


Abstract
The emergence of MRI has challenged the long-standing primacy of skeletal scintigraphy in pediatric cases of suspected acute hematogenous osteomyelitis (AHO) with nondiagnostic radiographs. This study evaluated a strategy in which skeletal scintigraphy is the primary and MRI a supplemental test. Methods: We reviewed the records of 213 children (age range, 8 mo–18 y; mean age, 67 mo) with musculoskeletal symptoms and nondiagnostic radiographs who were referred for skeletal scintigraphy because of the possibility of AHO. MRI was performed when diagnostic uncertainty persisted after skeletal scintigraphy or when abscess was suspected. Results: Diagnosis was made using skeletal scintigraphy without referral for MRI in 179 (84%) of the children, including 79 (92%) of 86 with a final diagnosis of AHO. In no instance was the diagnosis of AHO indicated only by MRI. Treatment and diagnosis were accomplished without referral for MRI in 146 (69%) of all cases and 46 (53%) of the AHO cases. Abscesses that required drainage were found in 3 (6%) of 48 cases of major-long-bone AHO. Each of these 3 had exhibited a slow therapeutic response before MRI. Drainable abscesses were found in 5 (20%) of 25 cases affecting the pelvis, which was the other preponderant location of AHO. These were found with pelvic foci both when MRI was performed at diagnosis and when MRI was performed during treatment. Conclusion: An imaging strategy in which skeletal scintigraphy is the first test used when AHO is suspected but radiographs are negative remains highly effective. This approach can be most strongly advocated when symptoms are poorly localized or are localized to major long bones. MRI should be performed after skeletal scintigraphy shows major-long-bone AHO if treatment response is slow. Skeletal scintigraphy is also an appropriate first test for suspected radiographically occult pelvic AHO. Because of the association of abscesses with pelvic AHO, however, the use of MRI should be strongly considered after pelvic AHO is detected, and MRI might be substituted diagnostically for skeletal scintigraphy when symptoms are well localized to the pelvis.
Acute hematogenous osteomyelitis (AHO) is a common pediatric problem. Early diagnosis helps prevent sepsis, chronic infection, growth arrest, and deforming bone damage. Unfortunately, diagnosis can be difficult. The initial imaging test when AHO is suspected, plain-film radiography (1–5), can show deep soft-tissue swelling as early as 48 h after the onset of symptoms but shows bone destruction or periosteal reaction only after 7–10 d (6). Skeletal scintigraphy has played a central role in expediting diagnosis and treatment since its use for this purpose was described by Gilday et al. (7), Treves et al. (8), and Majd and Frankel (9) in 1975 and 1976. Its sensitivity and specificity exceed 90% when it is interpreted with knowledge of clinical findings (10). It seldom requires sedation, is cost effective (11), and provides a whole-body survey. The last point is most important both when symptoms are poorly localized or referred and when AHO is multifocal, as occurs in about 6% of pediatric cases (12).
The emergence of MRI has raised questions about appropriate imaging of suspected AHO. Reports, although biased because MRI was performed after skeletal scintigraphy, have suggested that MRI is more sensitive to early abnormalities in AHO (11,13,14). Moreover, identification of intraosseous, subperiosteal, and soft-tissue abscesses with MRI (15) can enable early abscess drainage.
At our hospital, skeletal scintigraphy has remained favored as the initial test for assessing suspected radiographically occult AHO at all but vertebral locations. MRI is performed when the results of skeletal scintigraphy are equivocal, are too nonspecific to allow a diagnosis to be reached, or conflict with the clinical impression and when complications of AHO, particularly abscess, are suspected. The advocacy of this approach by us and others is based on opinion and experience (2–5,14,16,17). Data that directly address its effectiveness are lacking. The purpose of this study was to assess how effective this imaging strategy is by looking at how often MRI is requested after skeletal scintigraphy, how often diagnoses made with skeletal scintigraphy are changed after MRI, and how often the ability of MRI to show an abscess affects management of AHO.
MATERIALS AND METHODS
We retrospectively reviewed the imaging studies and medical records of 213 children older than 6 mo (age range, 8 mo–18 y; mean age, 67 mo) with musculoskeletal symptoms and nondiagnostic radiographs who were consecutively referred for skeletal scintigraphy because of the possibility of AHO and who had no known skeletal pathology or systemic illnesses predisposing to AHO. No patient had undergone MRI before skeletal scintigraphy. Sixty-seven underwent MRI after skeletal scintigraphy. The imaging strategy used was consistent with our institutional clinical practice guideline. The study was approved by our institutional review board; patient informed consent was not required.
