


Abstract
The goal of this study was to assess the value of hybrid imaging using a combined PET/CT device with 18F-FDG in the diagnosis and clinical management of suspected recurrent lung cancer. Methods: Forty-two patients with non–small cell lung cancer (NSCLC) with suspected recurrence due to new clinical, biochemical, and radiologic findings were prospectively evaluated. PET/CT results were compared with PET interpreted with side-by-side CT data. A final diagnosis of recurrence was confirmed by histologic tissue sampling during surgery or biopsy or by further clinical and radiologic work-up. The impact of PET/CT on patient management was assessed. Results: Twenty-four of 27 positive PET/CT studies (89%) were proven to have recurrent disease. Fourteen of 15 negative PET/CT studies (93%) had no evidence of disease. The sensitivity, specificity, and positive and negative predictive values of PET/CT for diagnosis of recurrence were 96%, 82%, 89%, and 93% compared with 96%, 53%, 75%, and 90%, respectively, for PET. PET/CT changed the PET lesion classification in 22 patients (52%), by determining the precise localization of sites of increased 18F-FDG uptake. PET/CT changed the management of 12 patients (29%) by eliminating previously planned diagnostic procedures (5 patients), by initiating a previously unplanned treatment option (4 patients), or by inducing a change in the planned therapeutic approach (3 patients). Conclusion: In patients with a suspected recurrence of NSCLC, PET/CT provides a better anatomic localization of suspicious lesions compared with PET interpreted with side-by-side CT data. This improved diagnostic performance of PET/CT has a further impact on the clinical management and treatment planning of the patients.
About half of the patients with newly diagnosed non–small cell lung cancer (NSCLC) have localized disease. They are further directed to potentially curative treatment, consisting of surgical resection, radiotherapy, or combined radiochemotherapy with curative intent (1). Follow-up of patients with NSCLC is aimed at early detection of recurrence or of a second lung cancer as well as managing treatment-related complications (2). CT is currently considered the modality of choice for diagnosis of local or distant recurrent lung cancer, due to its wide availability and low cost (3,4). However, detection of early recurrence or a second primary tumor can be a diagnostic challenge with CT. New clinical or imaging findings may be related to recurrent tumor as well as to previous treatment. CT-based diagnosis of treatment-induced necrotic or fibrotic tissue versus viable residual or recurrent cancer is difficult and sometimes impossible (3,5,6). A correct and timely diagnosis would make it possible to initiate therapy sooner or to avoid unnecessary treatment.
18F-FDG PET is a highly sensitive, specific, and accurate imaging modality for diagnosis and preoperative staging of lung cancer (7–9). 18F-FDG PET is also a highly sensitive test for diagnosis of recurrent NSCLC (6,10,11). PET, however, lacks anatomic information and the exact localization of the suspicious findings may be difficult. Treatment-distorted anatomy, as well as increased 18F-FDG uptake in inflammatory posttherapeutic sites, may hamper the correct PET diagnosis of recurrence. This is particularly true early in the course of recurrent disease, when CT findings may be normal in the presence of a small tumor burden.
Hybrid PET/CT makes it possible to sequentially acquire both PET and CT in a single session and to obtain precise fusion of anatomic and functional imaging data. PET/CT has been shown to be of additional value for accurate staging of NSCLC at initial diagnosis compared with PET interpreted with side-by-side CT (12). Because of the limitations of CT for the diagnosis of tumor recurrence and the difficult localization of metabolic changes found on PET, hybrid imaging may have a clinically significant role in the evaluation of patients with NSCLC after initial treatment with curative intent.
This study was designed to assess the role of PET/CT using 18F-FDG and to compare it to the performance of PET for the diagnosis and subsequent clinical management of patients with suspected recurrent lung cancer.
MATERIALS AND METHODS
Patient Population
Forty-two consecutive patients with NSCLC in whom recurrent disease was suspected, because of new clinical, biochemical, or imaging findings, were prospectively evaluated using PET/CT between July 2001 and June 2002. Eligibility criteria included (a) histologically confirmed NSCLC, (b) no evidence of active malignancy for at least 6 mo after initial therapy, and (c) uncertain diagnosis of recurrent disease or its extent after routine clinical and CT work-up. The institutional Ethics Committee approved the study protocol and all patients gave their informed consent.
