


Abstract
Ciprofloxacin labeled with 99mTc specifically binds to various bacteria. Thus, it potentially constitutes a specific marker allowing discrimination between septic arthritis/osteomyelitis and aseptic osteoarticular diseases. The aim of this prospective study was to evaluate such properties in patients with skeletal diseases. Methods: We prospectively investigated 2 groups of patients: patients with suspected osteoarticular infections (G1, n = 16) and a control group of patients with a presentation of osteoarticular diseases and no sign suggestive of infection (G2, n = 11). All had clinical, biologic, and radiologic evaluations and had 1-, 4-, and 24-h images from 99mTc-ciprofloxacin scintigraphy (370 MBq) before planned biopsy or surgery. For 23 patients, the scintigraphic results were compared with histologic and bacteriologic analyses of biopsy tissue samples; for 4 patients, the scintigraphic results were compared with the findings from 23 ± 5 mo of follow-up. Results: In G1, 99mTc-ciprofloxacin findings were true-positive in all 11 infected sites, true-negative in 2 cases, and false-positive in 3. In G2, 99mTc-ciprofloxacin was true-negative in 4 cases and false-positive in 7. Neither the location of 99mTc-ciprofloxacin activity nor its intensity or kinetics between 1, 4, and 24 h allowed discrimination between infection and aseptic diseases (sterile loosened joint replacement, pseudoarthrosis, or arthrosis). Sensitivity, specificity, and accuracy were 100%, 37.5%, and 63%. Conclusion: 99mTc-Ciprofloxacin scintigraphy showed good sensitivity and a high negative predictive value for the detection of bone and joint infection, but it did not discriminate between infected and aseptic osteoarticular diseases in symptomatic patients referred for surgery.
Discrimination between bacterial infection and sterile inflammation is clinically relevant in many situations. Accurate diagnosis between septic and aseptic painful orthopedic hardware is crucial, as both the surgical management and outcome may differ. In the presence of infection, delayed reconstruction after prolonged antibiotherapy is needed in most cases (1–3). Clinical, biologic, and radiologic criteria in cases of mild torpid infection are neither sensitive nor specific (1,2). Fluid cultures after joint aspiration may be negative for infection in the presence of infection (about 50% sensitivity) (4). Radionuclide imaging has been extensively used for this issue. However, most of the radiopharmaceuticals proposed constitute tracers of the inflammation process (5). Labeled autologous leukocytes carry the drawback of ex vivo blood cell manipulation, with the associated infectious risk and long duration of radiolabeling. Clearly, radiopharmaceuticals that bind to a variety of bacteria would be better candidates for specific infection imaging (5). The first to be proposed was ciprofloxacin radiolabeled with 99mTc (Infecton; Draximage Inc.), which is supposed to bind to DNA-gyrase and topoisomerase IV of bacteria, as does unlabeled ciprofloxacin (6,7). However, previously reported data about the specificity of 99mTc-ciprofloxacin for infection are contradictory (8–16).
This prospective study aimed to determine the value of 99mTc-ciprofloxacin imaging for discrimination between septic and sterile osteoarticular diseases, using bacteriologic and histologic analyses of biopsy samples as the gold standard for scintigraphic evaluation, by selecting patients with planned biopsy or revision surgery.
MATERIALS AND METHODS
Patients
Two groups of patients were prospectively included in the study: 16 patients with suspected septic arthritis or osteomyelitis (G1, 7 men and 9 women) and 11 patients with a presentation of osteoarticular disease with no sign suggestive of infection (G2, 5 men and 6 women). Biopsy or revision surgery was planned for all patients, and all were experiencing pain and motion limitation. G1 included patients who additionally had local or general clinical signs of infection (edema, redness, purulent fistula, or fever), persistent biologic inflammatory syndrome (plasma C-reactive protein elevation with or without blood leukocyte elevation), or radiologic signs suggestive of osteomyelitis. G2 included patients who had no local sign of infection, no fever, normal white blood cell counts, and normal blood C-reactive protein levels and who had received no antibiotic therapy for at least 3 mo before inclusion in the study. Patients less than 19 y old were excluded. Mean age was 60 ± 18 y.
All patients underwent clinical, radiologic, biologic, and 99mTc-ciprofloxacin scintigraphic evaluations. Fifteen patients also had joint fluid aspiration with bacteriologic and cytologic analyses. At the time of scintigraphy, 5 G1 patients had been receiving antibiotic therapy for 16.0 ± 16.2 d.