Skeletal scintigraphy was performed using 99mTc-methylene diphosphonate. The administered dose was 7.4 MBq/kg (dose range, 74–740 MBq). A gamma camera (Orbiter, Multispect-3, or E-Cam; Siemens Gammasonics, Hoffmann Estates, IL) equipped with a high-resolution collimator was used. Angiographic- and tissue-phase imaging was directed at the site of highest clinical suspicion. Whole-body skeletal-phase imaging was performed 3–4 h after dose administration. Spot planar images, whole-body sweep images, or both were obtained. At the discretion of the interpreting physician, these were supplemented with pinhole magnification imaging or SPECT. Sedation was not used in any patient. No study was considered technically inadequate.
MRI was performed with a 1.5-T system (Signa; General Electric Medical Systems, Milwaukee, WI). Sagittal or coronal T1-weighted and fast spin echo inversion recovery images, axial fast spin echo T2-weighted fat-saturated images, and gadolinium-enhanced axial and coronal or sagittal fat-suppressed T1-weighted images were obtained. Sedation was used in 30 (45%) of the 67 patients who underwent MRI, including 27 (87%) of the 31 patients who were 72 mo old or younger.
Skeletal scintigraphy was interpreted by staff nuclear medicine physicians. MRI was interpreted by staff pediatric radiologists. The interpreting physicians were aware of the clinical findings and the results of all preceding tests.
The principal diagnosis indicated by skeletal scintigraphy was recorded. For patients who underwent MRI, the indication for referral, the principal diagnosis indicated in the MRI report, and MRI findings indicative of complications were recorded. The diagnosis made by the referring physicians after their evaluation of clinical, laboratory, and imaging findings was used as the final diagnosis.
RESULTS
The principal diagnoses indicated by skeletal scintigraphy and the final diagnoses of the 213 children are found in Table 1. The principal diagnosis indicated by skeletal scintigraphy was AHO in 86 children: 85 (99%) of the 86 in whom the final diagnosis was AHO and 1 (1%) of 127 in whom other final diagnoses were reached. Among the cases with a final diagnosis of AHO, a solitary uptake abnormality was shown in 83, 2 uptake abnormalities were shown in 2, and no uptake abnormality was shown in 1. The uptake abnormalities in children whose final diagnosis was AHO were in the major long bones of 48, the pelvis of 25, the feet of 7, the spine of 2, the clavicle of 2, and the patella of 1. Skeletal scintigraphy facilitated diagnosis in 57 (86%) of 66 patients who presented with only poorly localized symptoms and 14 (9.5%) of 147 patients who described localized pain but whose only uptake abnormalities were at sites removed from the painful locus.
Principal Diagnoses Indicated by Skeletal Scintigraphy and Final Diagnoses
The diagnosis was made using skeletal scintigraphy without referral for MRI in 179 (84%) of the children: 127 with and 52 without abnormalities shown by skeletal scintigraphy. These included 79 (92%) of 86 with a final diagnosis of AHO. In addition to the diagnosis being made, therapy was completed using skeletal scintigraphy but not MRI in 146 (69%) of all cases and 46 (53%) of the AHO cases.
MRI was requested to increase diagnostic certainty in 34 children. Eighteen of these MRI examination were due entirely to clinical questions (Fig. 1), and 16 were due to nonspecificity of scintigraphic findings and clinical concerns (Fig. 2). Diagnoses suggested by skeletal scintigraphy and MRI along with the final diagnoses for children who were referred for MRI are listed in Table 2. The results of skeletal scintigraphy and MRI were concordant for 30 (88%) of these patients (AHO, 6; other conditions, 17; no abnormalities, 7). The diagnoses suggested by skeletal scintigraphy and MRI, the interval (in days) between studies, and the final diagnoses for the 4 children with discordant results are detailed in Table 3. The results of MRI did not alter management in any of the patients with AHO in whom diagnostic uncertainty persisted after scintigraphy, although MRI did show subcentimeter soft-tissue abscesses in 1 child with iliac AHO and subcentimeter intraosseous abscesses in 1 child with tibial AHO (Fig. 1). Both children were treated medically without intervention. In no instance was the diagnosis of AHO indicated only by MRI. In 1 instance, skeletal scintigraphy suggested AHO but MRI supported a noninfectious process. One child, for whom both skeletal scintigraphy and MRI were interpreted as showing nonspecific abnormalities, was treated empirically for AHO without subsequent confirmation by bone aspiration or biopsy. No other child for whom a diagnosis other than AHO was indicated by skeletal scintigraphy was later found to have AHO.
