


Article Figures & Data
Figures
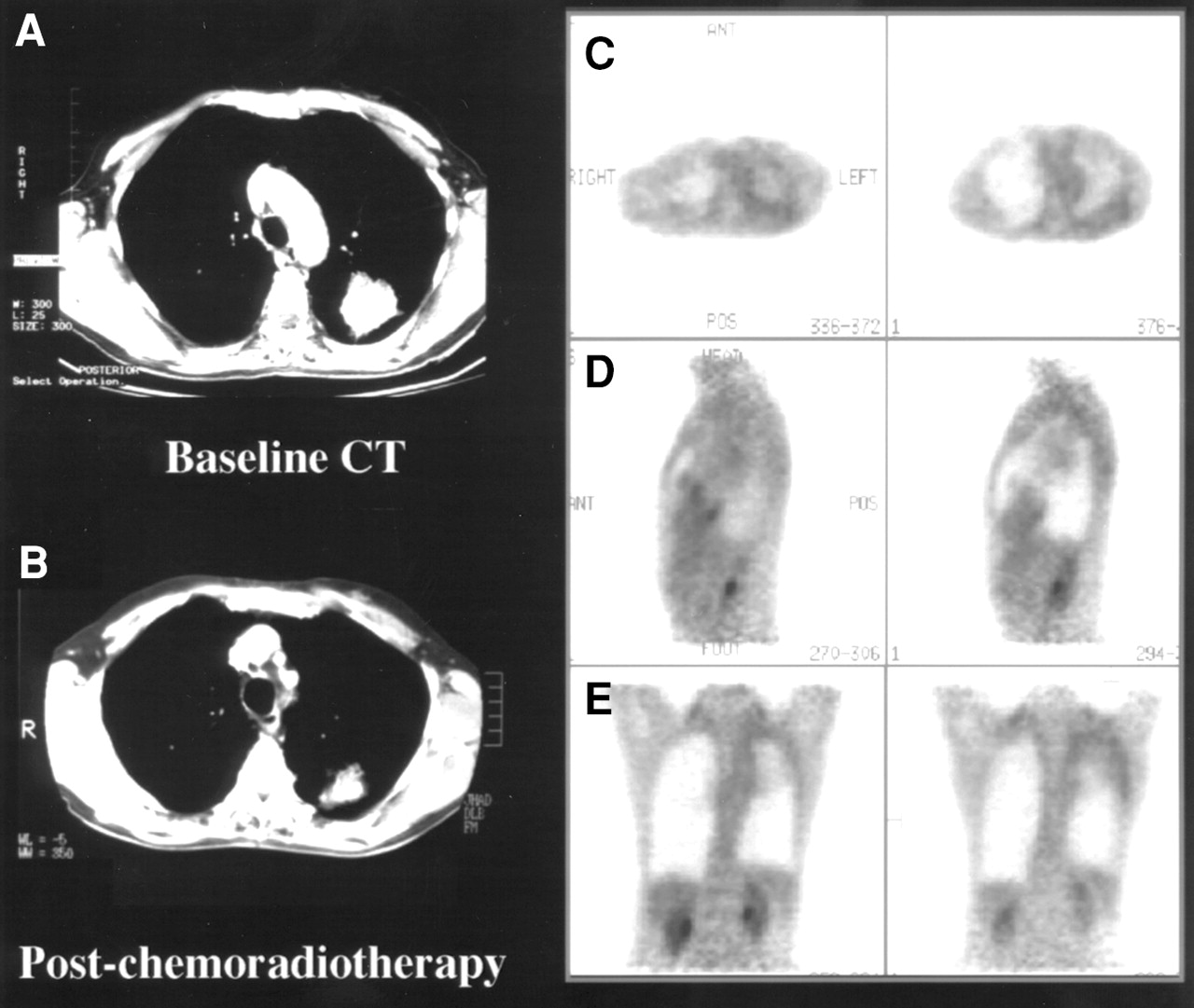
- FIGURE 1.