99mTc-Ciprofloxacin Scintigraphy
All patients were referred for scintigraphy after they gave informed consent. The nuclear medicine physician to whom the patient was referred was unaware of the patient group and the results of other imaging modalities, both at the time of imaging and at the time of imaging evaluation. As previously described (11,14,17), 99mTc-ciprofloxacin was prepared according to manufacturer instructions, using a kit provided by the Nuclear Medicine Department of St. Bartholomew’s Hospital. The 99mTc-ciprofloxacin kits comprise 2 vials: vial 1, containing 1 mL of 99mTc-ciprofloxacin (including 2 mg of ciprofloxacin), and vial 2, containing 500 μg of stannous tartrate. Sodium pertechnetate (400 ± 20 MBq) was drawn up from a 99mTc generator that had been freshly eluted (within 24 h). The content of vial 1 was drawn up using a 25-gauge orange needle (to reduce the number of metal ions in the needle complexing with the 99mTc-ciprofloxacin). One milliliter of 0.9% sodium chloride was injected into vial 2, which was shaken to dissolve the dried powder. The sodium pertechnetate was then added to vial 2, immediately followed by the 99mTc-ciprofloxacin. The vial was shaken, and after incubation for 5 min at room temperature, quality control was performed. Then, 370 MBq of the preparation were drawn up with a blue 23-gauge needle attached to the end of the syringe and were injected into the patient within 1 h of radiolabeling. For quality control, paper chromatography (number 1 paper; Whatman International), with butanone as eluent, and Sep-Pak (Waters Corp.) chromatography were used. The radiochemical purity was always >96% using the 2 techniques. This level of purity excluded a significant amount of radiolabeled colloids in the preparation. The use of 99mTc-ciprofloxacin was approved by the Medical Ethical Committee of our hospital.
Planar anterior and posterior views, with or without profile views, were obtained 1, 4, and 24 h after injection. The images were acquired by a dual-head gamma camera (DST or DST-Xli; SMV International) fitted with high-resolution parallel collimators, using a 15% window centered on 140 KeV, as previously described (8–14,17). Matrix size was 256 × 256 and acquisition times were 600 s at 1 and 4 h and 900 s at 24 h. Whole-body acquisitions were also performed 1 and 4 h after injection for 11 patients, with a scan speed of 12 cm/min and a matrix size of 128 × 512.
Bacteriologic and Histologic Analyses
Tissue biopsy samples were obtained from 15 of 16 G1 patients (during surgery for 12; by external biopsy puncture for 3) and from 8 of 11 G2 patients (during surgery for 7; during knee arthroscopy for 1). Surgery, arthroscopy, and biopsies were performed after 99mTc-ciprofloxacin scintigraphy. At the time of surgery, 4 patients of G1 had been receiving antibiotic therapy for 46 ± 42 d. During surgery, joint fluid and tissues were sampled and then bacteriologically and histologically analyzed. The macroscopic findings, the sites of sampling, and the histologic and bacteriologic data obtained from each sample were recorded for data analysis.
One G1 patient and 1 G2 patient refused surgery and were followed for 24 and 18 mo, respectively. Two G2 patients were not operated on because the symptoms were finally found to be related to a cause other than the initially suspected disease.
Data Analysis
The 99mTc-ciprofloxacin scintigrams were visually evaluated by 2 experienced nuclear medicine physicians unaware of the patient group and of the results of other imaging modalities.
The scintigrams were interpreted as positive or negative for infection by visual analysis. They were considered positive for infection when 99mTc-ciprofloxacin uptake at the site studied was greater than that in healthy tissues of the contralateral or ipsilateral adjacent sites on 1-, 4-, and 24-h images. Because 99mTc-ciprofloxacin is supposed to bind specifically to live bacteria, increased 99mTc-ciprofloxacin uptake was considered positive for infection whatever the anatomic structure concerned (bone, the synovial cavity, or extra-articular soft tissues). The scintigrams were considered negative for infection when 99mTc-ciprofloxacin uptake was comparable to that observed in healthy tissues of the contralateral or ipsilateral adjacent sites at any imaging time or when increased 99mTc-ciprofloxacin uptake that had been visible on 1- and 4-h images dramatically decreased to become scarcely visible on 24-h images.
On each anterior scintigram positive for infection, regions of interest (ROIs) were drawn: one over the pathologic site and one over the normal contralateral or ipsilateral adjacent site. Mean activity (cpm) per pixel was determined in each ROI. Then, the pathologic-to-normal-site activity ratios (PNARs) were scored. PNARs were not used to determine whether 99mTc-ciprofloxacin scans were positive or negative for infection; they were obtained only for scans that had been considered positive on visual analysis.
The final diagnosis was determined by both the orthopedic surgeon and the medical physician (a specialist in osteoarticular infection), by analysis of bacteriologic and histologic data obtained from tissue biopsies (n = 23) or by 3 ± 5 mo follow-up (n = 4). Infection was confirmed when one of the following criteria was present: positive cultures of biopsy specimens, purulence at the time of surgery, or acute inflammation consistent with infection on histopathologic examination. Infection was disproved in the absence of such criteria or in the absence of any suggestive sign or symptom during at least 1 y of follow-up.
For statistical analysis, differences between the PNARs were analyzed using the t test. The level of significance was set at P < 0.05.
RESULTS
Patient data are recorded in Table 1.
Patient Data
Final Diagnosis
According to bacteriologic and histologic analyses of biopsy samples, 11 of 16 G1 patients were infected and 4 were not. One G1 patient (patient 18) with recrudescent pain in a prosthetic knee refused surgery. During a 24-mo follow-up without antibiotic therapy, the symptoms were stable, the inflammatory syndrome disappeared, and the patient was considered uninfected.
In all G2 patients who underwent surgery (n = 8), bacterial and histologic analyses of intraoperative samples revealed no infection. In 1 G2 patient who refused surgery (patient 25), an 18-mo follow-up without antibiotic therapy did not reveal any clinical, biologic, or radiologic signs of infection, and the diagnosis of aseptic prosthetic loosening was retained. Two other G2 patients (patients 15 and 17) were finally found to have no prosthetic infection or loosening but, rather, cement extrusion and sciatica; surgery was cancelled, and follow-up (30 and 21 mo, respectively) did not reveal any sign of infection.
