated and served as a second control group. Before inoculation, the animals were sedated with a subcutaneous injection of 0.7 mL of Hypnorm (fentanyl, 0.315 mg/mL, plus fluanisone, 10 mg/mL; Janssen Pharmaceutical). During inoculation, the rabbits received inhalation anesthesia with a mixture of isoflurane, nitrous oxide, and oxygen and were placed on the operation table. The inoculum of 1 × 108 conidia (250 μL) was given intratracheally into the left lung, together with 50 μL of 5% Evans blue dye (E2129; Sigma-Aldrich) via a syringe attached to a polyethylene 0.76 × 1.22 mm catheter (PE tube; Maxxim Medical).
Schematic Overview of Animal Experiments
Imaging and Biodistribution
At day 0 (3 d after inoculation of A. fumigatus), 9 rabbits (2 healthy, 2 injected with cytarabine only, and 5 both injected with cytarabine and infected with A. fumigatus) received an injection of 11 MBq of 111In-DPC11870 (3 μg) via the ear vein. The other 5 animals pretreated with cytarabine and infected with A. fumigatus received 11 MBq of 67Ga-citrate intravenously. Images (300,000 counts per image) were acquired immediately after injection of the radiolabeled preparations and at 2, 4, 6, and 24 h after injection. For scintigraphic imaging, the rabbits were immobilized in a mold and placed prone on the medium-energy parallel-hole collimator of the γ-camera in the anterior position (Orbiter; Siemens). Images were stored digitally in a 256 × 256 matrix. All images were windowed identically, allowing a fair comparison of the images acquired during the various experiments. The scintigraphic results were analyzed using regions of interest (ROI) drawn over the abscess and the contralateral noninfected lung (normal). Ratios of infected lung to normal lung (infected-to-normal ratios) were calculated. At 24 h after injection, all rabbits were euthanized with a lethal dose of sodium pentobarbital and organs were dissected. A blood sample was taken by cardiac puncture and tissues were weighed and the amount of radioactivity measured to determine the biodistribution of both agents. The activity in tissues was measured in a shielded well-type γ-counter (Wizard; Pharmacia-LKB) together with the injection standards. Radioactivity concentration was expressed as percentage injected dose per gram (%ID/g).
Hematologic and Histopathologic Studies
Blood samples were collected from all rabbits, both at day −4 before the first cytarabine injection and at day 0 (time of injection of the radiolabel), to determine the WBC count of the animals.
During dissection of the animals, samples of the infected (left) and noninfected lung were aseptically removed. One part of each lung sample was cultured for A. fumigatus for 24 h at 37°C on Sabouraud dextrose agar plates. A second specimen of lung tissue was fixed in phosphate-buffered formalin. After measurement of radioactivity, these tissues were embedded in paraffin. Tissue sections were stained with hematoxylin–eosin or Grocott methenamine silver and histopathologically examined.
Statistical Analysis
All values are presented as mean ± SD. Statistical analysis was performed using the 2-sided Student t test. The level of significance was set at 0.05.
RESULTS
Radiolabeling of DPC11870
Quality control tests by reversed-phase HPLC analysis and instant thin-layer chromatography indicated that the radiochemical purity exceeded 99%. The specific activity was 3.7 MBq of DPC11870 per microgram (12 MBq/nmol).
A. fumigatus
Culturing of the conidia solution confirmed that the inoculum consisted of A. fumigatus conidia. Animals infected with A. fumigatus began to show clinical symptoms 2 d after conidia inoculation. Respiration was more frequent and shallower in infected animals than in control animals. Intake of water and food was normal.
Hematologic and Histopathologic Studies
The mean WBC concentration of the rabbits at the time of the first cytarabine injection (day −4) was 13.5 ± 5.7 × 109/L. Four days after cytarabine administration, the WBC concentration of these rabbits was significantly reduced (5.2 ± 2.4 × 109/L, P = 0.0036). Normal WBC counts in NZW rabbits vary between 5.0 and 11.0 × 109/L (15). The WBC counts after induction of aspergillosis and injection of cytarabine indicated that the rabbits were not persistently neutropenic, but the numbers were much lower than on the first day of the experiment (day 0).
At dissection, all animals inoculated with A. fumigatus showed macroscopic infectious lesions in the lungs. In all but 1 rabbit, the infected area of lung corresponded to the area marked with Evans blue. In 1 rabbit (injected with 111In-DPC11870), the infection had affected both lungs. Culture of A. fumigatus was positive in 3 of 5 animals injected with 67Ga-citrate. In 3 of the 5 cases in which animals were injected with 111In-DPC11870 and inoculated with A. fumigatus conidia, positive cultures were found (1 of these animals showed positive cultures in both lungs). One animal was positive only for staphylococcus species. Both lungs from the 4 control rabbits and the remainder lung tissues (control lungs not inoculated with A. fumigatus) were negative after culturing.
Histologic examination of tissue sections of the healthy animals showed no signs of infection; that is, infiltration of macrophages or granulocytes was absent (Fig. 1A). The sections of lungs infected with A. fumigatus conidia showed massive infiltration of mainly granulocytes (Fig. 1B). Staining with Grocott methenamine silver revealed truncated A. fumigatus hyphae and germinating conidia in all animals that were inoculated with A. fumigatus conidia (Fig. 1D). Staining of the tissue samples obtained from healthy lungs was negative for aspergillosis (Fig. 1C).