There were 28 men and 14 women, with a mean age of 66 y (range, 35–82 y). The clinical characteristics of the patient population are presented in Table 1. High-resolution, contrast-enhanced CT of the chest and the upper abdomen was performed in all 42 patients 1–13 wk before the PET/CT study (average, 4 wk). In 31 patients, the suspicion for recurrence was based on new abnormal or equivocal imaging findings. In 6 of the 42 patients, recurrence was suspected due to the onset of new clinical symptoms with no evidence of recurrent disease on routine imaging work-up. In 5 patients, tumor recurrence was suspected due to the asymptomatic finding of elevated serum tumor markers (carcinoembryonic antigen in 4 patients and an incidental finding of elevated cancer antigen 125 in 1 patient) without abnormal imaging studies (Table 2).
Clinical Characteristics of 42 Patients with Suspected Recurrent NSCLC
Indications for PET/CT Study in 42 Patients with Suspected Recurrent NSCLC
PET/CT Acquisition and Processing
Patients were instructed to fast, except for glucose-free oral hydration, for 4–6 h before the injection of 370–555 MBq (10–15 mCi) 18F-FDG. Blood glucose was measured before injection of the tracer to ensure glucose blood levels of <200 mg/dL. After injection of the tracer, patients were kept lying comfortably. No urinary bladder catheterization was performed and no oral muscle relaxants were administered. Whole-body PET and non–contrast-enhanced CT were acquired consecutively 1 h after the injection, using a PET/CT system (Discovery LS; General Electric Medical Systems), combining a third-generation multislice spiral CT scanner with a dedicated full-ring PET scanner with bismuth germanate crystals. The PET and CT devices are mechanically aligned back to back and share a common table. Proper registration of the 2 images is ensured by shared positional information of the table and the patient for both the CT and the PET acquisitions. Data obtained from the CT was used for low-noise attenuation correction of PET emission data and for fusion with attenuation-corrected PET images. PET images were reconstructed iteratively using ordered-subset expectation maximization software. PET, CT, and fused PET/CT images were available for review, displayed in axial, coronal, and sagittal planes. The PET data were displayed as noncorrected and attenuation-corrected images and also in a rotating maximum intensity projection.
Interpretation and Analysis of PET/CT Images
All studies were interpreted prospectively and reviewed with knowledge of the patient’s clinical history and results of previous imaging studies, performed from initial diagnosis to the time when suspicion for recurrence arose. Two experienced nuclear medicine physicians, aware of the clinical history and results of previously performed imaging tests, initially interpreted the stand-alone 18F-FDG PET images. PET images were reviewed with data of previously performed contrast-enhanced CT and the CT component of the hybrid imaging study available for side-by-side evaluation. The PET study was interpreted as negative when no areas of abnormal 18F-FDG uptake were seen. Every focus of increased 18F-FDG uptake was recorded and classified as malignant, equivocal, or benign on the basis of the shape, size, and intensity of the uptake. A site of increased 18F-FDG uptake was defined as benign and unrelated to cancer when it was located in an area of known physiologic biodistribution of the tracer or in a known nonmalignant process. When focal 18F-FDG uptake, with intensity higher than that of surrounding tissues, was seen in areas unrelated to physiologic or benign processes, it was defined as malignant. Any other area of increased 18F-FDG uptake that could not be clearly characterized was defined as equivocal. A PET study showing at least 1 site of abnormal 18F-FDG uptake characterized as malignant was defined as positive. PET studies with all lesions defined as equivocal or benign were interpreted as equivocal or negative, respectively.
A combined team of nuclear medicine physicians and a chest radiologist interpreted the fused PET/CT images after completion of the PET review. Changes in lesion definition and localization provided by PET/CT were recorded. Fused images were considered to provide additional information when they led to a change in the initial characterization or localization of sites of increased 18F-FDG uptake as previously assessed by the PET study reviewed with side-by-side CT data. PET/CT was also found to be contributory when it led to the retrospective detection of lesions on the prior high-resolution, contrast-enhanced CT scans. These lesions had been missed during the independent reading of the visual side-by-side comparison of the PET and CT studies. PET/CT images were also evaluated for the presence of misregistration or respiratory motion artifacts.
