


Abstract
Distraction osteogenesis is an effective method for lengthening long bones and filling bone defects that result from bone resection. Insufficiency of bone consolidation in the distraction segment is problematic. In this study, we examined whether 3-phase bone scintigraphy can predict the outcome of distraction osteogenesis. We also investigated the effects of chemotherapy and surgical treatment on distraction osteogenesis. Methods: We performed 3-phase bone scintigraphy on 60 patients (9 high-grade malignant bone tumors as group A, 11 low-grade malignant or benign tumors as group B, 40 nontumoral conditions as group C) with distraction osteogenesis at the lengthening phase of the long bones. By setting the region of interest on the distraction segment and contralateral normal area, we calculated the perfusion index (PI), the uptake ratio of the blood-pool image (BPR), and the uptake ratio of the delayed image (DR). Patients were classified into poor and good consolidation groups from the radiographic findings of the distraction segment. Results: Good to fair correlations were obtained between the PI and BPR, the PI and DR, and the BPR and DR (r = 0.65, 0.45, and 0.57, respectively). The PI and BPR indicated no significant differences among group A-C (1.7 ± 0.6, 2.1 ± 0.7, and 1.8 ± 0.8 in PI, respectively; 1.8 ± 1.1, 1.9 ± 0.5, and 2.0 ± 0.7, in BPR, respectively). The DR of group A (2.4 ± 1.2) was significantly lower than that of group B (6.3 ± 1.8; P = 0.001) and group C (5.9 ± 2.8; P < 0.001). Eleven patients were classified in the poor consolidation group. The other 49 patients showed good consolidation. The poor consolidation group showed lower values in all indices obtained by 3-phase bone scintigraphy than the good consolidation group. The optimal cutoff levels, sensitivity, specificity, and accuracy of each index for detection of patients with poor consolidation were as follows: 1.1, 36%, 90%, and 80% in the PI, respectively; 1.2, 55%, 94%, and 87% in the BPR, respectively; and 2.2, 82%, 96%, and 93% in the DR, respectively. Conclusion: Three-phase bone scintigraphy is a promising method for the assessment of distraction osteogenesis. The delayed image of 3-phase bone scintigraphy, especially, is an excellent modality for predicting the outcome of distraction osteogenesis.
- 99mTc-methylene diphosphonate
- 3-phase bone scintigraphy
- distraction osteogenesis
- external fixation
- chemotherapy
Distraction osteogenesis is an effective method for lengthening long bones and filling the long bone defects resulting from the resection of various bone lesions including bone tumors. Osteogenesis is determined by many factors, including the age of the patient, waiting period, distraction rate, location and method of the osteotomy, soft-tissue condition, local bone blood flow, weight-bearing status, use of antineoplastic agents, and other unknown factors (1,2). Specifically, blood supply is thought to have a close relationship with osteogenesis. The surgical procedure and chemotherapy are also thought to have significant effects on osteogenesis. Delayed or insufficient bone consolidation in the distraction segment is found in 3%-8% of all cases as a complication with distraction osteogenesis (1). Three-phase bone scintigraphy is a noninvasive method to evaluate changes in blood flow, blood distribution, and bone metabolism semiquantitatively (3).
In this study, we examined whether 3-phase bone scintigraphy can predict the outcome of distraction osteogenesis. We also evaluated the effects of the surgical procedure and chemotherapy on distraction osteogenesis.
MATERIALS AND METHODS
Patients
Sixty patients (37 men, 23 women; mean age, 27 ± 19 y) who had undergone distraction osteogenesis were evaluated. The patients were divided into 3 groups according to the nature of their lesions.
Group A.
The first group consisted of 9 patients with high-grade malignant tumors. Seven patients had osteosarcomas and 2 had Ewing sarcomas. All group A patients received chemotherapy before and after surgery. Chemotherapy was performed according to the K2 protocol (4,5). The preoperative chemotherapeutic regimen consisted of 5 courses of intraarterial cisplatin (120 mg/m2 for 1–2 h) and caffeine (1.5 g/m2/d for 3 d continuously) with doxorubicin (30 mg/m2/d for 2 d continuously) at 3-wk intervals. The postoperative regimen consisted of intravenous cisplatin, caffeine with doxorubicin and high-dose methotrexate (8–12 g/m2), along with the citrovorum factor (15 mg, 10 times) and vincristine (1.5 mg/m2), each administered 3 times.
Group B.
The second group consisted of 11 patients with low-grade malignant tumors or aggressive benign tumors. Four patients had giant cell tumors, 2 had low-grade osteosarcomas, 2 had adamantinomas, 1 had chondroblastoma, 1 had low-grade chondrosarcoma, and 1 had fibrous dysplasia. Group B patients were treated without chemotherapy.
Group C.
The third group consisted of 40 patients with nontumoral conditions. Twenty-two patients had leg length discrepancies, 9 had osteomyelitis, 5 had nonunion of fractures, and 4 had open fractures.