Histologic sections of healthy lung tissue (A and C) and lung tissue with IPA (B and D) from NZW rabbits. Hematoxylin–eosin staining (A and B) shows massive infiltration of polymorphonuclear cells in the infected lung tissue. Grocott methenamine silver staining (C and D) indicates the presence of A. fumigatus hyphae and germinating conidia in the infected lung tissue. (A–D, ×200; inset in D, ×400)
Imaging and Biodistribution
The scintigraphic images acquired immediately and at 2, 4, 6, and 24 h after injection of 111In-DPC11870 or 67Ga-citrate are shown in Figure 2. Immediately after injection, rabbits injected with 111In-DPC11870 showed uptake of radioactivity in heart, lung, liver, and kidneys (Fig. 2A). At later times, accumulation of activity was seen in spleen and bone marrow. The radioactivity concentration in the heart (circulation) and in the lungs decreased with time. The infectious area in the lungs first became visible at 6 h after injection, after radioactivity had lessened in the normal lung tissue and circulation and had accumulated in the infectious foci. Images obtained at 24 h after the injection of the radiolabeled LTB4 antagonist showed an even more evident clearance of radioactivity from noninfected lung areas. This continuous clearance in combination with ongoing accumulation of radioactivity in the infected lung tissue resulted in distinct visualization of the lung lesions at 24 h after injection of the radiolabel. The images showed that, except for the kidneys, activity concentration in the remainder of the body was low.
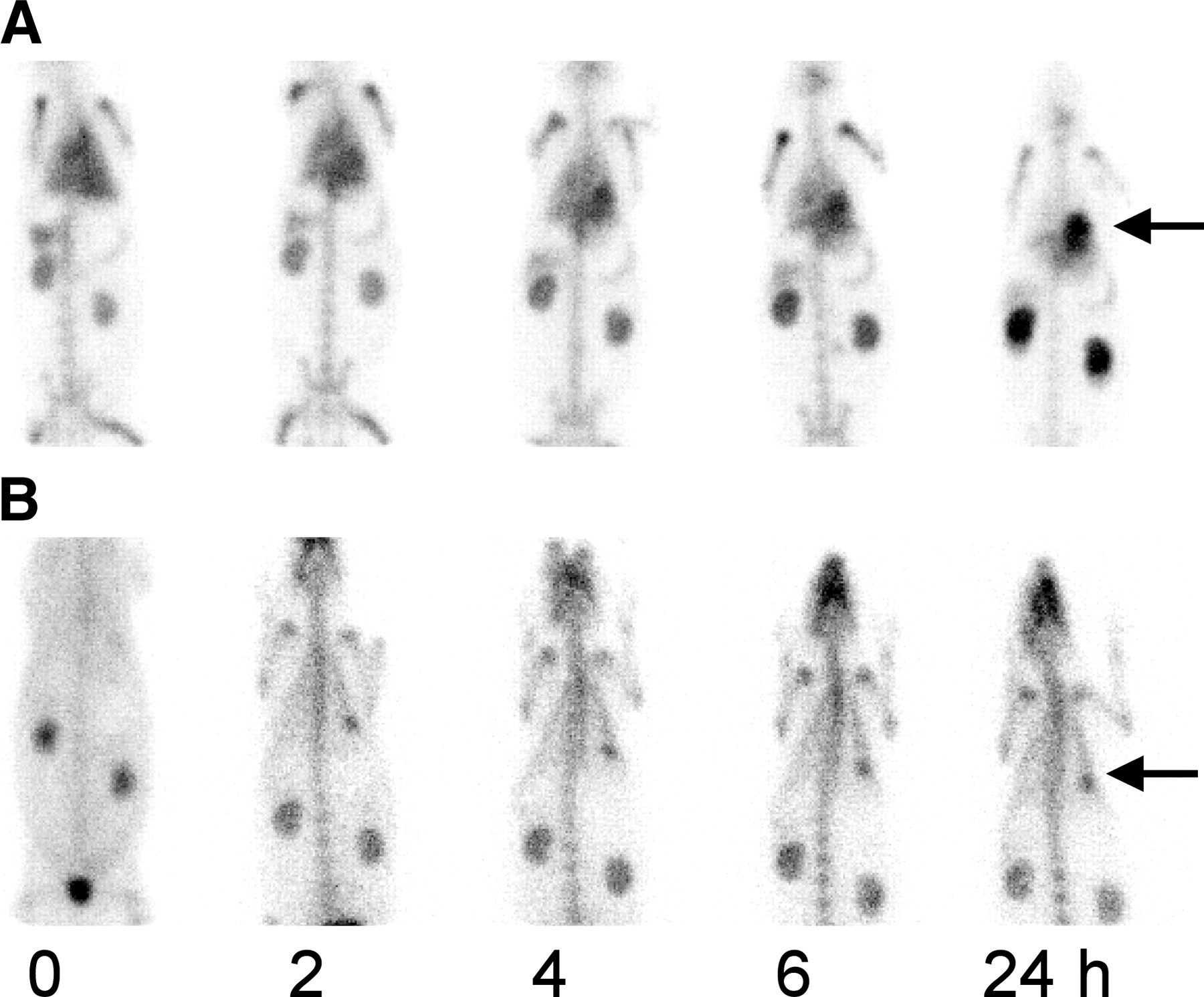
Scintigraphic images of NZW rabbits with pulmonary aspergillosis. The rabbits received 11 MBq of 111In-DPC11870 (A) or 67Ga-citrate (B) intravenously. Anterior images were acquired immediately and at 2, 4, 6, and 24 h after injection of the radiolabel. Arrows indicate focus of infection.
