


Abstract
This study was designed to examine the relationships between the uptake of 14C-deoxyglucose (DG) and the uptake of 201Tl in a rat model of autoimmune myocarditis. Methods: Autoimmune myocarditis was induced in normal rats by immunization with pig cardiac myosin. Dual-tracer autoradiography with DG and 201Tl was performed on frozen slices of the animals’ hearts 3 wk (acute phase), 8 wk (subacute phase), and 14 wk (chronic phase) (each n = 5) after immunization. The extent of inflammatory damage was classified histologically into three categories on the basis of cell infiltration: mild (Mi), moderate (Mo), and severe (Sv). The regional count in the region of interest set on the autoradiogram was normalized on the basis of that of control rats. The ratio of total cardiac uptake to the injected dose (%ID/g × BW, where ID is injected dose and BW is body weight) was calculated by tissue counting. Expressions of glucose transporters GLUT1 and 4 were evaluated by the enzyme-labeled antibody method. Results: The total cardiac uptake of DG in the acute phase of myocarditis was significantly higher than in normal control rats (3.43% ± 0.92% vs. 0.97% ± 0.38%; P < 0.0001); it then decreased in the chronic phase but was still higher than in the controls (1.85% ± 0.37% vs. 0.97% ± 0.38%; P < 0.01). The total cardiac uptake of 201Tl in the acute phase of myocarditis was significantly lower than in the controls (7.4% ± 0.7% vs. 12.0% ± 3.3%; P < 0.005); it then increased in the chronic phase and reached normal levels (13.0% ± 3.3% vs. 12.0% ± 3.3%; not significant [NS]). In the acute phase, the regional uptakes of DG in the Mi, Mo, and Sv regions were 143.1% ± 107.9%, 169.6% ± 59.9%, and 317.5% ± 103.3%, respectively, whereas those of 201Tl were 88.4% ± 31.9%, 72.1% ± 34.6%, and 48.4% ± 21.5%, respectively. GLUT expression was evaluated visually and classified into four grades (0, 1, 2, and 3). In the acute phase, GLUT1 expression was higher in rats in the Sv group than in the controls (2.87 vs. 0.87). GLUT4 was not expressed in the Sv areas but was found in the Mi areas. Conclusion: In the acute phase of autoimmune myocarditis in rats, cardiac uptake of DG was accelerated by severe inflammation. Cardiac uptake of 201Tl, on the other hand, was suppressed. Our results suggest that GLUT1 expression accelerates DG uptake by cells in areas of severe inflammation.
The prognosis of myocarditis patients depends greatly on both a diagnosis in the early stage and the initial treatment. The clinical symptoms and signs are often nonspecific, and conventional examinations for myocarditis, such as electrocardiograms, serum cardiac enzymes, and chest radiographs, are insensitive (1). The most specific changes in the heart that characterize myocarditis are the presence of numerous infiltrating cells and the appearance of giant cells (2). However, histologic methods require invasive procedures that carry a risk of accidental injury, making noninvasive diagnostic methods important for patients with myocarditis. Previous reports on myocarditis have included diagnostic studies with 99mTc-pyrophosphate (3), 67Ga-citrate (4,5), 131I-antimyosin monoclonal antibody (5), and 111In-antimyosin Fab (4,6); FDG PET also detects inflammation (7,8). It has been proposed that FDG PET is more sensitive than other methods in detecting inflammation in the diagnosis of myocarditis.
This study assessed changes in glucose metabolism based on myocardial damage in the acute, subacute, and chronic phases of autoimmune myocarditis in rats by performing dual-tracer autoradiography with 14C-deoxyglucose (DG) and 201Tl on the hearts of affected animals.
MATERIALS AND METHODS
Induction of Autoimmune Myocarditis in Rats
Experimental myocarditis was induced in rats by immunizing them with cardiac myosin, as described previously (9). Cardiac myosin was purified from the porcine ventricular myocardium and was used as the antigen. It was dissolved to a concentration of 20 mg/mL in phosphate-buffered saline containing 0.3 mol/L KCl; then it was mixed with an equal volume of complete Freund’s adjuvant containing 11 mg/mL Mycobacterium tuberculosis (Difco Laboratories, Detroit, MI). The antigen–adjuvant emulsion (0.2 mL) was injected subcutaneously into the footpads of Lewis rats (8-wk-old males; Charles River Japan, Inc., Yokohama, Japan). Control rats received 0.1 mL saline mixed with an equal volume of complete Freund’s adjuvant. Rats were maintained under specific pathogen-free conditions in facilities for comparative medicine and animal experimentation at the Osaka University Graduate School of Medicine.