Hemoptysis and residual mass 9 mo after radical chemoradiotherapy for left upper lobe NSCLC suggested local relapse despite partial CT response between baseline (A) and posttreatment (B) scans. Representative transaxial (C), sagittal (D), and coronal (E) planes of PET scan showed low-grade pleural changes consistent with postradiotherapy effects but no evidence of recurrent disease. Palliative radiotherapy was cancelled, and patient remained well >12 mo after PET without evidence of active disease.
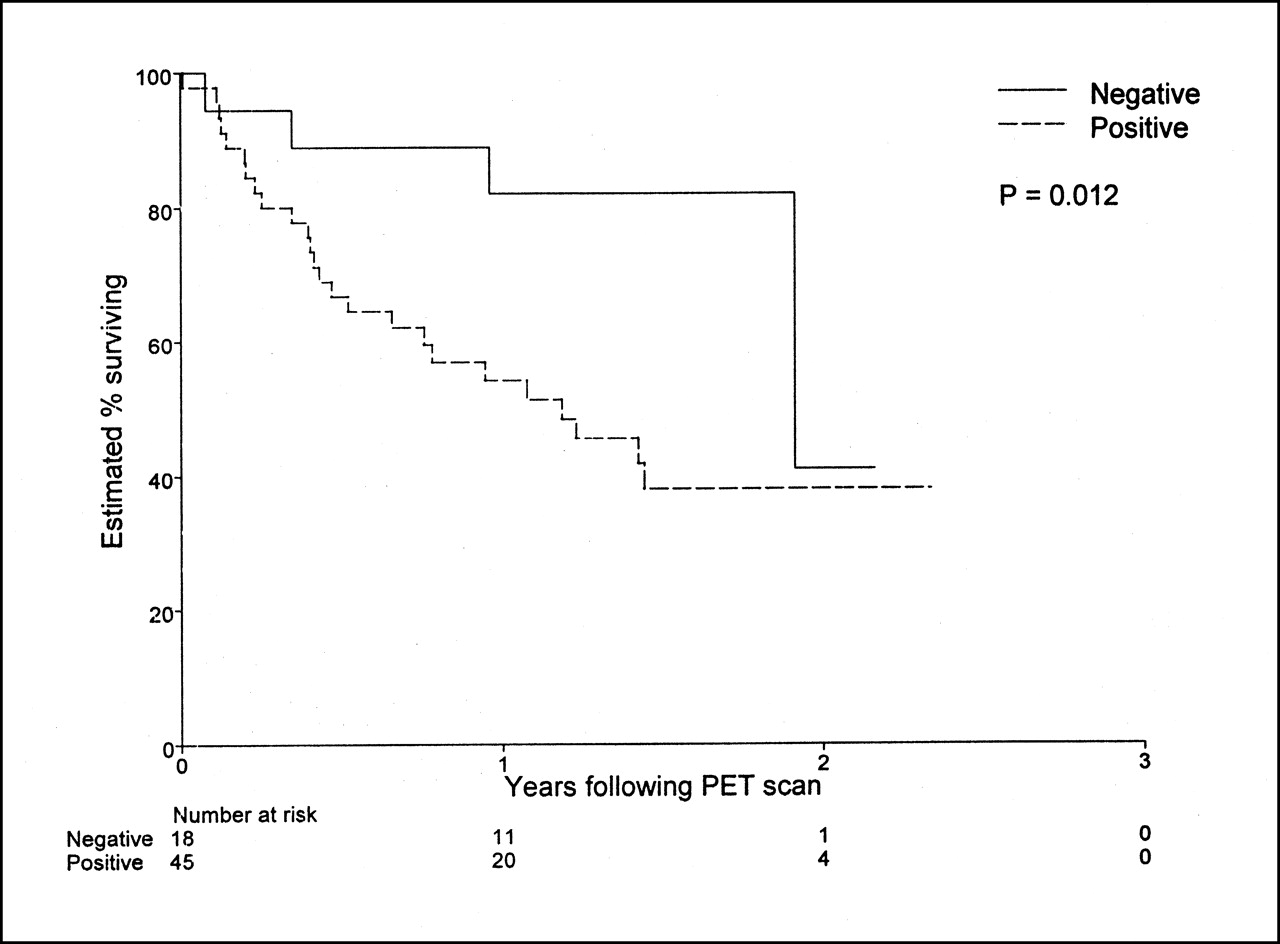
- FIGURE 2.