Scintigraphic Results
The biodistribution pattern of 99mTc-ciprofloxacin was identical to that described in previous studies: high uptake in the kidneys with excretion to the urinary bladder, moderate uptake in the liver and spleen, no bone marrow uptake, and blood-pool activity (visible cardiac cavities) on 1- and 4-h images (Fig. 1) (9,17).
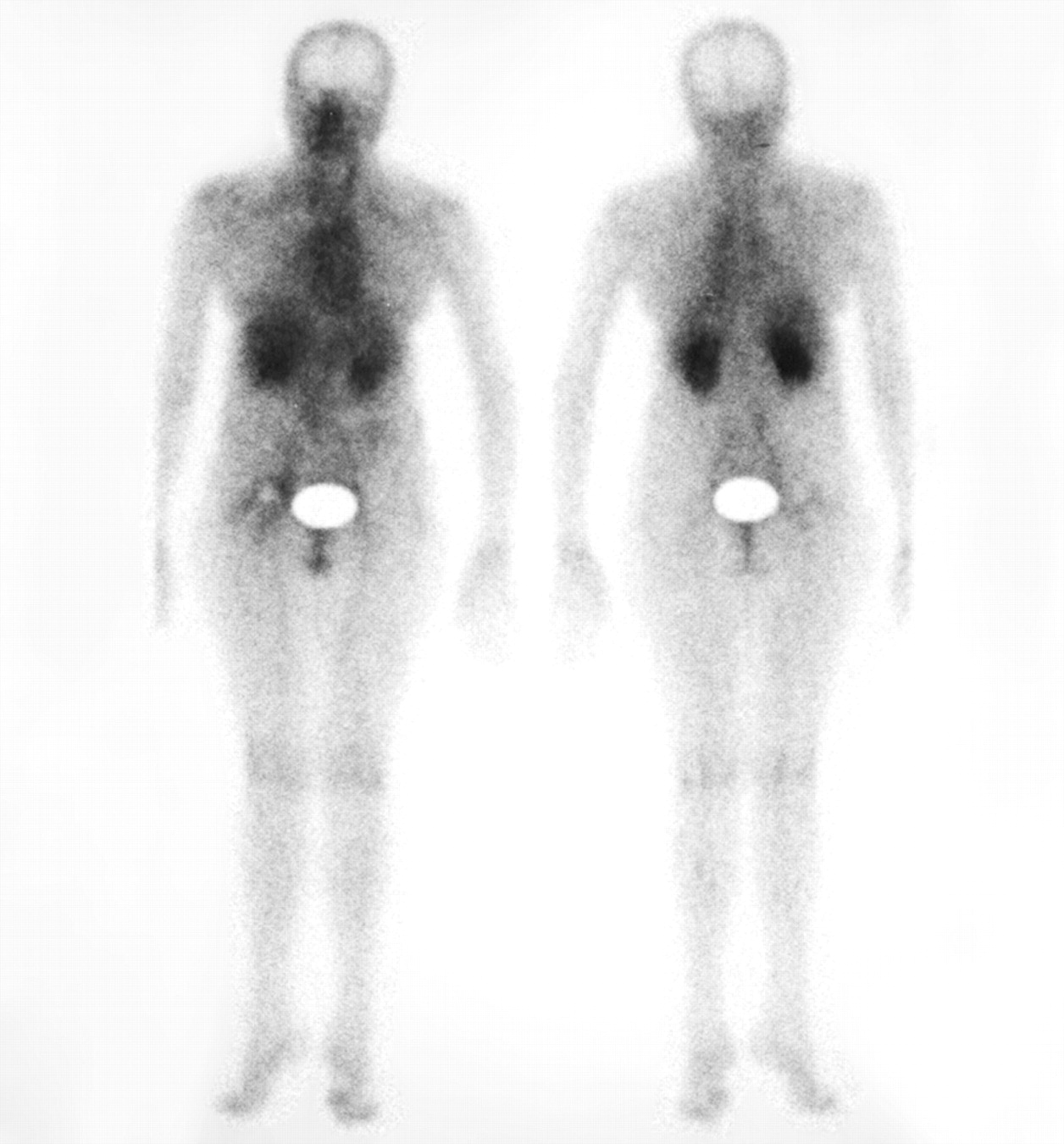
Anterior and posterior whole-body 99mTc-ciprofloxacin images 4 h after injection.
In G1, 99mTc-ciprofloxacin findings were positive for all 11 infected sites (i.e., true-positive) (Figs. 2B, 3A, and 4A). The findings were true-negative for 2 G1 patients with no infection but false-positive for 3 uninfected G1 patients, including 1 with sterile pseudoarthrosis and 1 with a sterile loosened hip replacement. The sensitivity, specificity, and positive and negative predictive values for 99mTc-ciprofloxacin scintigraphy in G1 were 100%, 40%, and 78% and 100%, respectively.