A final diagnosis of recurrence was confirmed by histologic tissue sampling during surgery or biopsy or by a decision of the referring clinical team, which included oncologists and thoracic surgeons. Exclusion of recurrent malignancy was based on histologic findings or on a clinical and radiologic follow-up period of at least 18 mo with no evidence of active malignancy.
Performance of PET and PET/CT for image interpretation was compared on a per-patient basis. A true-positive PET or PET/CT study showed at least 1 site of abnormal or equivocal 18F-FDG uptake that was further confirmed to be malignant. A patient with abnormal 18F-FDG uptake on PET or PET/CT who had no evidence of active disease on biopsy or other imaging modalities, or a negative clinical follow-up of at least 18 mo, was classified as a false-positive study. A negative PET or PET/CT study in a patient who showed no evidence of active cancer for at least 18 mo was defined as a true-negative study. A negative PET or PET/CT study in a patient who had further evidence of active disease was defined as a false-negative study. The sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) for PET and PET/CT were calculated using standard definitions. The differences in performance between PET and PET/CT were compared using the McNemar test for paired proportions, with P < 0.05 considered to be statistically significant.
The role of hybrid imaging in patient management was evaluated. Changes in the clinical decision making induced by PET/CT were reviewed for each patient by the referring clinical team as part of the study protocol. PET/CT was considered to be of value if it provided additional information that eliminated the need for previously planned diagnostic procedures or if it resulted in the initiation of previously unplanned treatment or changed the previously planned therapeutic approach.
RESULTS
Forty-two patients were evaluated for suspected recurrent NSCLC using combined PET/CT. Recurrence was the final diagnosis in 24 patients.
Impact of PET/CT on Diagnostic Accuracy of PET Studies: Patient-Based Analysis
Thirty-two PET studies evaluated in the presence of side-by-side CT data were interpreted as positive and 10 studies were interpreted as negative. Twenty-seven PET/CT studies were interpreted as positive and 15 were interpreted as negative (Table 3). Twenty-four positive PET/CT studies (89%) were true-positive with recurrence proven by histologic tissue sampling (n = 15) and by clinical or imaging follow-up (n = 9). Three patients had a false-positive PET/CT study with no evidence of disease for a follow-up ranging between 19 and 26 mo. One patient had an 18F-FDG–avid Warthin’s tumor in the left parotid gland, a second patient had only inflammatory changes in mediastinal 18F-FDG–avid lymphadenopathy at bronchoscopy, and the third patient showing increased bilateral hilar 18F-FDG uptake had no evidence of disease for a clinical follow-up of 26 mo.
Comparison of Performance Indices of PET Versus PET/CT for Diagnosis of Recurrent NSCLC in 42 Patients
Fourteen patients with negative PET/CT studies had no evidence of disease for a mean follow-up of 24 mo (range, 20–30 mo). One patient with a history of bronchoalveolar cancer and equivocal findings on CT had a false-negative PET/CT study. This patient showed no changes on the CT component of the hybrid imaging study compared with the previous CT study and also no foci of abnormal 18F-FDG uptake. Recurrence was diagnosed after the appearance of new structural changes on another CT scan obtained 2 mo later.
In 5 patients (12%) the PET study, interpreted with side-by-side CT data available for comparison, was defined as positive, whereas the PET/CT study was negative (Fig. 1). None of these 5 patients developed a recurrence on follow-up ranging between 24 and 30 mo. PET/CT accurately localized increased 18F-FDG uptake to posttreatment changes (n = 3), a benign bone lesion (n = 1), and aortic calcifications (n = 1).
