


Abstract
The use of recombinant human thyroid-stimulating hormone (rhTSH) has recently become available as an alternative diagnostic tool to assess the persistence and recurrence of differentiated thyroid carcinoma (DTC) in patients on thyroid hormone–suppressive therapy (THST) after near-total or total thyroidectomy and ablative doses of 131I. We report the results of rhTSH administration in patients who were monitored for DTC. Methods: Thirty-three adult DTC patients (13 men, 20 women; mean age ± SE, 45.6 ± 2.31 y; age range, 21–65 y) underwent diagnostic follow-up after rhTSH administration at a dose of 0.9 mg once a day for 2 d. Whole-body scanning and serum thyroglobulin (Tg) measurement were performed after rhTSH administration. Patients were divided into 2 groups depending on serum Tg concentrations on THST: 29 patients had Tg concentrations of <2 ng/mL (group A) and 4 patients had Tg values of >2 ng/mL (group B). Results: In group A, Tg values remained at <2 ng/mL in 25 patients and increased from 1.1 ± 0.14 ng/mL to 22.0 ± 5.75 ng/mL (mean ± SE) in 4 patients after rhTSH administration. Whole-body scanning did not reveal any uptake of 131I in the 25 patients without an increase in Tg, whereas 131I uptake was evident in 2 of the 4 patients with a rise in Tg. In group B, Tg values increased in all 4 patients from 17.3 ± 6.35 ng/mL to 55.3 ± 12.75 ng/mL, and 131I uptake was evident in 3 of the 4 patients. No major adverse effects were reported after rhTSH administration. Conclusion: Our results show that the measurement of serum Tg concentrations after rhTSH has a higher diagnostic value than whole-body scanning in detecting the persistence of thyroid tissue. Therefore, rhTSH should be administered in TSH-suppressed patients with basal serum Tg concentrations of <2 ng/mL because the increment in serum Tg concentrations may reveal the persistence of thyroid tissue in these patients.
Although adequate treatment of differentiated thyroid carcinoma (DTC) by means of total thyroidectomy followed by radioiodine ablation generally leads to its cure, long-term follow-up is necessary in all patients, especially those at high risk, for the presence of residual thyroid bed tissue or recurrent or metastatic thyroid cancer. Whole-body scanning and serum thyroglobulin (Tg) measurements after discontinuation of thyroid hormone–suppressive therapy (THST) are the most sensitive methods in the follow-up of such patients (1–4). Withdrawal of THST is required to increase endogenous thyroid-stimulating hormone (TSH) to stimulate adequate 131I uptake from the thyroid bed or metastatic tissue and to stimulate Tg release (5–10). However, this procedure is associated with a negative impact on the quality of life because of the appearance of symptoms of hypothyroidism (11). Moreover, l-thyroxine withdrawal for a long period of time might increase the risk of cancer growth (12).
The availability of recombinant human TSH (rhTSH) has provided a new tool in the diagnostic management of DTC (13–16). Recent studies have shown the ability of rhTSH to promote radioiodine uptake on diagnostic scans and raise serum Tg concentrations (17,18) with a diagnostic accuracy comparable with that of THST withdrawal (19,20), avoiding the morbidity of hypothyroidism.
This report describes the results obtained after rhTSH administration in patients monitored for DTC who had been treated previously with total or near-total thyroidectomy and a high ablative dose (3.7 kBq [100 mCi]) of 131I. We evaluated whether Tg measurement after rhTSH can be a sensitive marker for the presence of thyroid remnants or metastatic disease when used alone or in combination with whole-body scanning.
MATERIALS AND METHODS
Patients
Thirty-three adult DTC patients (13 men, 20 women; mean age ± SE, 45.6 ± 2.31 y; age range, 21–65 y) underwent diagnostic follow-up after rhTSH administration. All patients had been treated previously with total or near-total thyroidectomy, with lymph node dissection in 20 cases, and treated with a high ablative dose (3.7 kBq [100 mCi]) of 131I. Twenty-one patients (63.6%) had papillary carcinoma, 8 (24.2%) had a follicular variant of papillary carcinoma, 3 (9.1%) had an insular variant of papillary carcinoma, and 1 (3%) had follicular carcinoma. All subjects were on THST in doses sufficient to suppress serum TSH concentrations to <0.1 mIU/L. All subjects underwent diagnostic or posttherapy 131I whole-body scanning 6–24 mo before this rhTSH study.
