


Abstract
In about half of all patients with Legg-Calvé-Perthes disease (LCP), severe hip disorders that could be prevented by early surgery will develop. A prognostic test for this complication is also needed as part of routine care to help the surgeon manage LCD. The purpose of this study was to confirm the prognostic value of the bone scanning and pinhole imaging of the hip in LCP that Conway’s group proposed in 1997 and to define accurate prognostic scintigraphic patterns. Methods: Fifty-eight patients with LCP were recruited at initial presentation and followed for 1 y. Each patient underwent bone scanning initially and after 5, 8, and 12 mo of disease. The severity of the disease was assessed by radiography (the Catterall classification), MRI, and arthrography. Retrospectively, initial scintigraphic findings were correlated with severity. Results: Among the 60 hips studied (2 patients had bilateral disease), severe hip disorders developed in 36. The positive predictive value of the scintigraphic classification proposed by Conway’s group was 97% for the B pathway (absence of lateral column formation) and 85% for the A pathway (presence of lateral column formation). The hyperactivity of the metaphyseal growth plates was a sign of poor prognosis. The sensitivity was only 33%, but the positive predictive value was 92%. This prognostic information was obtained in as few as 5 mo after initial presentation. Conclusion: This study confirms the high prognostic value of bone scanning in LCP as reported by Conway’s group not only in terms of the accuracy of the classification but also in terms of the short time in which the prognostic information can be obtained. Thus, we propose that bone scanning be used as part of routine care for the management of LCP.
Legg-Calvé-Perthes disease (LCP) is a necrosis of the proximal femoral epiphysis. Multiple studies have demonstrated its vascular origin (1). Its diagnosis is based on clinical and radiographic signs. Structural modification of the femoral epiphysis can be assessed by serial radiographs. In the most severely affected patients, subluxation or severe flattening of the femoral head, associated with late persistent hip disorders, will progressively develop. Early surgery prevents the development of these risk signs, but to be more efficient, surgery has to be performed early, before the appearance of radiographic signs such as subluxation or severe flattening of the femoral head. The prognostic value of the radiographic head-at-risk signs is also limited by the long time before they appear.
Bone scintigraphy has been proven an essential tool for the early diagnosis of LCP (2–12). Conway’s group demonstrated the prognostic value of serial bone scintigraphy and proposed a new scintigraphic classification using 2 pathways (13,14). The A pathway is defined by the early appearance of a lateral column formation (before any radiographic sign) in the capital femoral epiphysis, indicating early and rapid revascularization. This pathway is associated with a good final outcome. The B pathway is defined by centrally extended scintigraphic activity from the base of the capital femoral epiphysis or by the absence of radioactivity in the epiphysis after 5 mo. This pathway is associated with a poorer functional prognosis because of the extent of the initial necrosis and the prolonged interval required for healing (Fig. 1). Finally, this scintigraphic classification is useful for the early detection of necrosis, allowing early treatment and providing prognostic information that may affect therapy. To the best of our knowledge, no confirmation of the work of Conway’s group has been published. Our study was designed to, first, confirm the prognostic value of bone scintigraphy by defining the sensitivity and the specificity of the Conway classification patterns; second, define additive scintigraphic prognostic patterns; and third, define when scintigraphy should be used in the management of LCP.

Scintigraphic stages of Conway classification of LCP. Stage I (total avascularity of proximal femoral epiphysis) is observed at initial stage of disease. Appearance of lateral column formation (a) characterizes A pathway (stages IIA and IIIA). In B pathway, as neovascularization progresses, extension of activity from metaphysis is observed (stages IIB and IIIB), without lateral column formation (b).
MATERIALS AND METHODS
Patients
Fifty-eight patients (10 female, 48 male; mean age ± SD, 6 ± 4 y) were prospectively recruited between March 1997 and June 2001 on initial presentation of LCP, as defined by clinical, radiographic, and scintigraphic signs. All patients were followed up by a pediatric orthopedist with a clinical examination, anterior and frog-leg lateral radiographs, and scintigraphy, initially and after 5, 8, and 12 mo or until surgery. The Catterall classification, which specifies 4 different stages as a function of the extension of the avascular necrosis, was used. As soon as the diagnosis was made, the child was confined to a wheelchair. If there was stiffness of the hip, the patient was placed under traction for 2 or 3 mo. Patients were allowed to walk as soon as radiographic signs of reconstruction appeared. To assess the severity of the disease and to indicate surgery, MRI with or without arthrography was performed when Catterall stage III or IV was observed on the radiographs (15,16). Retrospectively, initial scintigraphic findings were compared with the existence of severity signs observed on the radiographs at the final follow-up by MRI or arthrography.
