


Abstract
Early detection of recurrence is clinically important and can improve the prognosis and survival of patients with cancer. CT, considered the primary method of investigation because of its low cost and widespread availability, provides high-resolution anatomic details but may underestimate the actual tumor burden by overlooking small tumor clusters in areas of distorted anatomy after treatment. 18F-FDG PET is an effective whole-body imaging technique that detects metabolic changes preceding structural findings. However, the specificity of PET is impaired by false-positive or equivocal results attributable to the lack of precise anatomic landmarks and to sites of increased 18F-FDG uptake of nonmalignant etiology. PET/CT provides fused images that demonstrate the complementary roles of functional and anatomic assessments in the diagnosis of cancer recurrence through the precise localization of suspected 18F-FDG foci and their characterization as malignant or benign. In addition to the accurate diagnosis and definition of the whole extent of recurrent cancer, PET/CT has an impact on patient management because it can assist in defining potential candidates for surgery for cure, planning the appropriate surgical or radiotherapy approach, and referring patients with unresectable disease to other therapeutic options.
Early diagnosis of relapsing malignancies is important for planning future therapeutic strategies which, if initiated without delay, aim either to cure or to prolong disease-free survival and to improve the quality of life of patients with cancer. Although it is commonly appreciated in the oncologist community that there is a gap between diagnostic capabilities and the curative treatment options for relapsing cancer, a variety of therapeutic strategies can be applied for recurrent malignancies. The correct and timely identification of local–regional recurrence or of a single metastasis will affect the choice of definitive, often curative therapy, such as surgery, innovative ablation procedures, or 3-dimensional intensity-modulated radiotherapy, preceded by aggressive systemic chemotherapy regimens when indicated. A relevant example is the case of colorectal cancer, in which early detection of local recurrence or liver metastases, at a stage when still resectable, can provide up to 40% long-term survival with treatment (1). Patients with limited disease and treated for cure have a better prognosis and prolonged survival. The diagnosis of disseminated recurrence indicates that curative resection, often mutilating, or the administration of high doses of radiation is likely to be more detrimental than helpful. Systemic treatments, such as chemotherapy, hormones, immunotherapy, or radioimmunotherapy, need to be considered in these situations.
The diagnostic armamentarium for the detection of recurrent tumors includes a multitude of laboratory and imaging tests as well as various invasive procedures. Tumor markers are biologic substances that are produced and secreted by malignant tumors and that enter the circulation in detectable amounts. Ideally, if tumor specific and if detectable in the presence of minimal disease, these markers could be used to screen, diagnose, and monitor the response to the treatment of cancer.
At present, tumor marker measurements are used mainly for the assessment of recurrent malignancies. Rising levels in serum can precede the detection of overt disease by other diagnostic modalities, with a time interval that may range from a few months to 2 y (2–4). However, significant drawbacks limit the clinical usefulness of tumor marker measurements. A progressive increase in circulating tumor marker levels is suggestive of but not definitive for the diagnosis of a recurrence. Although increasing tumor marker levels may be the earliest indication of recurrent cancer, with high levels being measured in malignancies with various histologies, false-positive results may be found in some benign and physiologic conditions as well (5,6). On the other hand, a large proportion of patients with further proven recurrent tumors, such as colorectal cancer, may have normal blood marker levels (7,8).
Rising marker levels do not indicate the localization of cancer. No correlation has been found between levels in serum or velocity of rising marker levels and the extent of recurrent disease, a clinical parameter with a major impact on the further choice of the appropriate treatment modality (5). The routine use of tumor marker measurements has not led to a substantial improvement in the survival of patients with malignancies such as colorectal or ovarian cancer (5,9). If the tumor sites cannot be detected, then further investigation of the abnormal results of this test will involve sophisticated technology and invasive procedures and may increase the level of a patient's anxiety.
When recurrent cancer is clinically suggested, localization is of utmost importance for planning the appropriate management strategy and is based, as a rule, on conventional imaging procedures, such as CT, MRI, or ultrasound. Diagnosis of recurrent malignancy by high-resolution anatomic imaging modalities is based on the detection of a new abnormal mass or a change in the size of a known lesion caused by renewed cancer growth (8,10).
CT is the primary tool for the clinical routine evaluation of patients with suspected recurrence because of its availability and relatively low cost, despite its rather low sensitivity and specificity for the follow-up of tumors after therapy (11). Although it is considered by surgeons to be the gold standard for assessing the resectability of cancer (12), CT may significantly underestimate the real tumor burden, leading to unnecessary surgery, often mutilating and with wide margins (13). Between 60% and 90% of patients with colorectal cancer, rising carcinoembryonic antigen (CEA) levels, and negative CT results had viable tumors at surgery, with only about half of them being resectable (14,15). Up to 50% of patients considered suitable for curative surgery on CT are found to have unresectable, disseminated disease during surgery (14).