Patients were divided into 2 groups depending on serum Tg concentrations on THST: Group A includes 29 patients with Tg concentrations of <2 ng/mL; group B includes 4 patients with Tg values of >2 ng/mL This cutoff value for Tg results was chosen because a Tg value of 2 ng/mL has been suggested as the threshold level indicative of persistence of DTC (20). The characteristics of the patients are reported in Table 1.
Tumor Characteristics, Serum Tg Concentrations, and 131I WBS in 33 DTC Patients Before Study
No patients had evidence of other medical disorders, were pregnant, or were on medications known to affect thyroid function or interfere with hormone measurements. None of the subjects received radiographic contrast agents that could interfere with the 131I uptake by a thyroid remnant or metastatic tissue. A low-iodine diet was recommended before whole-body scanning. None of the patients discontinued THST. All patients gave written informed consent to participate in the study, which was approved by the respective local ethical committees.
Study Design
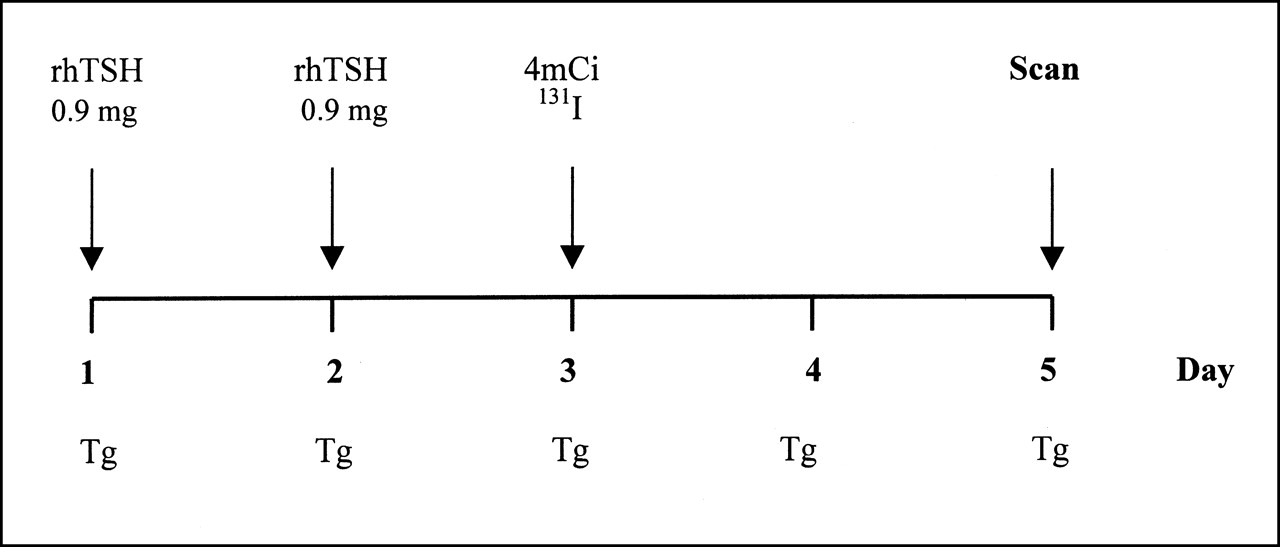
All patients were hospitalized from Monday to Friday and received intramuscular rhTSH (Thyrogen; Genzyme Corp., Cambridge, MA) at a dose of 0.9 mg once a day for 2 d. Twenty-four hours after the last dose of rhTSH, 148 MBq (4 mCi) 131I were administered.
Whole-body scanning was then performed with a double-head gamma camera fitted with a high-energy collimator, and uptake was measured 48 h after 131I had been administered (Fig. 1). Scanning was performed at a constant low speed with acquisition at a minimum of 30 min or of at least 140,000 counts. Single spot images of body regions were acquired after scanning a minimum of 10–15 min or after obtaining 60,000 counts for a large-field-of-view camera or 35,000 counts for a small-field-of-view camera. The extent of disease was defined on the basis of the presence of 131I uptake in the thyroid bed or abnormal activity elsewhere in the neck, lungs, mediastinum, bone, or other sites. All previous 131I diagnostic scans, posttherapy scans, and those obtained after rhTSH stimulation were evaluated by 2 independent observers.