Scintigraphy
All patients received an intravenous dose of 99mTc-diphophonate (185–259 MBq [5–7 mCi]). Images were captured with a double-head γ-camera (DST; General Electric Medical Systems/SMV America). Early images (blood pool) were acquired 5 min after injection, with low-energy high-resolution parallel-hole collimators, at an acquisition time of 5 min. Late images were acquired 3 h after injection; static images of pelvis, hips, and entire legs were acquired in the same manner as were the early images. Hip images, with the leg in internal rotation, were acquired by a pin-hole collimator, with the femoral epiphysis in the center of the field and the bladder outside the field. The number of counts obtained per image was 150,000, with an identical interval for the opposite hip (13). No sedation was used. To maximize the cooperation of the children, we distracted them by showing them cartoons on television.
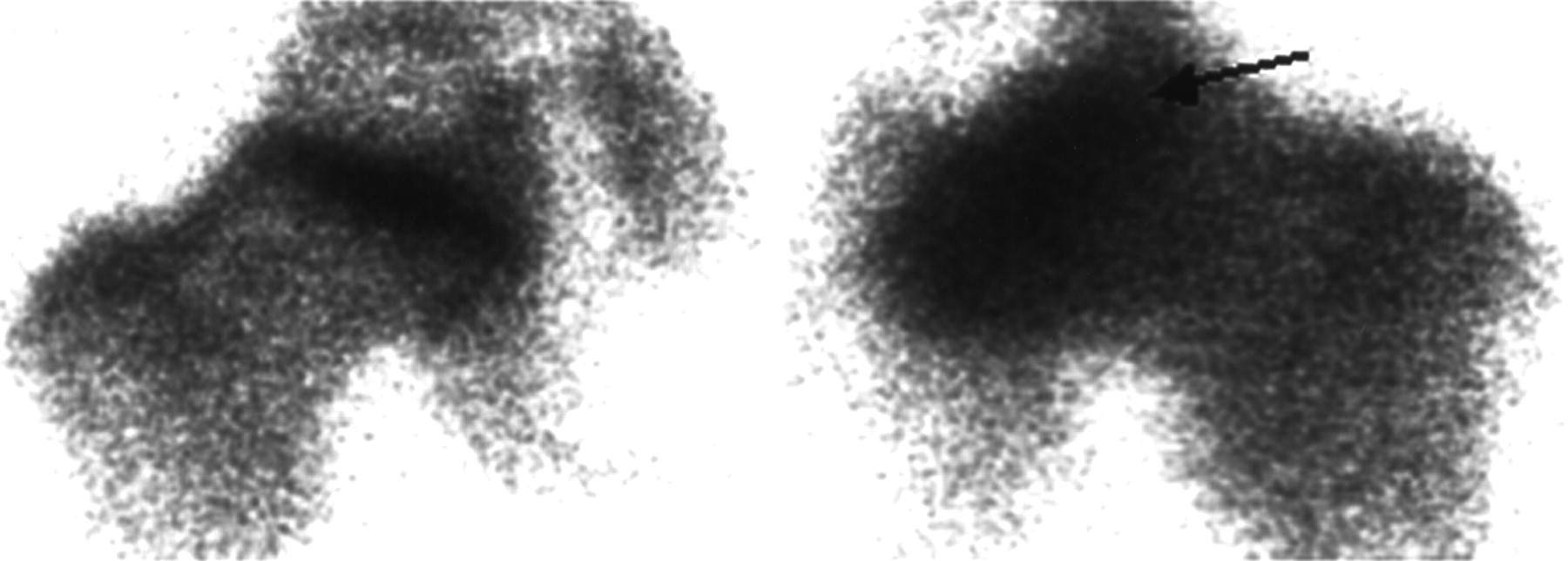
The images were read by 2 nuclear medicine physicians. The method of analysis was visual comparison of the 2 hips. The radioactivity of the proximal femoral epiphysis was analyzed to determine the stage of the Conway classification (Table 1). The degree of hyperactivity of the metaphyseal growth plate was also determined. Examples of the scintigraphic stages of the Conway classification and the hyperactivity of the metaphyseal growth plates are shown in Figures 1 and 2.