CT criteria for malignancy that are based on size, such as the presence of enlarged lymph nodes with a diameter of 15 mm or more, have been shown to represent an inaccurate estimate of tumor involvement (13). New lesions detected on follow-up CT studies can be the expression of recurrent malignant disease or of inflammatory conditions. Fibrotic or necrotic tissue that develops inside a tumor mass after treatment cannot be differentiated by CT from a viable malignant tumor (16). CT results are particularly difficult to interpret in regions with distorted anatomy after surgery or radiation treatment (15).
Diagnosis of cancer by PET after the injection of 18F-FDG is based on the increased use of glucose by viable malignant cells. Abnormal cancer-related 18F-FDG uptake is attributable to metabolic alterations and increased glycolysis that occur in malignant tissues. 18F-FDG PET is extensively used for the detection of recurrent cancer. PET has the ability to scan the whole body including, as a rule, the area from the head to the midthighs, without exposing the patient to additional radiation and therefore improves the rate of detection of recurrent cancer. The potential to demonstrate the presence of extensive disease can lead to a reduction in further morbidity and expenses related to unnecessary radical treatment (17).
Cancer-related metabolic abnormalities usually precede structural changes and are readily detected by PET (17,18). PET is a highly sensitive imaging test for the detection of occult recurrences, such as those seen in colorectal cancer (14,19). A meta-analysis including 11 studies with 577 patients showed that 18F-FDG PET had an overall sensitivity of 97% and a specificity of 75% for the diagnosis of recurrent colorectal cancer (20). For recurrent ovarian cancer, the sensitivity of PET ranged between 80% and 94% and the specificity ranged between 75% and 84% (10,18).
However, even when PET is used as the initial diagnostic modality in patients with a clinical suggestion of recurrence, there appears to be no significant decrease in the number of further diagnostic procedures performed. Although PET, as a stand-alone modality, performed well for the diagnosis of colorectal tumor recurrence in a patient-based analysis, with a sensitivity of 86% and a positive predictive value of 96%, these same performance indices were significantly lower in a lesion-based analysis, 57% and 78%, respectively, mainly because of the relatively large number of lesions defined as equivocal or inconclusive (14). Although cancer relapse can be diagnosed by PET months and even years before it becomes evident on CT, the detection of early 18F-FDG–avid metabolic changes caused by recurrent tumors is impaired by the intrinsic limitations of this imaging modality. Small tumors may be missed, and increased tracer uptake also may be of physiologic or benign etiology (6,19). In patients with known, previously treated cancer, in particular, increased 18F-FDG uptake may be associated with treatment-related inflammatory conditions (21,22). In addition, PET has a relatively high interobserver variability. A comparison of PET results from 2 independent readers showed differences in the interpretation of approximately 7% of the studies with suspected sites of recurrent cancer (23). False-positive or inconclusive PET reports often require additional confirmatory, at times invasive, examinations.
PET and CT may yield incongruent findings. Each modality offers only a partial solution for the diagnostic challenges of the early detection of recurrent cancer and the precise assessment of its extent. Hybrid PET/CT provides the precise anatomic localization of areas of increased 18F-FDG uptake and combines structural and metabolic assessments of pathologic processes during a single diagnostic session (Fig. 1) (24–26). Simultaneously available anatomic and functional data define the presence, localization, and extent of cancer and are more sensitive and specific than either PET or CT data alone. The topographic coordinates of CT are of major significance for further tissue sampling, particularly in the presence of small hypermetabolic foci suggestive of recurrent tumors (Figs. 2 and 3). PET/CT is a valuable tool for determining whether a patient is a potential candidate for surgery with curative intent, for planning or optimizing the surgical approach, for planning localized radiotherapy, or for the referral of patients with extensive disease to systemic treatment options.
