


Abstract
This study examined the degree to which cigar smokers inhale when they smoke cigars. A second objective was to assess the level of association between self-reported inhalation and observable cigar particle deposition in the lung. We hypothesized that cigar smokers with a history of cigarette smoking would show a greater amount of smoke deposition than would cigar smokers with no history of cigarette smoking. We conjectured that self-reported cigar smoke inhalation would be a reliable predictor of observable smoke particle deposition in the lung. Methods: Twenty-four male cigar smokers were recruited to participate in the study. Twelve of the participants were current or past regular cigarette smokers, and the remaining 12 participants had no history of cigarette smoking. The volunteers completed an anonymous questionnaire commenting on the frequency of their current cigarette and cigar use as well as the degree to which they inhale when they smoke cigars. Volunteers smoked a cigar through a holder that permitted cigar smoke to mix with a radioaerosol of 99mTc-labeled sulfur colloid particles. The total radioactivity administered to each volunteer was 100 MBq. Lung ventilation scanning was subsequently performed. Results: Total lung counts showed that volunteers inhaled the cigar smoke to varying degrees, although 100% of nonsmokers and 58% of smokers in the study reported that they never or rarely inhaled when they smoked cigars. With respect to total lung counts, smokers as a group inhaled less than their nonsmoking counterparts; however, this difference reflected a trend in the data and did not reach statistical significance. Conclusion: Contrary to the widely held belief that cigar smokers do not inhale when they smoke cigars, we concluded that cigar smoke is inhaled regardless of self-reported inhalation and smoking history.
Cigar use is increasing in every age group, race, and socioeconomic level and in both sexes (1–4). This trend is mainly the result of increases in occasional cigar smoking by young and middle-aged men of relatively high socioeconomic status; however, cigar smoking is also increasing among teenagers and women (5). The increase in cigar smoking, occurring at a time when cigarette smoking is becoming increasingly socially unacceptable, can be attributed to 2 factors. First, despite the established associations between cigar smoking and cancers of the upper aerodigestive tract (5,6), diseases of the heart and lungs, and chronic obstructive pulmonary disease (5,7,8), cigars are generally perceived as safer than cigarettes (9). Second, cigars are heavily advertised and actively glamorized in the mass media (10).
It is well documented that cigar smoke contains the same toxic and carcinogenic compounds that are found in cigarette smoke (5,2,11). This raises the important question of whether cigar smokers typically inhale when they smoke cigars. To date, studies measuring cigar inhalation have relied either on self-reports or measurements of serum carboxyhemoglobin levels, given that alveolar levels of carbon monoxide and blood levels of carboxyhemoglobin are linearly related. According to our search of MEDLINE (U.S. National Library of Medicine, Bethesda, MD), no studies have specifically examined particle deposition in the lungs during cigar smoking. However, a study did examine regional deposition of smoke particles in the human lung during cigarette smoking (12). The authors recruited 11 habitual cigarette smoker volunteers and compared regional deposition of particles during cigarette smoking with normal tidal breathing. They constructed a cigarette holder that permitted cigarette smoke to mix with an aerosol of 99mTc-labeled sulfur colloid particles drawn from a reservoir bag. The results documented that smoke particles were deposited in the lungs and that all volunteers had a shift toward more apical and central deposition during smoking, compared with their own deposition pattern during tidal ventilation. The authors concluded their report by speculating that the apical predominance of centrilobular emphysema may be in a direct dose-response relationship with the deposition of cigarette smoke particles.
The current study investigated the hypothesis that cigar smokers with a history of cigarette smoking would show a greater level of smoke deposition in the lung than would cigar smokers with no history of cigarette smoking. This difference was predicted in light of the presumed prior experience with inhalation practice that is characteristic of cigarette smokers but not necessarily of cigar smokers. Furthermore, in view of previous research demonstrating the usefulness of self-reported inhalation in assessing the risks of cigarette smoking (13), it was conjectured that self-reported inhalation during cigar smoking would be a predictor of cigar smoke particle deposition in the human lung.
MATERIALS AND METHODS
Twenty-four male volunteers were recruited to participate in the study. All participants had smoked cigars on at least a single occasion in the past. Twelve of the participants were current or past regular cigarette smokers (mean age ± SD, 33.8 ± 5.36 y), and the remaining 12 participants had no history of cigarette smoking (mean age, 32.33 ± 5.12 y). The protocol and consent form were approved by the Human Investigations Committee of Memorial University of Newfoundland.