Biodistribution Study of 201Tl and DG
All rats fasted for more than 12 h before the studies. Three weeks (acute phase), 8 wk (subacute phase), and 14 wk (chronic phase) after immunization, rats were anesthetized with 1.0% isoflurene using a small animal anesthetizer (model TK-4; Bio Machinery, Funabashi, Japan). DG (370 kBq; Dupont NEN, Boston, MA) was injected through the tail vein, and 201Tl (18.5 MBq; Nihon Mediphysics, Nishinomiya, Japan) was injected 30 min later. 201Tl activity was measured with a γ scintillation counter (Curiementor 2; PTW-FREIBURG, Freiburg, Germany). Rats were killed by injection of saturated KCl 10 min after the 201Tl injection. The heart was excised, placed on filter paper, and weighed. The basal half of the heart was cut into small samples, and these samples were carefully weighed.
Myocardial uptake of 201Tl was measured with a γ counter (Auto-Gamma 5000; Packard, Meriden, CT) and calculated as follows:

 where ID is injected dose, BW is body weight, and HW is heart weight.
where ID is injected dose, BW is body weight, and HW is heart weight.
One month after the rats were killed, which was sufficient time for 201Tl to decay, the sample was dissolved in 2 mL tissue solubilizer (Soluene-350; Packard, Downers Grove, IL). On complete dissolution, 12 mL liquid scintillator fluid (Hionic-fluor; Packard) were added to the sample, and β radioactivity was measured with a liquid scintillation counter (model 1414; Wallac Oy, Turku, Finland). Myocardial uptake of DG was calculated with the same equation used for 201Tl uptake above.
Dual-Tracer Autoradiography
The same heart groups used in the biodistribution study were also prepared for autoradiography. Dual-tracer autoradiography with 201Tl and DG was performed in the acute, subacute, and chronic phases. Rats were initially injected intravenously with 370 kBq DG and then with 18.5 MBq 201Tl 30 min later. Ten minutes after the 201Tl injection, the rats were killed by injection of saturated KCl. The heart was rapidly excised, rinsed with saline, and incised in the midline. The apical side of the heart was rapidly embedded in Tissue Mount (Chiba Medical, Soka, Japan) and frozen in n-hexane cooled with dry ice. The frozen tissue was cut into 20-μm-thick sections perpendicular to the short axis of both ventricles with a cryostat at −20°C. The sections were mounted on a clean glass slide and quickly air-dried. To visualize 201Tl, the specimens were exposed to an imaging plate (BAS-SR 2025; Fuji Photo Film Co., Ltd., Tokyo, Japan) for 30 min. One month after the rats were killed, which was sufficient time for 201Tl to decay, the same section was exposed to an imaging plate for 3 d to visualize DG. Microscales of DG (Nycomed Amersham, Buckinghamshire, U.K.) were used to quantitate the regional DG uptake, and the image data were analyzed with a computerized imaging analysis system (BAS 5000 Mac; Fuji). Regions of interest (ROIs) (0.08 mm2) were set on each autoradiogram, and the average count of all ROIs was calculated to quantitate the regional uptakes of 201Tl and DG.
Histopathologic Assessment
Consecutive 5-μm-thick myocardial tissue slices were cut and stained with hematoxylin and eosin. The extent of inflammatory cell infiltration and myocyte necrosis was evaluated by two independent observers.
The specimens were classified, according to the histologic degree of infiltration as follows: mild (a few infiltrating cells in a section), moderate (numerous infiltrating cells in a section but with the area of infiltration not exceeding 0.20 mm2), and severe (numerous infiltrating cells in a section with the area of infiltration exceeding 0.20 mm2) (Fig. 1).