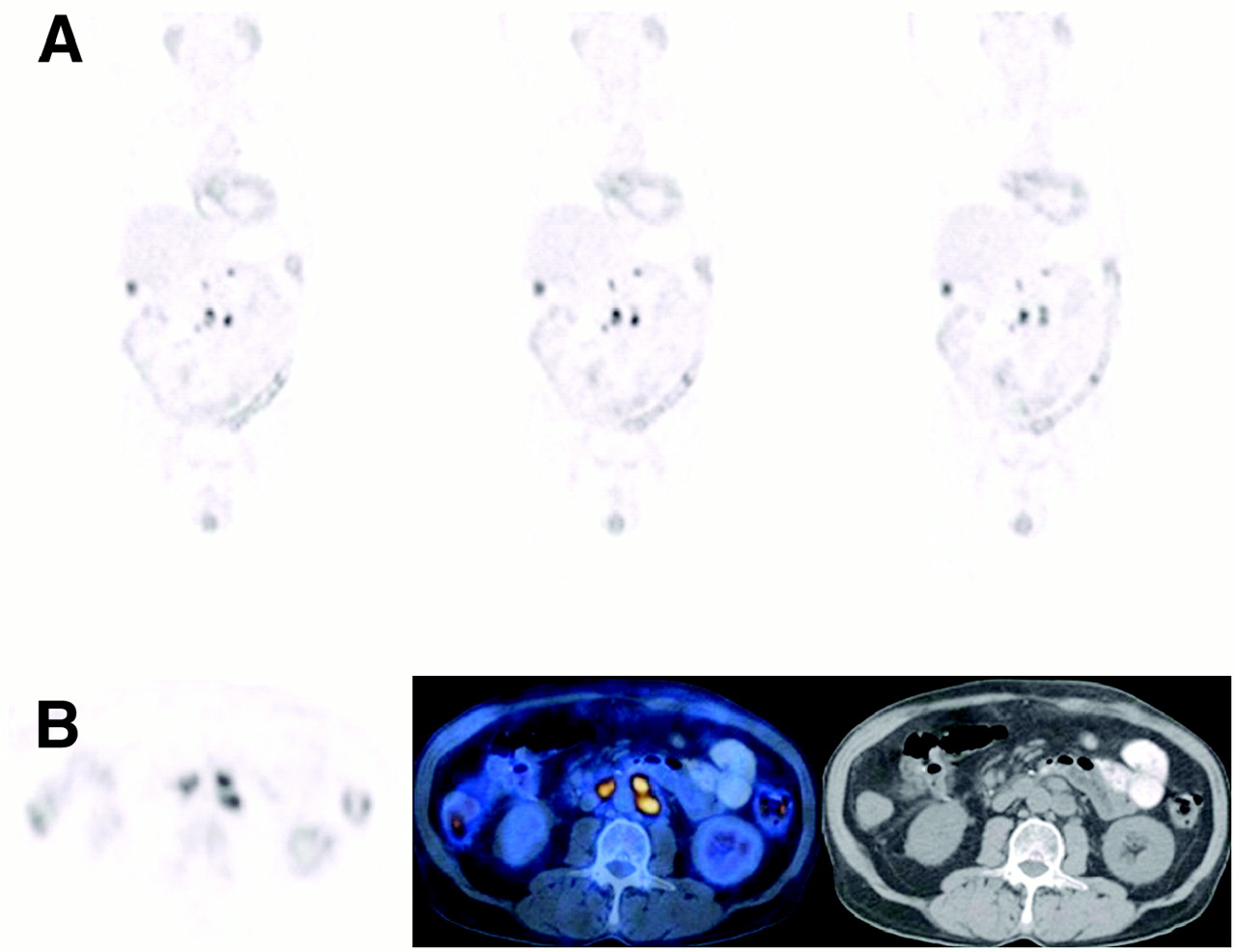
PET/CT precisely localizes suspected foci of abnormal 18F-FDG uptake for diagnosis and estimation of extent of recurrence. A 66-y-old man with colon cancer, stage C, after surgical removal of primary tumor, was assessed for recurrence suggested by elevated levels of CEA serum marker. Results of CT scan performed 2 wk before present examination were negative. (A) 18F-FDG PET study (coronal slices) demonstrates foci of abnormal 18F-FDG uptake in right and middle abdomen. (B) Transaxial slices at level of these findings show paramedian left and right abnormal 18F-FDG foci seen on PET (left), localized by PET/CT (center) to slightly enlarged para-aortic lymph nodes, as demonstrated on CT (right), consistent with metastatic lymphadenopathy. (Focus of increased 18F-FDG uptake in right abdomen is localized by PET/CT to physiologic bowel activity.) On basis of these findings, chemotherapy regimen was changed from adjuvant protocol to drug combination used for treatment of metastatic disease. At follow-up 5 mo later, tumor markers had returned to normal, and repeat PET/CT results were negative. Patient is being reevaluated for consideration of consolidation radiotherapy to area of involved lymph nodes.
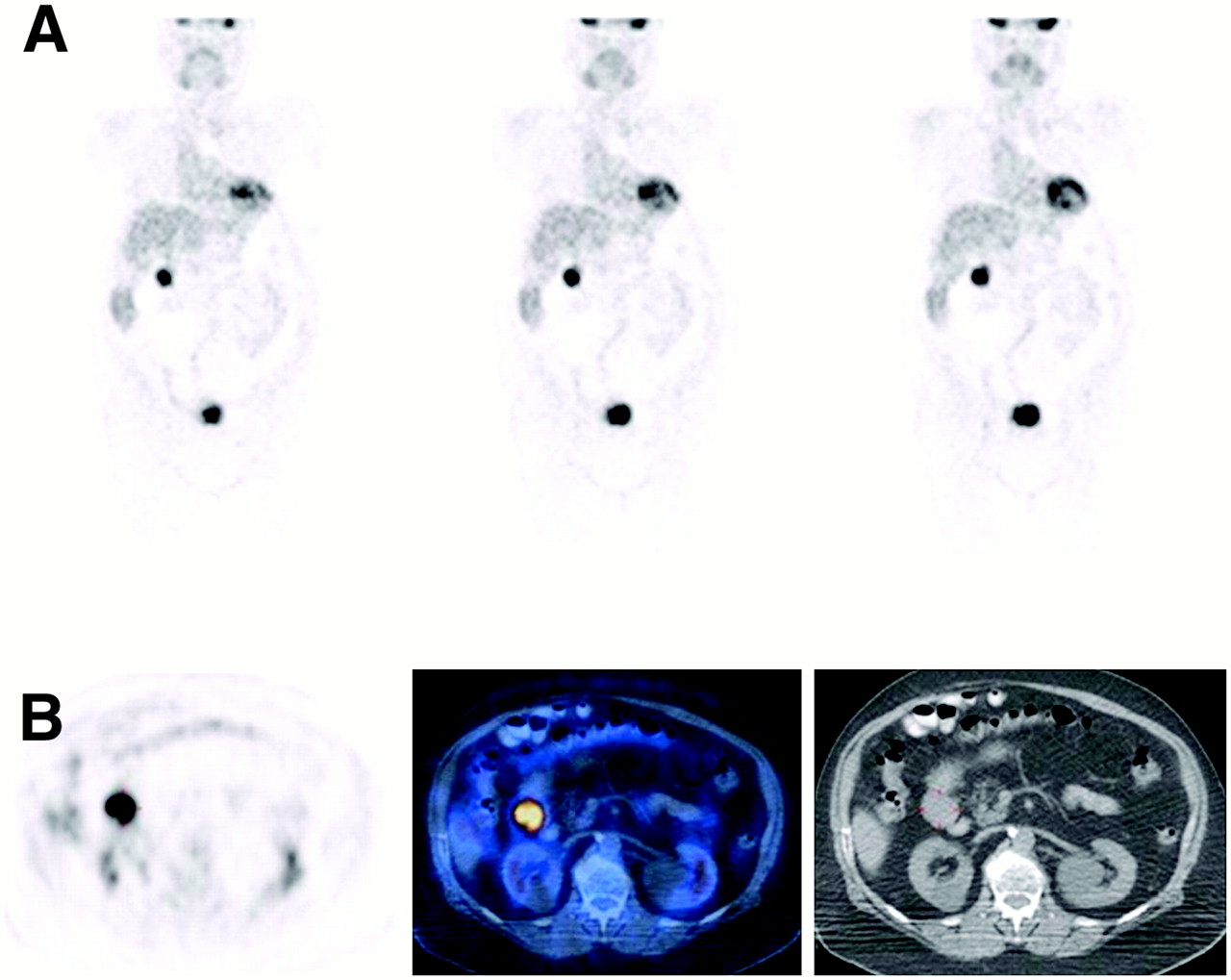
PET/CT detects and characterizes pattern of metastatic spread. An 80-y-old woman with ovarian cancer, after surgery and chemotherapy, was assessed for recurrence suggested by elevated levels of CA-125 tumor marker. CT scan performed 16 d before present examination showed inconclusive findings in liver and renal cysts. (A) 18F-FDG PET study (coronal slices) demonstrates focal area of increased tracer uptake (marker) in right upper abdomen, adjacent to right kidney. (B) Transaxial slices at level of this suspected lesion show focus of increased 18F-FDG uptake on PET (left), localized by PET/CT (center) to