To establish the cigar-smoking apparatus, an aerosol of 99mTc-sulfur colloid particles was generated into an aerosol bag. This was the same material that is used in a standard ventilation and perfusion lung scan series. The total administered activity for each participant was approximately 100 MBq.
Using a method similar to that of Pearson et al. (12), a cigar holder was devised allowing smoke drawn from a standard-sized cigar to mix with the 99mTc-sulfur colloid aerosol particles along a plastic tube. In this manner, the colloid was a reliable indicator of regional aeration with the likelihood that the smoke particles followed aeration. A mouthpiece was designed to allow the mixed aerosol and smoke to be inhaled by each participant. The distance between the mouthpiece and the cigar was adjusted so that, although the cigar smoke was diluted, its flow characteristics were similar to those of the smoke from a standard cigar. A 1-way valve was attached to the apparatus to prevent bidirectional aerosol flow. Thus, the air flow in excess of the subject’s inhaled volume was contained within the system, with the aerosol nebulizer remaining on during the subject’s session.
Protocol
Informed consent was obtained from the volunteers before they participated in the study. They completed a 1-page anonymous, number-coded questionnaire. The questionnaire classified individuals into 1 of 2 groups: those having a prior or current history of cigarette smoking and those having no smoking history. All volunteers were asked to indicate whether they inhale when they smoke cigars (i.e., never, rarely, sometimes, usually, or always).
The volunteers were then seated comfortably next to a fume hood and instructed to smoke a cigar through the smoking apparatus in their normal fashion in their own time, and to exhale into the fume hood to ensure that exhaled particles would be safely eliminated. Initially, volunteers were asked to smoke the cigar in their usual way for approximately 1 min without the apparatus to ensure that the cigar was well lit. Then, to allow the volunteers an opportunity to get used to the apparatus, they were instructed to smoke the cigar through the smoking apparatus for another minute before the aerosol was turned on. The aerosol was then turned on for 2 min, and the volunteers smoked during this period.
Using a SPECT gamma camera (Orbiter; Siemens Gammasonics, Inc., Des Plaines, IL), imaging was performed immediately afterward while the volunteers were seated. Posterior views were taken and stored for subsequent analysis. Each lung was divided into 3 zones—upper (apical), middle, and lower (basal)—and the total number of radioactive counts was determined for each zone.
Statistical Analysis
Total lung counts for cigarette smokers and nonsmokers were compared using an independent-samples t test. To facilitate analysis, the participants’ self-report about their cigar inhalation tendencies was coded as 1 (rarely or never), 2 (sometimes), or 3 (usually or always). The association between self-reports of cigar inhalation and total lung counts was analyzed using the Kruskal-Wallis test for χ2 analysis for a nonparametric ANOVA.
RESULTS
Uptake Studies
The results of the total lung counts showed that all volunteers inhaled the cigar smoke to varying degrees. The range of total lung counts for all participants was 457 to 24,454. Figures 1 and 2 depict actual lung scans of volunteers who had relatively high and low lung counts, respectively. The mean and SD values for total lung and lung zone counts of the cigarette smokers and nonsmokers are detailed in Table 1. With respect to total lung counts, smokers as a group inhaled less (mean, 6,375.3; SD, 8,466.1) then did their nonsmoking counterparts (mean, 7,737.4; SD, 6,706.6); however, although reflecting a trend in the data, this difference did not reach statistical significance.