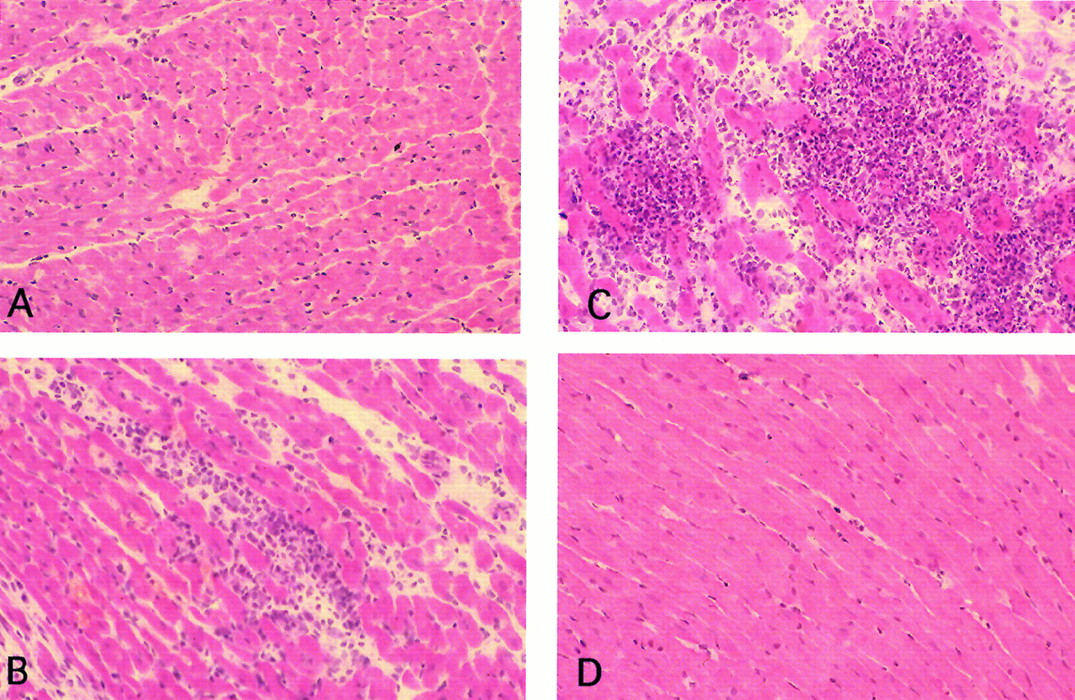
Pathologic grading of extent of inflammatory damage. Mild damage (A), moderate damage (B), severe damage (C), and normal control (D). (×200).
Immunohistochemistry
The 5-μm sections were stained with polyclonal anti-GLUT1 and anti-GLUT4 antibodies (rabbit anti-GLUT1 AB 1340, anti-GLUT4 AB 1346; Chemicon International, Inc., Temecula, CA). The sections were incubated with anti-GLUT1 and anti-GLUT4 antibodies after preincubation with H2O2 and goat albumin and then incubated with biotinylated antirabbit immunoglobulin (IgG) (second antibody; Vector Laboratories, Burlingame, CA). Finally, the bound antibody was visualized with horseradish peroxidase streptavidin (Vector). Consecutive sections incubated with normal rabbit IgG were used as negative controls, and sections from normal nonfasted rats were used as positive controls.
GLUT expression was visually evaluated and divided on the basis of microscopic findings into the following four grades: 0, no expression; 1, minimal expression; 2, expression between those of 1 and 3; and 3, the strongest expression seen in any of the specimens.
Statistical Analysis
Data are expressed as the mean ± SD. Groups were compared by ANOVA with a multiple comparison test. A value of P < 0.05 was considered to indicate a statistically significant difference.
RESULTS
Body Weight and Heart Weight
In both the acute and subacute phase (each n = 5) of myocarditis, body weight was significantly lower than in the control rats (225.9 ± 15.8 g [acute] vs. 322.8 ± 17.7 g; 309.8 ± 26.7 g [subacute] vs. 386.8 ± 31.2 g; P < 0.0001). In the chronic phase, however, body weight was not significantly different from that of the controls (395.1 ± 40.1 g vs. 413.6 ± 32.0 g; not significant [NS]). In both the acute and the chronic phase, heart weight was significantly greater than in the controls (2.0 ± 0.5 g [acute] vs. 1.0 ± 0.1 g; P < 0.0001; 1.8 ± 0.6 g [chronic] vs. 1.1 ± 0.1 g; P < 0.0001).
