


Abstract
In squamous cell carcinoma of the head and neck, staging of the neck cannot rule out occult metastatic disease. An improved staging is necessary to avoid elective neck dissection in patients staged as N0. The study was performed to determine the feasibility of the detection of occult metastatic disease by ultrasound-guided fine-needle aspiration cytology (USgFNAC) of sentinel lymph nodes (SLN). Methods: Sixteen consecutive patients diagnosed with oral, oropharyngeal, or dermal squamous cell carcinoma who had been staged as N0 underwent lymphoscintigraphy in double tracer technique to localize SLNs. A USgFNAC was performed on SLNs before elective neck dissection. The results of USgFNAC were compared with pathohistologic findings, which were regarded as the gold standard. Results: Seven of 16 patients were upstaged to N+ after histopathologic examination of the neck dissection specimen. In only 1 of these patients was metastatic disease detected by USgFNAC of the SLN. Conclusion: The combination of lymphoscintigraphy and USgFNAC of the SLN improves preselection of N+ patients and, thus, the staging procedures. However, based on present results this method does not seem reliable in deciding whether an elective neck dissection can be avoided. A biopsy of the SLN with close histopathologic work-up seems to be mandatory for the detection of occult metastatic disease, because the merely incidental aspiration of micrometastatic material within normal-sized lymph nodes results in a high number of false-negative results by USgFNAC.
Detection of lymphatic metastases of malignant tumors of the head and neck is pivotal for the management of the neck. Evidence of metastatic disease results in neck dissection and, in most cases, postoperative radiotherapy of the neck. However, lack of evidence of metastatic disease does not rule out occult metastatic disease. Therefore, elective neck dissection has been proposed as a staging procedure with a therapeutic aspect in patients with occult metastatic disease. Patients with occult metastases benefit from this strategy. Yet, the majority of patients will suffer from the morbidity of a neck dissection without gaining advantages, because the preoperative diagnosis of an N0-neck will be confirmed. Therefore, improved staging of the neck is necessary to differentiate patients with occult metastatic disease from those who do not need treatment of the neck.
Ultrasound-guided fine-needle aspiration cytology (USgFNAC) has been shown to improve staging of the neck (1). A USgFNAC is performed on lymph nodes that suggest malignancy on ultrasound examination. Ultrasonographic criteria for suspected malignancy are size > 8 mm in diameter for subdigastric nodes and > 7 mm for all other nodes (2). However, these criteria do not work if metastatic disease has not yet resulted in an enlargement of the lymph node. Therefore, a lymph node with a small volume of metastatic cells may be missed by ultrasound, CT, MRI, and PET. Small lymph node metastases are detectable by PET in those instances in which tracer uptake is relatively high compared with the background activity, as with highly metabolic active tumor cells. On the other hand, lymphoscintigraphy visualizes the sentinel lymph node (SLN), thus identifying the lymph node most likely to contain metastatic disease (3). An SLN biopsy, however, is not yet a standard part of the clinical routine and may result in scarring, making subsequent neck dissection more difficult. A combination of the advantages of lymphoscintigraphy in visualizing the SLN and USgFNAC of the SLN may improve staging by detecting occult metastastic disease and offer the possibility of a more well-founded decision in favor of or against elective neck dissection. We addressed the question of whether a combination of USgFNAC of SLNs visualized by lymphoscintigraphy is able to detect occult metastatic disease.
MATERIALS AND METHODS
The SLN was assessed in 16 patients with squamous cell carcinomas of the head between August 1997 and December 1999. Primary tumors were located in the oropharynx (n = 6), floor of the mouth (n = 4), mobile tongue (n = 3), lip (n = 2), or ear (n = 1). T-status is listed in Table 1. Staging of the neck was performed by ultrasound only using a 7.5-MHz linear array transducer (SONOLINE Versa Pro; Siemens, Erlangen, Germany). All patients were staged as N0. Staging was performed according to the guidelines of the Union Internationale Contre le Cancer (4).