Distraction Osteogenesis
Three techniques of distraction osteogenesis were applied to patients according to the status of their lesions: bone transport, shortening distraction, and distraction osteogenesis combined with an intramedullary nail (6). We used an Ilizarov external fixator or a unilateral fixator for bone lengthening.
Group A patients were treated with wide or marginal excision that was based on the chemotherapeutic response. Group B patients were treated with wide or marginal or en block excision according to the pathologic findings of grade of malignancy obtained by open biopsy (7). Group C patients were treated with simple osteotomy in patients with leg length discrepancy or resection of necrotic bone in patients with nonunion or resection of infected bone in patients with osteomyelitis or open fracture (8).
Distraction started after a postoperative waiting period of 5–14 d. Initially, the limbs were lengthened at a rate of 1 mm/d (distraction phase). Callus formation was checked by radiography every 2 wk. If inadequate callus formation was seen, the rate of lengthening was reduced to 0.75 mm/d or 0.5 mm/d. The period from the termination of distraction until removal of the external fixator was defined as the consolidation phase. During this period, consolidation was checked by radiography every 3–4 wk.
Three clinical indices were used to evaluate distraction osteogenesis: (a) the distraction index (d/cm), which was obtained by dividing the duration of the distraction phase by the length of the distraction segment; (b) the maturation index (d/cm), which was obtained by dividing the duration of the consolidation phase by the length of the distraction segment; and (c) the external fixation index (d/cm), which was obtained by dividing the entire duration of external fixation by the length of the distraction segment (6,8).
Clinical Classification of Poor and Good Consolidation Groups
Patients were classified into poor and good consolidation groups. The former was defined as the patients who needed a bone graft from the iliac crest to stimulate osteogenesis because of poor consolidation on radiographs at the end of the consolidation phase. Other patients were classified into the good consolidation group.
Three-Phase Bone Scintigraphy
Three-phase bone scintigraphy was performed in the midphase of the distraction phase (at the time point of 54% ± 18% of the distraction period). Immediately after the bolus injection of 740 MBq 99mTc-methylene diphosphonate (MDP) into the right medial antecubital vein followed by flushing with 20 mL saline, first-pass radionuclide angiographic data were obtained, with 128 × 128 matrices, in the anterior view every 2 s for 2 min. The blood-pool image was obtained at 3 min after injection for 3 min, with 256 × 256 matrices. A delayed image was obtained 4 h later in the same position, with 256 × 256 matrices. Energy discrimination was centered on 140 keV with a 20% window. All data were obtained using a large-field-of-view gamma camera (GCA-901A; Toshiba, Tokyo, Japan) equipped with a low-energy, high-resolution, parallel-hole collimator.
We used a UNIX system (GMS/UI; Toshiba) for data analysis. For semiquantitative analysis, on the blood-pool image and delayed image, we set manually the region of interest (ROI) on the distraction segment and set a symmetric ROI on the contralateral normal area as a control. Radiographs were used as reference (Fig. 1). The uptake ratio of the blood-pool image (BPR) and the uptake ratio of the delayed image (DR) were calculated by dividing the count density of the distraction segment by that of the contralateral normal area in each image.

A 10-y-old boy, with osteosarcoma of left femoral metaphysis, received chemotherapy before and after surgery. He had marginal excision of tumor and bone transport with Ilizarov external fixator. (A) Radiograph shows callus formation in diaphysial distraction segment. (B) Blood-pool image and delayed image show increased activities in distraction segments. Increased activities are also shown in growth plates in both images. ROI was set on distraction segment and symmetric ROI was set on contralateral normal area as control. Uptake ratio of blood-pool image was 1.3, and uptake ratio of delayed image was 4.4.
The perfusion index (PI) was obtained by radionuclide angiography. We set symmetric ROIs on the distraction segment and contralateral normal area to calculate the PI. The time-activity curve of each ROI was generated, and the PI was determined by dividing the peak count of the arterial phase of the distraction segment by that of the contralateral normal area. When a peak count was not obtained, the time-activity curve always showed a shoulder point, which was the turning point between the rapid count increase due to the arterial phase and the steady-state or gradual count increase due to 99mTc-MDP accumulation to the distraction segment and the contralateral normal area. The count of the turning point of the time-activity curve was used to calculate the PI (9,10).
Statistical Analysis
Values are expressed as mean ± SD. The differences of groups were examined using the nonparametric Mann-Whitney U test. The Kruskal-Wallis test was used when appropriate, followed by the Scheffé test for multiple comparisons. The correlation between 2 groups was evaluated by the Pearson correlation coefficient. To appraise the discrimination abilities of the PI, BPR, and DR for the prediction of poor consolidation, receiver operator characteristic (ROC) curves were generated, and the areas under the curves were calculated. The differences between the areas under the 2 ROC curves were examined using the 1-tailed paired t test (11,12). The optimal cutoff levels were identified as each index value minimizing the total number of false results (13). P < 0.05 was considered statistically significant.