Total Cardiac Uptakes of DG and 201Tl
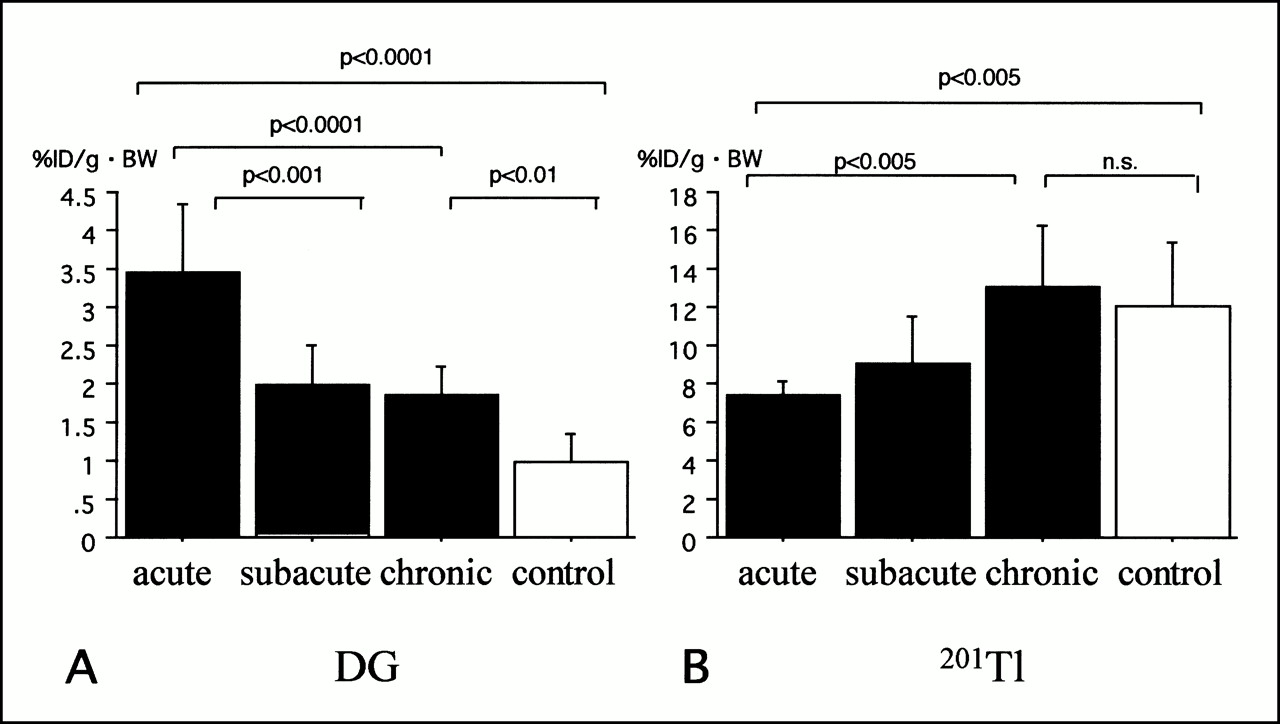
The total cardiac uptake of DG in the acute phase of myocarditis (n = 5) was significantly increased in comparison with the control uptake (n = 5) (3.43% ± 0.92% vs. 0.97% ± 0.38%; P < 0.0001). In the subacute phase, the total DG uptake was significantly decreased in comparison with the acute phase (1.97% ± 0.53% vs. 3.43% ± 0.92%; P < 0.001). A decrease was seen in the chronic phase (n = 5), but the total DG uptake was still higher than in the controls (1.85% ± 0.37% vs. 0.97% ± 0.38%; P < 0.01). The total 201Tl uptake in myocarditis was significantly reduced in comparison with that of the controls in the acute phase (7.4% ± 0.7% vs. 12.0% ± 3.3%; P < 0.005), but it recovered to the control uptake in the chronic phase (13.0% ± 3.3% vs. 12.0% ± 3.3%; NS) (Fig. 2).

Total cardiac uptakes of DG (A) and 201Tl (B) in acute, subacute, and chronic phases of myocarditis. Open and closed bars indicate average values of all phases in controls and myocarditis, respectively.
Regional Uptakes of DG and 201Tl
Acute-phase autoradiograms of DG and 201Tl are shown in Figures 3A and B, and chronic-phase autoradiograms are shown in Figures 3C and D.