Graph shows strong prognostic stratification by whether PET was positive or negative for relapse in 63 consecutive patients in whom relapse was suspected on basis of conventional imaging findings (n = 61) or clinical features (n = 2).
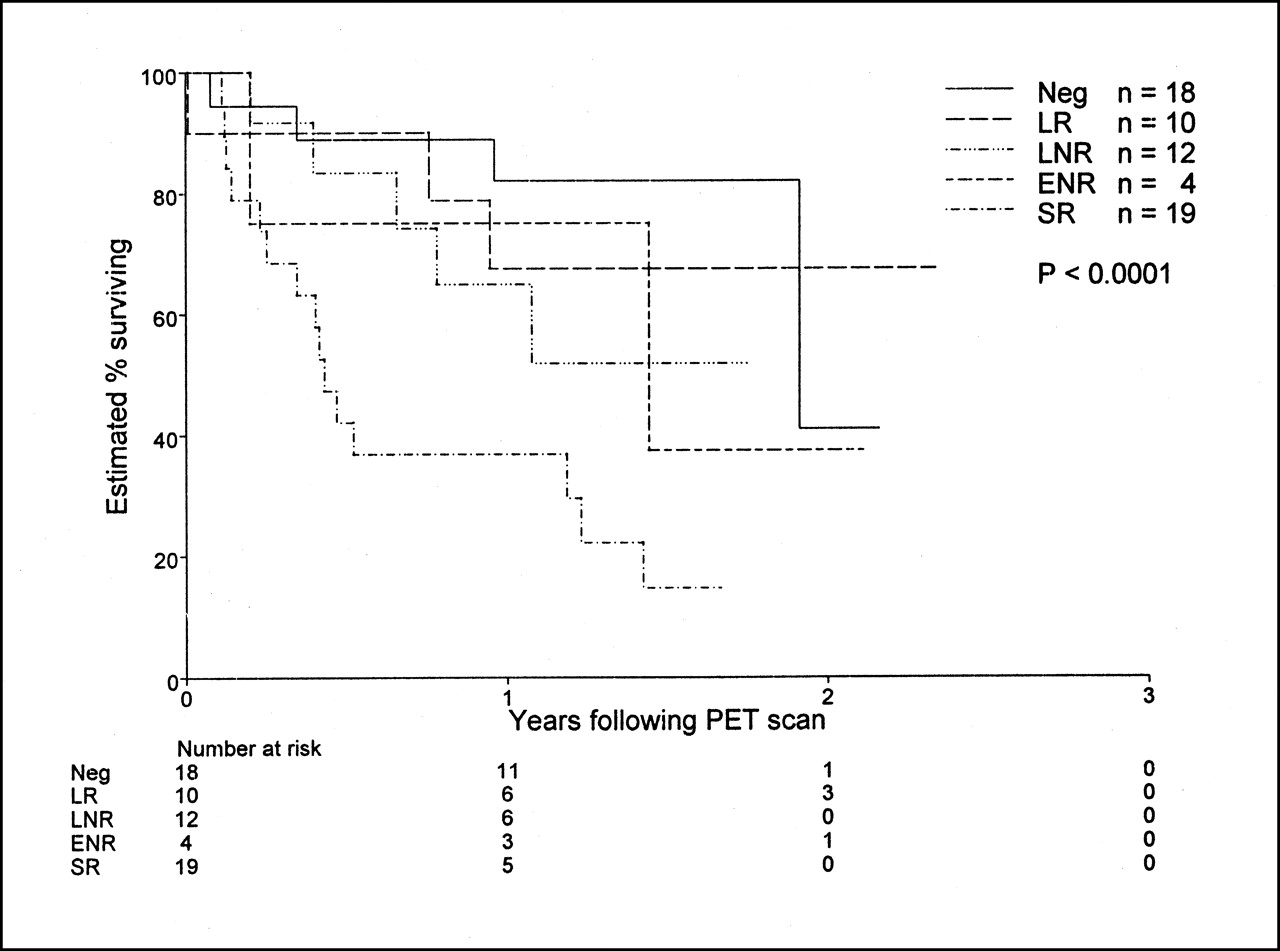
- FIGURE 3.