Images acquired at several times after injection of 67Ga-citrate showed distinct pharmacokinetics for this compound, as compared with 111In-DPC11870 (Fig. 2B). Immediately after injection, 67Ga-citrate distributed to the different organs and high activity concentrations were seen in the kidneys and bladder. 67Ga first revealed pulmonary infection at 2 h after injection. The pulmonary lesion was visible as a small focal spot in the left lung. At that moment, uptake of 67Ga in the bone was also present. In contrast to images obtained with the 111In-LTB4 antagonist, all 67Ga-citrate images obtained more than 2 h after injection remained similar.
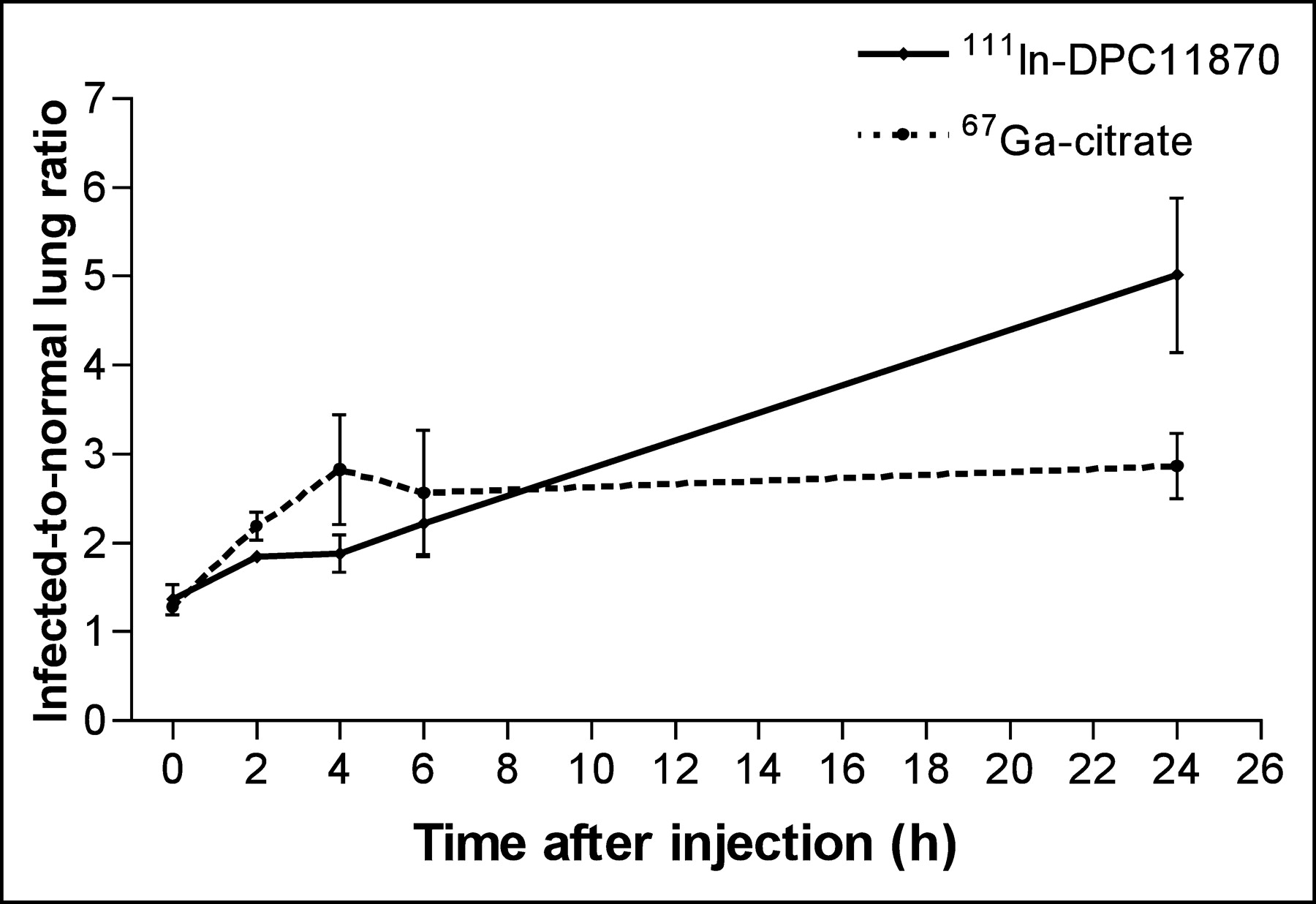
Region-of-interest analysis of the normal and infected lung areas showed that, after injection of 111In-DPC11870, infected-to-normal ratios increased at a constant rate throughout the experiment (Fig. 3). The ratios for 67Ga-citrate increased during the interval 0–4 h after injection but remained constant at later times. At 24 h after injection, the ratios for 67Ga-citrate images were 1.7-fold lower than those for 111In-DPC11870 images (5.0 ± 1.5 and 2.9 ± 0.6 for 111In-DPC11870 and 67Ga-citrate, respectively, P = 0.020).