RESULTS
Good correlations were obtained between the PI and BPR (r = 0.65; P < 0.001) and between the BPR and DR (r = 0.57; P < 0.001). A fair correlation was obtained between the PI and DR (r = 0.45; P = 0.002).
Comparisons Among Groups A–C
Comparisons among groups A–C in the length of the distraction segment and periods of distraction osteogenesis are summarized in Table 1. In all parameters, group A tended to show larger values than the other 2 groups. However, there were no significant differences among the groups.
Length and Periods of Distraction Osteogenesis: Comparisons Among Groups A–C
Comparisons among groups A–C in each clinical index of distraction osteogenesis are summarized in Table 2. In all parameters, group C tended to show larger values than the other 2 groups. However, these were not statistically significant.
Clinical Indices of Distraction Osteogenesis
The PI and BPR showed no significant differences among groups A–C (1.7 ± 0.6, 2.1 ± 0.7, and 1.8 ± 0.8 in PI, respectively; 1.8 ± 1.1, 1.9 ± 0.5, and 2.0 ± 0.7 in BPR, respectively). The DR of group A (2.4 ± 1.2) was significantly lower than that of group B (6.3 ± 1.8; P = 0.001) and group C (5.9 ± 2.8; P < 0.001). However, the DR did not differ significantly between groups B and C (Fig. 2).
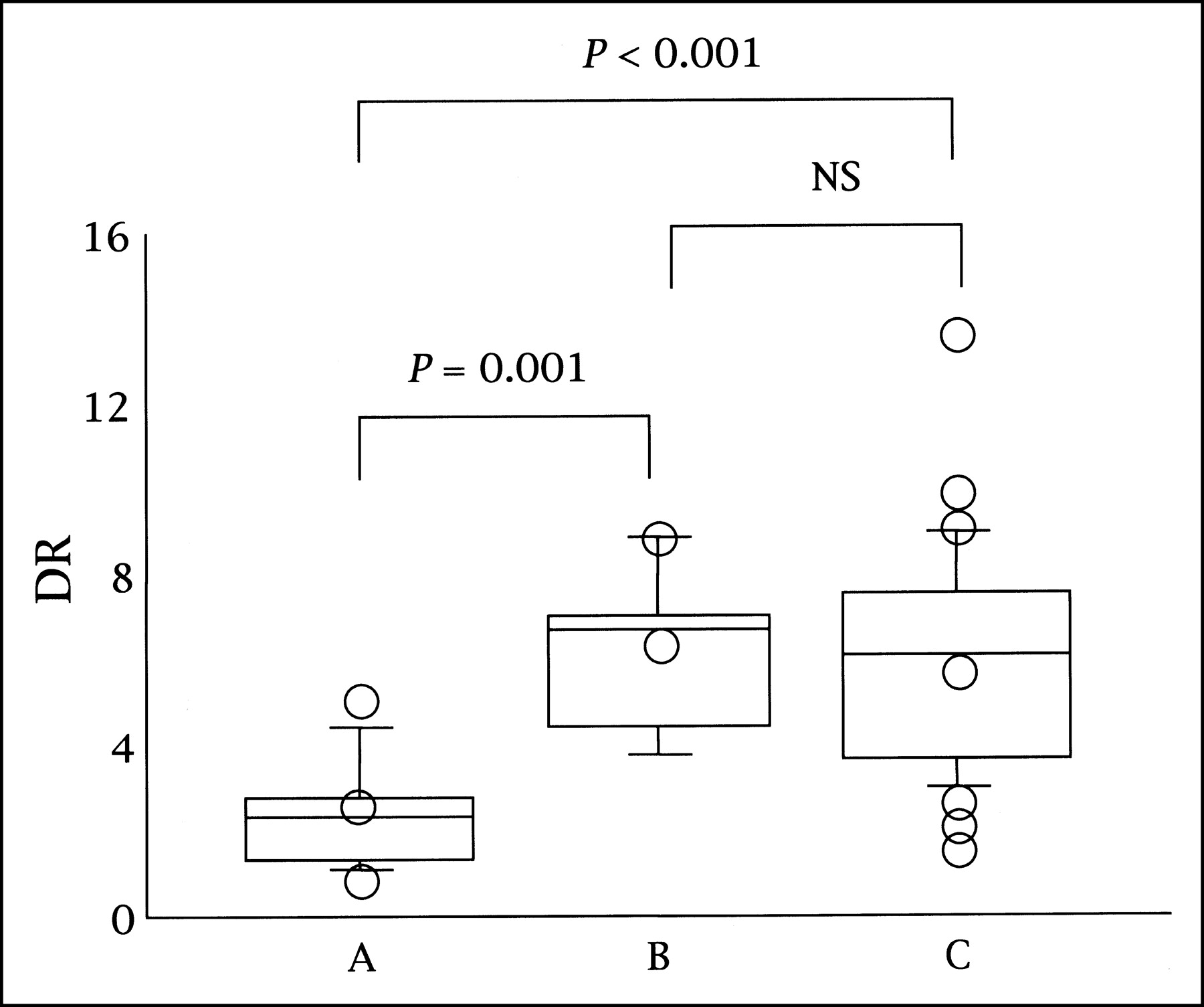
Box plot graphics of DR in groups A–C. Box indicates lower and upper quartiles, and central line and open circle in box are median and mean, respectively. Upper and lower ends of vertical line indicate 90 percentile and 10 percentile, respectively. NS = not statistically significant. DR of group A was significantly lower than that of other 2 groups.