mass (4 cm in diameter) in close proximity to duodenum, as demonstrated on CT (right). On basis of detection of single site of recurrence, it was decided to embark on curative approach, and patient was referred for surgery. Peritoneal metastasis was completely removed, and no other sites of disease were found in abdominal cavity. At follow-up 6 mo later, tumor marker had returned to normal levels, repeat PET/CT results were normal, and there was no evidence of active malignancy.
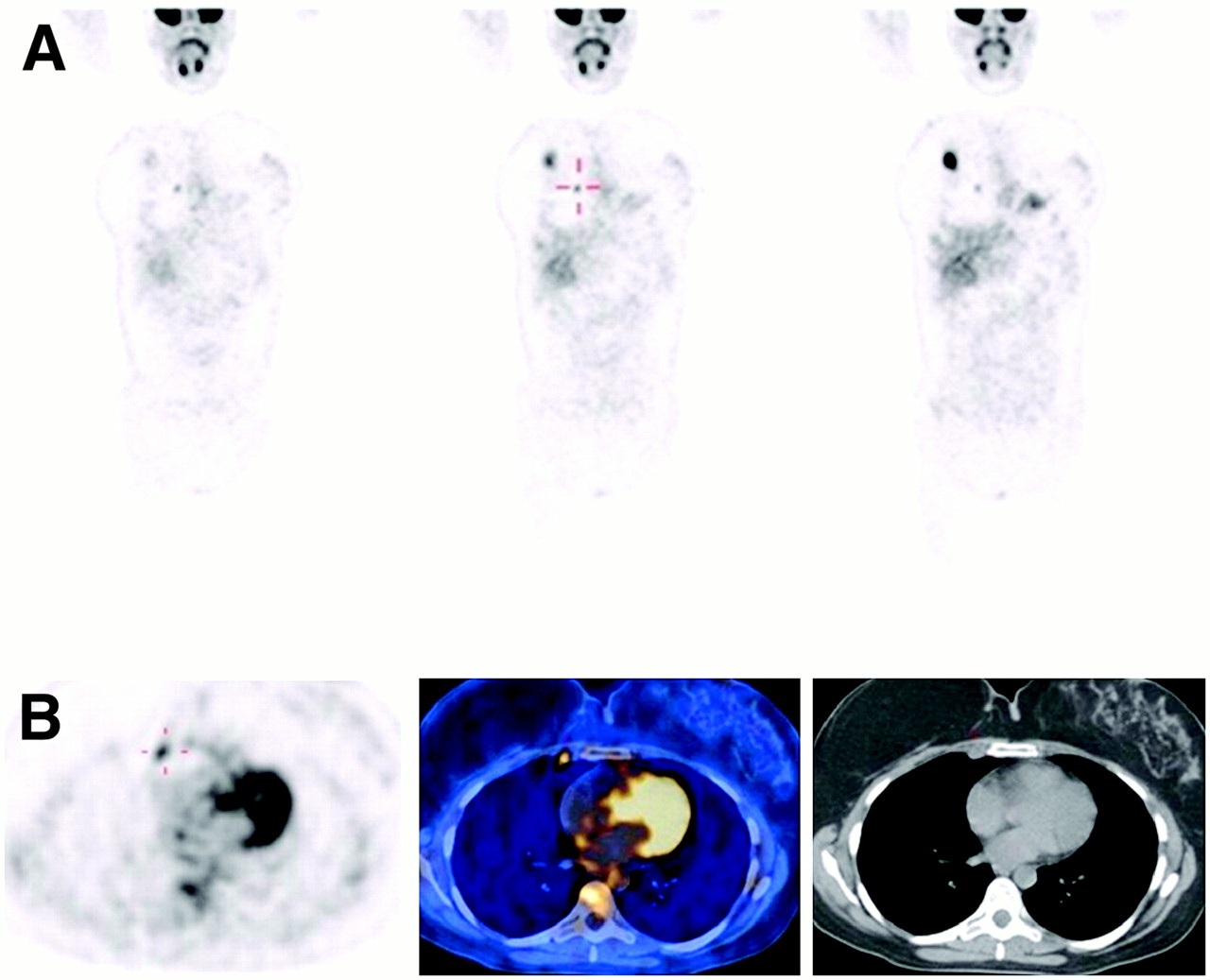
PET/CT defines whole extent of recurrence in areas with complicated anatomy showing changes after treatment. A 46-y-old woman with breast cancer, after right mastectomy 9 y ago, presented with local recurrence and was referred for PET/CT study for treatment planning. (A) 18F-FDG PET study (coronal slices) demonstrates area of intense 18F-FDG uptake in right breast, consistent with known local recurrence. Additional small focus of slightly increased tracer uptake is seen in anterior chest wall (marker). (B) Transaxial slices at level of this equivocal 18F-FDG focus on PET (left) show that focus is localized by PET/CT (center) to lymph node in right internal mammary chain (9 mm in diameter), retrospectively identified on CT (right). After these PET/CT findings were obtained, patient was started on hormone therapy with aromatase inhibitor letrozole (Femara; Novartis). On basis of PET/CT findings, radiotherapy was planned to include internal mammary chain, in addition to irradiation of axilla and supraclavicular fossa. After completion of external radiation, patient received 192Ir brachytherapy implant. At 30 mo after therapy, patient was without evidence of disease, and PET/CT results were negative.
