


Abstract
This study evaluated the effects of low-dose cisplatin plus 89Sr versus 89Sr alone in the treatment of painful bone metastases from prostate cancer, addressing both pain palliation and cytostatic effects. Methods: Seventy patients with metastatic hormone-refractory prostate cancer were randomized into 2 groups: One group (arm A) received 148 MBq 89Sr plus 50 mg/m2 cisplatin, and the other group (arm B) received 148 MBq 89Sr plus placebo. After treatment, the patients were followed up until death to evaluate the outcome variables: grade and duration of pain palliation, onset of new painful sites, changes in bone disease, global survival, serum prostate-specific antigen and alkaline phosphatase changes, and hematologic toxicity. Results: Overall pain relief occurred in 91% of patients in arm A and 63% of patients in arm B (P < 0.01), with a median duration of 120 d in arm A and 60 d in arm B (P = 0.002). New painful sites on previously asymptomatic bone metastases appeared in 14% of patients in arm A and in 30% of patients in arm B (P = 0.18). The median survival without new painful sites was 4 mo in arm A and 2 mo in arm B (P = 0.04). Bone disease progression was observed in 27% of patients in arm A and in 64% of patients in arm B (P = 0.01). Median global survival after therapy was 9 mo in arm A and 6 mo in arm B (P = 0.30). Transient and moderate hematologic toxicity, as determined by World Health Organization criteria, was apparent in both arms without significant differences. Conclusion: The addition of a low dose of cisplatin enhances the effect of a standard dose of 89Sr without significant side effects, producing a significant improvement in pain palliation and a cytostatic effect on bone disease.
Painful bone metastases are a challenging problem in the management of patients with hormone-refractory prostate cancer because of its high prevalence and high morbidity (1,2). Effective palliative treatment of painful bone metastases is a key therapeutic goal in these patients, aiming at improving their quality of life. External-beam irradiation, although effective on localized lesions, cannot routinely be used in the treatment of diffuse or multifocal bone disease because hemibody irradiation is associated with significant marrow toxicity (3). Chemotherapy has not shown encouraging results in metastatic prostate cancer (4), and the efficacy of the pharmacologic approach with analgesics is limited by drug tolerance and adverse effects when drugs are used at high doses and for prolonged periods (5).
Radionuclide therapy with 89Sr-chloride (89Sr) is an effective alternative for bone pain in prostate cancer, producing a palliation rate of 51%–96% (6–9). Despite these encouraging results some problems remain to be clarified, such as the significant percentage of unresponsive patients (up to 30%), the low complete response rate (up to 20%), and the effect on bone disease progression (6). Although total target doses for 89Sr are quite high, up to 5,000 cGy using a standard dose of 148 MBq (10,11), the dose rate at which the radiation is delivered is low, <4 cGy/h (12), and may limit 89Sr efficacy by allowing repair of sublethal radiation injury and being insufficient to counteract proliferation of tumor cells (13).
Preliminary strategies for increasing the response rate to 89Sr have been devised using platinum-mediated radiosensitization of cancer cells, but these preliminary encouraging results have not yet been validated in a randomized clinical trial (12,14,15). This article reports a randomized phase III clinical trial evaluating the effects of low-dose cis-diamminedichloroplatinum (II), or cisplatin, plus 89Sr versus the effects of 89Sr alone in the treatment of 70 prostate cancer patients with painful bone metastases.
MATERIALS AND METHODS
Study Design
The study was a phase III prospective clinical trial. It was controlled, randomized, and masked and was approved by the local Ethic Committee. Eligible patients were randomized into 2 groups receiving different treatment: One (arm A) received the treatment to be tested (89Sr plus cisplatin); the other (arm B) received 89Sr plus placebo and served as the control group. Each patient gave written informed consent.
A data manager randomly allocated patients to either arm by applying a previously established algorithm to a set of random numbers. Patients were also randomized separately into 2 strata to avoid confounding effects from different baseline clinical conditions. Subdivision of patients into the 2 strata was based on their general condition and their performance status score on the Karnofsky Scale. Stratum 1 included patients with a mildly impaired general condition and a Karnofsky score of 60–100. Stratum 2 included patients with a strongly impaired general condition and a Karnofsky score of 10–50. Neither patients nor clinicians knew the group to which patients had been assigned, ensuring a correct double blinding of the study and avoiding confounding factors during follow-up. Pain palliation, cytostatic effect, and marrow toxicity were the endpoints addressed.