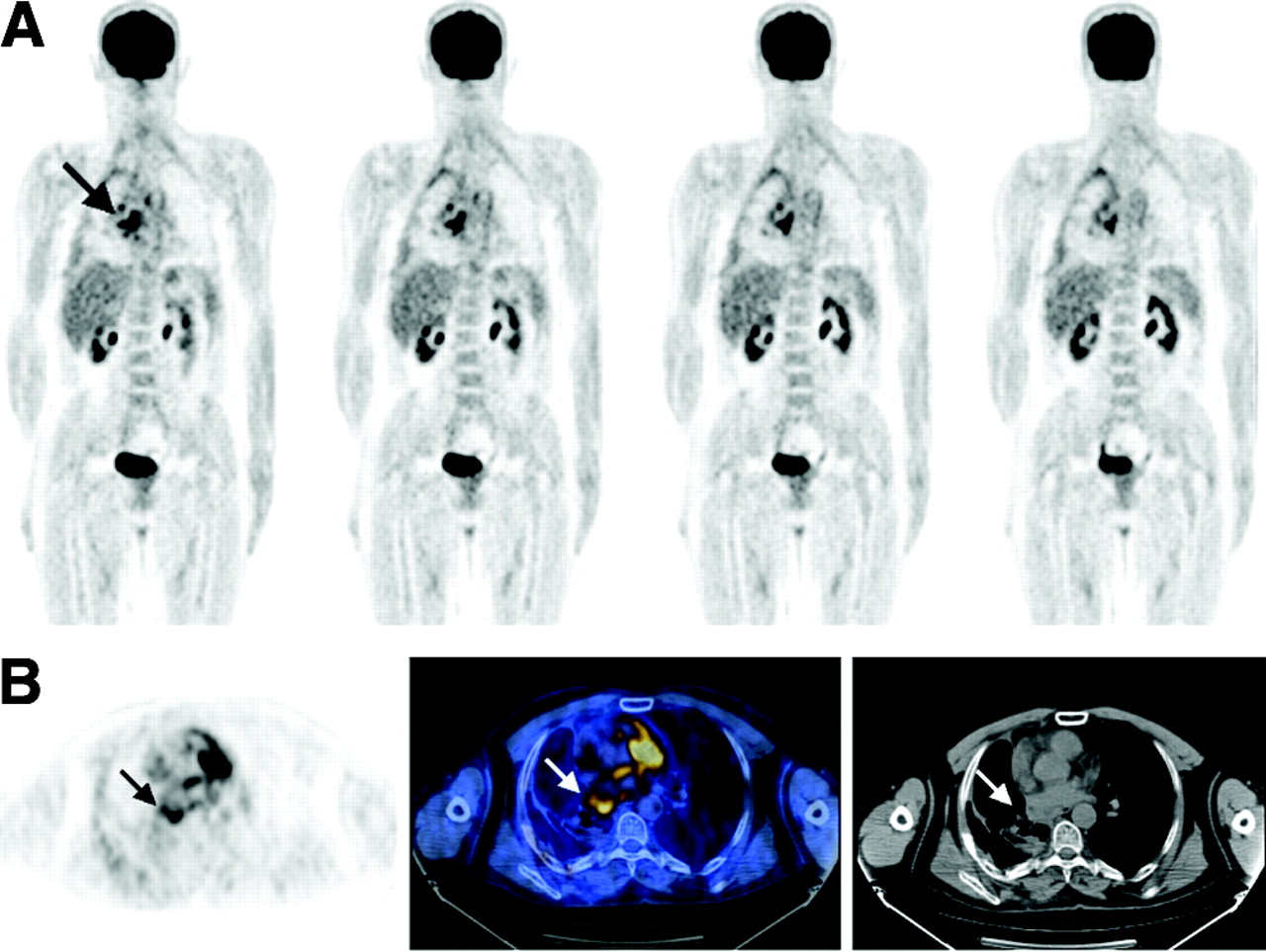
PET/CT-based exclusion of suspected recurrent disease in site of increased 18F-FDG uptake localized to postoperative inflammatory changes. A 57-y-old man with a history of NSCLC showed equivocal CT findings in the area of right upper bronchus stump. (A) 18F-FDG PET coronal images show area of increased 18F-FDG uptake in upper aspect of right hilum (arrow). PET/CT (B, center) precisely localizes abnormal 18F-FDG uptake (B, left) to postoperative pleural thickening (arrows) adjacent to left atrium evident on CT (B, right). No 18F-FDG uptake was seen in area of equivocal CT findings in right upper bronchus stump. No further diagnostic procedures were performed. Patient had no evidence of disease for a clinical follow-up of 27 mo.
The sensitivity, specificity, NPV, and PPV with 95% confidence intervals were calculated. PET/CT showed a sensitivity of 96%, specificity of 82%, NPV of 89%, and PPV of 93% compared with 96%, 53%, 75%, and 90%, respectively, for PET interpreted with side-by-side CT data. No statistically significant difference between these values was found (Table 3).