Detection of Poor Consolidation Group
Eleven patients were classified in the poor consolidation group (2 in group A, 5 in group B, and 4 in group C). The other 49 patients showed good consolidation (7 in group A, 6 in group B, and 36 in group C).
Comparisons between the poor and good consolidation groups in the length of the distraction segment and periods of distraction osteogenesis are summarized in Table 3. The poor consolidation group tended to show higher values in all parameters than the good consolidation group. However, these differences between the poor and good consolidation groups were not significant.
Length and Periods of Distraction Osteogenesis: Comparisons Between Poor and Good Consolidation Groups
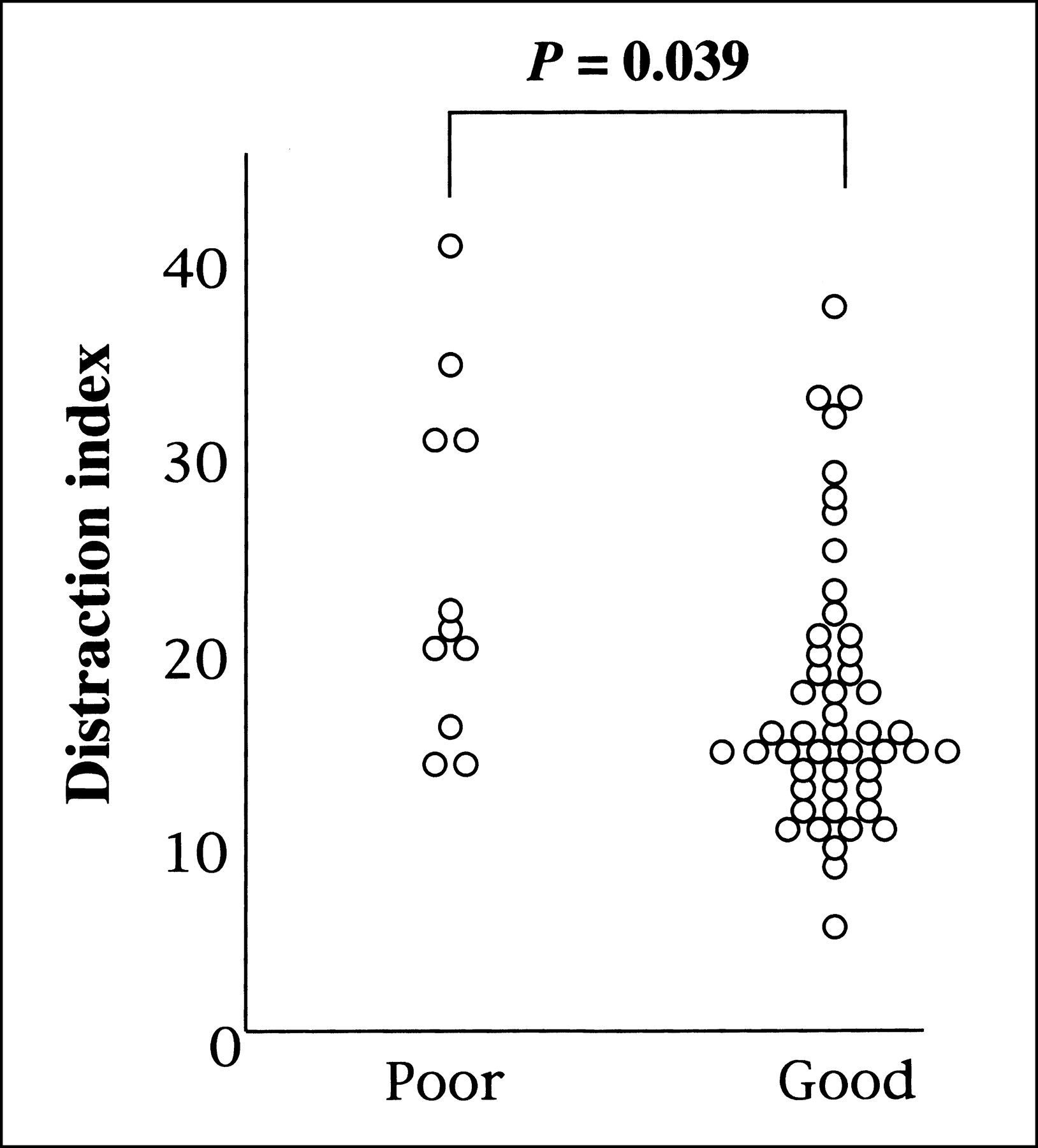
In the poor consolidation group, the maturation index and the external fixation index tended to be larger than those of the good consolidation group. However, there were no significant differences between the poor and good consolidation groups. (44.2 ± 63.8 vs. 31.9 ± 22.2, respectively; and 60.9 ± 64.7 vs. 54.1 ± 19.2, respectively). The distraction index of the poor consolidation group was larger than that of the good consolidation group (22.3 ± 9.7 vs. 16.7 ± 7.4; P = 0.039). However, the distraction index could not distinguish between poor consolidation and good consolidation because of significant overlap of both distraction indices (Fig. 3).