Patients
Seventy patients (age range, 51–89 y; mean age, 69 y) with bone metastases from histologically proven prostate cancer entered the study after a baseline clinical examination and were randomized into the 2 arms, each containing 35 patients. Eleven patients had been treated by chemotherapy, 20 by local external-beam radiotherapy, and 6 by both. A minimum of 6 mo had elapsed after the completion of previous chemotherapy or radiotherapy. Hormone therapy had not been altered in the previous 3 mo and was continued without change during the study. All patients had hormone-resistant disease that was progressing after being treated with at least 2 hormone schedules.
Patients were enrolled into the study according to the usual eligibility criteria, as previously defined (16). Patients were excluded if they had difficulty complying with the follow-up schedule or had suspected disseminated intravascular coagulation or evidence of spinal cord compression.
Baseline Evaluation
Before randomization, all enrolled patients underwent a complete clinical evaluation to measure baseline pretherapy variables: age, hematologic and renal function, serum alkaline phosphatase (AP) level, prostate-specific antigen (PSA) level, and performance status score on the Karnofsky Scale. Pain was evaluated by a 5-point score assigned using a modified Wisconsin test (16) and by a pain map illustrating the number and topography of painful sites. Bone disease was assessed by 99mTc-methylene diphosphonate bone scanning, with assignment of a 5-point scintigraphic score based on the number or extent of metastases according to the criteria of Soloway et al. (17). All bone scanning was performed, and the results classified, by well-trained nuclear physicians at our institute.
Treatment Protocol
Arm A. Two short hospitalizations, at an interval of 10 d, were required for each patient. In the first hospitalization, a slow intravenous cisplatin infusion (Cisplatino Teva; Teva Pharma, Milan, Italy) of 18 mg/m2 in 1,000 mL 0.9% sodium chloride solution plus 20 mg furosemide was administered over 3 h. At the end of the infusion, 148 MBq 89Sr (Metastron; Nycomed-Amersham International, Buckinghamshire, U.K.) were injected as a bolus (day 0). In the second hospitalization, an intravenous cisplatin infusion of 16 mg/m2 in 1,000 mL 0.9% sodium chloride solution plus 20 mg furosemide was administered over 6 h (day 10) and repeated the day after (day 11), for a total cisplatin dose of 32 mg/m2 infused over 48 h. Standard support consisting of intravenous hydration, steroids, and antiemetic drugs was used during both treatments.
Arm B. The protocol was the same as for arm A, except that a placebo infusion (1,000 mL 0.9% sodium chloride solution plus 20 mg furosemide) was administered in place of the cisplatin infusion.
Patient Follow-Up
After treatment, follow-up continued until the patient’s death, and the following variables were monitored at predetermined intervals: hematologic and renal function, AP and PSA serum levels, pain score, pain map, bone scan findings, and Karnofsky performance score.
Data Analysis
Pain Palliation. This outcome was evaluated 2 mo after 89Sr administration and was defined as positive (responders) if the pain score improved or negative (nonresponders) if it did not (16). A positive outcome was characterized on the basis of grade and duration of pain palliation. Grade was classified as complete response, partial response, or minimal response (16). Duration (survival time free of pain relapse) was determined by considering a worsening of the pain score to be a marker of the end of the palliative effect. The onset of new painful sites on previously asymptomatic bone metastases was also considered a pain palliation variable. Accordingly, the following factors were evaluated: for both arms of the study, the prevalence of patients presenting with new painful sites; for each arm of the study and each patient, the number of observed sites; and the survival time without onset of new painful sites.
Cytostatic Effect. This outcome was evaluated by classifying changes in bone disease and global survival. Bone disease was classified as showing a partial response, stability, or progression according to the National Prostate Cancer Project criteria for stage D2 prostate cancer (18). Global survival after therapy was evaluated as survival free of pain relapse plus survival after pain relapse and was illustrated by Kaplan–Meier curves. All deaths, both tumor related and tumor unrelated, were included in the analysis. In addition, changes in AP and PSA serum levels were evaluated as indirect measures of cytostatic effect.
Marrow Toxicity.