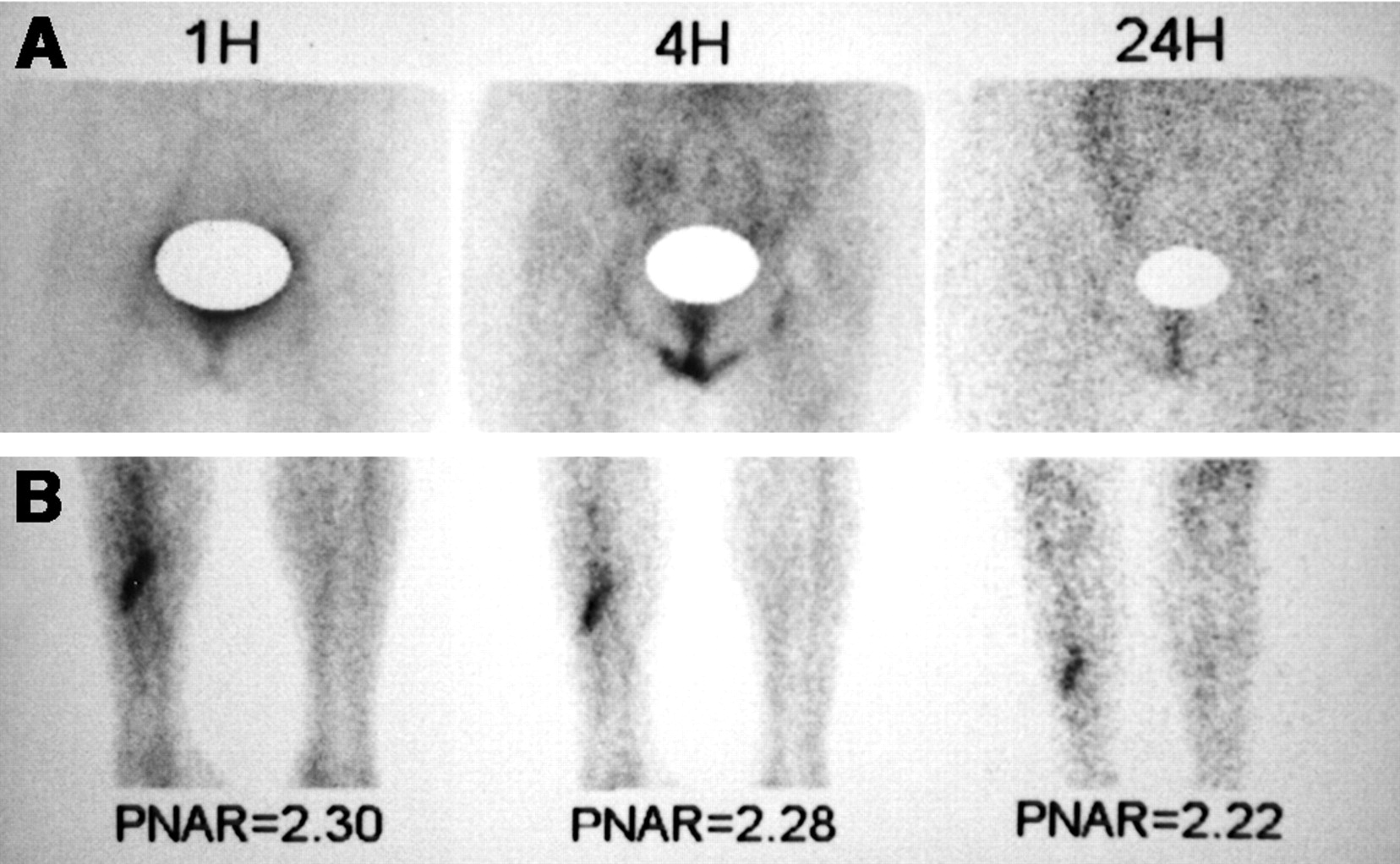
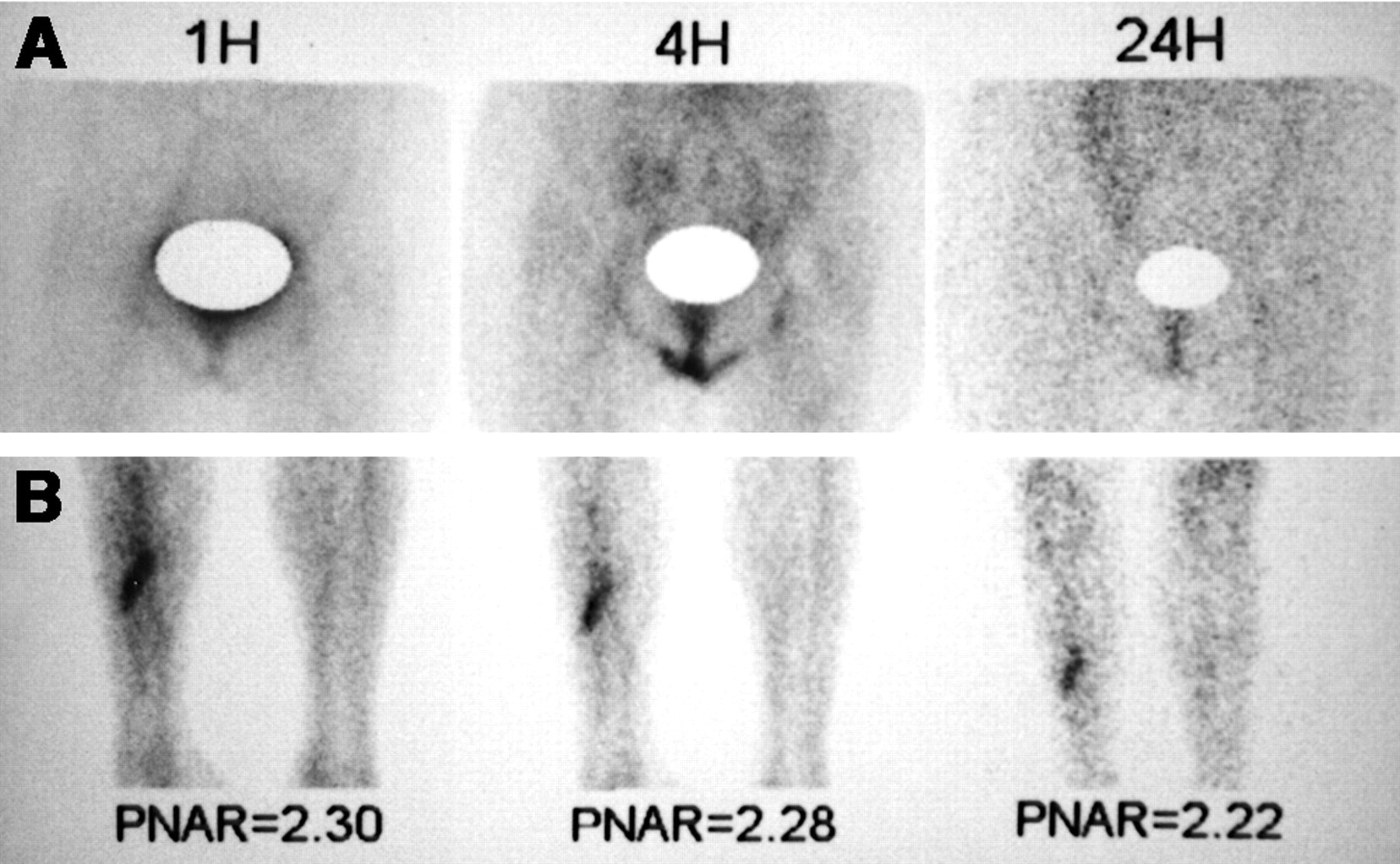
1-, 4-, and 24-h images of negative and positive 99mTc-ciprofloxacin findings. (A) Negative findings (patient 3 with aseptic loosening of left hip prosthesis). (B) Positive findings (patient 9). Increased 99mTc-ciprofloxacin uptake is seen at seat of fracture (right tibia) on all images.

Examples of 99mTc-ciprofloxacin scintigraphy in prosthetic hips. (A) Patient 13, with