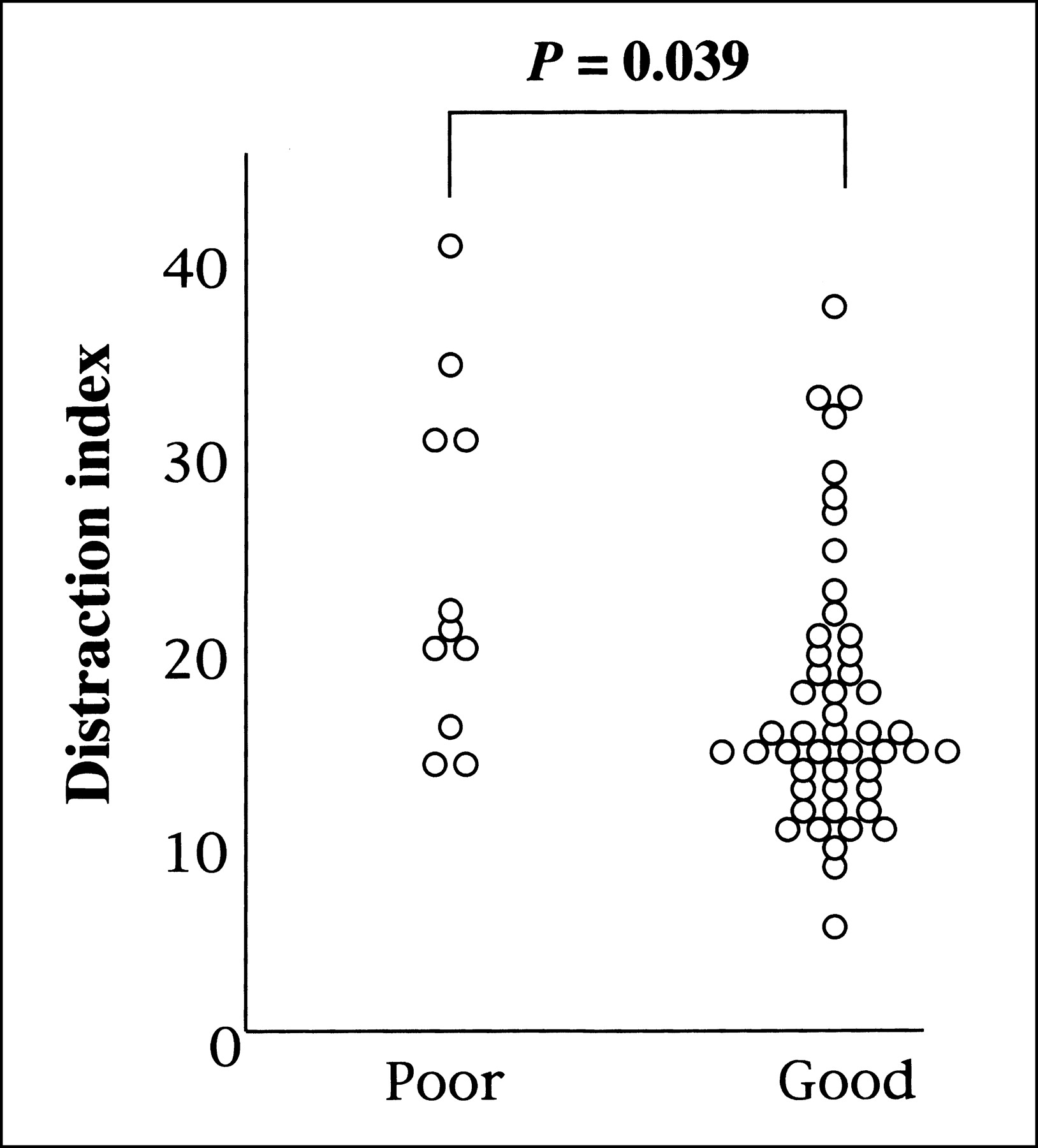
Distraction indices of poor and good consolidation groups. Distraction index of poor consolidation group was significantly larger than that of good consolidation group. However, poor consolidation group was not differentiated from good consolidation group because of significant overlap.