Patient Characteristics and Staging
Lymphoscintigraphy was performed using a double-tracer technique before the treatment of the primary tumor (5). One hundred MBq 99mTc-colloid (Nanocoll; Solco, Basel, Switzerland) dissolved in 0.1–0.2 mL were injected into 3–4 peritumoral sites. Particle size was <80 nm in diameter. Next, 2 mL perchlorate solution (Irenat; Bayer, Leverkusen, Germany) were administered orally to block the thyroid and salivary glands. In a third step, 50 MBq 99mTc-pertechnetate were injected intravenously 20 min later for body contouring. Planar images were acquired using a large-field-of-view gamma camera equipped with a LEAP-collimator (Gammadiagnost Tomo; Philips, Hamburg, Germany). The sequence for the first 10 min was 30 s per frame from a frontal, left, or right lateral view. From 10–30 min and 4 h after injection, the sequence was 5 min per frame from all 3 directions. Lymphatic drainage was assessed by visual inspection. Lymph nodes accumulating tracer were assigned to compartments I–VI of the neck, as designated by the Committee for Head and Neck Surgery and Oncology of the American Academy of Otolaryngology—Head and Neck Surgery (6).
The first lymph node in a patient to accumulate tracer was regarded as the SLN. In case of several ipsi- or contralateral lymph nodes accumulating tracer simultaneously, all were regarded as SLNs.
All SLNs were subjected to USgFNAC after they had been localized by lymphoscintigraphy and ultrasound. A 40 × 0.9 mm needle attached to a 20-mL syringe in a syringe holder was introduced into the skin on the lateral side of the transducer. The point of the needle was guided into the SLN under ultrasound control. Once the tip of the needle was visualized inside the node, multiple passages were performed on each SLN without withdrawing the needle from the lymph node. The aspirate was dispersed on a slide and fixed in 100% isopropyl alcohol. After staining with hematoxylin-eosin, the slides were examined under the microscope.
After completion of the staging, the tumor was excised. A bilateral neck dissection was performed on 5 patients and an ipsilateral neck dissection on 11 patients (Table 1). For histologic examination, the neck dissection specimens were fixed in formalin. All lymph nodes palpated or found after specimen sectioning were examined microscopically in the Department of Pathology. The lymph nodes were embedded in paraffin. One 3- to 5-μm section was prepared from every paraffin block and stained with hematoxylin-eosin.
Metastases detected in the neck dissection specimens were analyzed according to the compartments of the neck. Cytologic results of the SLNs and the histopathologic findings of the neck dissection specimens were compared.
RESULTS
In 14 of 16 patients, a lymphatic drainage of the tracer into the cervical lymph nodes could be visualized. Two patients did not exhibit lymphatic drainage of the tracer.
In patients with lymphatic drainage, 29 lymph nodes accumulated tracer within 4 h after peritumoral injection. Of these, 17 ipsilateral and 4 contralateral nodes were identified as SLNs (Table 2). In 9 of 21 SLNs, it was difficult to differentiate the sentinel node from other lymph nodes in close proximity in the ultrasound examination.
Characteristics of Sentinel Lymph Nodes and Results*
USgFNAC was unsuccessful in 3 lymph nodes. One of these lymph nodes measured only 3 × 4 × 3 mm and was too small to be punctured. In 2 cases, a cytologic diagnosis was not possible, because the material aspirated was insufficient. The sizes of these lymph nodes were 9 × 10 × 7 mm and 7 × 4 × 20 mm, respectively. Eighteen lymph nodes were punctured successfully under ultrasound guidance (Table 2).
Based on histopathology of the neck dissection specimens, 9 patients were staged as N0. Two of these patients did not exhibit lymphatic drainage. In the remaining 7 patients, 9 SLNs were detected. No cytologic signs of malignancy were found in 8 of the sentinel nodes (Table 2). In one instance, a cytologic diagnosis was not possible because of insufficient material.