infected right prosthetic hip and extensive soft-tissue infection (surgical findings of inflamed cutaneous scar and pus in muscles), shows activity in periprosthetic femur and soft tissues. (B) Patient 7, with aseptic loosening of total right-hip replacement (histologic intraoperative findings of reactive inflammation to metallosis), shows activity around prosthetic femoral neck, in periprosthetic femur, and in socket.
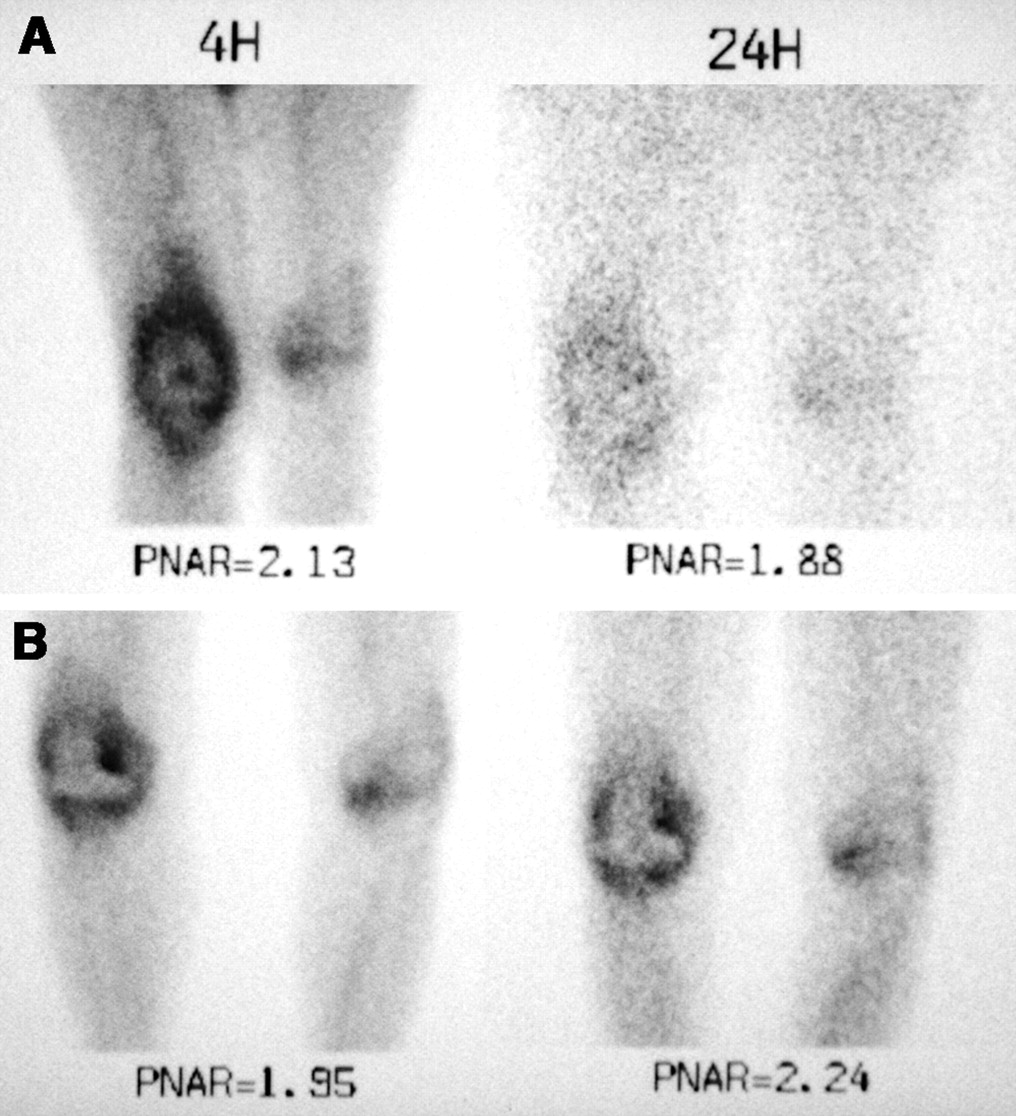