Impact of PET/CT on Characterization of 18F-FDG–Avid Lesions: Site-Based Analysis
There were 102 sites of increased 18F-FDG uptake in the 42 patients evaluated. Based on PET and side-by-side CT, 69 lesions were characterized as malignant, 20 were benign, and 13 were equivocal. PET/CT changed the final assessment of 28 lesions in 22 patients (Table 4). Sixteen equivocal or malignant sites of 18F-FDG uptake (16%) were localized to physiologic or noncancer–related structures by PET/CT. There was no evidence of disease in 14 sites; no follow-up was available in 2 sites, with the patients being treated for additional malignant lesions.
PET Versus PET/CT Change in Characterization of 28 18F-FDG–Avid Lesions in 22 Patients
PET/CT determined the precise anatomic structures involved in 7 malignant sites (7%) detected by PET, including bone metastases (n = 3), normal-size mediastinal lymph node involvement (n = 2), 1 mediastinal lymph node recurrence in the presence of postoperative changes on CT, and 1 cervical soft-tissue metastasis. The final diagnosis and localization were confirmed in all lesions by biopsy or by changes on follow-up MRI and CT.
PET/CT enabled the retrospective detection of 5 lesions (5%) missed or not considered pathologic on the previously performed high-resolution, contrast-enhanced CT, including 3 mediastinal lymph nodes (12, 10, and 10 mm in size), 1 pulmonary nodule (10 mm in diameter), and 1 retrocrural lymph node (9 mm in diameter). Malignancy was confirmed in all sites by histologic specimens obtained at surgery or by changes on follow-up imaging.
Impact of PET/CT on Patient Management
Results of PET/CT were found to have an impact on the management of 12 patients (29%) by eliminating the need for previously planned diagnostic procedures, by initiating previously unplanned treatment, or by changing the previously planned therapeutic approach (Table 5).
PET/CT Contribution to Clinical Management of 12 Patients
In 5 patients who showed no further evidence of recurrence, PET/CT changed the characterization of focal 18F-FDG uptake from malignant or equivocal to benign and, therefore, eliminated the need for further investigations (Fig. 1).