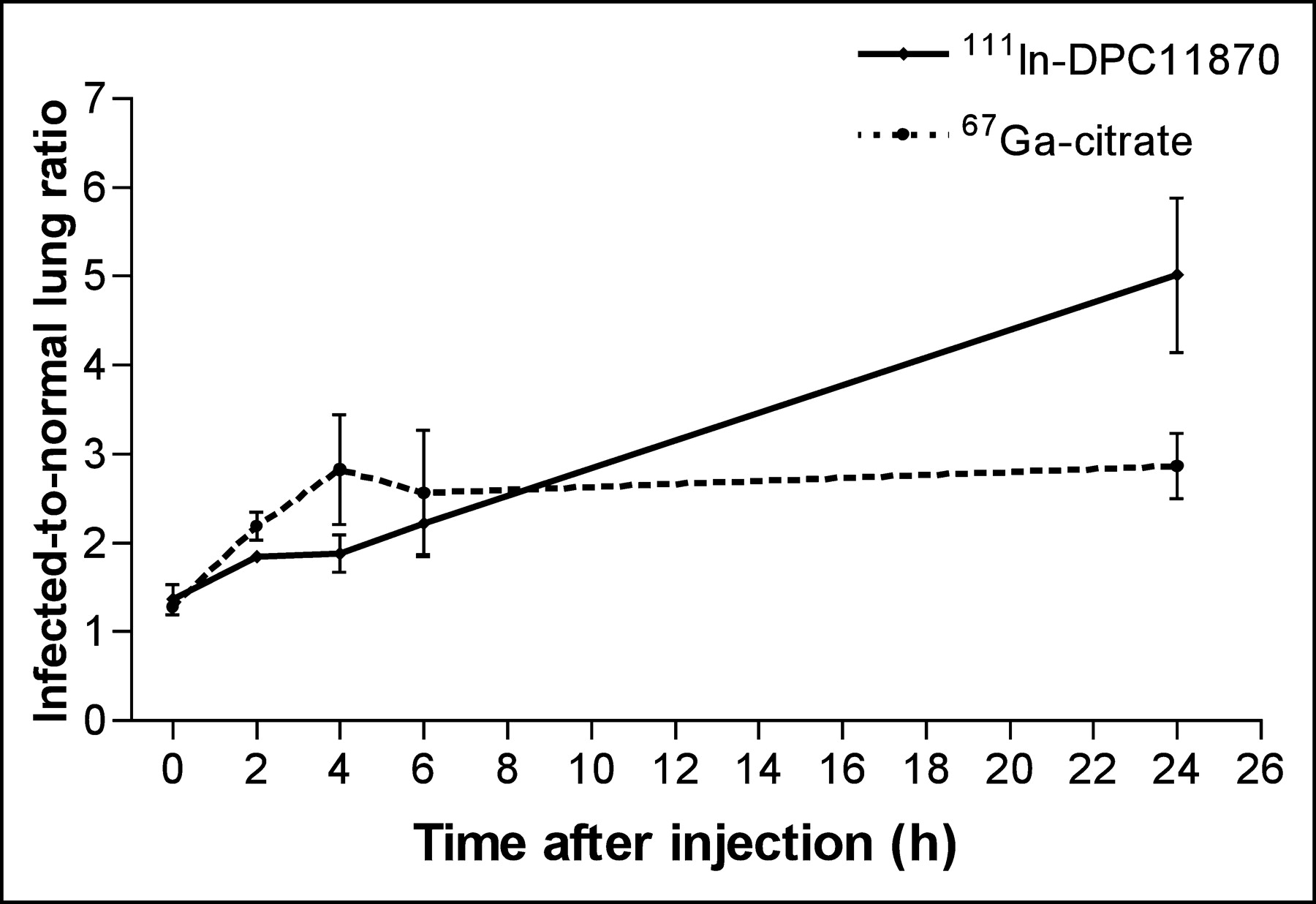
Plot of infected-to-normal ratios vs. time after injection of 111In-DPC11870 (n = 5) or 67Ga-citrate (n = 5) in NZW rabbits with pulmonary aspergillosis. Region-of-interest analysis from images acquired at several time points after injection gave the ratios. Error bars indicate SD.
Biodistribution data (24 h after injection) derived from ex vivo counting of dissected tissues are presented in Figure 4. Uptake of 111In-DPC11870 in infected lung tissue at the time of biodistribution was very high. Uptake of radioactivity was 16-fold higher in infected lung tissue than in normal lung tissue (0.82 %ID/g vs. 0.05 %ID/g, respectively, P = 0.008). Relatively high uptake of the compound was also measured in bone marrow and spleen. Biodistribution data obtained with 67Ga-citrate were concordant with the images, and the highest radioactivity concentration of this radiopharmaceutical was measured in infected lung tissue. As noticed on the images, the radioactivity concentration of 67Ga-citrate was relatively high in the bone and in the kidneys. In contrast to the derived ROI ratios, the infected-to-normal ratio calculated from the biodistribution data at 24 h after injection was significantly (4.1-fold) higher for 67Ga-citrate than for 111In-DPC11870 (P = 0.0005).