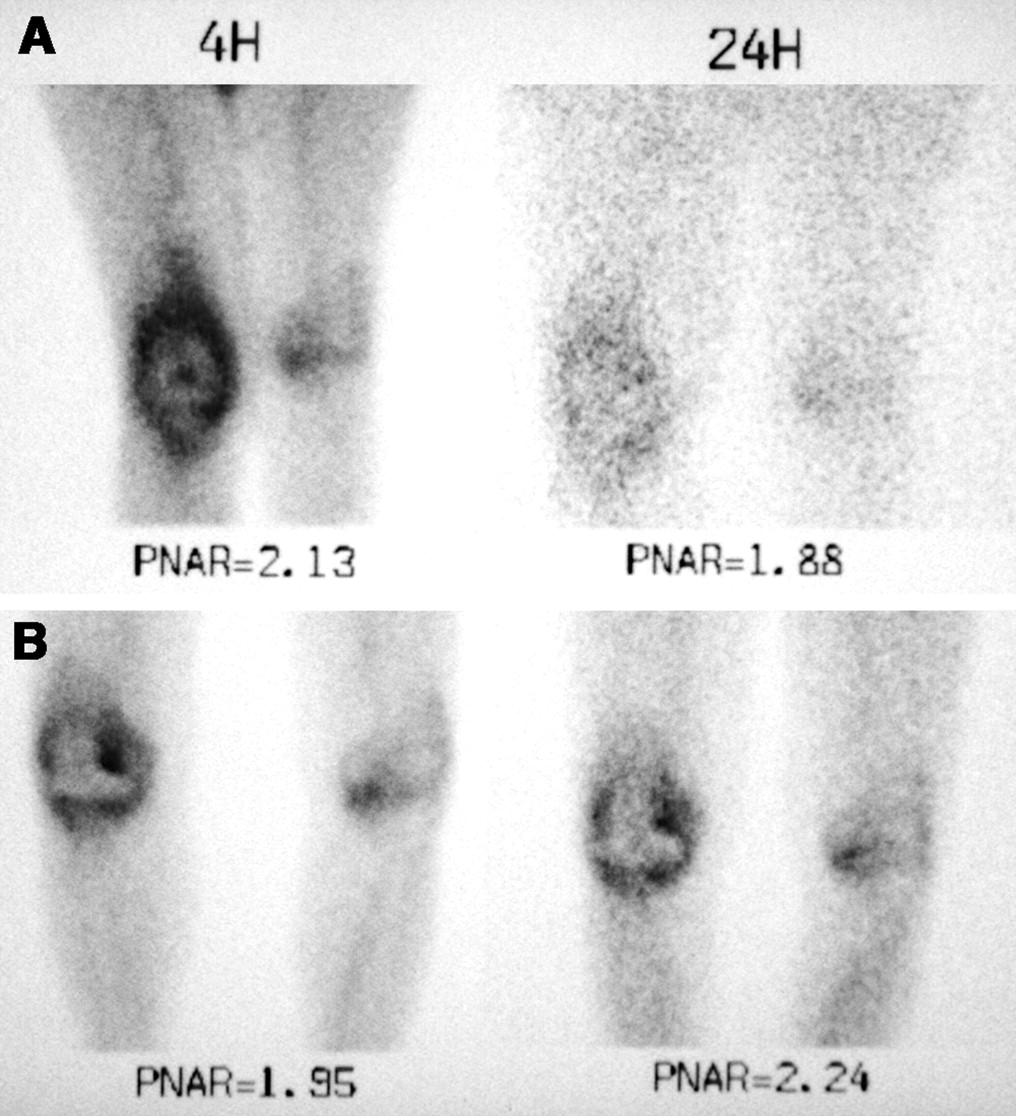
Examples of 99mTc-ciprofloxacin scintigraphy in prosthetic knees. (A) Patient 26, with infected right prosthetic knee, shows activity in synovial cavity and periprosthetic tibia. (B) Patient 27, with aseptic total right-knee replacement, shows activity in synovial cavity, periprosthetic tibia, and femur. Both patients show mild but significant 99mTc-ciprofloxacin activity in left knee arthrosis.