PET/CT has been reported to improve the localization of up to 1 in 3 malignant lesions diagnosed on PET and to define the malignant nature of up to 1 in 6 hypermetabolic foci detected on PET with no associated structural changes on CT (25). In the absence of anatomic lesions, biopsy of abnormalities detected only by PET is difficult to perform. Tissue samples are, however, mandatory to confirm the suspected relapse and to start new treatment (27). The alternative strategy of relying only on observation and clinical follow-up of findings suggestive of relapse may result in a missed opportunity to resect and cure limited disease (11).
Unexpectedly at first, PET/CT has shown an additional benefit. Through mapping of abnormal PET findings on the CT component of the combined study, previous CT examinations that were analyzed de novo showed up to 15% additional, previously missed malignant lesions that were only retrospectively detected (25). The significant improvements in CT technology in recent years have provided exquisite anatomic details but, probably because of the large amounts of data that must be examined, may lead to misinterpretations, even when imaging studies are performed at the highest imaging standards (28).
PET/CT adds a new dimension to the management of cancer by optimizing the accurate decision-making process. Precise diagnosis followed by appropriate treatment choices has a significant impact on the cost of cancer management, especially through avoidance of superfluous expensive diagnostic procedures. The planned therapeutic path may be obsolete in a particular patient, and knowing this spares discomfort and side effects resulting from unnecessary treatment and also shortens the time for referral to a more appropriate treatment strategy. Better presurgical identification of the subgroup of patients who may benefit from curative resection or a radical course of radiotherapy improves the risk-to-benefit ratio as well as the cost-to-benefit ratio in the therapeutic decision-making process for recurrent cancer.