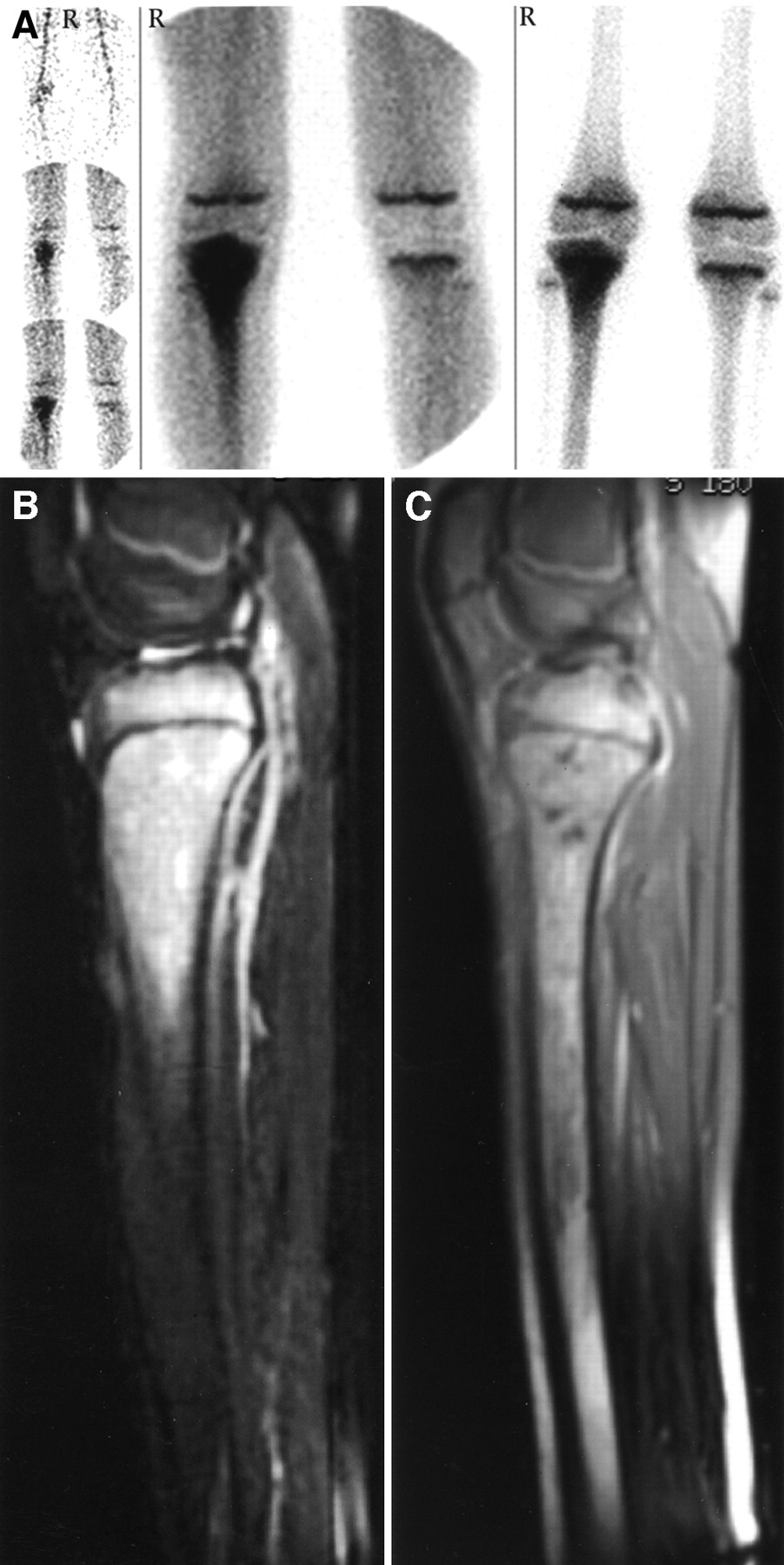
AHO: MRI performed for diagnostic uncertainty. (A) High tracer localization and uptake are shown in right proximal tibial metaphysis on angiographic-, tissue-, and skeletal-phase images of 13-y-old boy. Findings are typical and highly supportive of diagnosis of AHO. (B) Based entirely on clinical concerns, referring orthopedist obtained MRI. Sagittal fast spin echo inversion recovery MR image shows high signal intensity indicative of marrow edema in right proximal tibial epiphysis, metaphysis, and diaphysis. (C) Sagittal T1-weighted MR image after gadolinium administration shows small (<5 mm) nonenhancing regions indicative of intraosseous abscesses in metaphysis. Although these findings are no more specific than those shown by skeletal scintigraphy, combined results of 2 examinations were clinically regarded as confirmatory of AHO. Patient’s symptoms abated and his erythrocyte sedimentation rate returned to normal during treatment with antibiotics.