In G2, 99mTc-ciprofloxacin findings were true-negative for 4 uninfected patients (Fig. 2A). The findings were false-positive for 7 uninfected patients: 4 with a sterile loosened joint replacement, 1 with sterile pseudoarthrosis, 1 with coxarthrosis, and 1 with an uninfected and unloosened joint replacement (patient 15) (Figs. 3B and 4B). The normalcy rate in this uninfected group was 36.4%.
The overall sensitivity of 99mTc-ciprofloxacin scintigraphy was 100%, specificity was 37.5%, and accuracy was 63%. Intraoperative histologic data indicated that increased 99mTc-ciprofloxacin uptake in uninfected patients was related to pseudoarthrosis, to arthrosis, or to sterile prosthetic loosening with reactive inflammation to metallosis (with histiocytes and giant cells) (Table 1). The PNARs obtained for infected sites were not significantly different from those obtained for uninfected sites (positive scan findings): 2.47 ± 0.80 versus 1.88 ± 0.31 (not statistically significant [NS]) for 1-h images, 2.43 ± 0.81 versus 1.86 ± 0.33 (NS) for 4-h images, and 2.10 ± 0.41 versus 1.82 ± 0.35 (NS) for 24-h images. 99mTc-ciprofloxacin uptake was stable from 1 to 4 h after injection in all cases and dramatically decreased from 4 to 24 h in 3 uninfected patients, with only scarcely visible uptake on 24-h images (scan findings interpreted as negative). If only 1- or 4-h images had been considered for interpretation, these latter 99mTc-ciprofloxacin findings would have been interpreted as positive, and specificity would have dropped to 19%. In joints, the pattern of 99mTc-ciprofloxacin uptake (in synovial cavity, bone, or both) was not able to discriminate between infection and no infection for the final diagnosis (Table 1). 99mTc-Ciprofloxacin activity in extra-articular soft tissues was observed only in patients with soft-tissue infection (fistulae or inflamed cutaneous scars).
Increased 99mTc-ciprofloxacin uptake was also observed in 3 associated asymptomatic prosthetic joints (1 shoulder and 2 knees) and in 5 associated joints with arthrosis (2 shoulders and 3 knees; Fig. 4).
DISCUSSION
Radionuclide imaging has been extensively used to help in differential diagnosis between infected and aseptic osteoarticular diseases. 67Ga, radiolabeled polyclonal IgG, and nanocolloids show low specificity for infection because they accumulate in nonspecific inflammation, which is present in sterile prosthetic loosening (18,19). Some authors reported that coupled 99mTc-methylene diphosphonate (MDP)/67Ga scintigraphy had better specificity, with accuracy ranging from 60% to 80% (when considering matched 99mTc-MDP and 67Ga images to represent negative findings) (18). 111In or 99mTc-labeled autologous leukocytes seem more accurate, especially when associated with labeled colloids or when late 24-h images are obtained, with sensitivity ranging from 75% to 100% and specificity ranging from 73% to 100% (20–27). Late images obtained 24 h after the injection of 99mTc-hexamethylpropyleneamine oxime leukocytes seem useful for detecting chronic infections and for discriminating between infection (persisting or increasing uptake) and sterile inflammation (decrease in tracer uptake) (27). Labeled antigranulocyte antibodies seem comparable to or less specific than labeled leukocytes, according to some authors (28,29).
99mTc-Ciprofloxacin was the first tracer specially designed to differentiate infection from sterile inflammation by specifically targeting live bacteria (7). Some previous clinical studies reported good specificity (85%–96%) in skeletal infections (8–13). In contrast, we found good sensitivity (100%) but low specificity (37.5%), since we observed increased 99mTc-ciprofloxacin uptake in sterile loosened joint replacements with reactive giant cell inflammation to metallosis as well as in sterile pseudoarthrosis and arthrosis. Several factors may explain these discordant results. In most previous studies, uninfected patients may not have had aseptic osteoarticular diseases as severe as in our study, since the patients were not operated on in most cases (8–11). Most authors did not use the same criteria for infection as in our study (8–11). We must emphasize that microbiologic cultures from tissue samples remain the gold standard for the diagnosis of osteoarticular infections and that histologic examination of intraoperative tissue samples should also form part of the investigative protocol to distinguish between aseptic and septic disease (1). The interpretation criteria used for the 99mTc-ciprofloxacin scans differed from one study to another. Some authors considered 99mTc-ciprofloxacin uptake in the synovial cavity of the knees to be a negative finding (“nonspecific uptake”) (11,13). In our experience, the topography of 99mTc-ciprofloxacin uptake (bone, synovial cavity, or both) was not able to discriminate between infection and no infection for the final diagnosis (Table 1 and Fig. 3). Tracer uptake in soft tissues outside the synovial cavity was, as could be expected, observed in patients with soft-tissue infection (fistulae or inflamed cutaneous scars) but not in patients with localized, nonextensive septic arthritis or osteomyelitis (Table 1 and Figs. 3A and 4A). Other authors considered highly or moderately increased uptake to be the only positive scan finding. When slightly increased uptake, seen in 11 of 13 periprosthetic regions without infection, was also considered to be a positive result, specificity dropped from 92% to 23% (12). In our study, the intensity of 99mTc-ciprofloxacin uptake was comparable in infected and uninfected positive sites, with PNARs as high as 2.36 (mean, 1.86 ± 0.34) on 4-h images of uninfected sites. In addition, in agreement with the experience of Dumarey et al. (14), our experience was that late 24-h images were not able to discriminate infection. Despite low counting statistics, 24-h 99mTc-ciprofloxacin images were not difficult to interpret by direct comparison with 4-h images, as is routinely performed with 99mTc-leukocytes (Figs. 1, 3, and 4).