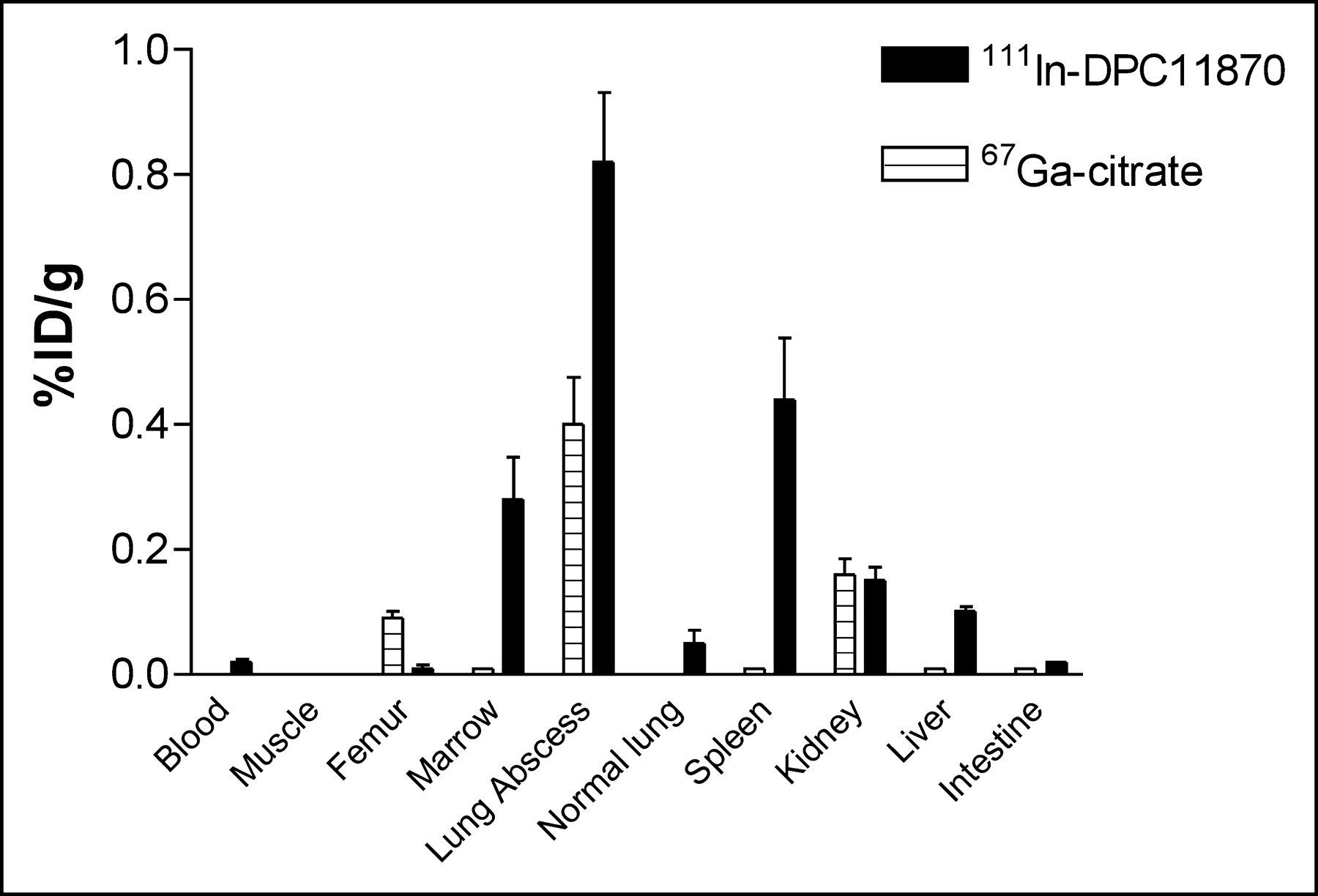
Biodistribution data obtained 24 h after injection of 111In-DPC11870 (n = 5) and 67Ga-citrate (n = 5) in NZW rabbits with pulmonary aspergillosis. Error bars indicate SD.
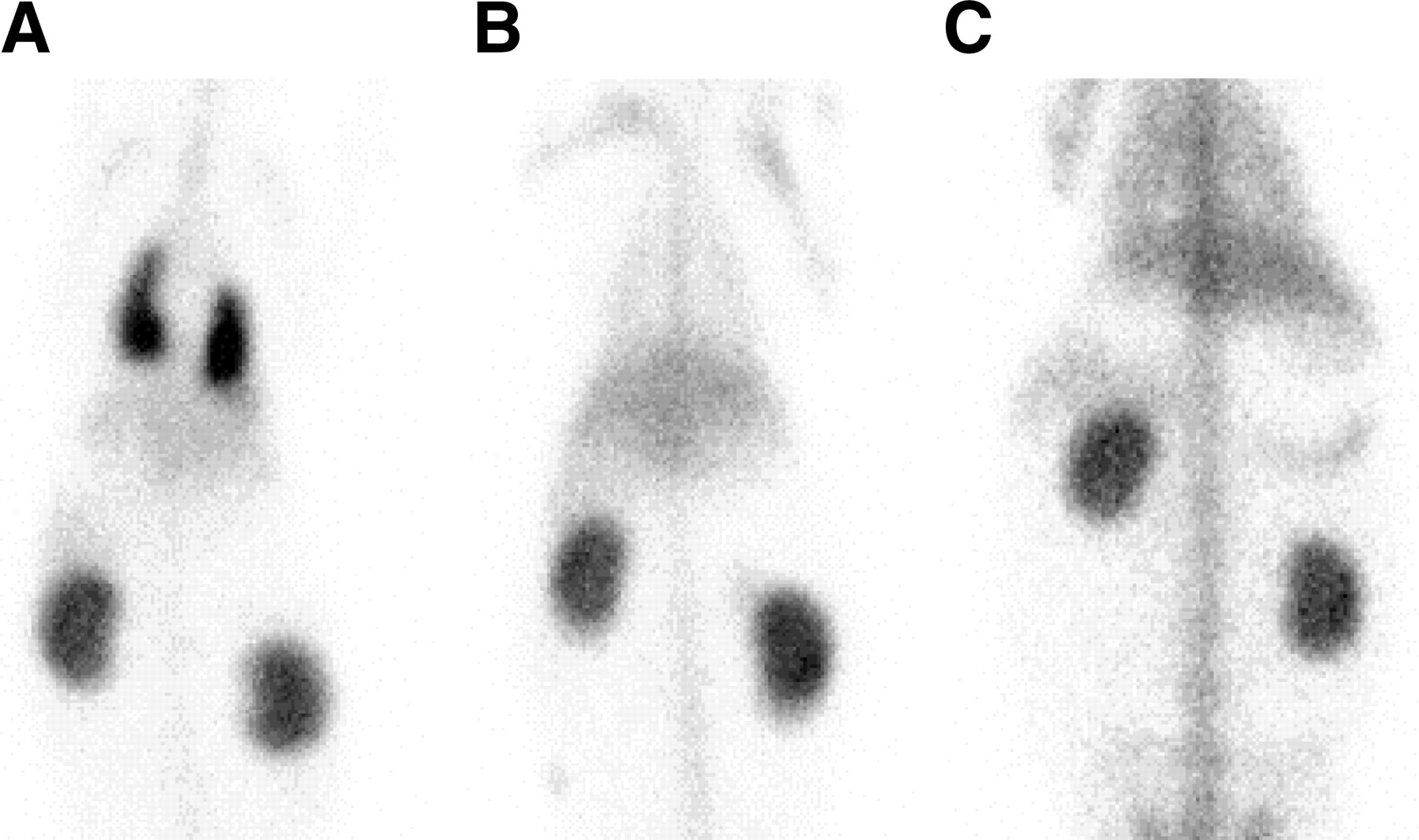
To determine whether the cytarabine injections affected the pharmacokinetics and biodistribution pattern of the radiolabeled LTB4 antagonist, noninfected control animals were included in this study. Images acquired immediately after injection of 111In-DPC11870 appeared similar in all groups. Figure 5 shows 24-h-postinjection images of a cytarabine-treated, A. fumigatus–infected animal; a cytarabine-treated, noninfected animal; and a healthy rabbit injected with 111In-DPC11870. Rabbits not infected with A. fumigatus conidia (either untreated or treated