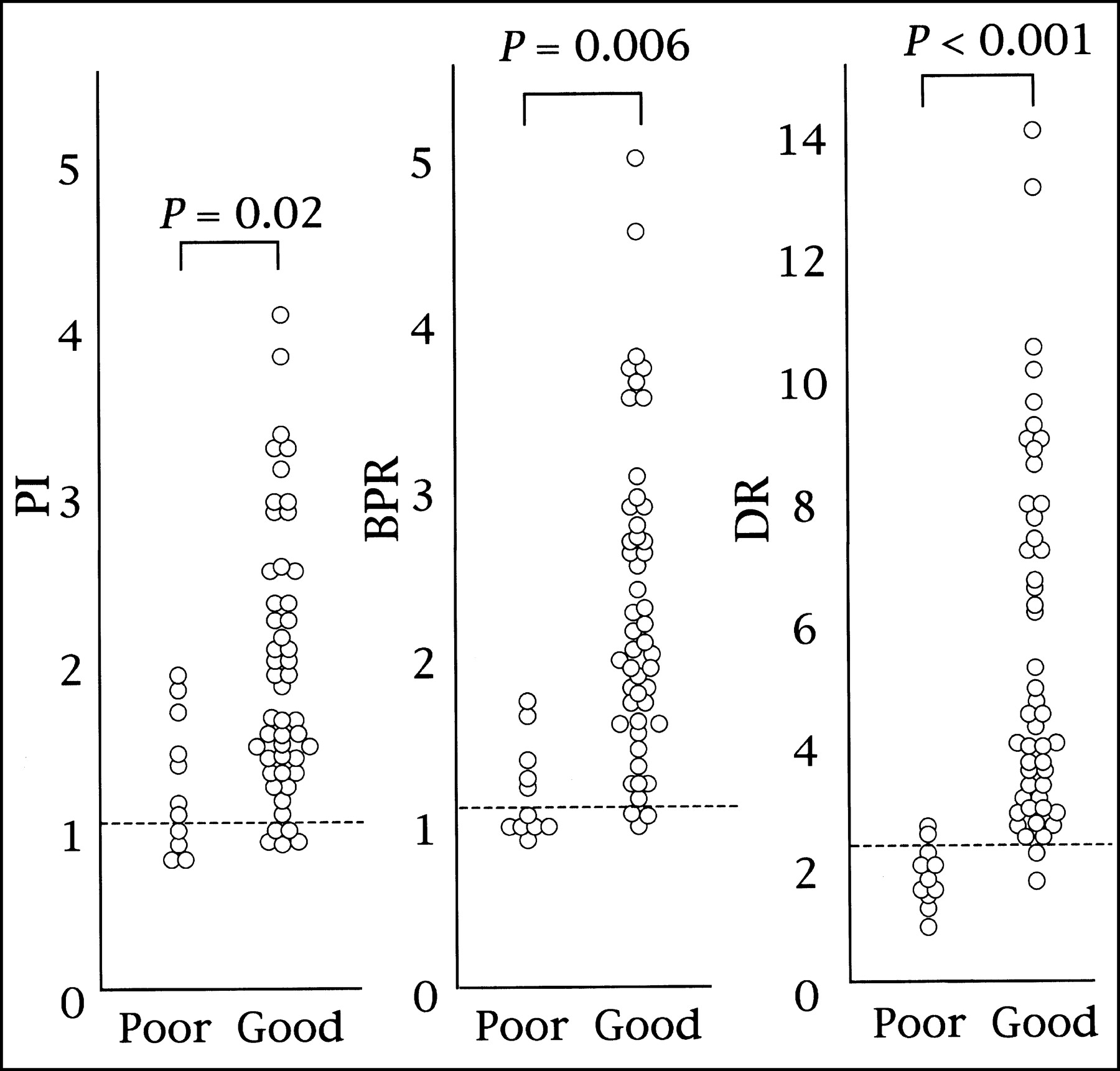
All 3 indices obtained by 3-phase bone scintigraphy in the poor consolidation group were significantly lower than those of the good consolidation group (1.3 ± 0.4 vs. 1.9 ± 0.8, P = 0.02 in the PI, respectively; 1.3 ± 0.3 vs. 2.2 ± 0.9, P = 0.006 in the BPR, respectively; and 1.8 ± 0.5 vs. 5.6 ± 2.9, P < 0.001in the DR, respectively) (Fig. 4).