This outcome was evaluated by measuring changes in platelets, leukocytes, and hemoglobin during the first 3 mo of follow-up and was classified by a 5-point toxicity score according to World Health Organization (WHO) criteria (19).
Statistical Analysis
Outcome variables (responders and response grade, new painful sites, and bone disease progression) were compared by the χ2 test. Survival times (survival free of pain relapse, survival without new painful sites, survival after pain relapse, and global survival after therapy) were assessed by Kaplan–Meier curves and compared by the log-rank test. Differences in pretherapy variables between the 2 arms were assessed by the t test for paired data or by the χ2 test, as appropriate, whereas differences between pretherapy and posttherapy variables in each arm were evaluated by the t test with Bonferroni adjustment and by the Wilcoxon signed rank test, as appropriate.
For ease of analysis, exact P values are reported. The level of significance was set at the conventional value of P < 0.05, and probability values just slightly greater than the α value of 0.05 were considered marginally significant (20). Confidence intervals (CIs) were also evaluated.
RESULTS
Patient baseline characteristics for each arm of the study are presented in Tables 1 and 2. No significant differences were observed in baseline variables between the 2 arms.
Baseline Variables in Patients Enrolled in Arm A
Baseline Variables in Patients Enrolled in Arm B
Pain Palliation
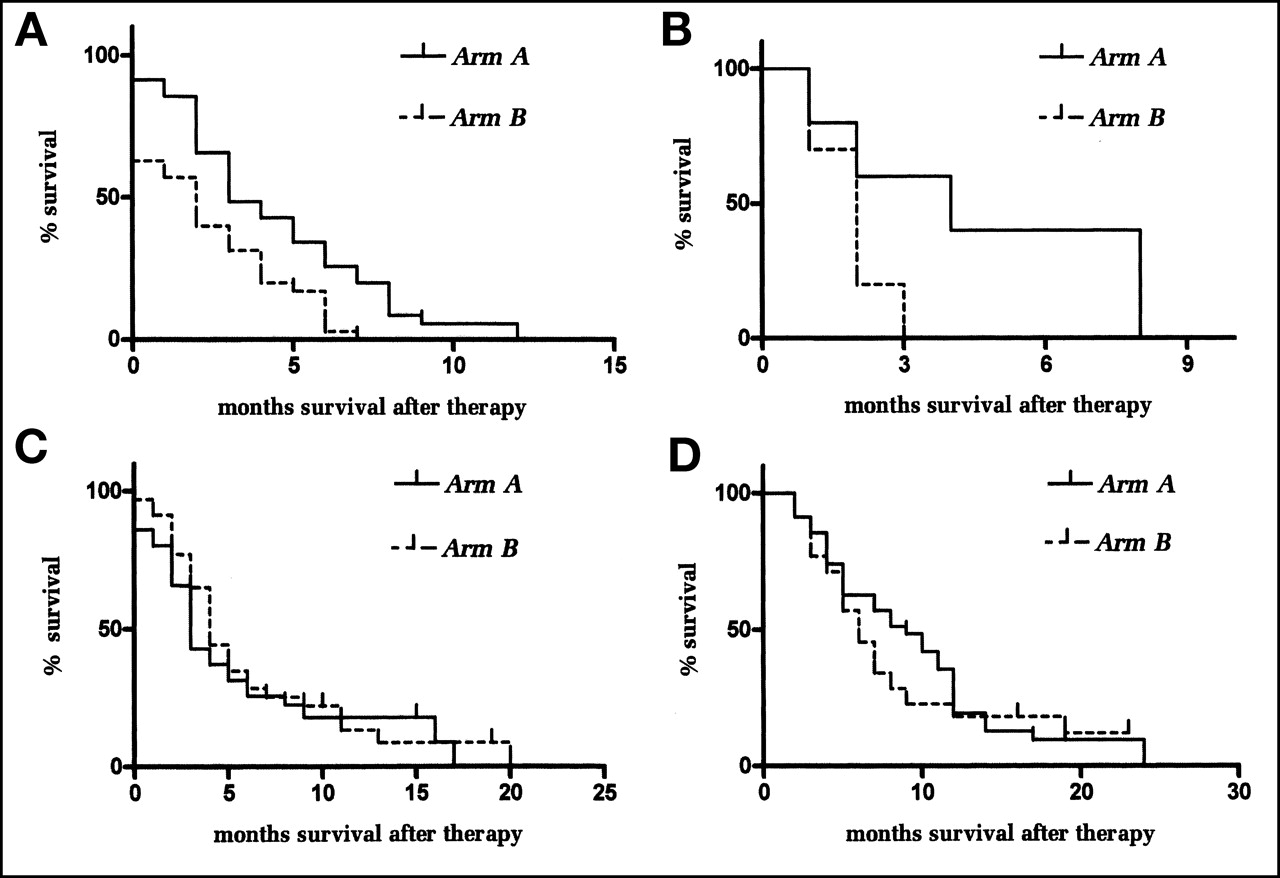
Overall pain relief occurred in 32 patients of arm A and in 22 patients of arm B (91% and 63%, respectively; P < 0.01). The grade of pain palliation in the 2 arms is reported in Table 3. Clinically evident pain relief occurred within 1 mo, with a median onset at 15 d in both arms. Survival free of pain relapse ranged from 1 mo to 1 y in arm A and from 1 to 7 mo in arm B (Fig. 1A). The mean duration of pain palliation was 134 d in arm A and 68 d in arm B, with a median of 120 and 60 d, respectively (P = 0.002).