Hybrid PET/CT opens new pathways for the optimized management of recurrent cancer. Being able to work with one of the first PET/CT devices in a routine clinical setting (Discovery LS; GE Healthcare), both nuclear medicine physicians and clinical teams involved in patient care over the last 5 y at our center accumulated extensive experience in the use of hybrid imaging of cancer. For the purpose of this contribution, we reviewed the referral criteria and number of PET/CT studies performed at our center over the last 2 y. During the period from 2004 to 2005, we performed 4,100 PET/CT studies in patients with solid tumors. In 1,055 of these patients (26%), the cause for referral was the suggestion of recurrent cancer on the basis of clinical, laboratory, or prior imaging findings. The most frequent types of tumors referred for suspected relapse or for restaging of a newly diagnosed recurrence included lung and breast cancers, malignancies of the gastrointestinal tract (mainly colorectal cancer), gynecologic tumors (mainly ovarian), and tumors of the head and neck. Although, as stated previously, this is a summary of data at a single institution, we believe that the data represent, at least in part, generally used current referral patterns.
The following text is a partial summary of specific issues related to the role of hybrid imaging in the evaluation of recurrent disease of various types of malignancies.
COLORECTAL CANCER
Colorectal cancer is one of the most frequent malignancies in the Western world. Approximately one third of patients with newly diagnosed colon cancer will develop liver metastases. Liver metastasectomy is the only therapeutic option for cure. A meta-analysis comparing the performances of CT, MRI, and 18F-FDG PET for the diagnosis of colorectal liver metastases in over 3,000 patients evaluated in 61 studies concluded that PET had a significantly higher sensitivity than both CT and MRI in a patient-based analysis. However, a lesion-based analysis showed similar performances for all of the modalities (29).
Detection of the presence of liver metastases is not the only important criterion for treatment planning. Defining the precise extent and localization of disease is of major significance. A study by Selzner et al. (30) comparing contrast-enhanced CT and PET/CT in patients with colorectal cancer metastatic to the liver concluded that both modalities had similar performances for the diagnosis of hepatic metastases, with sensitivities of 95% and 91%, respectively. However, hybrid imaging proved superior for the diagnosis of recurrent disease at the site of or in close proximity to previous hepatic surgery, with a specificity of 100% (vs. 50% for contrast-enhanced CT), as well as for the diagnosis of recurrence at the site of the primary tumor. PET/CT also had a superior rate of detection of extrahepatic dissemination, with a sensitivity of 89%, compared with a 64% sensitivity for CT. The surgeons (coauthors of Selzner et al. (30)) indicated that PET/CT is now their diagnostic imaging modality of choice for assessment of the resectability of liver metastases in patients with colorectal cancer (30).
PET/CT also has been described, although in small series of patients, as a useful diagnostic test for the detection of residual or recurrent tumor after radiofrequency ablation of liver metastases in patients with colon cancer (31). If confirmed in larger cohorts, these initial encouraging results will provide additional evidence for the clinical utility of PET/CT in the assessment of patients with metastatic colorectal cancer.
Local recurrence of rectal cancer develops in approximately one third of patients undergoing curative resection, and early diagnosis is essential. With appropriate treatment, local control and relatively long-term survival can be obtained in one third of patients. PET/CT was shown to play an important role in the accurate diagnosis of presacral recurrence, mainly because of the exclusion of the presence of active malignancies in almost one half of suspected 18F-FDG foci localized by fused images to displaced normal organs (32). In a study including 51 patients, PET/CT had an accuracy of 88% for the diagnosis of recurrent colorectal cancer, compared with a 71% accuracy for PET. Software-based coregistration of PET and CT failed in 24% of the same study population and therefore should not be considered a routine clinical alternative approach (33). In an additional study, the overall PET/CT performance for recurrent colorectal cancer in the abdomen, the liver, and extraabdominal sites showed a sensitivity of 89%, a specificity of 92%, and an accuracy of 90% (34). The metabolic information provided by PET and superimposed on topographic CT landmarks optimized subsequent surgical and radiation treatment planning by differentiating surgical scar from recurrence and by precisely localizing malignant tissue and delineating its boundaries (35).
The current principal clinical indications for PET/CT in recurrent colorectal cancer at our institution include restaging for patients in whom a single site or limited disease has been diagnosed by other imaging modalities, confirming disease resectability before definitive surgery, and assessing suspected occult recurrence in patients with rising tumor marker levels (mainly CEA), with abnormal clinical symptoms, or with equivocal conventional imaging results.
OVARIAN CANCER
Ovarian cancer spreads early during the course of disease by direct extension and at a later stage by intraperitoneal seeding and by lymphatic and hematogenous routes. Omental and peritoneal implants as well as splenic and bowel involvements are common (36). Imaging diagnosis of regional or distant metastases is difficult, and interpretation of PET, in particular, may be suboptimal if malignant foci are localized in the vicinity of nonspecific bowel uptake, hydronephrotic kidneys, or dilated ureters. The specificity of PET is lower than its sensitivity, ranging between 54% and 86% (36).