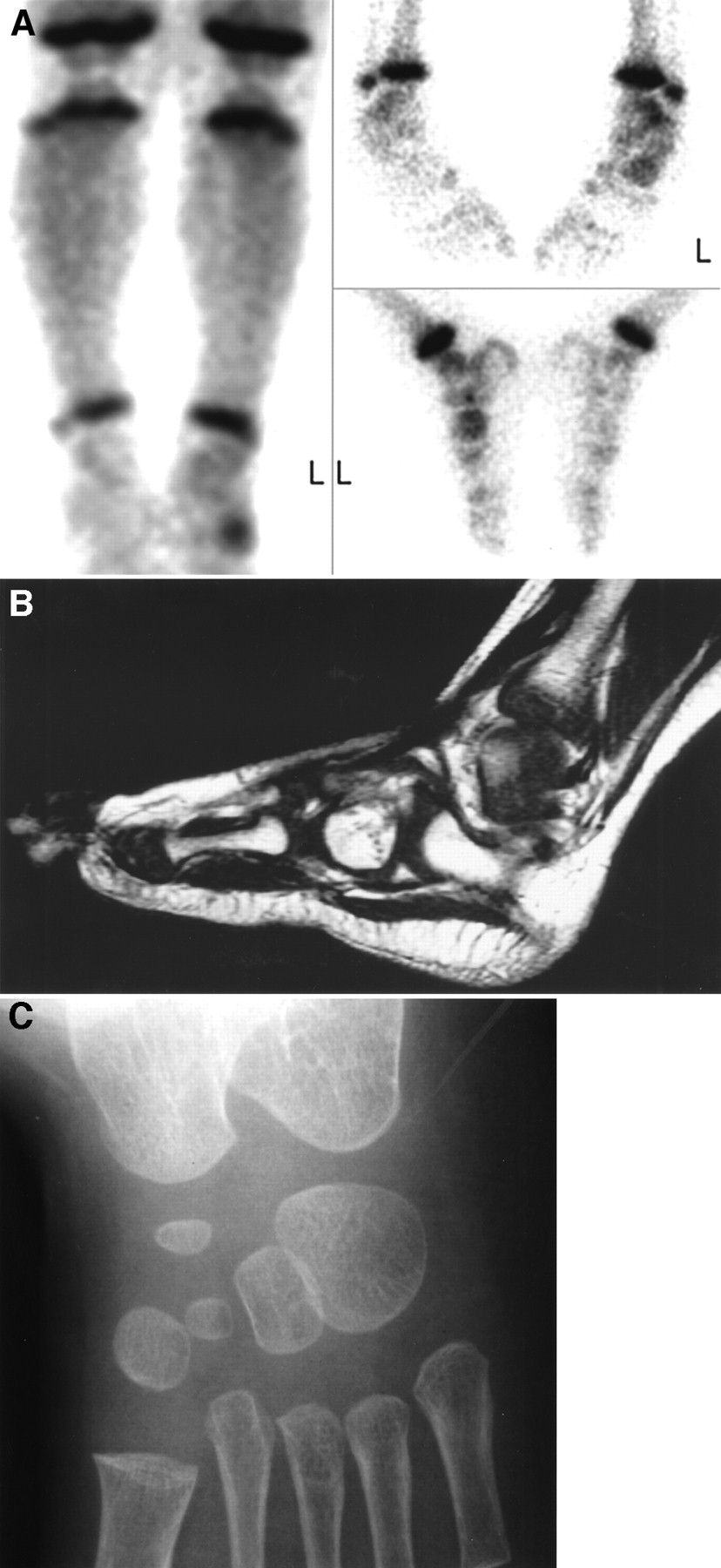
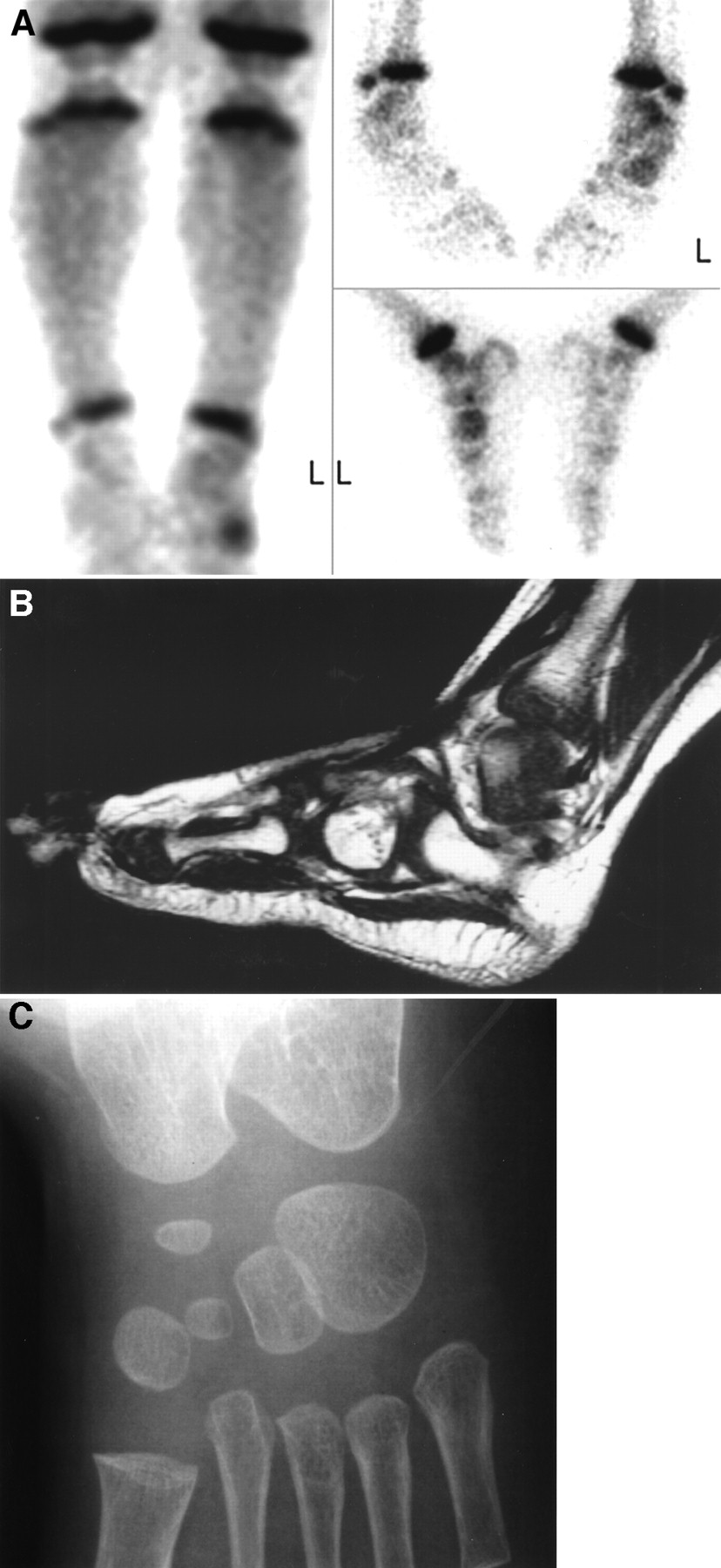
Cuboid fracture: MRI performed for diagnostic uncertainty. (A) Skeletal scintigraphy tissue- and skeletal-phase images of 19-mo-old boy with 2-d history of limp and 1-d history of fever demonstrates high tracer localization and uptake in left cuboid. This finding is most suggestive of cuboid fracture in child of this age. (B) Noting that traumatized bone is susceptible to AHO and that scintigraphic findings are not specific, referring orthopedist requested MRI. Sagittal T1-weighted gadolinium-enhanced MR image demonstrates linear nonenhancing band of low signal intensity indicative of fracture through base of left cuboid. (C) Fracture had not been shown by plain radiographs. Only after bone aspirate and blood cultures showed no growth and after symptoms of viral upper respiratory and gastrointestinal illness had developed was diagnosis of cuboid fracture without AHO believed to be confirmed and antibiotics discontinued. Symptoms resolved after short leg walking cast was placed.