with cytarabine) did not show any accumulation or retention of radioactivity in the lungs. Furthermore, the biodistribution of 111In-DPC11870 in the main organs of these animals (except bone marrow and spleen) was comparable to that in cytarabine-treated, infected rabbits. Distinct differences in radioactivity concentrations were observed in the spleen and bone marrow of healthy animals and animals with aspergillosis. The cytarabine-treated animals showed reduced uptake of 111In-DPC11870 in these organs.
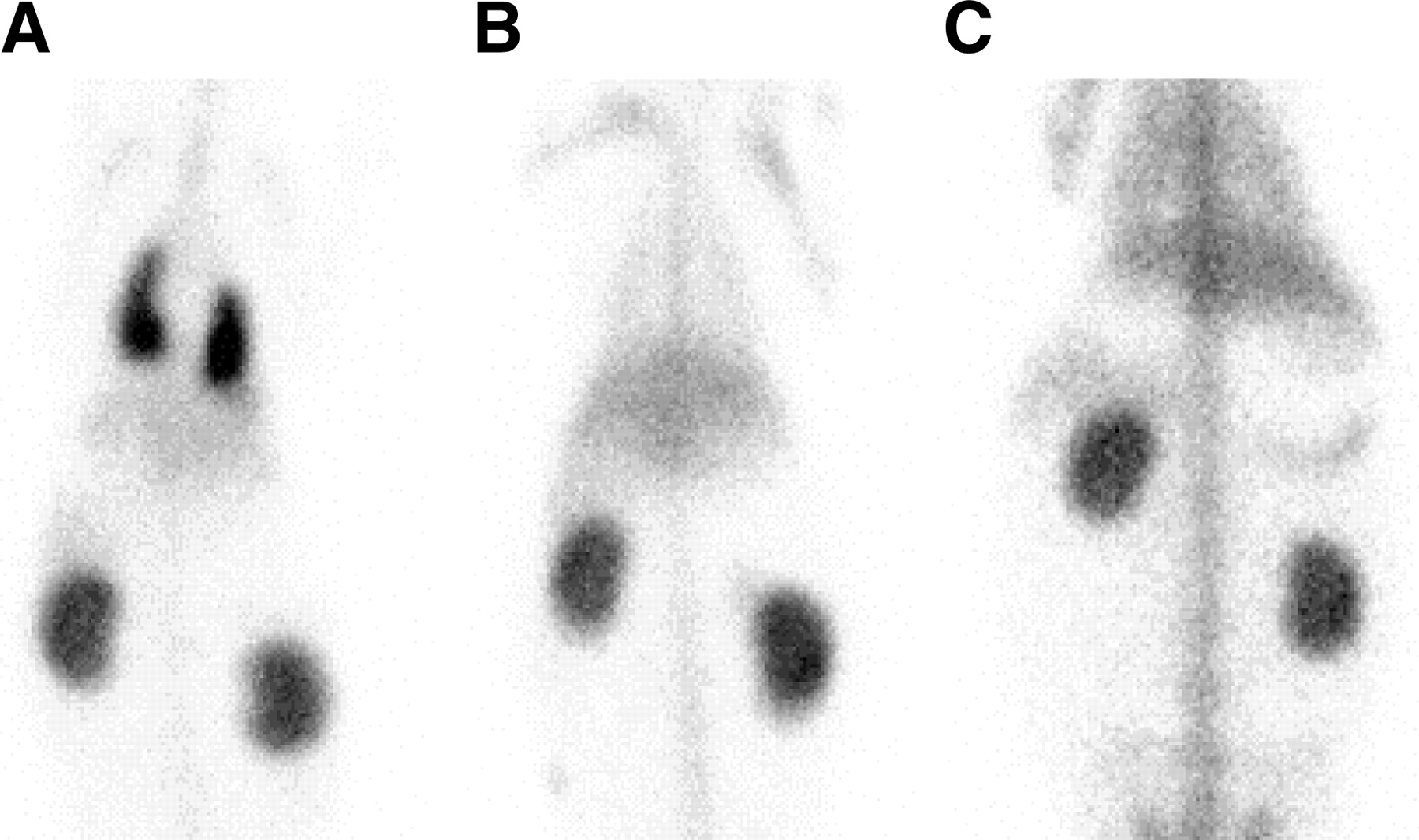
Anterior images acquired 24 h after injection of 111In-DPC11870 in a NZW rabbit with pulmonary infection in both lungs (A), a noninfected animal treated with cytarabine (B), and a rabbit neither infected with A. fumigatus nor treated with cytarabine (C).