Dual-tracer autoradiograms of myocardium in acute (A and B) and chronic (C and D) phases of autoimmune myocarditis. Arrowheads denote sites of severe infiltration corresponding to areas of high GLUT1 expression. DG image (A and C) and 201Tl image (B and D).
In the acute phase, the myocardial distribution of DG was different from that of 201Tl. The regional myocardial uptake in each ROI was normalized by that of the corresponding control. DG uptake was increased significantly in the area of severe inflammation in comparison with the controls (317.5% ± 103.3% vs. 100% ± 46.4%; P < 0.0005), but it was not increased in the areas of moderate (169.6% ± 59.9%) and slight (143.1% ± 107.9%) inflammation. Most of the areas with high DG uptake were located within the inflammatory foci. A few areas of high DG uptake were located at normal myocardial areas. In these areas, 201Tl uptakes were within the normal limit without exception. In the subacute phase, no areas of severe inflammation were found. In the moderate inflammation areas, DG uptake was significantly increased in comparison with the controls (367.1% ± 175.4% vs. 100% ± 12.8%; P < 0.0005). In the chronic phase, there were no severe inflammatory foci, but some areas of high DG uptake were observed in the pericardium. Regional DG uptake in the moderate infiltration areas was similar to that of the controls (129% ± 43% vs. 100% ± 48%; NS) (Table 1).
Regional Uptakes of DG and 201T1
201Tl uptake in the acute phase gradually decreased in parallel to the subsiding of inflammation and recovered to the control level in areas of mild infiltration (88.4% ± 31.9% vs. 100.0% ± 11.4%; NS). In the subacute phase, the regional 201Tl uptake was restored to the normal level in areas of moderate and mild infiltration (83.7% ± 23.1% [moderate] vs. 100.0% ± 23.0%; NS; 109.5% ± 27.2% [mild] vs. 100.0% ± 23.0%; NS). In the chronic phase, the regional 201Tl uptake in the moderate and mild infiltration areas did not differ from that of the controls (76.6% ± 29.6% [moderate] vs. 100.0% ± 7.5%; NS; 100.2% ± 25.4% [mild] vs. 100.0% ± 7.5%; NS) (Table 1).