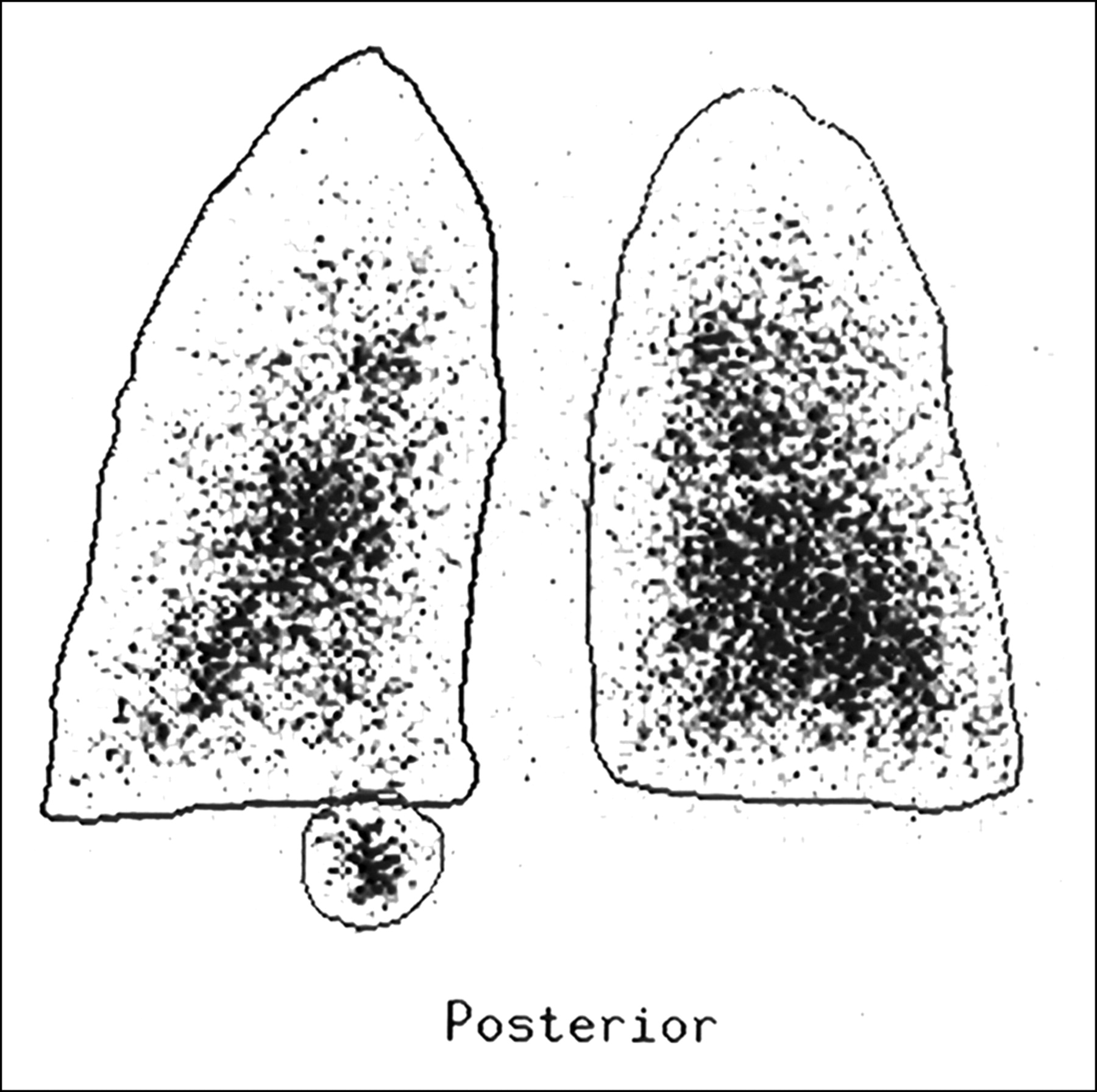
Lung scan depicting high total lung count.

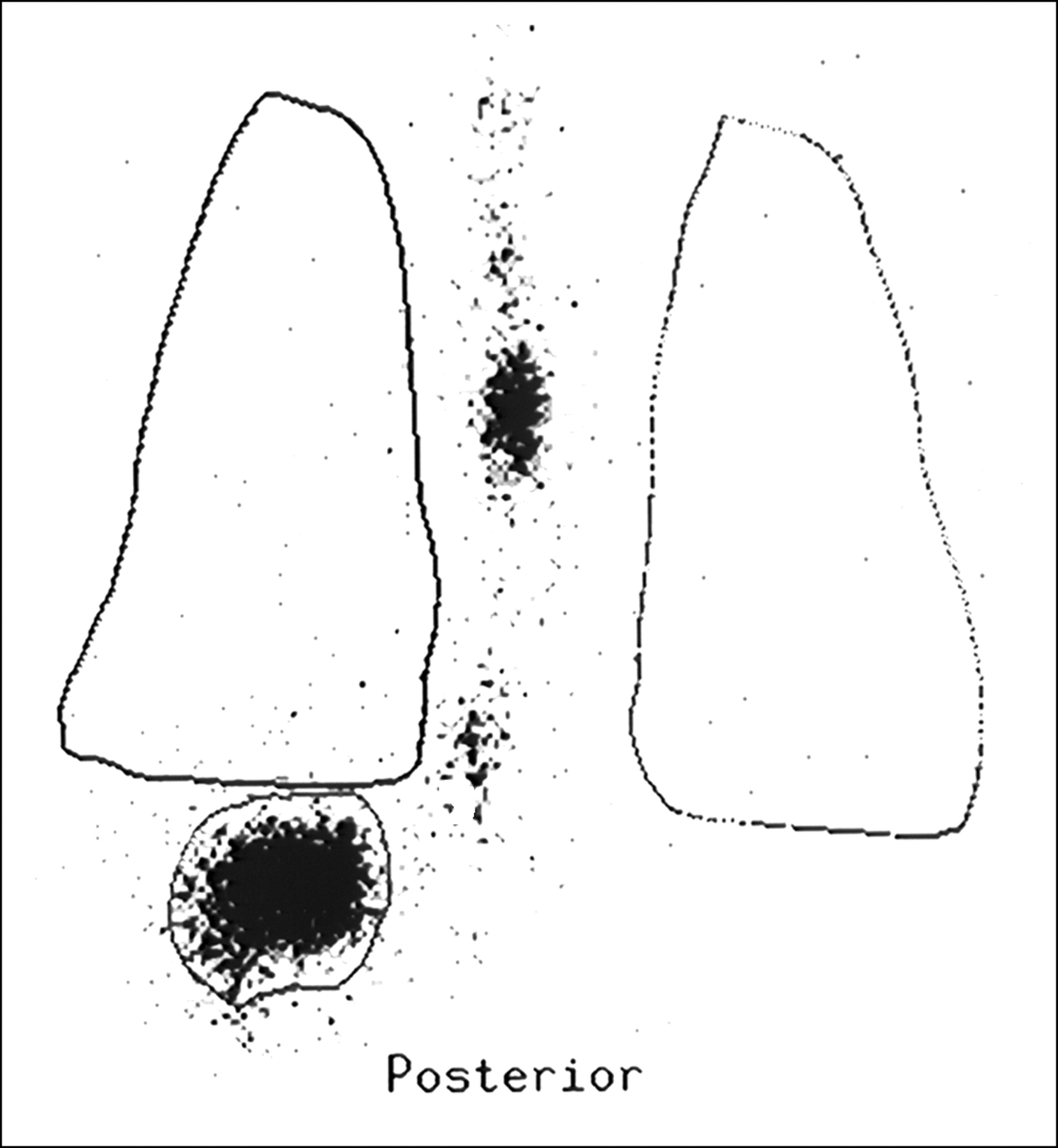
Lung scan depicting low total lung count.
Mean and SD of Zone and Total Lung Counts for Cigarette Smokers and Nonsmokers
There were no significant differences between groups of smokers and nonsmokers in either total apical (upper) or basal (lower) deposition counts. Apex-to-base ratios were also calculated for each volunteer’s lung scan, similar to the calculation used by Pearson et al. (12). No significant differences in apex-to-base ratios between groups were found using t test analysis.
Each volunteer’s overall lung deposition pattern was analyzed and classified into 1 of 3 categories of distribution: diffuse, central, or mixed (i.e., a combination of diffuse and central). Nine smokers and 10 nonsmokers showed a diffuse pattern. Only 1 smoker had a central pattern, and none of the nonsmokers showed a central pattern. Two smokers and 2 nonsmokers showed a mixed pattern. An interesting observation was that only 1 volunteer in the entire sample showed a central pattern of deposition; this same volunteer also demonstrated the highest total lung count overall.