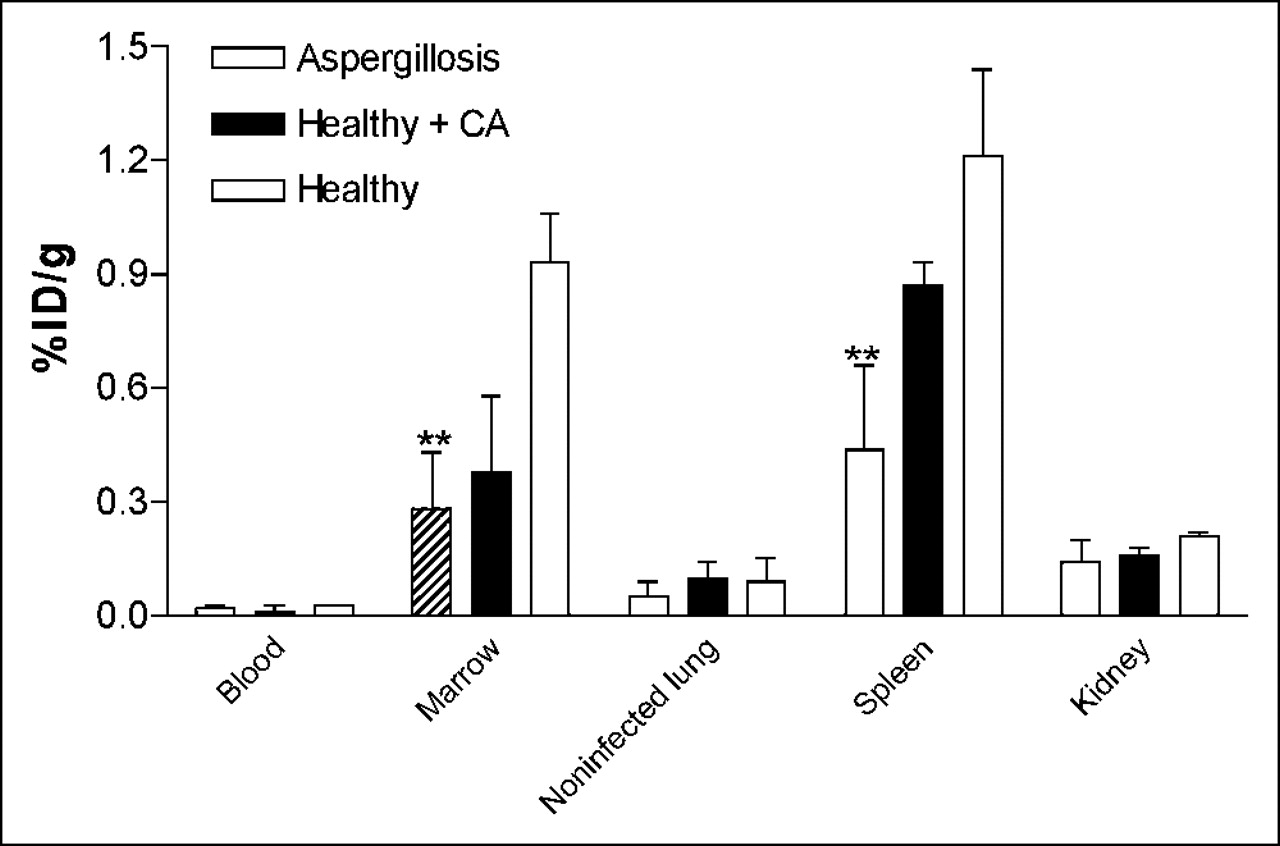
Quantitative measurement of radioactivity revealed that, except for the bone marrow and spleen, concentrations in dissected organs did not significantly differ between the rabbits (healthy or infected) treated with cytarabine and the healthy, untreated animals (Fig. 6). The radioactivity concentration in the bone marrow was lower for cytarabine-treated animals (both infected and noninfected) (0.28% ± 0.15 %ID/g and 0.38% ± 0.20 %ID/g, respectively) than for healthy animals (0.93% ± 0.13 %ID/g). The radioactivity concentration in the noninfected lungs of all 3 groups of animals was similar. Also, the 111In-DPC11870 concentration in the blood of rabbits from all 3 groups was similar (0.02% ± 0.01 %ID/g in rabbits with aspergillosis, 0.01% ± 0.02 %ID/g in rabbits healthy but treated, and 0.03% ± 0.01 %ID/g in rabbits healthy and not treated with cytarabine).

Biodistribution data obtained 24 h after injection of 111In-DPC11870 in NZW rabbits with pulmonary infection in the lung (n = 5), cytarabine (CA)-treated noninfected animals (n = 2), and healthy rabbits neither injected with cytarabine nor infected with A. fumigatus (n = 2). Error bars indicate SD. **P < 0.05; results differ significantly from results in healthy rabbits.