Principal Diagnoses Indicated by Skeletal Scintigraphy and by MRI and Final Diagnoses for Children Who Underwent MRI to Improve Diagnostic Certainty
Discordant Results
MRI was performed to determine whether AHO was associated with abscess (Figs. 3 and 4) in 33 children. In 15 of these, MRI was performed within 24 h of skeletal scintigraphy because of concern about an abscess based on a pelvic (n = 11) or vertebral (n = 2) site of involvement or soft-tissue abnormalities (n = 2) shown by skeletal scintigraphy. In the other 18 patients, concern about an abscess was based on failure of signs and symptoms to resolve after 2 or more days (range, 2–7 d; mean, 3.1 d) of antibiotic therapy. Indications of intraosseous, subperiosteal, or soft-tissue abscesses were found in 15 (45%) of the 33 children: 6 (40%) of the 15 who were studied because of concern at diagnosis and 9 (50%) of the 18 who were evaluated during treatment. Surgical or percutaneous drainage was performed on 11 (73%) of the 15 children in whom a suspected abscess was confirmed by MRI. Drainage was deferred and symptoms subsequently resolved in 2 children with pelvic AHO and subcentimeter abscesses and 2 children with femoral AHO and subcentimeter abscesses. Table 4 summarizes the distribution of cases with a final diagnosis of AHO for whom MRI was obtained and in whom abscesses were suspected, detected, and drained. Among the preponderant locations of AHO, drainable abscesses were shown by MRI in 3 (6%) of 48 cases affecting major long bones and 5 (20%) of 25 cases affecting the pelvis. All such abscesses associated with major-long-bone AHO were found after a slow therapeutic response. With pelvic AHO, 4 were found at diagnosis and 1 after a slow therapeutic response. Other sites of AHO that were associated with drainable abscesses were the clavicle (n = 2) and the spine (n = 1).

Pelvic AHO with soft-tissue abscess. (A) Tissue- and skeletal-phase images show high tracer localization and uptake extending from left anterosuperior to anteroinferior iliac spine of 9-y-old boy. MRI was requested to assess for possible abscess because of pelvic location of presumed AHO. (B) Coronal gadolinium-enhanced fat-suppressed T1-weighted MR image shows enhancement of ilium corresponding to abnormality shown by scintigraphy. Within enhancing region is nonenhancing area consistent with intraosseous abscess (long arrow). Lobulated rim-enhancing abscess is also present in proximal left musculus gluteus minimus adjacent to anterosuperior iliac spine (short arrow). Note that scintigraphic tissue-phase image also shows subtle degree of high soft-tissue tracer localization in this region. Percutaneous abscess drainage was performed.

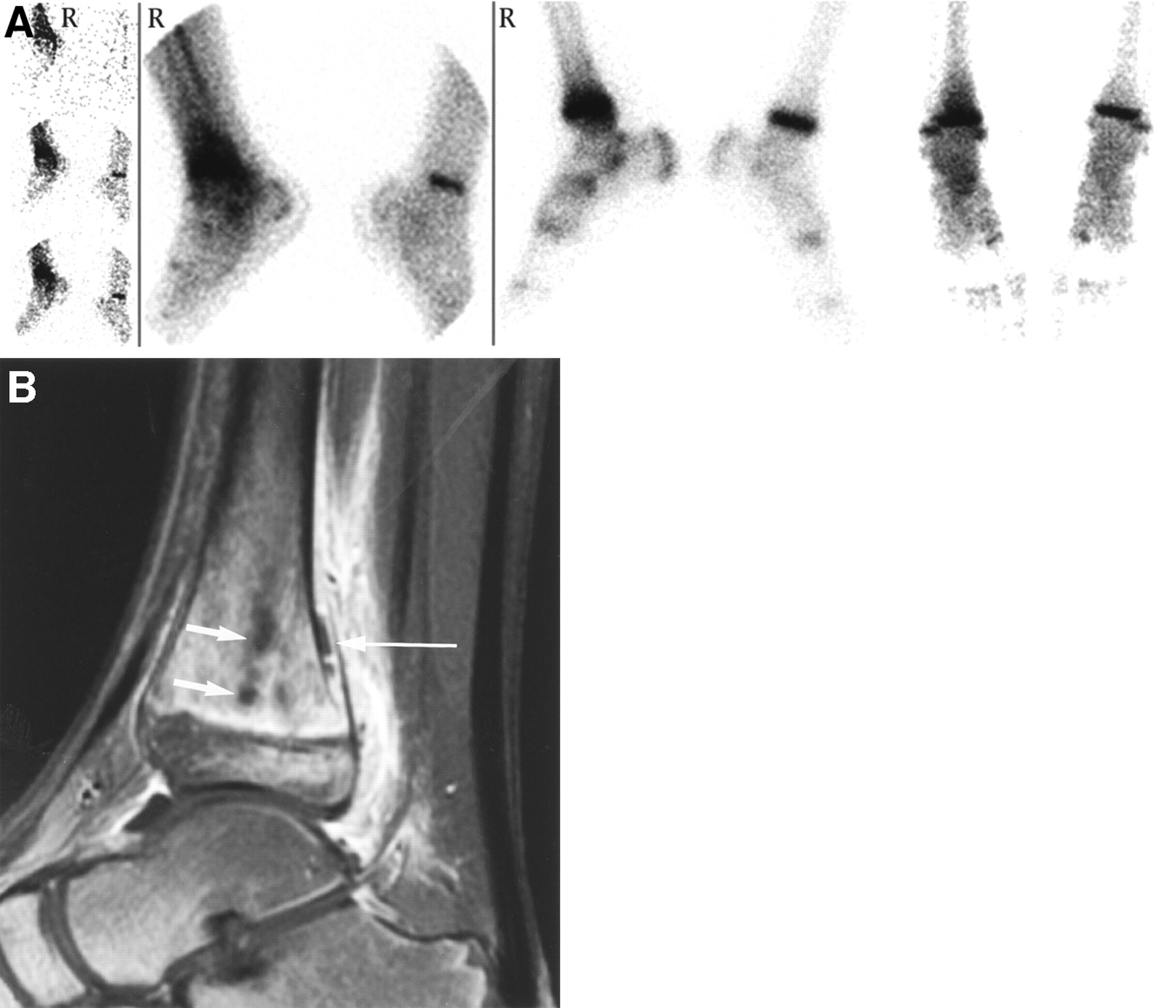
AHO with subperiosteal and intraosseous abscess. (A) Angiographic-, tissue-, and skeletal-phase images show high tracer localization and uptake in distal right tibial metaphysis of 11-y-old boy. (B) After fever and pain continued through 3 d of intravenous antibiotic therapy, MRI was requested to assess for suspected abscess. Sagittal gadolinium-enhanced fat-suppressed T1-weighted MR image shows focal intraosseous nonenhancing areas (short arrows) and periosteal elevation with nonenhancing subperiosteal collection (long arrow). Findings indicated intraosseous and subperiosteal abscesses, which were subsequently drained surgically.