Graph shows strong relationship between apparent extent of disease on PET scanning and survival in 63 consecutive patients in whom relapse was suspected on basis of conventional evaluation. This relationship remained significant after adjusting for pre-PET evaluation of extent of disease relapse or for treatment subsequently delivered. ENR = extensive nodal relapse; LNR = limited nodal relapse; LR = local relapse; SR = systemic relapse.

Tables
CSI extent of relapse* PET extent of relapse* % Less disease by PET % Same status % More disease by PET Neg LR LNR ENR SR Total Neg 2 0 0 0 0 2 0 100 0 LR 4 7 4 0 6 21 19 33 48 LNR 7 2 6 3 10 28 32 21 46 ENR 2 0 2 1 0 5 80 20 0 SR 3 1 0 0 3 7 57 43 0 Total 18 10 12 4 19 63 33 30 37 ↵* Data are numbers of patients.
CSI = conventional restaging investigations; Neg = negative; LR = local relapse; LNR = localized nodal relapse; ENR = extensive nodal relapse; SR = systemic relapse.
- TABLE 2
Concordance and Validation of Pre-PET and Post-PET Extent of Suspected Relapse Grouped by Impact of PET Scan
CSI/PET validation Impact of PET scan High (n = 40) Medium (n = 8) Low (n = 13) None (n = 2) Total Concordant 9 3 7 0 19 Both correct 8 1 2 0 11 Neither correct 1 0 1* 0 2 Not assessable 0 2 4 0 6 Discordant 31 5 6 2 44 PET correct 25 3 2 1 31 CSI correct 1 0 0 0 1 Both incorrect 2† 0 2‡ 0 4 Not assessable 3 2 2 1 8 ↵* Local recurrence was pathologically confirmed at salvage surgery, but adrenal metastasis developed at this location 4 mo after findings were negative on PET and CT.
↵† In both patients, PET correctly excluded relapse at suggestive site found on CT but was incorrect at another site.
↵‡ One patient had false-positive findings on both CT and PET because of changes after radiotherapy, and patient had only equivocal lung metastasis (2 mm) found on CT and was also understaged by PET.
CSI = conventional restaging investigations.
- TABLE 3
Summary of 40 Patients for Whom PET Changed Treatment Intent or Modality (High Impact)
Pre-PET plan Post-PET management Total PET −ve (observation) PET +ve Curative Palliative Active Expectant Curative (cSx, rRT) — — 6 — 6 (2, 4) Invasive diagnosis 1 1 1 2 5 Expectant palliative 6 — 4 — 10 Active palliative (pCT, pRT, pSx) 8* 3 2† 6‡ 19 (4, 13, 2) ↵* Includes 1 patient with false-negative PET result because of claustrophobia.
↵† Includes 2 patients in whom modality of active palliative treatment was changed.
↵‡ Includes 1 patient with false-positive PET result in lower neck in whom suspected local recurrence was correctly excluded.
PET −ve = no suggestive abnormality; PET +ve = abnormality suggestive of relapse; cSx = surgery with curative intent; rRT = radical radiotherapy ± platinum-based chemotherapy; pCT = palliative chemotherapy; pRT = palliative radiotherapy; pSx = palliative surgery without expectation of cure.
“Expectant” refers to withholding of treatment in patients thought to have disease until required for relief of clinical symptoms.