Kaplan–Meier curves illustrating survival times in the 2 arms: survival free of pain relapse (A), survival without new painful sites (B), survival after pain relapse (C), and global survival after therapy (D).
Response Rates in Arms A and B
The percentage of patients presenting with new painful sites on previously asymptomatic bone metastases in arm A was less than half that in arm B (14% and 30%, respectively), without, however, reaching statistical significance (P = 0.18). The global number of new painful sites was 7 in arm A and 22 in arm B, with a mean of 1.4 sites for patients in arm A and 2.2 sites for patients in arm B. Survival without new painful sites was significantly different in the 2 arms, at a median of 4 mo in arm A and 2 mo in arm B (P = 0.04) (Fig. 1B).
Cytostatic Effect
Because 13 patients died too soon (<6 mo) to undergo follow-up scanning, bone disease changes were evaluable for only 30 of 35 patients in arm A and only 28 of 35 patients in arm B. Bone disease progressed during the 6 mo after therapy in 27% of patients in arm A and 64% of patients in arm B (P = 0.01). Bone disease was stable in 70% of patients in arm A and 36% of patients in arm B (P = 0.02). Bone disease showed a partial response in only 1 patient in arm A (Fig. 2).

Pretherapy (left) and posttherapy (right) bone scintigraphy of patient 18 of arm A with bone disease and partial response. (A) Whole-body scan shows intense tracer uptake in right pelvis and in 1 left rib before therapy, with evident reduction in uptake after therapy. (B) Planar views of pelvis.
Survival after therapy is illustrated in Figure 1 by Kaplan–Meier curves. To date, 59 of 70 patients that had been enrolled in the study have died (29 in arm A and 30 in arm B). Three patients in arm A died of causes unrelated to the tumor. Global survival after therapy ranges from 2 to 24 mo (median, 9 mo) in arm A and from 2 to 23 mo (median, 6 mo) in arm B (P = 0.3).
Changes in PSA and AP serum levels after therapy are illustrated in Figure 3.

PSA (A) and AP (B) basal values and monthly values during 6 mo after therapy. Values are reported as mean ± SEM. ⧫ = arm A; □ = arm B.
Marrow Toxicity
Changes in platelets, leukocytes, and hemoglobin during follow-up are illustrated in Figure 4. No significant differences were observed in pretherapy platelet, leukocyte, or hemoglobin values between the 2 arms.