In 4 patients, radiotherapy planning was affected by the PET/CT results. One patient received previously unplanned local-field radiotherapy based only on PET/CT results, without any further invasive diagnostic procedures (Fig. 2). In 1 patient, PET/CT excluded the presence of mediastinal lymph node metastases suspected by PET alone, with further narrowing of the planned radiation field. In 1 patient with a recurrent lung nodule, precise localization of a second 18F-FDG–avid focus to a 10-mm subcarinal lymph node enabled more accurate radiotherapy planning to a previously irradiated area. In the fourth patient, PET/CT indicated that the PET-detected malignant lesion involved only the paravertebral cervical soft tissues and not the adjacent cervical vertebra as initially suspected by CT, with a further modification of previously planned radiation fields.
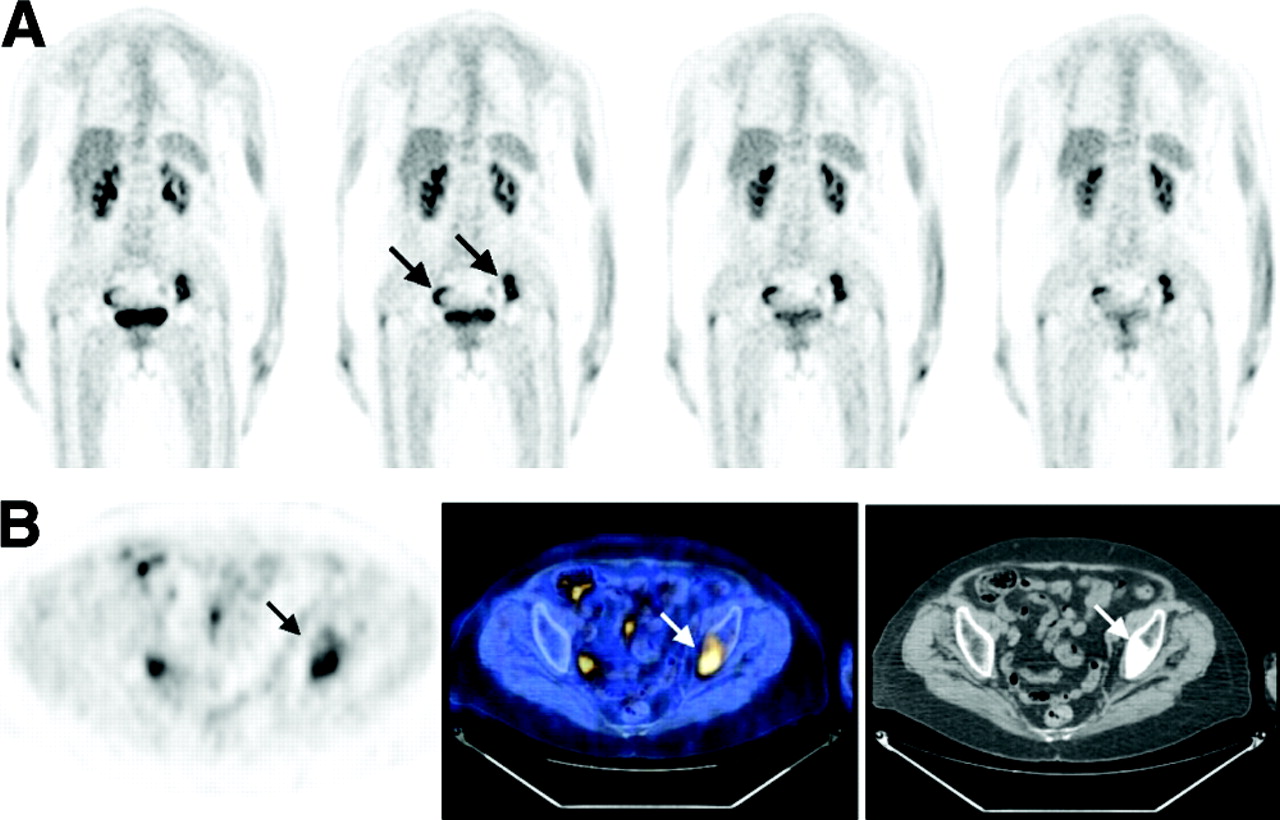
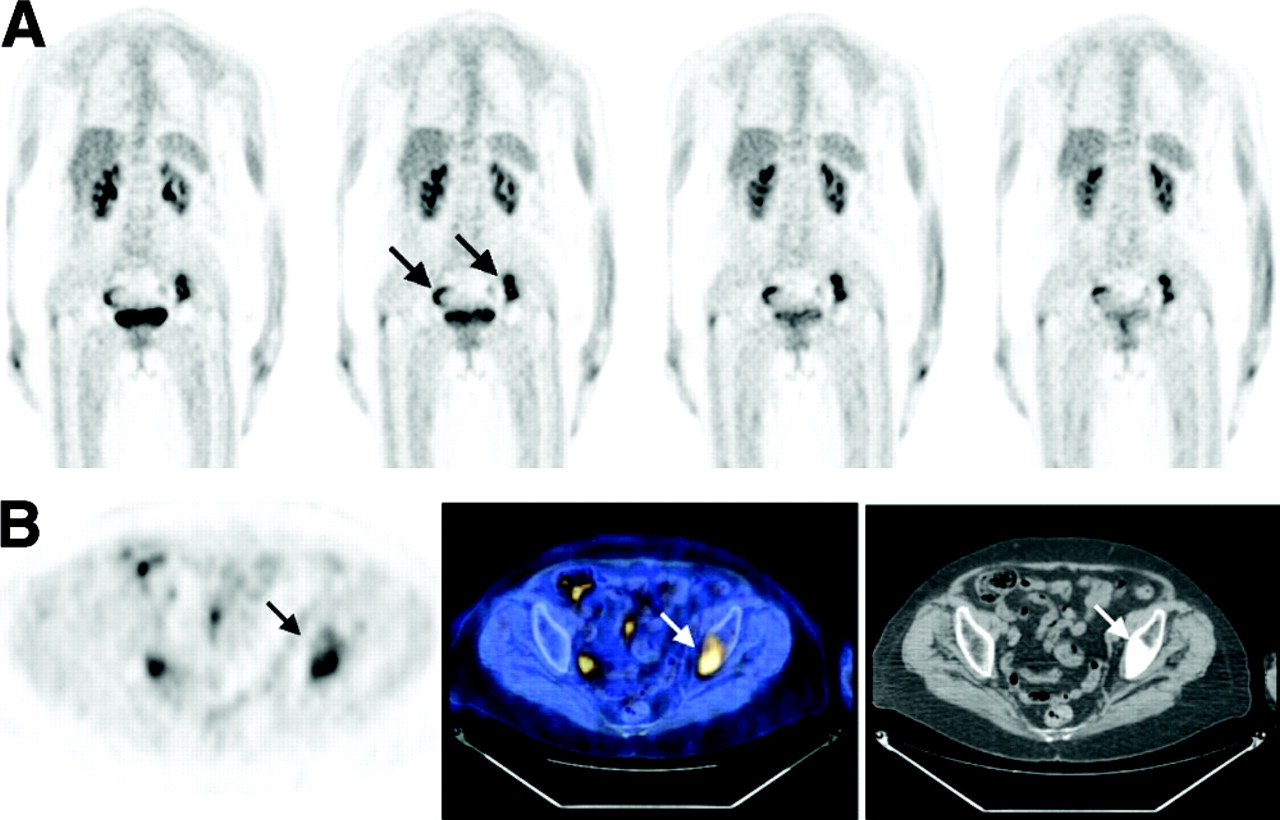
Precise PET/CT localization of equivocal 18F-FDG uptake and diagnosis of previously unknown bone metastasis. A 78-y-old woman with a history of bronchoalveolar NSCLC was evaluated for increasing serum carcinoembryonic antigen levels and negative whole-body, high-resolution, contrast-enhanced CT performed 2 mo earlier. (A) 18F-FDG PET coronal images show focal areas of increased 18F-FDG uptake in pelvis (arrows). PET/CT (B, center) precisely localizes area of increased 18F-FDG uptake (B, right) in right pelvis to physiologic bowel activity and lesion in left pelvis to left iliac bone (arrows). A mixed, lytic, and sclerotic lesion is demonstrated on corresponding slice of CT component evaluated with bone window (B, right, arrow). Retrospective evaluation of previous CT study demonstrated this previously missed bone lesion. Local-field radiotherapy was instituted based on PET/CT diagnosis of single bone metastasis.
In 3 patients, PET/CT precisely defined the extent of disease. Chemotherapy was added to the planned radiotherapy based on the PET/CT diagnosis of additional sites of disease in 2 normal-size metastatic lymph nodes and 1 pulmonary nodule.
DISCUSSION