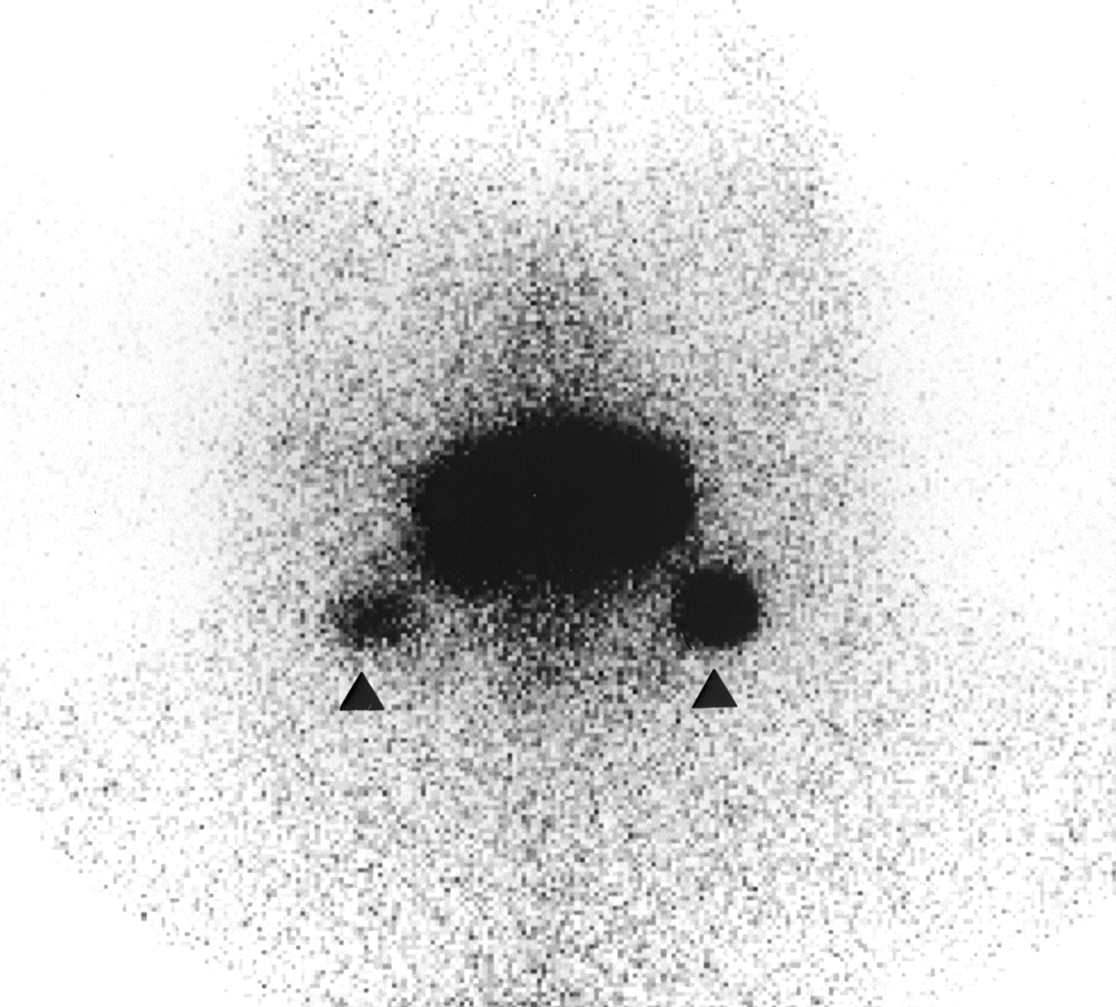
Seven patients were found to have occult metastatic disease in 12 ipsilateral lymph nodes in the neck dissection specimens. Three of the metastases were micrometastases. No contralateral metastases were found. In these 7 patients with occult metastatic disease, 9 ipsilateral and 3 contralateral SLNs were detected during lymphoscintigraphy. In 2 of 7 patients, the levels of the SLNs and additional metastases were not identical. USgFNAC was unsuccessful in 2 of 12 SLNs. In 1 case, the SLN was too small to be punctured. In the other, the material aspirated was insufficient. In 9 cases, no malignant material was found by cytologic examination. In 1 case, a metastasis was detected in an SLN by cytology in a patient with a carcinoma of the lip with bilateral SLNs (Fig. 1). Histopathologic examination showed this to be a micrometastasis (Table 2).