Protocol for rhTSH administration and radioiodine scanning procedure for patients on THST (148 MBq [4 mCi] 131I were administered).
Serum Measurements
Blood samples for measurements of TSH, free thyroxine (FT4), free triiodothyronine (FT3), Tg, and Tg antibodies were obtained in the morning before the first rhTSH administration and 24, 48, 72, and 96 h later. Serum Tg, TSH, FT4, FT3, and Tg antibodies were measured using the automated chemiluminescence system. All samples were processed in duplicate in the same assay. The Tg assay (Immulite; Diagnostic Products Corp., Los Angeles, CA) had a detection limit of 0.2 ng/mL and a functional sensitivity of 0.9 ng/mL, with intra- and interassay coefficients of variation of 5.3% and 7%, respectively. The TSH assay (ACS Centaur; Chiron Diagnostics Corp., East Walpole, MA) had an analytic sensitivity of 0.010 mIU/L, with intra- and interassay coefficients of variation of 2.41% and 3.17%, respectively. The FT3 assay (ACS Centaur; Chiron Diagnostics) had an analytic sensitivity of 0.46 pmol/L, with intra- and interassay coefficients of variation of 3.40% and 6.76%, respectively. The FT4 assay (ACS Centaur; Chiron Diagnostics) had an analytic sensitivity of 1.29 pmol/L, with intra- and interassay coefficients of variation of 4.69% and 4.59%, respectively. All samples collected from an individual patient were tested in a single assay. The basal serum specimens of all patients were also screened for the presence of Tg antibodies with the automated chemiluminescence system (Immulite; Diagnostic Products Corp.). The sensitivity was 2.0 IU/mL, and the intra- and interassay coefficients of variation were 4.2% and 8.7%, respectively.
Statistical Analysis
Results are reported as mean ± SE. ANOVA for repeated measures was used to compare the results of TSH, FT3, and FT4 during the protocol period. If values were significantly different (P < 0.05), a Student paired or unpaired test was also used.
RESULTS
All subjects tolerated rhTSH well. Three patients complained of nausea, which was mild and short-lived, and 1 patient experienced a transient headache.
Serum TSH concentrations before and after rhTSH administration in patients on THST are presented in Figure 2. Serum TSH concentrations increased from 0.03 ± 0.001 mIU/L on day 1 to 128 ± 6.90 mIU/L and 175 ± 9.05 mIU/L, 24 h after the first and the second rhTSH injections, respectively. Peak serum TSH concentrations after rhTSH administration were significantly higher (P < 0.001) than that measured (78.9 ± 3.39 mIU/L) on the day of 131I administration after l-thyroxine withdrawal on prior occasions.