Expressions of GLUT1 and GLUT4
In the acute phase of myocarditis, scattered inflammatory foci of various sizes were observed in the myocardium and some overlapped sites of GLUT1 expression (Figs. 4A and B). Moreover, some of the GLUT1 expression sites also corresponded to areas of high DG uptake (Fig. 3A). Areas of myocardium with few infiltrating cells, on the other hand, corresponded to GLUT4 expression sites (Fig. 4C).
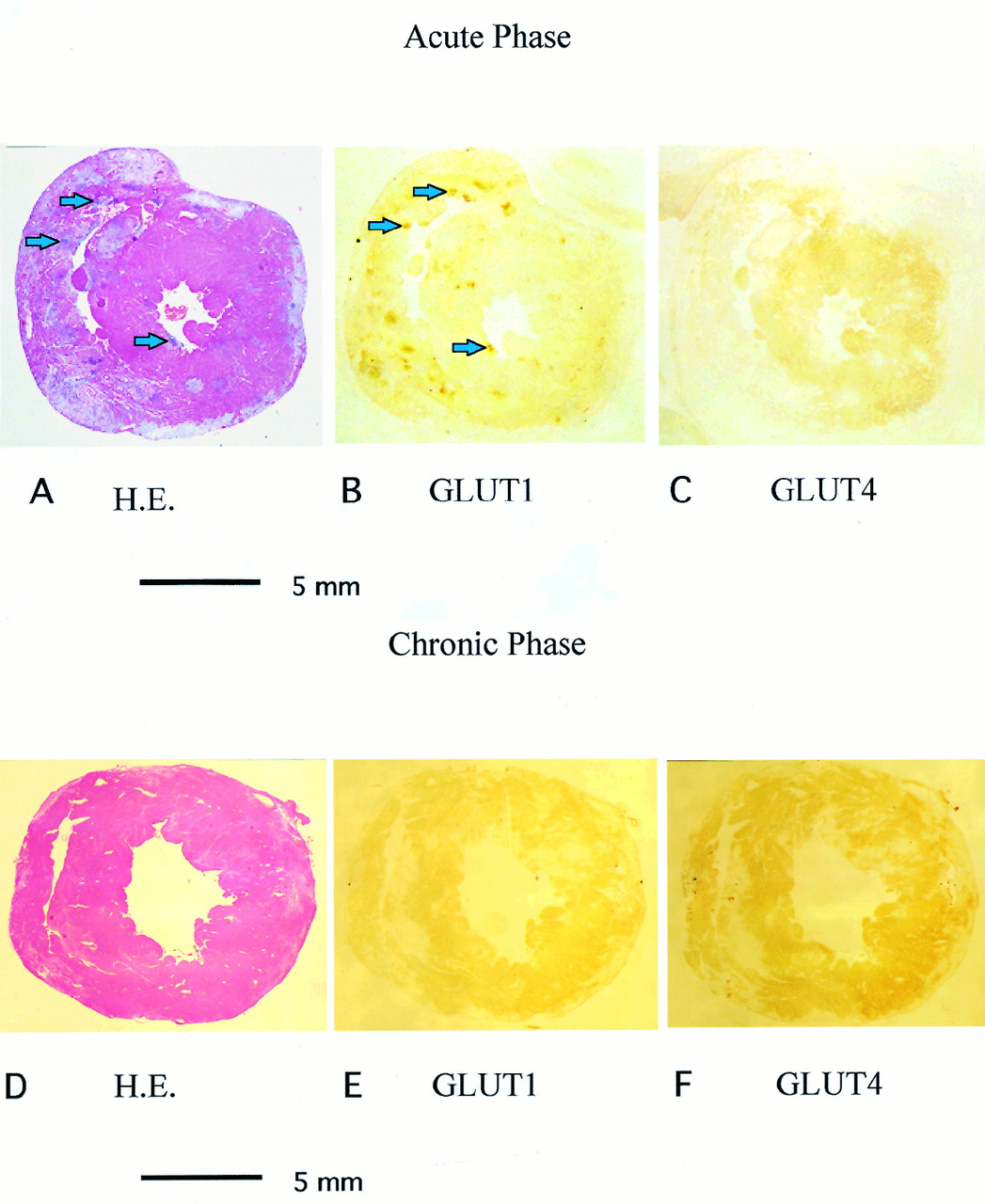
Microscopic findings in acute (A–C) and chronic (D–F) phases of myocarditis. Hematoxylin and eosin (H.E.) staining (A and D), GLUT1 (B and E), and GLUT4 (C and F). Arrowheads indicate sites of high DG uptake (×1).
In the chronic phase, all foci of infiltration were replaced by fibrosis. No foci of severe inflammation were observed, and GLUT1 and GLUT4 were expressed homogeneously throughout the section except in areas with scarring (Figs. 4D–F).
Regional analysis showed grade 3 GLUT1 expression, especially in the areas of severe infiltration in the acute phase (2.87 ± 0.30 vs. 0.87 ± 0.30; P < 0.0001). In the chronic phase, typical GLUT1 findings were absent (Table 2).
Visual Evaluation of Regional GLUT1 and GLUT4 Expressions
Grade 2 expression of GLUT4 was observed in the areas of mild infiltration in the acute phase (1.87 ± 0.30 vs. 1.07 ± 0.15; P < 0.0005). In the chronic phase, typical GLUT4 findings were absent (Table 2).
DISCUSSION
We investigated myocardial damage in myocarditis using ex vivo dual-tracer autoradiography with DG and 201Tl. The uptakes of DG and 201Tl varied with the severity of inflammation, and neither showed homogeneous uptake. These findings suggest that FDG PET and myocardial SPECT with 201Tl are potentially useful for assessing the severity of myocarditis.