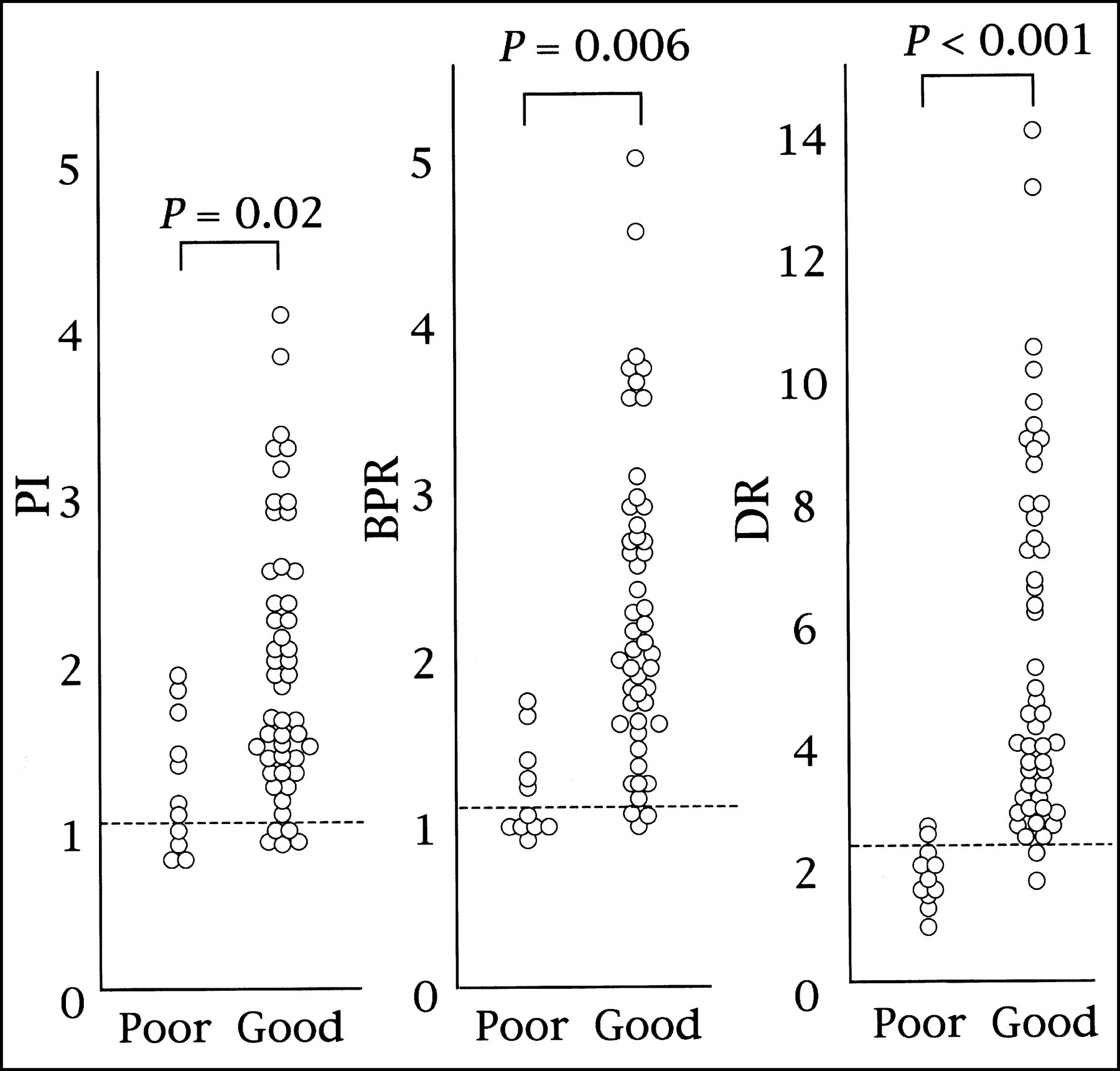
Comparison of poor and good consolidation group in PI, BPR, and DR. Each horizontal dashed line indicates optimal cutoff levels obtained by ROC analysis, which were 1.1 in PI, 1.2 in BPR, and 2.2 in DR.
Figure 5 shows ROC curves of detectability of the poor consolidation group in each index obtained by 3-phase bone scintigraphy. The area under the ROC curve of the DR was larger than that of both the PI and the BPR (P = 0.01 and P = 0.003, respectively). No significant difference was seen in areas under the ROC curves between the PI and the BPR. The optimal cutoff levels obtained by ROC analysis, sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of each index were summarized in Table 4.

ROC curves of detectability of poor consolidation group in PI, BPR, and DR. Area under ROC curve of DR was significantly larger than that of other 2 indices. FPF = false-positive fraction; TPF = true-positive fraction; Az = area under ROC curve.
Detectability of Patients with Poor Consolidation by 3-Phase Bone Scintigraphy
DISCUSSION
This study with 3-phase bone scintigraphy revealed that the delayed image is an excellent modality for predicting the outcome of distraction osteogenesis during the distraction phase. In contrast, none of the clinical indices could predict the outcome.