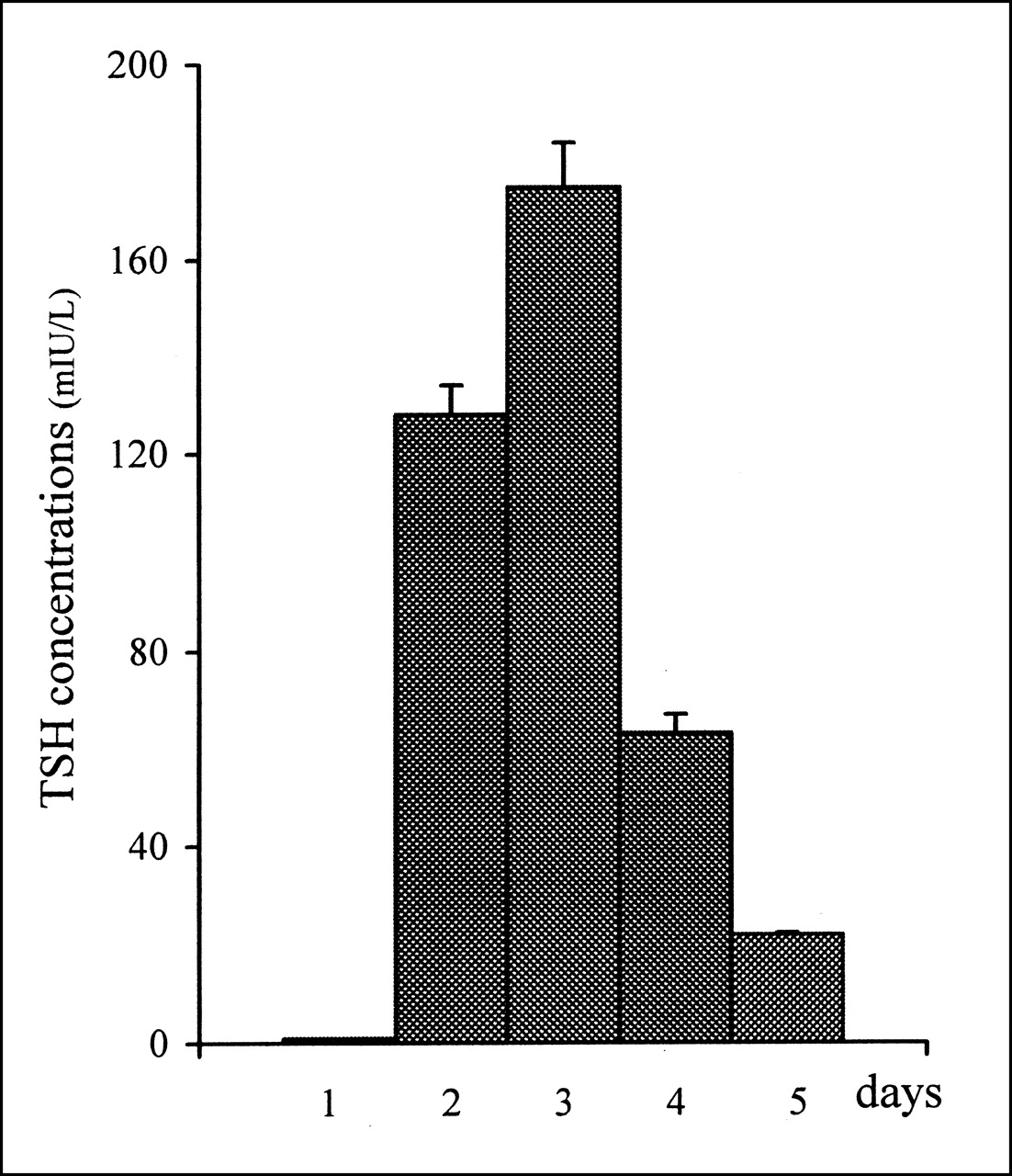
Serum TSH concentrations (mean ± SE) at baseline and after rhTSH injections during 5 d of study.
No significant changes in serum FT3 and FT4 concentrations were observed before and after rhTSH administration. No patients had circulating Tg antibodies.
Baseline serum Tg concentrations were <2 ng/mL in 29 patients (group A) and >2 ng/mL in 4 patients (group B). In group A, serum Tg concentrations remained <2 ng/mL in 25 patients and increased after rhTSH stimulation in 4 patients from 1.1 ± 0.14 ng/mL (range, 0.9–1.5 ng/mL) to 22.0 ± 5.75 ng/mL (range, 5–30 ng/mL) (Fig. 3A). Whole-body scanning obtained after rhTSH showed no uptake in the patients who did not have a rise in the serum Tg value after rhTSH, whereas uptake of 131I was observed in 2 of the 4 patients who had a rise in serum Tg concentrations of >2 ng/mL after rhTSH administration (Fig. 4).