AHO and Abscesses
DISCUSSION
Should skeletal scintigraphy still be used or should MRI take its place for radiographically occult AHO? Should both imaging tests be used? Conclusive answers would come only from a prospective study using standardized criteria for image interpretation and diagnosis. Nevertheless, our results provide insight into this important issue.
The results indicate that clinical practitioners found skeletal scintigraphy to provide all the imaging information that was needed for diagnostic evaluation in 84% of 213 children with suspected AHO and nondiagnostic radiographs in this study. Although cases in which AHO is not revealed by skeletal scintigraphy certainly occur, no child in this study had evidence of AHO by MRI but not by skeletal scintigraphy. This was observed despite the fact that MRI was performed after skeletal scintigraphy, which introduces the same bias favoring MRI that is found in reports indicating a higher sensitivity for MRI (11,13,14). A diagnosis of AHO that had been suggested by skeletal scintigraphy was refuted by MRI in only 1 case. Diagnoses of osseous pathology suggested by skeletal scintigraphy and MRI did not differ in any other case.
In children with suspected AHO, the value of skeletal scintigraphy was not limited to indicating sites of AHO. Abnormal skeletal scintigraphy with findings suggestive of other conditions and negative skeletal scintigraphy were valuable in excluding AHO. The final diagnosis was AHO in only 1 of 127 cases in which it was not the principal diagnosis indicated by skeletal scintigraphy. In that case, the findings of both skeletal scintigraphy and MRI were interpreted as normal. Skeletal scintigraphy was useful regardless of the degree to which symptoms were localized. A whole-body survey was particularly important in the 9% of our patients whose only site of disease was remote from the painful locus. Skeletal scintigraphy is potentially valuable in cases in which AHO is multifocal, but skeletal scintigraphy likely does not affect therapy in such cases. Whole-body MRI techniques (18) may eventually make MRI as effective as scintigraphy in evaluating children with poorly localized or referred symptoms, but these techniques are still under development.
For 69% of children with suspected AHO, decisions about management and diagnosis were made without referral for MRI. Among children with a diagnosis of AHO indicated by skeletal scintigraphy, management proceeded without referral for MRI in 54% of cases. Management proceeded without referral for MRI more frequently for AHO of major long bones than for AHO of pelvic bones, because of a higher concern about abscesses in patients with pelvic AHO. The higher concern was justified by MRI’s showing abscesses that required drainage in 20% of all cases of pelvic AHO, as opposed to 6% of all cases of major-long-bone AHO. Abscesses that required drainage were found in major-long-bone AHO only after signs and symptoms did not resolve rapidly during treatment. Conversely, with AHO of other sites, particularly the pelvis but also the spine and clavicle, drainable abscesses were discovered at diagnosis as well as during treatment.