Angiography of 3-phase bone scintigraphy reflects the regional blood flow of bone (3). The blood-pool image reflects the status of hyperemia. Accumulation of 99mTc-MDP in the delayed image reflects the activity of bone metabolism. Therefore, 3-phase bone scintigraphy is thought to be well suited for the assessment of distraction osteogenesis.
The distraction index, maturation index, and external fixation index were used as clinical indices of distraction osteogenesis. Only the distraction index of the poor consolidation group was larger than that of the good consolidation group, suggesting that callus formation was delayed in the former. But, no clinical indices of distraction osteogenesis could distinguish poor consolidation from good consolidation. In contrast, all indices obtained by 3-phase bone scintigraphy were able to predict poor consolidation. The DR, especially, demonstrated the highest predictability. These results suggest that the indices obtained by 3-phase bone scintigraphy are reliable and accurate indicators of distraction osteogenesis.
Blood supply has been thought to have a close relationship with osteogenesis. Many studies have focused on bone blood flow and detected increased perfusion in the distraction segment, although the relationship between blood flow and osteogenesis remains controversial (3,8,14–18). In this study, the correlation of the PI and DR was not so strong. The PI showed only limited ability in the discrimination of patients with poor consolidation from good ones compared with the DR. These results suggest that blood flow is not linked closely to bone metabolism. The accumulation of the delayed image, which reflects bone metabolism, might be a more important indicator of osteogenesis than bone blood flow because the delayed image showed the highest ability to predict poor consolidation.
Some authors have described the effects of chemotherapeutic agents on osteogenesis, although some controversy persists (19–23). The treatment of high-grade malignant bone tumor usually comprises a combination of both chemotherapy and wide excision. The wide excision causes loss of soft tissue around the distraction segment. However, the effect of wide excision on osteogenesis is unknown. Group B patients were treated with wide excision without chemotherapy, whereas group C patients were treated without loss of soft tissue adjacent to the bone. Between groups B and C, there were no significant differences in the PI, BPR, or DR, suggesting that a loss of soft tissue may not appreciably affect blood flow, blood distribution, and bone metabolism in the distraction segment.
Among groups A–C, no significant differences were seen in the PI or BPR. But, the DR of group A patients who were treated with chemotherapy before and after surgery was significantly lower than that of group B and C patients, who were not subjected to chemotherapy. These results suggest that chemotherapy might not affect blood flow and blood distribution but impairs bone metabolism. In histologic findings, methotrexate has been noted to cause a loss of bone volume, by diminishing new bone formation mainly compared with reduction of bone resorption. Doxorubicin decreased both bone formation and resorption equally, thereby causing little or no alteration in net bone volume despite the diminished rate of turnover (21). The decrease of the DR in group A patients was consistent with these histologic findings.
There are several limitations in this study. The ROIs used for the calculation of the PI and BPR contained not only bone but also overlapping soft tissue. This soft-tissue overlap might mask or overestimate the true status of perfusion and blood-pool activity of the bone because bone occupies a rather small volume compared with soft tissue in the ROIs. However, the counts from overlapping soft tissue were minimal in the delayed image. Accordingly, the delayed image was thought to be less affected by the soft-tissue overlap in calculating bone metabolism. All 3 indices were calculated using the contralateral normal area as a control. Patients with distraction osteogenesis generally have restrictions of exercise not limited to the distraction side extremities but also including the contralateral normal side. Furthermore, patients with high-grade malignant tumors received chemotherapy before and after surgery. Therefore, these patients’ activity was likely restricted for a long time. Hence, some patients in distraction osteogenesis might develop disuse atrophy in the contralateral normal side. Disuse atrophy of the normal side would result in a decrease in blood flow, blood pool, and accumulation in the delayed image. Therefore, overestimation might occur in all indices obtained by 3-phase bone scintigraphy. On the other hand, in patients without contralateral disuse, underestimation of scintigraphic indices might occur. Although there was a possibility of underestimation or overestimation, all 3 indices, especially the DR, were shown to be reliable indicators for predicting the status of osteogenesis.
CONCLUSION
Three-phase bone scintigraphy is a reliable modality to evaluate distraction osteogenesis compared with clinical indices. Three-phase bone scintigraphy performed in the distraction phase could predict the outcome of distraction osteogenesis. The delayed image of 3-phase bone scintigraphy, especially, is an excellent modality for assessing distraction osteogenesis.
Footnotes
Received May 16, 2002; revision accepted Sep. 25, 2002.
For correspondence or reprints contact: Masaya Kawano, MD, Department of Biotracer Medicine, Kanazawa University Graduate School of Medical Sciences, 13-1 Takaramachi, Kanazawa, Ishikawa, Japan 920-8640.
E-mail: mkawano-circ{at}umin.ac.jp
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.