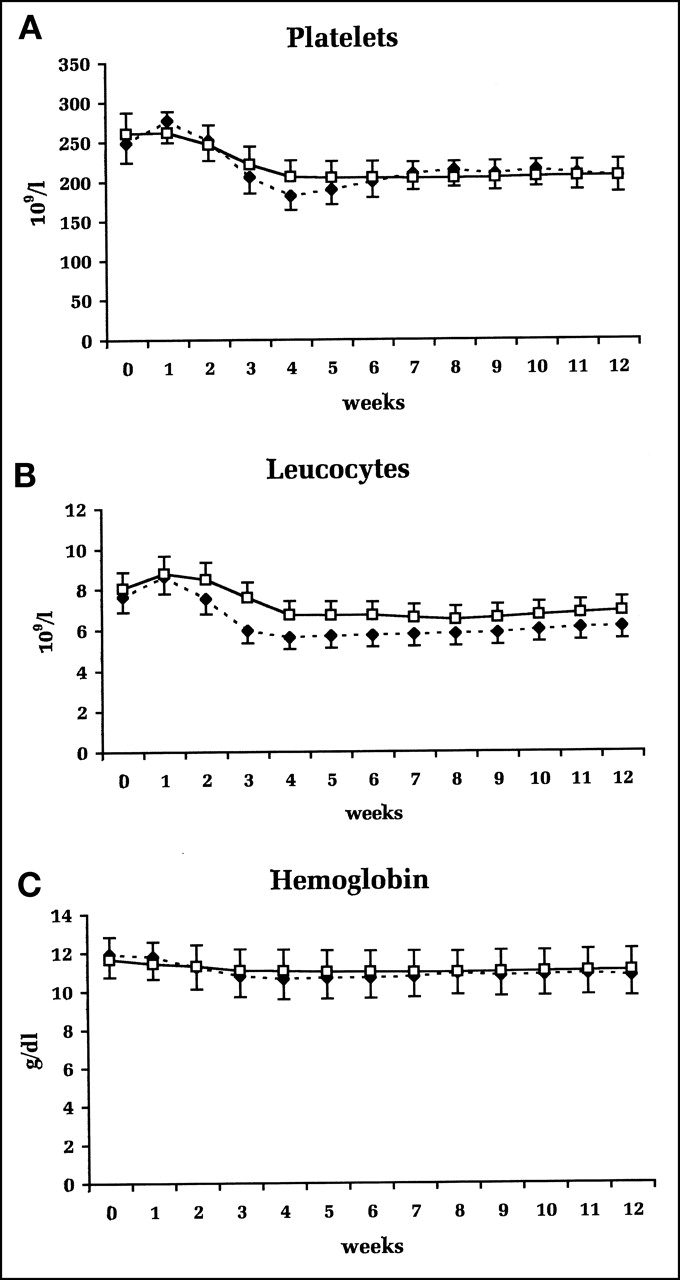
Platelet (A), leukocyte (B), and hemoglobin (C) basal values and weekly values during 3 mo after therapy. Values are reported as mean ± SEM. ⧫ = arm A; □ = arm B.
Arm A.
WHO grade 1 platelet toxicity was apparent in only 1 patient, in whom a 26% decrease in the mean platelet count at 4 wk slowly returned to normal within 3 mo after therapy. WHO grade 1–2 leukocyte toxicity was observed in 8 patients, who had a transient 26% decrease in the mean leukocyte count at 4 wk. Fourteen patients showed hemoglobin toxicity, which was WHO grade 4 in 2; WHO grade 3 in 1, and WHO grade 1–2 in 11. The mean hemoglobin values decreased 10% from baseline levels at 4 wk after therapy and remained mildly impaired for 2 mo.
Arm B.
WHO grade 1–2 platelet toxicity was apparent in only 2 patients, in whom a 22% decrease in the mean platelet count at 4 wk slowly returned to normal within 3 mo after therapy. WHO grade 2 leukocyte toxicity was observed in 2 patients, who had a 19% decrease in the mean leukocyte count at 6 wk. Thirteen patients showed hemoglobin toxicity, which was WHO grade 4 in 1, WHO grade 3 in 3, and WHO grade 1–2 in 9. The mean hemoglobin values decreased 6% from baseline levels at 2 mo after therapy and returned to normal within the following month.
Other Results
No side effects were clinically evident after cisplatin infusion. Ten patients (14%), 6 in arm A and 4 in arm B, experienced a mild, transient increase in pain, that is, a flare response, within 7 d after 89Sr injection. This response resolved within 24–48 h. No patient showed neurologic signs from nerve compression or renal function impairment. The Karnofsky performance score improved in 23 patients in arm A and 9 patients in arm B (66% and 26%, respectively; P = 0.002), remained the same in 6 patients in arm A and 11 patients in arm B (17% and 31%, respectively; P = 0.2), and worsened in 6 patients in arm A and 15 patients in arm B (17% and 43%, respectively; P = 0.03).