In agreement with our results, a low specificity of 99mTc-ciprofloxacin for osteoarticular infections (54.5%) was recently reported for a retrospective study in which 99mTc-ciprofloxacin accumulation in growth plates, noninfected prosthetic knees, pseudoarthrosis, palindromic rheumatism, and postoperative fibrosis of the lumbar spine was described (14). False-positive findings in avascular hip necrosis, fibrous dysplasia of the right ulna, rheumatoid and psoriatic arthritis, nonunion fracture, and uninfected prosthetic joints were also reported by other authors (10–12). Experimental animal studies demonstrated similar 99mTc-ciprofloxacin uptake in septic and sterile muscle abscesses in mice and in septic and sterile prosthetic rabbit joints (14–16). We previously showed that 99mTc-ciprofloxacin accumulates in synovial fluid and injured articular cartilage of inflamed aseptic prosthetic rabbit joints and in rabbit growth plates (16). These findings had also been reported using the same animal model with another radiolabeled quinolone, 14C-sparfloxacin (30). Such accumulation of 99mTc-ciprofloxacin may be explained by exudation in the interstitial space, favored by an increased capillary permeability. However, the persistence of increased activity on 24-h images may indicate other, more specific mechanisms for tracer uptake. As for unlabeled ciprofloxacin, specific binding to mammalian DNA-enzyme complexes may occur in inflammatory cells and also in activated chondrocytes, osteoblasts, and fibroblasts (12,15,16,30–36). These mechanisms are thought to explain ciprofloxacin inhibition of experimental fracture healing and toxicologic effects of ciprofloxacin therapy on growth cartilage and on tendons (37–39). They may also explain reported 99mTc-ciprofloxacin accumulation in growth plates, injured articular cartilage, sterile muscle abscesses, aseptic loosened joint replacements with reactive inflammation to metallosis, sterile pseudoarthrosis, and arthrosis (10,14–16).
The low specificity and low positive predictive value of 99mTc-ciprofloxacin scintigraphy are drawbacks in the clinical setting of our study (discrimination between septic and aseptic osteoarticular diseases). However, because 99mTc-ciprofloxacin scintigraphy shows very high sensitivity for infection and a high negative predictive value, greater value is expected of that method than of other scintigraphic methods in other clinical situations, such as axial skeletal infections or infections in leukocytopenic patients.
CONCLUSION
In this prospective study, 99mTc-ciprofloxacin, prepared according to the manufacturer’s recommendations, was very sensitive for the scintigraphic detection of bacterial osteoarticular infections, with a high negative predictive value. But it could not differentiate infections from sterile osteoarticular diseases in symptomatic patients needing surgery. Increased 99mTc-ciprofloxacin activity was observed in sterile pseudoarthrosis, sterile loosened joint replacements with reactive inflammation to metallosis, and arthrosis.
Acknowledgments
This study was supported by a grant from the Direction of Clinical Research of the Assistance Publique-Hôpitaux de Paris.
Footnotes
Received Jul. 1, 2002; revision accepted Oct. 24, 2002.
For correspondence or reprints contact: Dominique Le Guludec, MD, PhD, Service de Médecine Nucléaire, Hôpital Bichat, 46 rue Henri Huchard, 75018 Paris, France.
E-mail: dominique.leguludec{at}bch.ap-hop-paris.fr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exploring molecular imaging to investigate immune checkpoint inhibitor-related toxicity
- Infection Imaging: Focus on New Tracers?
- The Development and Validation of Radiopharmaceuticals Targeting Bacterial Infection
- Nuclear Imaging of Bacterial Infection: The State of the Art and Future Directions
- Molecular Imaging: a Novel Tool To Visualize Pathogenesis of Infections In Situ
- Molecular imaging of bacterial infections: Overcoming the barriers to clinical translation
- Bacterial infection imaging with [18F]fluoropropyl-trimethoprim
- A Systematic Approach for Developing Bacteria-Specific Imaging Tracers
- Imaging Enterobacteriaceae infection in vivo with 18F-fluorodeoxysorbitol positron emission tomography
- Accumulation of 99mTc-Ciprofloxacin in Staphylococcus aureus and Pseudomonas aeruginosa
- Imaging Infection with 18F-FDG-Labeled Leukocyte PET/CT: Initial Experience in 21 Patients
- Synthesis and Comparison of 99mTc-Enrofloxacin and 99mTc-Ciprofloxacin
- Ability of 99mTc-Ciprofloxacin Scintigraphy to Discriminate Between Septic and Sterile Osteoarticular Diseases
- Nuclear Medicine, the Painful Prosthetic Joint, and Orthopedic Infection