DISCUSSION
In the present study, scintigraphic imaging of pulmonary aspergillosis with a radiolabeled LTB4 antagonist was examined in a rabbit model. The imaging potential of the LTB4 antagonist was compared with that of 67Ga-citrate. Serial scintigraphic images showed that with 111In-DPC11870, the pulmonary infection could be seen from 6 h onward. The images showed that the radiolabeled LTB4 antagonist accumulated in the infectious lesion, whereas the activity concentration in the blood and normal lung tissue decreased with time. The pharmacokinetic properties of the compound in this model were concordant with results found in previous studies (13). Injection of the compound in healthy animals showed that except for the amount of radioactivity in bone marrow and spleen, localization of 111In-DPC11870 was not affected by administration of cytarabine). This finding implies that despite the lowered WBC counts in the circulation, sufficient activated neutrophils migrated to the site of infection. No differences were seen in radioactivity concentration in the blood and the major organs. The lower amounts of radioactivity in the spleen and bone marrow of animals pretreated with cytarabine were probably due to the reduced number of premature WBCs in these organs. Cytarabine is a nucleoside analog with cytotoxic activity mainly affecting replicating cells (16). The lower radioactivity concentration in the bone marrow may be due to the fact that repeated injection of cytarabine will immediately reduce the numbers of proliferating (LTB4 receptor–positive) promyelocytes in the bone marrow, whereas mature and activated neutrophils will be less affected and would require longer treatment with this antimetabolite. This is in agreement with the massive infiltration of leukocytes found in the infected lung tissue of these rabbits (histologic staining).
The primary aim of this study was to test whether the radiolabeled LTB4 antagonist 111In-DPC11870 could allow visualization of pulmonary aspergillosis in NZW rabbits. In addition, we compared the imaging and biodistribution characteristics of 111In-DPC11870 with those of 67Ga-citrate, the radiopharmaceutical generally used to visualize pulmonary infections in patients (17). Besides the relatively high sensitivity for acute and chronic infection and inflammation, a few other disadvantages of 67Ga-citrate include the relatively long biologic half-life, physiologic uptake in bone, and excretion via the bowel (the last mainly at later times) (18). Images acquired after injection of 67Ga-citrate in rabbits with A. fumigatus infection clearly delineated the infected lesions in the lungs at early times. Physiologic uptake in the bone was first seen on images 2 h after injection, and the amount of radioactivity did not decrease with time. Region-of-interest analysis indicated that the infected-to-normal ratios found with 111In-DPC11870 increased with time (in contrast to the ratios found after injection of 67Ga-citrate) and resulted in higher ratios for 111In-DPC11870 than for 67Ga-citrate at 24 h after injection of the radiolabeled agents. The increasing infected-to-normal ratios after injection of the radiolabeled LTB4 antagonist can be explained by the continuous accumulation of radioactivity at the site of infection in combination with ongoing clearance from the blood (corresponding to background). 67Ga-Citrate cleared more quickly from the circulation than did 111In-DPC11870; therefore, at later time points the ratios remained constant. Normally, regions of interest on images are evaluated to diagnose pulmonary infection. Physiologic uptake of 67Ga-citrate in the bone (background tissue) deteriorated the images and reduced the infected-to-normal ratios derived from region-of-interest analysis. Our data indicate that although pulmonary lesions are visualized, that visualization may be affected by physiologic uptake. This outcome may be more pronounced in patients, especially because images are generally acquired at 18–72 h after the injection of 67Ga-citrate (19,20).
In this study, we showed that 111In-DPC11870 allowed clear visualization of pulmonary aspergillosis in rabbits. Visualization was possible because of accumulation of radioactivity in the infection. In a previous study, we determined that this accumulation is specific and receptor mediated (13). Because of the massive infiltration of granulocytes in the infectious foci and accumulation of 111In-DPC11870 in the lesions, this model represents acute pulmonary infection, and presumably, 111In-DPC11870 might allow visualization of acute pulmonary infection in general. Because uptake of 111In-DPC11870 in the bone marrow and retention of radioactivity in the kidneys could limit the clinical applicability of the compound, we now aim to produce a new analog of the LTB4 antagonist DPC11870 that can be labeled with 99mTc. A 99mTc-labeled compound not only could reduce the absorbed dose to these organs but also might improve images because of the higher resolution and reduced visualization of bone marrow (due to higher attenuation by the bone). Nevertheless, because of the distinct visualization of pulmonary lesions made possible by injection of 111In-DPC11870, this agent could be a valuable tool for the diagnosis of acute pulmonary infections in patients.
CONCLUSION
The present study demonstrated that the radiolabeled LTB4 antagonist DPC11870 allows visualization of pulmonary infection in rabbits with aspergillosis. Visualization of lesions began 6 h after injection and improved with time because of retention of radioactivity in the infected lung tissue. The results of this study indicate that 111In-DPC11870 could contribute to the diagnosis of acute pulmonary infection.
Acknowledgments
The authors thank Gerry Grutters, Margo van den Brink, and Maichel van Riel (University of Nijmegen, Central Animal Laboratory) for technical assistance and microbiologic analysis.
Footnotes
Received Nov. 18, 2003; revision accepted Apr. 12, 2004.
For correspondence or reprints contact: Julliëtte E.M. van Eerd, BSc, Department of Nuclear Medicine, University Medical Center Nijmegen, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands.
E-mail: j.vaneerd{at}nucmed.umcn.nl





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}