Lymphoscintigraphy of patient with bilateral SLNs (▴) in level I from ventral view 30 min after peritumoral injection of 99mTc-nanocoll pertechnetate.
DISCUSSION
In the staging of squamous cell carcinoma of the head and neck, considerable attention is focused on the neck. Standard staging procedures include ultrasound, CT, and MRI. The success of these morphologic methods depends on increased size or structural changes in the lymph node as a symptom of metastatic disease (7). With PET as a functional diagnostic tool, metastases of <5 mm are difficult to detect (8). However, because in PET tumor-to-background ratios also play an important role, smaller metastases are detectable in instances of highly increased glucose metabolism. Chronic inflammation in pharyngeal lymphatic tissue, on the other hand, might be responsible for raising the nontumor background signal, thus making it difficult to identify small tumors, for example, in the tonsils. Therefore, small metastases may not be visualized by any of these imaging procedures. Consequently, even when no metastases are evident, occult metastatic disease may be present. As a solution to this dilemma, elective neck dissection is performed in many institutions if the risk of metastatic disease exceeds 15%–20%. It is applied as a staging procedure, and in lymphatic metastases usually results in additional irradiation of the neck. However, the majority of patients without neck disease suffer from considerable morbidity from neck dissection as a staging procedure, with no therapeutic benefit (9).
A more precise staging may obviate the need for elective surgery of the neck. Ultrasound staging of the neck has been improved with the performance of USgFNAC on lymph nodes suggestive of metastatic disease (1). Yet, even in the unsuggestive neck, several lymph nodes may be detected that harbor occult metastatic disease. The decision as to which lymph node should undergo USgFNAC is difficult and is based on the size of the lymph nodes and the likelihood of metastatic pathways (1). However, empiric metastatic pathways are not reliable, as skip metastases and aberrant lymphatic drainage of the tumors occur, for example, in 15.8% of carcinomas of the oral tongue (10). Therefore, reactively enlarged lymph nodes may be examined, whereas normal-size lymph nodes containing tumor cells may not be recognized as such (11). In this context, lymphoscintigraphy may be of great benefit, because it does not depend on the size of a lymph node but rather reveals the lymphatic drainage of a tumor into specific lymph nodes, indicating nodes with the highest risk of metastatic disease (3). In melanomas and breast cancer, the SLN seems to be of prognostic value (12,13). For squamous cell carcinomas of the head and neck, lymphoscintigraphy has been shown to have potential for the detection of occult metastatic disease in patients staged N0 (14). Several preliminary reports have addressed SLN biopsy in carcinomas of the head and neck (15–21). Results are promising. However, publications are based on small groups of patients, and a large multicenter study has not yet been published.
To our knowledge, no published accounts have reported on the performance of SLN biopsy alone without elective neck dissection in the setting of a prospective study. Only a few reports describe intensive pathohistologic and immunohistologic examination of the sentinel node and all other lymph nodes of the neck dissection specimen. Yet this seems to be mandatory to determine the presence of occult micrometastases, not only in the SLNs but also in other nodes. In an elective neck dissection, undetected micrometastases in nonsentinel lymph nodes are removed but will remain in situ if only the sentinel nodes are harvested. Thus, if only an SLN biopsy is performed, a sufficient follow-up for late regional recurrence is necessary to determine the validity of the SLN concept in head and neck cancer. Therefore, SLN biopsy at present is still experimental and not yet to be performed in routine clinical practice.