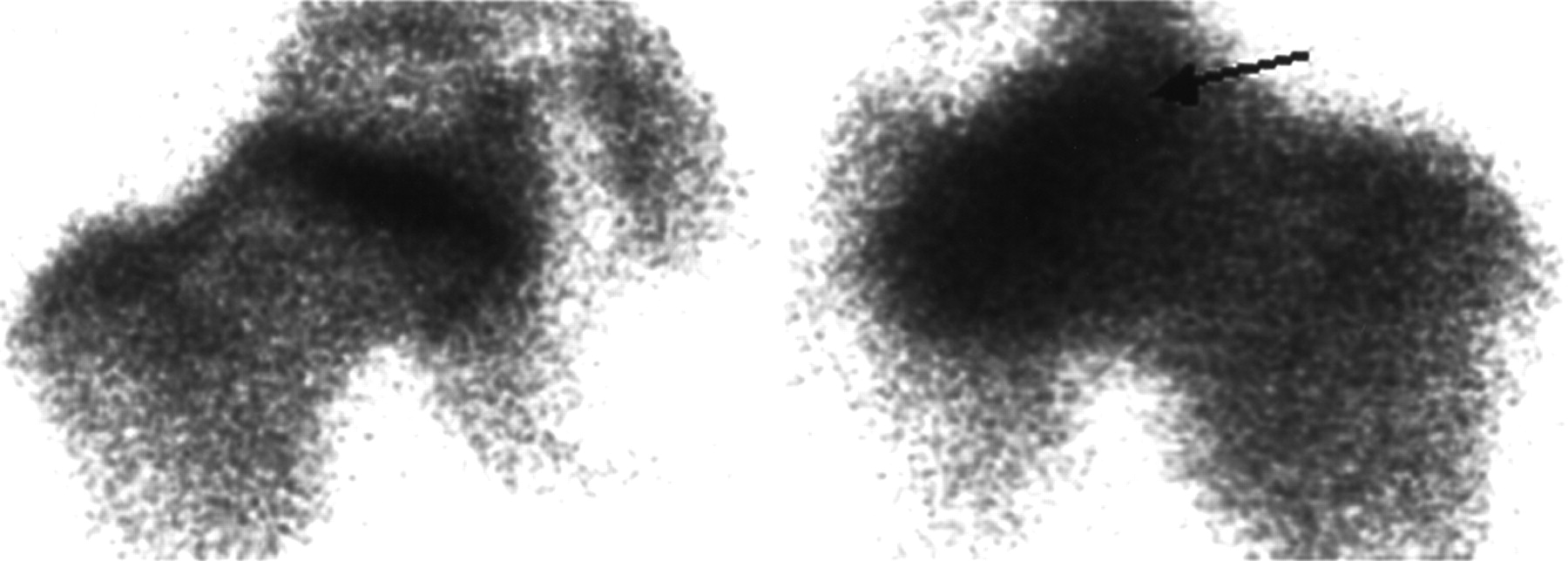
Hyperactivity (arrow) of left metaphyseal growth plates compared with other hip, which appears normal.
Scintigraphic Stages of the Conway Classification
MRI
MRI was performed on a 1.5-tesla unit (Siemens) using a body-array coil. In the coronal and sagittal planes, T1- and T2-weighted turbo spin-echo images (5 mm thick) and fat-saturation sequences were obtained. In the axial planes, T2-weighted images and fat-saturation sequences were also obtained. The field of view was 227 × 260. Images of 5-mm-thick contiguous slices were obtained and displayed on a 280 × 512 matrix.
The MRI signs of severity were assessed by the index of Salles de Gauzy et al. (17), the amount of flattening of the femoral head, and the position of the limbus as described by Milani et al. (18).