DISCUSSION
89Sr has widely been used for more than 50 y to relieve pain caused by bone metastases, the first clinical use dating to 1942 (21). Although the clinical efficacy of 89Sr is evident in 51%–96% of patients, only a small percentage of these patients experiences complete pain relief and only occasionally does objective evidence of tumor regression occur (7–9,22–25).
Cisplatin, a potent cytotoxic agent for a wide range of tumors, has radiosensitizing properties through several mechanisms when used at low doses (26–28). Preclinical data are available on the efficacy of cisplatin as a radiosensitizer in prostate cancer (29–31). The only available clinical experience with low-dose cisplatin plus β-emitter radionuclides is a preliminary report of Mertens et al. (12) on 18 patients with prostate carcinoma. That study, using a cisplatin schedule of 35 mg/m2 infused over 2 d, 1 wk, and 4 wk after 89Sr administration, showed good pain relief, mild toxicity, improvement in tracer uptake on posttreatment bone scans, and promising survival data. Unfortunately, the small sample size and single-arm design of the study made correlations between baseline variables and outcome difficult and did not support firm conclusions.
This study, being a randomized, controlled trial of a rational schedule of combined low-dose cisplatin and 89Sr in a relatively large sample of patients with advanced prostate cancer, addresses the question in a more structured way. A cumulative cisplatin dosage of 50 mg/m2 was chosen because doses of 20–100 mg/m2 ensure tissual drug levels high enough for biochemistry-based enhancement of radiation sensitivity in mammalian cells, that is, 0.5–2 ppm (27,32–34), avoiding the myelotoxic effects of the usual chemotherapeutic doses (>100 mg/m2).
The double administration of cisplatin (a few hours before and after 10 Gy 89Sr irradiation) was chosen on the basis of previous experience (27,35,36) to maximally enhance radiation damage. In fact, an enhancement ratio of 1.23–1.45 after 10 Gy continuous low-dose-rate irradiation and concurrent cisplatin infusion was reported by Fu et al. (35,36) for murine models, whereas other studies have suggested that cisplatin could be given before radiation because cisplatin–DNA adducts can take some hours to reach and then remain for several days (27,29).
The schedule of this study effectively enhanced the effect of 89Sr as addressed by all endpoints. In fact, the use of a low dose of cisplatin plus a standard dose of 89Sr significantly increased (P < 0.01) the prevalence of overall pain relief. This increase stemmed entirely from effects on the complete and partial response rates, with a true doubling of patients who had complete pain relief (10 patients in arm A vs. 5 patients in arm B). The current results confirm the preliminary results of Mertens et al. (12). Unfortunately, data on the prevalence of pain palliation from most trials using 89Sr alone are not comparable either with one another or with this study because of the small number of accrued or evaluable patients, the different or poorly defined criteria for evaluating responses, and the different inclusion criteria (7–9,22–25).
Pain palliation in this study was also significantly prolonged by the use of low-dose cisplatin plus 89Sr, with a doubling of the median duration of survival free of pain relapse (Fig. 1A). In addition, the relative risk of pain relapse in patients treated with 89Sr plus cisplatin was nearly half that in patients treated with 89Sr alone, with a hazard ratio (arm B to arm A) of 1.82 (95% CI, 1.40–4.45). These data fully agree with those of Mertens et al. (12), who reported a median duration of 4 mo for pain relief.
Both the number of patients presenting with new painful sites on previously asymptomatic metastases and the global number of new painful sites were consistently lower in arm A. In fact, in only 5 of 35 patients in arm A, versus 10 of 35 in arm B, did new painful sites develop on previously asymptomatic metastases, and onset was significantly later (P = 0.04) in arm A than in arm B. When the corresponding survival curves were analyzed (Fig. 1B), the hazard ratio for development of new painful sites for arm B was more than double that for arm A (ratio, 2.12). This finding could have important clinical significance well beyond the strictly palliative effect. In fact, only a small proportion of bone metastases become painful, and the factors that convert a painless lesion into a painful one are unknown (37). Pain onset may represent an increase in neoplastic bone invasion and be an early marker of bone disease progression.