If SLN biopsy can be validated for head and neck cancer, an open biopsy for occult metastatic disease will have to be followed by a neck dissection. This procedure is rendered more difficult as a result of the previous biopsy, in which anatomic units might have been dissected. If lymph nodes have been dissected, postoperative radiotherapy must be considered. This again will add to the morbidity of the patient in a situation that might otherwise have been avoided. Thus, the combination of the minimally invasive USgFNAC of the SLN depicted by lymphoscintigraphy seems to be an attractive alternative to an elective neck dissection or biopsy of the SLN.
In the present study, all patients except 2 (12%) accumulated tracer in SLNs within 4 h after peritumoral injection of the tracer. In 2 other studies, a lack of tracer accumulation in lymph nodes observed by a gamma camera has been described in 29% and 8% of cases (5,22). There are several reasons that an SLN might not be visualized in lymphoscintigraphy. Nieuwenhuis et al. (22) and Colnot et al. (23) were able to detect radioactivity in material aspirated from a node suspected to be the SLN but not visualized by a gamma camera. Thus, a gamma camera may be not sensitive enough to detect all SLNs. In addition, an SLN localized close to the primary is difficult to identify and distinguish from the primary (23). Moreover, an SLN may not reveal any uptake of the tracer if in an advanced stage of metastasis or if there is a tumor cell embolization of the lymphatic vessels resulting in a blockage of the lymphatic drainage into the SLN (14,24).
Another problem was encountered when several lymph nodes were located in close proximity. In 9 of 21 SLNs, it was difficult to decide which lymph node was the one accumulating tracer in lymphoscintigraphy. This problem is illustrated by the fact that, in 2 of 7 patients with metastatic disease, metastases were found in different levels of the neck from those in which SLNs had been localized. Therefore, the lymph node punctured may not have been the one that had accumulated tracer in lymphoscintigraphy. This problem may be addressed by the application of a γ-probe, offering a more precise identification of lymph nodes accumulating activity. In addition, it offers the chance to check for radioactivity in the material aspirated as a positive control for having punctured the SLN (22,23). However, a percutaneous application of a γ-probe probably will not enable the examiner to differentiate an SLN from a lymph node not accumulating activity in close proximity. Unfortunately, at the time of this study, a γ-probe was not available in the department of otorhinolaryngology where the USgFNAC was performed. Thus, we had to rely on lymphoscintigraphy in combination with ultrasound examination of the neck to identify the approximate location of the SLNs.
Cytology of 9 SLNs in 7 patients who did not have any metastatic disease in their neck dissection specimens was not suggestive of metastatic disease. Thus, there were no false-positive results in USgFNAC of the SLN.
All patients with occult metastatic disease had lymphatic drainage, with a total of 12 lymph nodes accumulating activity. In 1 node, USgFNAC did not produce suitable material on which to base a cytologic diagnosis. One node, sized 3 × 4 × 3 mm, was judged to be too small to be punctured. Size is a limiting factor of USgFNAC and, depending on the experience of the examiner, nodes < 5 mm are difficult to puncture (11). In addition, a fanning technique may result in withdrawing the needle from the lymph node. The present results of 9% of insufficient material of USgFNAC are comparable with results reported in the literature (21% of nodes, 8% of neck sides) (11,25).