PET/CT overcomes most of these limitations. Several studies have reported high performance indices for the use of PET combined with CT in the assessment of recurrent ovarian cancer (37–39). In 1 of these studies, for example, PET/CT had a sensitivity of 88%, a specificity of 71%, and an accuracy of 85% for the early diagnosis of recurrent ovarian malignancies (38). PET/CT was also able to detect more malignant sites than was PET or CT alone (40). Hybrid imaging differentiates between adjacent sites of physiologic and malignant 18F-FDG uptake and defines the pattern of metastatic peritoneal seeding, otherwise a diagnostic imaging challenge, sparing unnecessary invasive diagnostic and therapeutic procedures in patients with extensive disease (Fig. 2).
We perform PET/CT studies for patients with newly diagnosed recurrent ovarian cancer mainly to improve the surgical planning of resectable disease. Another frequent clinical indication is the suggestion of recurrence by rising levels of tumor markers (mainly CA-125) in the presence of a negative clinical examination.
BREAST CANCER
Breast cancer is the most frequent malignancy in women. Follow-up for the early detection of recurrence is important because the 5-y survival of patients with disseminated disease is significantly shorter than that of those who have only regional disease. A meta-analysis involving over 800 patients in 16 publications indicated that PET had a mean sensitivity of 93% and a mean specificity of 82% for the diagnosis of recurrent breast cancer (41). The availability of various new therapies for relapsing breast cancer makes early detection as well as determination of the extent of disease and its precise localization of utmost importance.
Initial data regarding the particular role of PET/CT in breast cancer have indicated an improvement in the accuracy of restaging of recurrent disease from 79% with PET to 90% with PET/CT; these results have only marginal statistical significance (42). PET/CT, however, increased the diagnostic confidence in approximately one half of the evaluated patients with breast cancer (43). PET/CT may precisely localize and thus characterize foci of increased 18F-FDG uptake in the chest wall (Fig. 3). It plays an important role in the diagnosis of bone metastases, providing information regarding the presence or absence of structural skeletal lesions on CT as well as their degree of metabolic activity (44–46). Following the increased clinical use of serum tumor marker measurements, noninvasive PET/CT can decrease the time lag between diagnosis and treatment of relapsing breast cancer and therefore increase the chances for cure or long-term palliation (47).
Patterns of referral for PET/CT in breast cancer include patients with elevated levels of tumor markers (mainly CA-15-3, mucin-like carcinoma–associated antigen and, less frequently, CEA or CA-125), patients with local recurrence or single brain metastases for which resection is considered, exclusion of disseminated disease, and patients with diffuse pain and negative conventional imaging study results.
LUNG CANCER
Lung cancer is monitored early after surgery for the diagnosis of treatment-related complications. Later during the course of the disease, patients enter a monitoring program for detecting recurrence. Early diagnosis of local relapse and mainly of a second primary lung cancer may enable potentially curative treatment or effective palliation (48). CT is limited in its capabilities to distinguish between nonspecific, inflammatory, treatment-related changes and malignancies (49,50). 18F-FDG PET has a high sensitivity but a lower specificity because of increased tracer accumulation in irradiated tissues and inflammatory changes after surgery.
PET/CT improves the diagnosis of recurrent lung cancer and has an impact on subsequent management and treatment planning. Compared with PET as a stand-alone procedure, PET/CT increased the true-positive rate from 75% to 89% and had calculated positive and negative predictive values of 89% and 93%, respectively. More important, PET/CT changed the management of 29% of patients by resulting in the elimination of previously planned diagnostic procedures, by resulting in the initiation of a previously unplanned treatment option, or by inducing a change in the planned therapeutic approach (51).
The main PET/CT referral patterns in this category include patients with single known sites of recurrence in the torso or single brain metastases for the assessment of their resectability status, and patients for whom conventional imaging modalities, mainly CT, show abnormal but unclear findings at sites of previous surgery or radiation.
CANCER OF HEAD AND NECK
Cancer of the head and neck requires precise discrimination of local–regional recurrence from inflammation after radiotherapy or surgical scar. This task is challenging because of the presence of persistent, significant edema after treatment, regardless of the presence of active malignancy. Biopsy for tissue sampling is associated with high morbidity. The trauma of multiple invasive procedures in heavily irradiated tissue may lead to radionecrosis or superimposed infection and failure to heal.
The region of the head and neck is characterized by very complex anatomy. 18F-FDG is physiologically present in normal structures such as vocal cords, cervical muscles, or activated brown fat in the neck and shoulder girdle and is taken up by inflammatory changes in recently irradiated areas. PET has been shown therefore to produce a relatively high ratio of false-positive results in studies performed because of suspected recurrent head and neck cancer (52). Hybrid imaging may decrease the incidence of false-positive results. PET/CT was reported to determine the precise localization of approximately two thirds of foci of abnormal 18F-FDG uptake in the region of the head and neck, with a significantly higher incremental value in patients previously treated with surgery or radiotherapy than in those with newly diagnosed tumors. PET/CT had an impact on management in 18% of patients (52).