- TABLE 4
Association Between Apparent Extent of Relapse and Survival in 63 Patients with Suspected Relapse of NSCLC
Extent of relapse by … Group No. of patients Hazard ratio 95% CI P* CSI Negative 2 0.00 0.00 (NA) LR 21 1.00 LNR 28 1.13 0.50–2.55 ENR 5 0.81 0.18–3.69 SR 7 0.82 0.22–3.00 0.59 Per increment 1.02 0.72–1.45 0.46† PET Negative 18 1.00 LR 10 1.16 0.26–5.24 LNR 12 2.18 0.58–8.18 ENR 4 1.94 0.35–10.7 SR 19 6.07 1.98–18.6 0.0044 Per increment 1.60 1.24–2.07 <0.0001† Negative 18 1.00 Positive 45 2.95 1.03–8.50 0.012‡ ↵* Based on 2-sided tests unless otherwise indicated.
↵† Indicates test for trend (1-sided test).
↵‡ One-sided test (Fig. 2).
CSI = conventional restaging investigations; NA = not applicable; LR = local relapse; LNR = localized nodal relapse; ENR = extensive nodal relapse; SR = systemic relapse.
Extent of relapse by CSI was relative to LR group, because remaining HRs were otherwise infinite.
- TABLE 5
Association Between Treatment Delivered After PET and Survival in 63 Patients with Suspected Relapse of NSCLC
Group No. of patients Hazard ratio 95% CI P* Specific treatment None 15 1.00 cSx 4 1.55 0.28–8.47 rRT 11 0.54 0.10–2.95 pRT 15 3.76 1.19–11.8 pCT 7 3.23 0.80–13.1 Supportive 9 1.98 0.49–7.93 0.032 Treatment intent None 15 1.00 Curative 15 0.80 0.20–3.21 Palliative 22 3.63 1.19–11.0 Supportive 9 1.98 0.49–7.93 0.011 ↵* Based on 2-sided tests.
cSx = surgery with curative intent; rRT = radical therapy combined with concurrent chemotherapy unless contraindicated; pRT = palliative radiotherapy; pCT = palliative chemotherapy.
Data on treatment given after PET exclude 2 patients who did not receive planned pRT. “Supportive” refers to delay in active management until dictated by symptomatic progression.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Injustice of Being Judged by the Errors of Others: The Tragic Tale of the Battle for PET Reimbursement
- Response Assessment Criteria and Their Applications in Lymphoma: Part 1
- 18F-FDG PET/CT and Lung Cancer: Value of Fourth and Subsequent Posttherapy Follow-up Scans for Patient Management
- Follow-up or Surveillance 18F-FDG PET/CT and Survival Outcome in Lung Cancer Patients
- Improvement in PET/CT Image Quality with a Combination of Point-Spread Function and Time-of-Flight in Relation to Reconstruction Parameters
- Doing More Harm than Good? Do Systematic Reviews of PET by Health Technology Assessment Agencies Provide an Appraisal of the Evidence That Is Closer to the Truth than the Primary Data Supporting Its Use?
- The role of positron emission tomography in the management of non-small cell lung cancer
- From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors
- Partnerships in Oncology and Radiology: The Role of Radiology in the Detection, Staging, and Follow-up of Lung Cancer
- PET Evaluation of Lung Cancer
- Progress and Promise of FDG-PET Imaging for Cancer Patient Management and Oncologic Drug Development
- The Role of PET Scan in Diagnosis, Staging, and Management of Non-Small Cell Lung Cancer
- PET/CT Using 18F-FDG in Suspected Lung Cancer Recurrence: Diagnostic Value and Impact on Patient Management
- Quantification of 18F-FDG Uptake in Non-Small Cell Lung Cancer: A Feasible Prognostic Marker?
- American Society of Clinical Oncology Treatment of Unresectable Non-Small-Cell Lung Cancer Guideline: Update 2003
- Positron Emission Tomography Is Superior to Computed Tomography Scanning for Response-Assessment After Radical Radiotherapy or Chemoradiotherapy in Patients With Non-Small-Cell Lung Cancer
- Use of a Dual-Head Coincidence Camera and 18F-FDG for Detection and Nodal Staging of Non-Small Cell Lung Cancer: Accuracy as Determined by 2 Independent Observers