Arthrography
Arthrography was performed with the patients under general anesthesia to confirm MRI signs of severity and to provide dynamic information to help the surgeon choose the best surgical strategy. A small quantity of contrast agent was injected into the hip. The position of the needle was followed by a C-arm. When the solution was in the joint, images were taken in different positions: neutral hip position, 35° abduction, abduction and external rotation (Salter position), and adduction. Containment of the femoral head within the acetabulum was assessed by a dynamic hip examination. The severity signs were the extent of the necrosis (extent > 75%), the degree of flattening of the femoral head, and the percentage of subluxation (index of Green et al. > 20% (19)). The classification of Laredo was applied (20).
RESULTS
Sixty hips were studied among the 58 children included in this study; 2 children had bilateral disease. At the fragmentation stage, 16 hips were in Catterall stage I or II, 17 hips were in stage III, and 27 hips were in stage IV. The average time before determination of the Catterall stage was 6.8 mo. Forty-two MRI examinations and 24 arthrographic examinations were performed, and signs of gravity were observed in 36 hips (60%). No signs of severity were observed in 8 of the 17 Catterall stage III patients (47%). Table 2 summarizes the results of radiography, MRI, and arthrography for the patients in Catterall stage III or IV.
MRI and Arthrography Results for Patients in Catterall Stage III or IV
During the first year of follow-up, 122 scintigraphic examinations were performed (mean, 2 per hip). The A pathway, defined by the existence of a lateral column formation in the proximal femoral epiphysis, was observed in 27 hips. For 22 of them, the lateral column formation was observed at the fifth month of evolution. Five patients did not attend the 5-mo scintigraphic control; consequently, for them this formation was observed only at the 8-mo examination. The B pathway was observed in 32 hips. One patient converted from the A pathway to the B pathway (regression pathway, according to Conway’s group) after about 6 mo.
Table 3 shows the correlation between the severity of the disease and the scintigraphic pathway. Concerning the significance of the lateral column formation, seen at the fifth month, we found a 96% sensitivity, 88% specificity, and 85% positive predictive value (PPV) of good final outcome (no radiographic, MRI, or arthrographic signs of severity at the last follow-up). In 4 patients with an A pathway on the initial scintigram, progressively severe hip disorders developed. For these patients, the scintigraphic pilar formation was not seen exactly in the lateral position of the proximal femoral epiphysis and thus could be considered atypical. Considering the significance of the B and regression pathways, we found an 88% sensitivity, 96% specificity, and 97% PPV for a poor final outcome and severe hip disorders. In one patient, the B pathway was observed without a severe hip disorder at the follow-up.
Number of Patients with Good or Poor Final Outcome Depending on Pathway
Among the 60 hips studied, 13 showed hyperactivity of the metaphyseal growth plates on presentation or at the 5-mo control scintigraphy. Progressively severe hip disorders developed in 12. This scintigraphic pattern showed a 33% sensitivity, 96% specificity, and 92% PPV for a poor final outcome.
DISCUSSION
The prognosis of LCP disease is related to the extent of the initial necrosis (21–23). Without specific treatment, severe hip disorders such as arthritis (16,23) and severe osseous destruction will develop later in about half the patients with LCP disease. Several studies showed that surgical containment of the femoral head improves the prognosis of the most severe forms (24–26). Therefore surgery, when indicated, has to be done early, before collapse of the femoral head.
Many radiographic classifications can be used to assess the prognosis of the disease (15,22,26), but the prognostic value of the radiographic signs is limited by the delayed time course in which they appear. To be efficient, the radiographic classifications have to be made at the end of the fragmentation stage, just before the beginning of the reconstruction stage (15), 7–8 mo after initial necrosis. In our study, we used the Catterall classification. The average time before determination of the Catterall classification was 6.8 mo. Given the difficulty of dating the onset of the disease, this average time is also difficult to assess. We found that severe hip disorders developed in only 53% of Catterall stage III patients. To the best of our knowledge, this finding has never been reported before, and further studies are necessary to confirm this observation. The prognostic value of the Catterall classification is limited not only by the necessary delay needed but also by the lack of significance of stage III.