Considering the second endpoint of the study, the cytostatic effect of using cisplatin plus 89Sr, the likelihood of such an effect on bone disease is confirmed by the changes in bone scan findings observed during follow-up. In fact, a significantly lower proportion of patients had disease progression in arm A (27%; 95% CI, 12%–45%) than in arm B (64%; 95% CI, 44%–81%). Objective measures of the response of bone disease to treatment with 89Sr alone have only occasionally been reported, with most patients exhibiting either stable disease (24) or progressive disease (23) on bone scans. In addition, comparison of trials is difficult because of differences in the extent of disease in the patients enrolled, when that extent has been adequately described (38). The response of osteoblastic bone metastases to treatment remains, however, difficult to quantify accurately (39). The National Prostate Cancer Group conducted a series of randomized phase II trials in the 1970s and established criteria for quantifying the response of measurable lesions (18). Our study reports for the first time the results of an objective evaluation of the response of bone disease to 89Sr, using strict, established criteria. However, consideration of other changes in scan findings, not strictly included in the established criteria, could also be worthwhile. In 2 arm A patients who were considered to have progressive disease because of the appearance of new metastases, previously evident metastases (in the pelvis and femur) disappeared, whereas 2 arm A patients who were classified as having stable disease showed a marked and diffuse decrease in tracer uptake in all metastatic sites. On the contrary, in no arm B patients did metastases previously detected on bone scans disappear, and only 1 patient showed a diffuse decrease in tracer uptake after therapy. A retarding effect of cisplatin on bone disease progression was also confirmed by changes in serum AP levels after therapy in the 2 arms. In fact, a significant decrease in AP levels was evident in arm A (P < 0.001), whereas only a marginally significant decrease was observed in arm B (P = 0.06). In addition, this effect was more prolonged in arm A (median, 4 mo) than in arm B (median, 2 mo).
This study did not show significant differences in global survival between the 2 arms, even though bone disease progressed more slowly in arm A. In fact, survival after pain relapse was quite similar in the 2 arms, with a median value of 4 mo in arm A and 3 mo in arm B (P = 0.40), whereas global survival after therapy increased in arm A without reaching statistical significance (P = 0.30) (Figs. 1C and 1D). Accordingly, PSA values had not significantly changed after therapy in either arm. The hazard ratio of arm B to arm A for global survival was 1.26, showing that the relative risk of dying was moderately higher in arm B than in arm A. Further investigation of these results in a larger number of patients could be worthwhile to firmly rule out the chance of a β-error. Another question for future studies to address is whether enrolling patients with less advanced cancer or using more aggressive cisplatin schedules may affect global survival.
Marrow toxicity was only slightly increased by the addition of cisplatin, without significant differences between the 2 arms.
CONCLUSION
A low dose of cisplatin enhances the effect of a standard dose of 89Sr without significantly increasing marrow toxicity. Combined treatment not only significantly improves pain palliation, increasing the response rate and prolonging pain-free survival, but also has a cytostatic effect on bone disease, decreasing the risk of progression.
Acknowledgments
This study was supported in part by grant 96/01/R/40 from the Italian Ministry of Health.
Footnotes
Received Nov. 29, 2000; revision accepted Apr. 9, 2001.
For correspondence or reprints contact: Rosa Sciuto, MD, via della Giuliana 83/a, 00195, Rome, Italy.
E-mail: sciuto{at}ifo.it
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Radium-223: Insight and Perspectives in Bone-metastatic Castration-resistant Prostate Cancer
- Molecular radiotherapy
- Phase II Trial of Consolidation Docetaxel and Samarium-153 in Patients With Bone Metastases From Castration-Resistant Prostate Cancer
- High-Linear Energy Transfer Irradiation Targeted to Skeletal Metastases by the {alpha}-Emitter 223Ra: Adjuvant or Alternative to Conventional Modalities?
- Therapy Tolerance in Selected Patients With Androgen-Independent Prostate Cancer Following Strontium-89 Combined With Chemotherapy
- Intensity of 18Fluorodeoxyglucose Uptake in Positron Emission Tomography Distinguishes Between Indolent and Aggressive Non-Hodgkin's Lymphoma
- First Clinical Experience with {alpha}-Emitting Radium-223 in the Treatment of Skeletal Metastases
- Bone-Seeking Radionuclides For Therapy
- Repeated Bone-Targeted Therapy for Hormone-Refractory Prostate Carcinoma: Randomized Phase II Trial With the New, High-Energy Radiopharmaceutical Rhenium-188 Hydroxyethylidenediphosphonate
- Radioisotope Therapy and Clinical Trial Design: The Need for Consensus and Innovation