Self-Report Studies
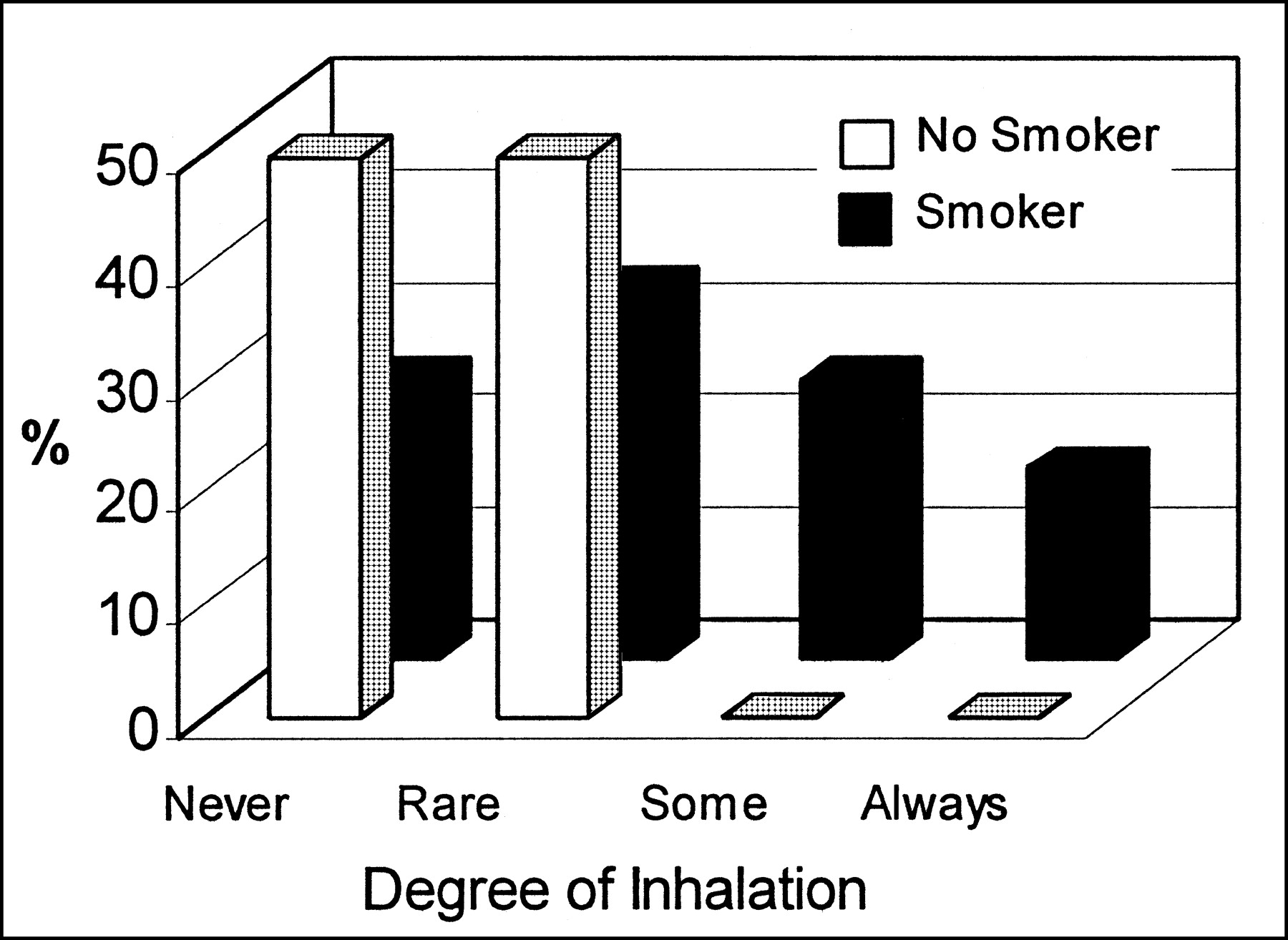
Self-reports of inhalation practices are displayed in Figure 3. The results of χ2 analyses using the Kruskal-Wallis test for a nonparametric ANOVA showed no association between degree of self-reported inhalation and total smoke deposition in the lung (χ22 = 2.71). Although the results clearly showed that every volunteer inhaled the cigar smoke to some degree, 79% of the total volunteer population reported that they did not believe they were inhaling when they smoked cigars. This trend was reflected well in the data of the nonsmokers: 50% of nonsmokers reported that they never inhale cigar smoke, and 50% reported that they rarely inhale cigar smoke. Despite their belief that they were not inhaling, the total lung counts in this group ranged from 507 to 21,527. Similarly, 58% of volunteers in the smoking group reported that they rarely or never inhale cigar smoke. An exception to this finding occurred in the cigarette-smoking group, in which the 3 highest lung counts were recorded for volunteers who acknowledged that they sometimes or usually inhale cigar smoke.

Degree of self-reported cigar inhalation for all subjects.
An interesting yet unexpected finding was that the lung scans of every volunteer showed variable amounts of uptake in the region of the stomach. This occurred regardless of their total lung counts, as the correlation between total lung count and total stomach uptake did not show a significant relationship (r = 0.23). Figure 4 displays a lung scan of a volunteer who had relatively high counts in the upper digestive tract. Another interesting finding was that 2 volunteers in the smoking group reported that they never inhaled cigar smoke; these same individuals showed up to 2 times more stomach counts than total lung counts.

Lung scan depicting uptake in digestive tract.