In previous studies, the positive scintigraphic tracers 99mTc-pyrophosphate (3), 67Ga-citrate (4,5), 131I-antimyosin monoclonal antibody (5), and 111In-antimyosin Fab (4,6) were shown to be capable of detecting myocarditis. Furthermore, 99mTc-pyrophosphate can detect myocardial necrosis. However, the inability of 99mTc-pyrophosphate to detect either the center of a necrotic focus or its margin is problematic. 67Ga-citrate can detect inflammation but with unsatisfactory sensitivity. 111In-antimyosin Fab was found to be capable of detecting myocarditis in a previous experiment and a clinical study. Yasuda et al. (6) reported the sensitivity of 111In-antimyosin Fab in detecting myocarditis to be 61%. The problem with 111In-antimyosin Fab is that image acquisition is a 48-h process. There have been no clinical reports on the detection of myocarditis in the acute phase by FDG PET. However, inflammatory cells in tissue can be detected by FDG (7,8), and FDG PET is reportedly more useful than 67Ga-citrate in making a diagnosis of sarcoidosis (8). Consequently, FDG PET is considered to be better than the other methods for detecting early inflammatory change.
The total cardiac DG uptake was significantly higher in rats with myocarditis than in control rats, and the histologic findings showed DG uptake to be much higher in areas of severe inflammation than in areas of slight inflammation. The expression of GLUT1 was significantly increased in areas of severe infiltration in the acute phase. Severe infiltration was observed in hearts affected by myocarditis; infiltrating cells were thus considered to be primarily responsible for the increase in DG uptake. In contrast, 201Tl uptake was significantly lower than in normal controls.
In cardiac specimens from rats with acute-phase myocarditis, which were stained with hematoxylin and eosin, areas of severe cell infiltration merged and produced foci. GLUT1 was mainly expressed in inflammatory foci, whereas GLUT4 was expressed in the myocardium with minimal cellular infiltration. The locations of inflammatory foci corresponded to areas showing GLUT1 expression and high DG uptake. This observation was considered to indicate that the infiltrating cells increased DG uptake through enhanced GLUT1 expression. Total cardiac uptake of DG also depended on the number of infiltrating cells. In contrast, little 201Tl uptake occurred in the inflammatory foci. The 201Tl kinetics depend on the Na/K pump in the cell membrane (10), suggesting that none of the myocardial cells within the foci had functioning Na/K pumps in their cell membranes. Thus, the finding of low 201Tl uptake can be considered an indication of myocardial cell damage.
In the acute phase of myocarditis, DG uptake definitely depended on the extent of cell infiltration, whereas in the subacute and chronic phases, it was increased in comparison with the controls despite the small number of infiltrating cells. Heart failure increases the levels of plasma catecholamines and insulin, and these hormonal factors have been suggested to alter myocardial metabolism (11,12). 201Tl uptake is thought to have been restored to the control level because Na/K pump function in the myocardium recovered.
In the clinical setting, FDG PET and 201Tl SPECT are excellent methods for detecting myocardial ischemia, myocardial viability, and myocardial damage. Although FDG uptake does not usually occur in normal myocardium during fasting, ischemia induces translocation of GLUT1 and GLUT4 in the myocardium (12), and FDG uptake consequently increases in ischemic myocardium. In our experiment, however, infiltrating cells showed an apparent increase in cardiac DG uptake during myocarditis. No relationship was seen between ischemia caused by coronary stenosis and this increased DG uptake. Clinically, high FDG uptake does not always reflect ischemia in the myocardium, but it is possible that infiltrating cells are responsible for the increased FDG uptake in the setting of myocarditis. Heterogeneous distribution of FDG sometimes is seen for unknown reasons in the healthy subject after fasting (13). It is difficult to discriminate between normal myocardium and infiltration cells in myocarditis in subacute and chronic phases. In the acute phase in this study, however, the area with high FDG uptake and low 201Tl uptake occurred at the area of infiltrating cells. The detection of infiltration foci in myocarditis in the acute phase is a significant finding.
CONCLUSION
The results of our study show increased cardiac DG uptake in the acute phase of autoimmune myocarditis, whereas 201Tl uptake is decreased. The increased DG uptake in the acute phase was caused by increased GLUT1 expression in the infiltrating cells. Therefore, FDG can be used as a positive tracer to detect myocarditis, and 201Tl can be used as a negative tracer. The combination of FDG and 201Tl can show clearly whether or not severe infiltration is present in acute myocarditis.
Footnotes
Received Mar. 15, 2000; revision accepted Aug. 14, 2000.
For correspondence or reprints contact: Tsunehiko Nishimura, MD, PhD, Division of Tracer Kinetics, Biomedical Research Center, Osaka University Graduate School of Medicine, (D9) 2-2 Yamada-oka, Suita, Osaka 565-0871, Japan.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.