Pinhole imaging of the hip, showing no radioactivity in the proximal femoral epiphysis, has proven to be useful to affirm the diagnosis of LCP on the initial presentation. Moreover, the scintigraphic pinhole classification proposed by Conway’s group could provide early and important prognostic information. This classification was established after only a 5-mo duration of the disease and showed, in our study, a 97% PPV for a poor final outcome for the B pathway (absence of a lateral column formation after 5 mo of disease) and an 85% PPV for good final outcome for the A pathway (presence of a lateral column formation in the fifth month of progression). In 4 hips the A pathway was observed but severe hip disorders appeared progressively. Indeed, when we observed retrospectively the images of these 4 hips, the initial column formation was not strictly in a lateral position and was neither high enough nor large enough to be considered significant; the 5-mo control did not show any scintigraphic change. Any doubt as to the presence of a lateral column formation on the initial scintigraphy should prompt prudence in interpretation and justifies the 5-mo scintigraphic control.
Hyperactivity of the metaphysis is a sign of metabolic changes. This sign provides additional prognostic information: When observed at presentation or after 5 mo, the hyperactivity of the metaphyseal growth plates, as shown in Figure 2, had a high PPV (92%) for a poor final outcome. In contrast, this sign was not sensitive (33%); hyperactivity was not observed initially in all the severe forms. This lack of sensitivity could be explained by the delay needed before the neovascularization process sets in.
In our study, MRI was used to assess the severity of the disease only at the radiologic fragmentation stage. Several authors have reported the prognostic value of MRI when performed at the initial stage (27–30), and others have compared this modality with scintigraphy (31,32). For Uno et al. (31), MRI was superior to bone scanning in detecting the extent of involvement of the capital femoral epiphysis, and Kaniklides et al. (32) showed that the revascularization process was more clearly demonstrated with MRI than with scintigraphy. But in these 2 studies, given that the Conway classification was not used, the scintigraphic analysis could not be considered optimal. Lamer et al. (33), in a recent study based on the Conway classification, showed that MRI using a dynamic gadolinium-enhanced subtraction technique can demonstrate reperfusion patterns and metaphyseal changes similarly to bone scintigraphy. As a consequence and because of the radiation risk of scintigraphy, the authors proposed MRI as a substitute for bone scanning in the assessment of the prognosis of LCP. However, the use of MRI in routine pediatric management is limited by the needed cooperation of the patient. As reported in different studies, MRI frequently requires sedation for children (29,31) and should not be considered a noninvasive modality. Thus, given that these 2 modalities show similar performance in the detection of necrosis and the assessment of prognostic information, both can be used. The use of scintigraphy or MRI should be discussed with regard to risks to the patient (radiation risk for scintigraphy vs. sedation risk for MRI), availability and cost of MRI, and comfort of the children. In our institution, because of the accessibility and relatively low radiation of scintigraphy, it is routinely used in the management of LCP.
Thus, as proposed by Conway’s group (13,14), when the radiograph shows no head-at-risk signs at first presentation, indicative of an early stage of disease, bone scintigraphy is needed at that time to confirm LCP and again after 5 mo to provide prognostic information. The absence of bone uptake on the proximal femoral epiphysis after 5 mo or metaphyseal hyperactivity is highly correlated with severe forms. The existence of a lateral column formation is associated with a good prognosis, but another scan 3 mo later is highly advised to confirm the A pathway.
CONCLUSION
Bone scanning is useful as a clinical tool not only to confirm the diagnosis of LCP but also to obtain prognostic information. The external pilar classification proposed by Conway’s group provides early prognostic information. The hyperactivity of the metaphyseal growth plates, when observed, is an additional sign predictive of a poor final outcome. Considering the ease of performing scintigraphy, its low dosimetry, and its relatively low cost, this modality should be used in routine management of LCP to identify patients with a high risk of a poor final outcome. Two scintigraphic examinations, performed 5 and 8 mo after presentation, could provide accurate prognostic information.
Acknowledgments
The authors thank Dr. Sharon Lynn Salhi for carefully reviewing the manuscript and providing constructive comments.
Footnotes
Received Feb. 21, 2003; revision accepted Jun. 13, 2003.
For correspondence or reprints contact: Frédéric Comte, MD, Service Central de Médecine Nucléaire, CHU Lapeyronie, 191 Avenue Giraud, 34295 Montpellier Cedex 5, France.
E-mail: f-comte{at}chu-montpellier.fr




{kind=link}
{kind=link}