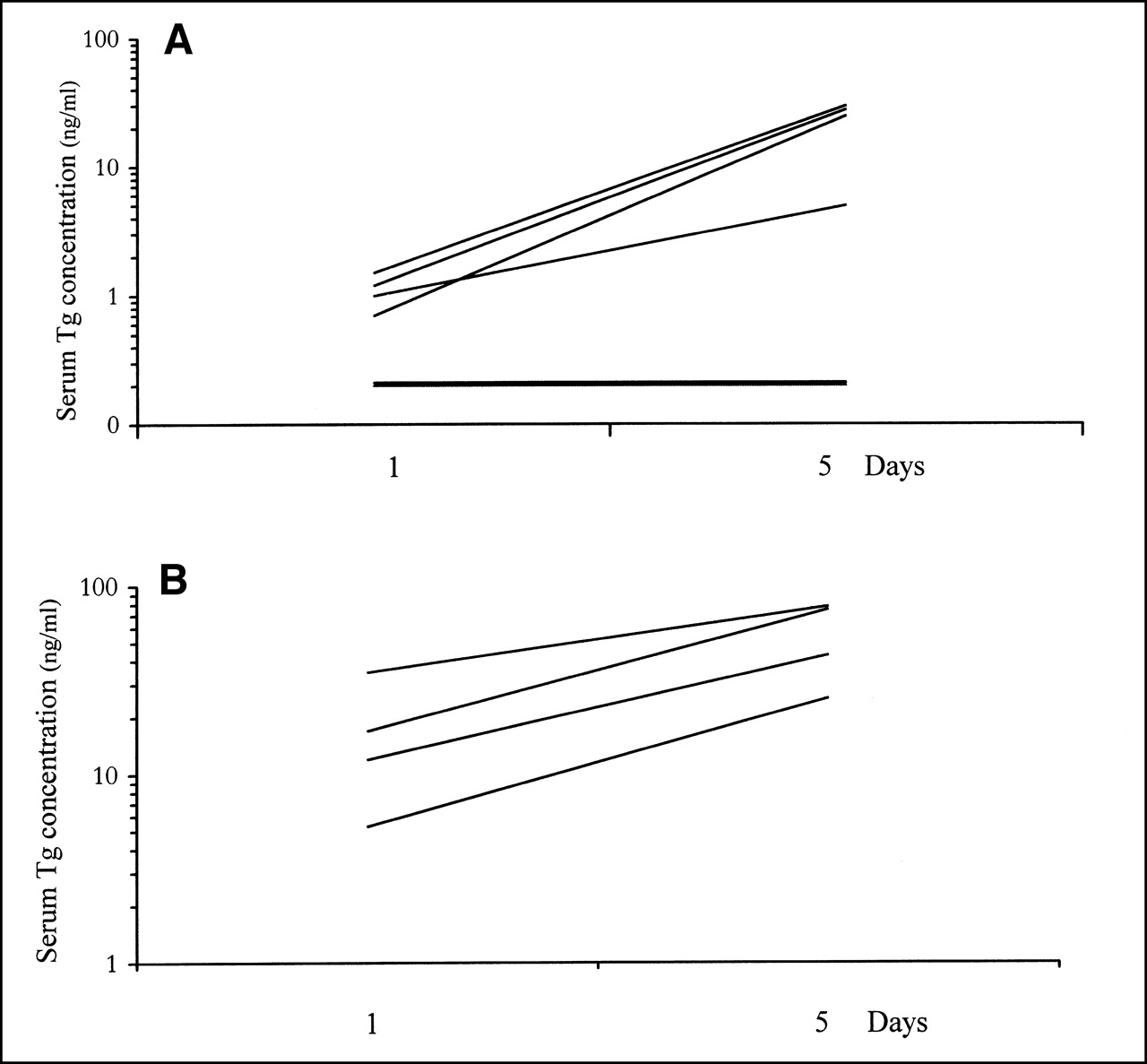
Serum Tg levels at baseline and after rhTSH administration in 29 patients of group A (A) and in 4 patients of group B (B).

Results of whole-body scanning and Tg measurements after rhTSH administration in 29 patients with baseline Tg levels of <2 ng/mL (group A) on THST.