Clinical oncologic guidelines indicate that NSCLC, which has been treated with curative intent, should be assessed for treatment-related complications for the first 3–6 mo, followed by a monitoring program for detecting recurrence (2). In a surveillance program of lung cancer patients, CT was not found to be of value for diagnosis of recurrence (2,13), though other reports have shown that conventional imaging methods can detect recurrent disease or a second primary lung cancer (4,14,15). The role of CT is controversial because of its limitations in distinguishing nonspecific treatment-related changes from malignancy (2,16). In spite of these difficulties CT has been considered the diagnostic modality of choice when there is suspicion of recurrence (3).
18F-FDG PET plays an important role in assessment of newly diagnosed lung cancer (7–9) and has also been used for diagnosis of recurrent disease (10,11). Although 18F-FDG PET is a very sensitive metabolic imaging modality it lacks specificity after therapy, due to 18F-FDG accumulation in irradiated tissues and postsurgical inflammatory changes up to 6 mo after the end of treatment. Noncancer–related 18F-FDG uptake accounts for about 8% of false-positive PET studies (17).
Anatomic CT and functional PET have a complementary role in the evaluation of cancer patients (12,18). Visual side-by-side comparison of these 2 modalities in the presence of structural and metabolic posttherapy alterations may be challenging.
In the present study, PET/CT improved image interpretation compared with PET with side-by-side CT in 27% of the detected lesions in 52% of the study population. Defining malignancy on CT by size criteria may be problematic. Normal-size lymph nodes may contain malignant tissue, whereas lymphadenopathy may be due to benign processes (19). In the present study, PET/CT indicated the exact localization of 18F-FDG uptake in normal-size mediastinal lymph node metastases in 2 patients.
PET/CT can also determine the precise relationship of the malignant lesions with neighboring organs as shown in 4 patients in whom increased 18F-FDG uptake in the vicinity of bony structures was differentiated from skeletal involvement.