In carcinoma of the larynx in particular, laryngeal edema that persists after radiation treatment confronts the surgeon with a diagnostic dilemma, with recurrent cancer being found in 50% of patients. Laryngeal biopsy is the diagnostic gold standard but can cause additional edema, radionecrosis of cartilage, and impairment of airways requiring tracheotomy and is confounded by up to 30% false-negative results. A positive PET/CT study can accurately guide a biopsy to the hypermetabolic foci in an edematous larynx and achieve 2 goals: decreasing tissue-sampling errors and avoiding damage to nonmalignant normal but edematous laryngeal structures. PET/CT was recently reported to have a sensitivity of 92% for the detection of recurrent cancer of the larynx (53). PET/CT had a significant impact on patient care and modified the further diagnostic or treatment strategy in 59% of patients with laryngeal cancer, mainly by eliminating previously planned invasive diagnostic procedures. The performance of PET/CT in patients with laryngeal cancer was even better for the diagnosis of distant metastases, with an accuracy of 100%, probably because treatment-related changes are not encountered outside the cervical region (53).
The main clinical indications for PET/CT in this group of tumors differ from most scenarios described for other types of tumors. The presence of severe anatomic distortion after surgery and the reluctance to perform biopsy in heavily irradiated tissues have defined the noninvasive PET/CT procedure as the first diagnostic step in patients with clinically suggested recurrence of head and neck malignancies. Patients are referred for PET/CT mainly to elucidate the etiologies of local–regional edematous changes, of newly palpable cervical lymphadenopathy on physical examination, and of new or persistent clinical symptoms.
THYROID CANCER
Thyroid cancer is monitored mainly with measurements of serum thyroglobulin, with the first suggestion of recurrence being based on the presence of increasing marker levels. The next diagnostic step in this group of patients is total-body radioiodine scintigraphy which, if abnormal, indicates the need for high-dose radioiodine treatment. Patients with non–iodine-avid recurrent thyroid cancer pose a therapeutic dilemma because they will not respond to 131I treatment. Patients with a single resectable metastasis have the best chances for long-term survival. Ultrasound may reliably detect regional recurrence in the neck and direct the resection of cervical sites. 18F-FDG is taken up by metastatic non–iodine-avid thyroid cancer as a result of a tumor dedifferentiation process, and PET therefore provides important prognostic information (54). Initial studies in small series of patients showed PET/CT to be superior to either PET or CT alone for approximately 25% of patients by identifying recurrent tumors or metastatic lymphadenopathy before surgery (55). PET/CT had a reported sensitivity of 66% and a specificity and a positive predictive value of 100% for the diagnosis of recurrent thyroid cancer. Despite a lower negative predictive value, PET/CT provided additional, previously unknown information that altered further management in 40% of patients (56). Another study reported similar results for patients with iodine-negative suspected recurrence of thyroid cancer, with an improved diagnostic accuracy of PET/CT of 93%, compared with an accuracy of PET of 78%. In addition, fused images led to a change in management in 48% of patients (57). Initial observations in a small series of patients suggested that stimulation with thyroid-stimulating hormone before hybrid imaging may further improve PET/CT results, including those in patients with only slight to moderate increases in thyroglobulin levels (58).
The main clinical indications for PET/CT in this category at our institution include all patients who have well-differentiated thyroid cancer, who have a suspected recurrence because of rising thyroglobulin levels, and who have negative 131I whole-body scintigraphy results. Less frequent indications include palpation of newly enlarged cervical lymph nodes or further assessment of the nature of single pulmonary nodules detected by CT.
CONCLUSION
In the early years, PET and CT were regarded as competing procedures, and much effort was invested into comparing and proving their respective advantages and limitations. The medical community has now come to the understanding that neither of these modalities can provide the single answer to complex clinical questions. PET/CT, a single-step metabolic and structural whole-body imaging procedure, is being advocated, and rightly so, as the tool of the future in challenging clinical scenarios, such as early diagnosis and restaging of recurrent cancer (59).
The ultimate measurement of the clinical value of a new diagnostic test is the assessment of its impact on further patient management. Although PET has been confirmed as a good and effective test for the diagnosis of cancer recurrence, hybrid PET/CT appears to be the better tool for the estimation of tumor extent. PET/CT may therefore allow for optimized planning of the surgical approach or radiotherapy fields and dosage as well as for the referral of patients with disseminated disease to palliative treatment modalities. Although this technique has already been applied at a limited level, large-scale randomized trials addressing the clinical utility of PET/CT may lead to a change in the routine diagnostic algorithm and follow-up protocols for patients with cancer by providing correct and early diagnosis of recurrence as well as by establishing its precise significance for further clinical management.
Acknowledgments
This work was supported in part by a research grant from the Israel Cancer Association and by Functional Imaging/CT, GE Healthcare Technologies.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 30, 2006.
- Accepted for publication June 8, 2006.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Indications and Impact on Management: Fourth and Subsequent Posttherapy Follow-up 18F-FDG PET/CT Scans in Oncology Patients
- Prognostic Significance of (18) F-Fluorodeoxyglucose - Positron Emission Tomography After Treatment in Patients With Limited Stage Small Cell Lung Cancer
- Dual-Modality Imaging: Combining Anatomy and Function
- In vivo imaging of molecular targets and their function in endocrinology
- Introduction