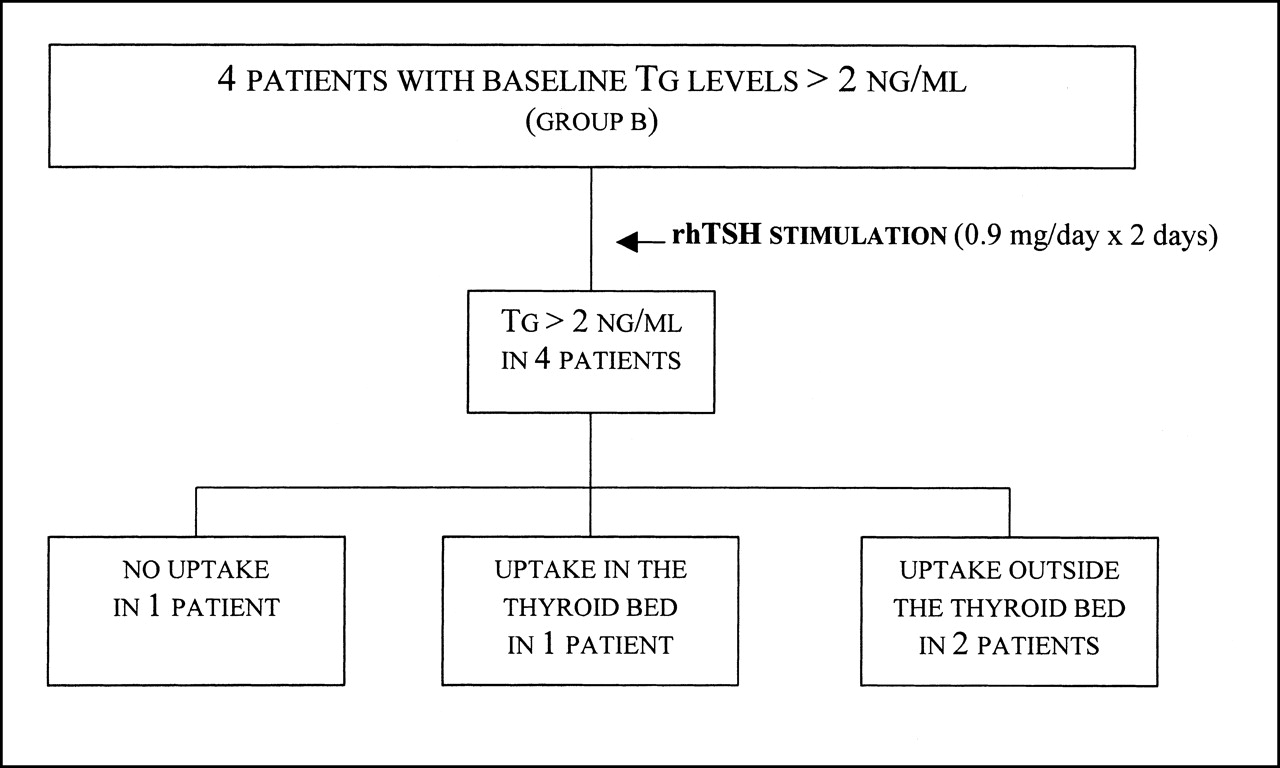
In group B, rhTSH administration induced a marked rise in serum Tg concentrations in all patients from 17.3 ± 6.35 ng/mL (range, 5.3–35.0 ng/mL) to 55.3 ± 12.75 ng/mL (range, 25.3–78.0 ng/mL) (Fig. 3B). Whole-body scanning obtained after rhTSH administration showed 131I uptake in 3 of these 4 patients: in the thyroid bed in 1 patient and outside the thyroid bed in bone or lung in 2 patients (Fig. 5).

Results of whole-body scanning and Tg measurements after rhTSH administration in 4 patients with baseline Tg levels of >2 ng/mL (group B) on THST.
Seven of the 8 patients with a rise in serum Tg concentrations after rhTSH (group A, 3 patients; group B, 4 patients) were treated with therapeutic doses of 131I after l-thyroxine withdrawal. In these 7 patients, posttherapy 131I whole-body scanning revealed uptake in or outside the thyroid bed. In particular, the 2 patients with increased serum Tg concentrations and negative whole-body scans after rhTSH showed 131I lung uptake after receiving therapeutic dose of 131I.
DISCUSSION
We report the results of rhTSH administration in 33 DTC patients on THST, who were treated previously by near-total thyroidectomy and radioiodine therapy, to detect the persistence or recurrence (or both) of thyroid disease. The patients given rhTSH preserved a good quality of life, avoiding the physical discomfort, the metabolic alterations, and the mood disorders occurring after THST withdrawal. Moreover, patients did not have any serious adverse reactions to the administration of rhTSH. Only mild nausea and headache were observed in 9% of the cases, similar to findings of other studies (18,19).