PET/CT allowed the retrospective identification of malignant lesions on CT, initially missed on independent and side-by-side reading due to the complexity of imaging studies in 5 patients with treatment-related distorted anatomy.
Treatment planning for recurrent lung cancer demands precise definition of the cancer-involved structures and the extent of disease. Overall, PET/CT results induced changes in clinical management in 29% of patients. Radiation therapy for locoregional intrathoracic recurrences aims to include all viable cancer tissue while also limiting damage to previously irradiated and healthy tissue in its vicinity (20). In the present study population, PET/CT improved the planning of radiotherapy in 4 patients. The addition of chemotherapy is indicated for multifocal recurrent NSCLC. This was the case in 3 of the patients in this study after the precise assessment of the extent of recurrence by PET/CT.
Disease was excluded by PET/CT in sites of physiologic or noncancerous 18F-FDG uptake in 5 patients. The PET/CT-based change in classification of 18F-FDG–avid foci from malignant or equivocal by PET to benign eliminated the need for further invasive diagnostic procedures, shortened the time of the patients’ anxiety, and spared the potential costs related to unnecessary additional diagnostic procedures.
While the present study evaluated a consecutive series that included all patients referred to PET/CT due to a clinical suspicion of recurrence, these patients may have represented a group with clinically problematic cases who had inconclusive clinical or CT findings. Although the average time that elapsed between the diagnostic CT and the PET/CT studies was 4 wk, several of the patients were evaluated by the 2 imaging modalities at a time lag that can be responsible for some of the differences in rapid-growing malignancies. Tissue sampling was not available for final diagnosis in all cases and, therefore, decisions of the referring clinical team were also based on a summary of clinical, laboratory, and imaging findings including high-resolution, contrast-enhanced CT and MRI when needed. Although the clinical decisions may have been affected by the imaging results, they were always based on combined data of several modalities, and not of a single test.
Although not statistically significant, PET/CT performed better then PET interpreted with side-by-side CT, showing, in particular, a higher specificity and PPV. Furthermore, the incremental value of the precise lesion localization by PET/CT was expressed mainly by the impact of this modality on further patient management.
In a recent report investigating the value of PET/CT in a heterogeneous cancer patient population (18), the impact rate of hybrid imaging on patient management was lower (14%) compared with the results of the present study (29%). The different results obtained in the present study for PET/CT-guided patient management may be due to the different and more specific diagnostic challenges posed by a suspicion of recurrence in patients with previously treated lung cancer.
CONCLUSION
The results of this study demonstrate the potential value of PET/CT in patients with suspected recurrent NSCLC. PET/CT improved the diagnosis of recurrent NSCLC through better anatomic localization and characterization of suspicious PET findings. This resulted in a clinically significant impact on patient management.
Acknowledgments
The authors thank Drs. Thomas H. Hauser and J. Anthony Parker from the Beth Israel Deaconess Medical Center, Boston, Massachusetts, for their many useful suggestions and Julia Buchanan for her editorial assistance. This research was supported in part by a grant from the L. Rosenblatt Fund for Cancer Research of the Technion Foundation and by a grant from the Israeli Cancer Association.
Footnotes
Received Feb. 12, 2004; revision accepted Apr. 23, 2004.
For correspondence or reprints contact: Zohar Keidar MD, PhD, Department of Nuclear Medicine, Rambam Medical Center, Haifa, Israel.
E-mail: zohar{at}keidar.net
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FDG PET/CT and Lung Cancer: Value of Fourth and Subsequent Posttherapy Follow-up Scans for Patient Management
- Follow-up or Surveillance 18F-FDG PET/CT and Survival Outcome in Lung Cancer Patients
- Large Decreases in Standardized Uptake Values After Definitive Radiation Are Associated with Better Survival of Patients with Locally Advanced Non-Small Cell Lung Cancer
- The role of positron emission tomography in the management of non-small cell lung cancer
- Can PET/CT Replace Separate Diagnostic CT for Cancer Imaging? Optimizing CT Protocols for Imaging Cancers of the Chest and Abdomen
- Early Detection of Cancer Recurrence: 18F-FDG PET/CT Can Make a Difference in Diagnosis and Patient Care
- Improvements in Cancer Staging with PET/CT: Literature-Based Evidence as of September 2006
- The contribution of PET/CT to improved patient management