Only 1 of 12 SLNs or 1 of 7 patients with occult metastatic disease were shown to have metastatic material in USgFNAC. Nieuwenhuis et al. (22) reported on USgFNAC in 12 patients staged as N0 by palpation. In this study, in addition to our protocol, the SLN also was localized by application of a γ-probe. After puncture of a lymph node, the aspirate was checked for radiation. In 5 patients, an elective neck dissection was performed. Seven patients underwent clinical follow-up and ultrasound examination ranging from 4 to 12 mo. Of 3 patients with occult metastatic disease, 1 was diagnosed by USgFNAC of the SLN. In 1 patient, lymphoscintigraphy did not reveal an SLN. However, in this patient a USgFNAC was performed on a suspect lymph node. The aspirated material contained radioactivity and metastatic cells. In 1 patient whose aspirate was negative for occult metastases, regional recurrence developed after 3 mo of follow-up. The authors concluded that the method is feasible for the detection of occult metastatic disease in patients with N0 necks. The same authors reported on a similar group of 12 patients (23). Again, of 3 patients with occult metastatic disease, 1 was diagnosed by USgFNAC in the SLN localized by lymphoscintigraphy and γ-probe. The authors concluded that USgFNAC is feasible as a staging procedure in head and neck squamous cell carcinomas. The higher sensitivity noted by Nieuwenhuis et al. might be explained by the fact that they were able to test the aspirated material for radiation. Therefore, if a nonsentinel node had been punctured, it would have been noticed and another USgFNAC would have been performed until the sentinel node was aspirated. Therefore, it is possible that in our study a nonsentinel node might have been punctured and the sentinel node with occult metastatic disease might not have been aspirated. On the other hand, in the Dutch group, elective neck dissection was not performed on every patient and not all occult metastases may have been detected. This is demonstrated by the fact that a regional recurrence developed in 1 patient in the Dutch group during follow-up. In our group, an elective neck dissection was performed on every patient, probably raising the number of occult metastases detected and thus decreasing the sensitivity of USgFNAC of the SLN.
The low rate of detection, however, is troublesome. It may be attributable to the small size of occult metastases. Van den Brekel et al. (26) reported a rate of 38% of micrometastases in occult neck disease. In the present study, 25% of occult metastases were found to be micrometastases. Although in 1 case in our study micrometastases were detected by USgFNAC, this case must be regarded as accidental. Malignant cells of micrometastases probably will be missed in a high number of cases by USgFNAC, even when performed in a fanning technique. Yet, even routine histopathologic examination of complete lymph nodes does not detect all micrometastases. Additional serial sectioning with immunostaining reveals micrometastases in up to 8.2% of patients in whom neck dissection specimens had been diagnosed N0 after previous routine pathohistologic examination (27). In a study on SLNs in patients with breast cancer, the value of histopathologic examination was analyzed. In specimen cuts of 2-mm intervals stained with hematoxylin and eosin, 12% of patients were found to have metastases compared with 58% of patients whose specimens were sectioned at 0.25-mm intervals and stained with cytokeratin (28). If a surgeon, therefore, opts for the SLN instead of elective neck dissection as a means of further staging, he or she should do so with the most trustworthy method. A USgFNAC will not reliably sample all metastatic material needed to make patient management decisions. Thus, a biopsy of the SLN and close histopathologic and immunopathologic examination seem to be mandatory in detecting micrometastatic disease. Otherwise, sparing the patient from elective neck dissection may result in understaging of the neck.
CONCLUSION
Lymphoscintigraphic localization of the SLN in combination with USgFNAC offers the possibility of detecting occult metastatic disease in patients staged as N0. However, the potential inability of the method to puncture small sentinel nodes and incidental aspiration of micrometastatic material within a node strongly limit the negative predictive value of this method. Thus, it does not seem to be an alternative to biopsy of the SLN. An intensive histopathologic and immunopathologic work-up of the SLN for the detection of occult and micrometastatic disease seems to be the most promising method at the present. Therefore, we are focusing our research on γ-probe-guided intraoperative detection of the SLN.
Acknowledgments
Material in this article was originally presented at the 2nd International Sentinel Node Congress, December 1–4, 2000, in Santa Monica, CA.
Footnotes
Received Feb. 5, 2002; revision accepted Jun. 24, 2002.
For correspondence contact: Steffen Maune, MD, Department of Otorhinolaryngology, Head and Neck Surgery, Christian-Albrechts-University of Kiel, Arnold-Heller-Strasse 14, 24105 Kiel, Germany.
E-mail: maune{at}hno.uni-kiel.de




{kind=link}