Several clinical trials using rhTSH have shown that its administration is an effective means to stimulate serum Tg secretion and 131I uptake by thyroid tissue in THST patients monitored for DTC (18–23). Our study shows that the administration of rhTSH to 25 patients did not reveal any increment of serum Tg concentration or 131I uptake, thus indicating an excellent concordance between Tg and whole-body scan findings. Furthermore, this study shows that, even in THST patients with Tg values of <2 ng/mL, the cutoff value reported for persistence of bed uptake or DTC (20,21), rhTSH administration stimulated Tg secretion, suggesting the presence of thyroid tissue remnants or metastatic thyroid cancer in 4 other patients (13.8%). This finding is in agreement with the findings of other studies (18,20). In a large multicenter study, the increment of serum Tg concentrations above the cutoff value of 2 ng/mL after rhTSH administration increased the detection rate of thyroid tissue from 22% to 52% in patients with 131I uptake limited to the thyroid bed and from 80% to 100% in patients with metastatic disease (19).
In addition, our study indicates that 131I whole-body scanning performed after rhTSH administration does not provide information that improves the detection rate of DTC. In fact, in 4 patients in group A, with serum Tg concentrations of <2 ng/mL on THST, a 20-fold increase in serum Tg concentrations was observed after rhTSH administration, whereas only 2 patients had whole-body scans that revealed 131I uptake in the thyroid bed. In the 4 patients in group B with elevated baseline serum Tg concentrations, rhTSH administration induced a marked rise in serum Tg values. In these patients, with Tg values suggesting the presence of metastatic disease or local recurrence, whole-body scanning performed after rhTSH stimulation revealed 131I uptake in only 3 of the 4 patients: in the thyroid bed in 1 patient and outside the thyroid bed in 2 patients.
The presence of 131I uptake on the posttherapy whole-body scans of the patients with a rise in serum Tg concentration and negative whole-body scans after rhTSH confirms that the measurement of serum Tg after rhTSH can have a higher diagnostic value than whole-body scanning in detecting the presence of thyroid tissue.
Our results are in agreement with the findings of other studies indicating that discordant results between 131I scans and Tg measurements after rhTSH administration may be seen in patients with metastatic thyroid cancer (20,24). Furthermore, a rise in serum Tg values after rhTSH administration indicates that the thyroid cells are sensitive to TSH stimulation. The failure to detect any abnormal 131I uptake after rhTSH administration could be attributed to the 2-fold higher clearance of 131I when patients are euthyroid compared with hypothyroid patients (25,26) or to a short-time exposure of thyroid tissue to TSH stimulation. At present, serum Tg testing after rhTSH stimulation has not been reported to give false-positive results (20,27).
CONCLUSION
Our findings indicate that in DTC patients on THST, Tg measurements should be performed after rhTSH administration and may have a higher diagnostic value in comparison with whole-body scans for the selection of subjects with persistent normal or neoplastic thyroid tissue. However, Tg testing cannot be used as a precise method for the detection of DTC when anti-Tg antibodies are present or the thyroid tissue is unable to secrete Tg in response to TSH.
Acknowledgments
The authors thank Genzyme Corporation for providing the rhTSH. This work was supported by grants from the Italian Ministry of University and Scientific and Technological Research (project 9906153187-004, 40% in 1999 and 60% in 2000).
Footnotes
Received Dec. 12, 2001; revision accepted May 29, 2001.
For correspondence or reprints contact: Ettore C. degli Uberti, MD, Section of Endocrinology, Department of Biomedical Sciences and Advanced Therapies, University of Ferrara, via Savonarola, 9, 44100 Ferrara, Italy.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Reply: Utility of Diagnostic Whole-Body Iodine Scanning in High-Risk Differentiated Thyroid Carcinoma
- The Role of Routine Diagnostic Radioiodine Whole-Body Scintigraphy in Patients with High-Risk Differentiated Thyroid Cancer
- Recombinant TSH-Stimulated, Radioguided Differentiated Thyroid Carcinoma Surgery