The results of this study support use of skeletal scintigraphy as the initial test for diagnosis of AHO after negative radiography results, particularly when symptoms are poorly localized or indicate major-long-bone involvement. The relative ease of performing a whole-body evaluation with skeletal scintigraphy and the absence of a practical method for doing so with MRI mean that no significant disagreement is likely to arise in regard to imaging children with poorly localized symptoms. The infrequency with which MRI altered management in cases of long-bone AHO seems not to justify imaging all cases of suspected major-long-bone AHO by MRI or routinely performing MRI after major-long-bone AHO is indicated by skeletal scintigraphy. Whether skeletal scintigraphy should be used in preference to MRI for evaluating suspected pelvic AHO is less certain. This study indicated that pelvic AHO is readily diagnosed by skeletal scintigraphy but suggested that use of MRI to assess for abscesses may be warranted when skeletal scintigraphy indicates pelvic AHO.
Other issues worth considering when developing an algorithm for children with suspected radiographically occult AHO are the need for sedation during examination, the relative monetary costs of skeletal scintigraphy and MRI, and the implications of exposure to ionizing radiation. Of these, only the use of sedation is directly addressed by our data. All skeletal scintigraphy images, none of which was considered technically inadequate, were obtained without sedation, whereas performance of MRI required sedation for 45% of all patients and 87% of patients younger than 72 mo old. Sedation may be used more frequently elsewhere than at our pediatric hospital for performing skeletal scintigraphy, but these results confirm that the need for sedation is greater with skeletal scintigraphy than with MRI.
It is important to emphasize that this study did not directly compare skeletal scintigraphy with MRI. The relative sensitivities and specificities of the 2 modalities can be established only by the type of prospective study mentioned above, in which all patients undergo both studies at nearly the same time. Such a study would be difficult to perform. It is certainly possible that fewer children would be referred for skeletal scintigraphy after MRI than have been referred for MRI after skeletal scintigraphy. To some extent, however, requests for MRI after skeletal scintigraphy are likely driven by the greater familiarity of clinicians with the specificity limitations of scintigraphy than of MRI (19) and with the conclusions than with the methodologic flaws of studies suggesting a higher sensitivity for MRI (11,13,14). In this regard, it is important to note that performance of MRI on our patients infrequently altered diagnoses made by combined assessment of clinical findings and skeletal scintigraphy.
This study had limitations. First, diagnosis of AHO was not always proven; reliance was placed on the final clinical impression. We chose not to insist on bacteriologic confirmation because infective organisms are identified by blood or bone culture in only 50%–70% of cases of AHO (20–22). We believe that the methodology accurately portrayed the effectiveness of the imaging strategy in clinical practice, in which the treatment for cases with bacteriologically confirmed and presumptive diagnoses is identical. The methodology has led us not to try to determine sensitivity and specificity, however. Second, factors specific to individual situations must be considered in devising an imaging strategy. Different levels of expertise in performing imaging and interpreting the findings can significantly affect its value. Similarly, different practitioners will have different ideas about what incremental improvement in certainty warrants referral for additional testing. This factor likely affected our results, in which the need for MRI was determined by referring physicians acting without standardized criteria. Third, the use of other modalities was not evaluated. The imaging strategy was based on a belief that MRI provides the most accurate and expeditious means of confirming or refuting diagnoses suggested by skeletal scintigraphy and of anatomically localizing abscesses before drainage. How ultrasonography, CT, or imaging with other radiopharmaceuticals such as radiolabeled leukocytes, 67Ga-citrate, and 99mTc-sulfur colloid might serve the same purposes was not addressed.
CONCLUSION
An imaging strategy in which skeletal scintigraphy is the first test used when AHO is suspected but radiography findings are negative remains highly effective. This approach can be most strongly advocated when symptoms are poorly localized or are localized to major long bones. MRI should be performed after skeletal scintigraphy shows major-long-bone AHO if treatment response is slow. Skeletal scintigraphy is also an appropriate first test for suspected radiographically occult pelvic AHO. Because of the association of abscesses with pelvic AHO, however, the use of MRI should be strongly considered after pelvic AHO is detected, and MRI might be substituted diagnostically for skeletal scintigraphy when symptoms are well localized to the pelvis.
Acknowledgments
The authors thank N. Thorne Griscom, MD, for valuable editorial comments.
Footnotes
Received Dec. 10, 2001; revision accepted Jun. 11, 2002.
For correspondence or reprints contact: Leonard P. Connolly, MD, Division of Nuclear Medicine, Children’s Hospital, 300 Longwood Ave., Boston, MA 02115.
E-mail: connolly_l{at}TCH.Harvard.edu





{kind=link}
{kind=link}
{kind=link}
{kind=link}