DISCUSSION
This study directly examined particle deposition in the human lung during cigar smoking. Contrary to the widely held belief that cigar smokers do not inhale when they smoke cigars, the results of the present study showed that all volunteers who smoked a cigar inhaled the smoke to some degree, whether or not they intended to do so. This lack of association is reflected in Table 2, which depicts the mean and SD values of total lung counts grouped according to degree of self-reported inhalation (i.e., never/rarely, sometimes, or usually/always). This finding is of concern, given our knowledge of the toxic and carcinogenic ingredients of cigar smoke.
Mean and SD of Total Lung Counts According to Degree of Self-Reported Inhalation
Past studies of cigar inhalation have used measures of self-report or serum levels of carboxyhemoglobin (13–15). Collectively, the results of these studies reflect 2 trends. Specifically, cigar smokers with a history of cigarette smoking tend to inhale significantly more cigar smoke than do cigar smokers with no smoking history, as reflected by their relatively higher serum carboxyhemoglobin concentrations (14). Moreover, self-reported cigar smoke inhalation has been shown to predict carbon monoxide levels in expired air more accurately than does cigarette smoking history (13).
In contrast to these earlier findings, none of the nonsmokers in the present study endorsed our determination that they inhaled cigar smoke, yet a trend existed in the data showing that, as a group, they had higher total lung counts overall than did the cigarette-smoking group. This trend in the results did not support our hypothesis that cigar smokers with no history of cigarette smoking would inhale less than would cigar smokers with a history of cigarette smoking. It is possible that cigar smokers with no cigarette-smoking history were relatively inexperienced in their smoking behavior, such that they could not regulate their smoke inhalation as well as experienced cigarette smokers could.
Overall, 79% of participants reported that they never or rarely inhale smoke when they smoke cigars, yet everyone inhaled the cigar smoke to some degree. Thus, contrary to our hypothesis, self-reported inhalation during cigar smoking was not a reliable indicator of cigar smoke particle deposition in the human lung. These data raise concern about the public perception that cigar smoking is safe in the context of the belief that cigar smokers do not tend to inhale cigar smoke. Our data showed that cigar smokers do inhale cigar smoke and remain generally unaware that they are doing so.
A serendipitous finding to emerge in the data was that the lung scans of every volunteer showed uptake in the region of the stomach. It is likely that the colloid aerosol was combined with smoke particles and then mixed with saliva in the mouth and was subsequently swallowed, leading to variable degrees of uptake in the stomach. This finding is relevant in light of growing evidence of a relationship between cancer development in the aerodigestive tract and cigar smoking (5,6). It is possible that some portion of cigar smoke particles is digested as the particles mix with saliva from the mouth, and this may be related to the future development of cancers in the digestive system.
Small sample size was the major limitation of this study. Although larger than comparison studies, the sample size was relatively small, leading to difficulty in interpreting trends in the data such as the greater number of lung counts in the nonsmoking group compared with the smoking group. It would be useful to replicate the study with a larger sample size to further explore this trend in our data.
CONCLUSION
In summary, our results clearly showed that all cigar smokers inhaled cigar smoke to some degree, and they tended to be unaware that they were doing so. Prior experience with smoking cigarettes did not seem to significantly influence the amount of cigar smoke inhalation, although nonsmokers tended to inhale a little more cigar smoke than did cigarette smokers. Given the toxic and carcinogenic potential of cigars, as well as a public perception that cigar smoking is relatively safer than cigarette smoking, our results point to the reality that cigar smoking is becoming an increasing public health concern.
Acknowledgments
The authors thank Tim Hatfield, Brent Oram, and Clayton Kennedy (Department of Nuclear Medicine, Memorial University of Newfoundland) for their development of the study apparatus and their skillful assistance in the implementation of the study protocol. The authors also thank Dr. Veeresh G. Gadag (Department of Community Medicine, Memorial University of Newfoundland) for his contributions to the statistical analysis of the data. This study was performed in and supported in part by the Department of Nuclear Medicine, Memorial University of Newfoundland. Additional support was provided by the Department of Radiology, Memorial University of Newfoundland.
Footnotes
Received Feb. 5, 2002; revision accepted Jul. 31, 2002.
For correspondence contact: Lori J. McDonald, MD, 329 LeMarchant Rd., St. John’s, Newfoundland, A1E 1R1 Canada.
E-mail: h54ljm{at}morgan.ucs.mun.ca




{kind=link}
{kind=link}
{kind=link}
{kind=link}