


Abstract
Abnormal exercise perfusion findings have been described as false-positive for coronary artery disease in patients with suspected angina and angiographically normal coronary arteries. Methods: The significance of this finding was further investigated by obtaining intravascular sonograms and Doppler guidewire measurements of at least 2 coronary arteries in 20 consecutive patients who had chest pain, normal coronary angiography findings, and positive stress–rest sestamibi SPECT findings. The summed reversible score was used to describe the extent and severity of reversible perfusion defects. On the basis of scintigraphy findings, vessels were grouped as supplying underperfused myocardial segments (target vessels, n = 20) or normal territories (reference vessels, n = 25). The presence and extension of atherosclerotic disease of the epicardial arteries were assessed by intracoronary sonography. Measurements of plaque area (PA), vessel area (VA), and relative cross-sectional PA (RPA) (RPA = PA/VA) were obtained at the site of maximum plaque concentration. The coronary flow velocity reserve (CFR) was assessed during adenosine-induced hyperemia, and the relative flow reserve was calculated as the target-to-reference coronary reserve ratio. Results: The median summed reversible score was 3 (range, 1–6). Intracoronary sonography showed occult atherosclerosis in 19 patients (95%), with RPA greater than 40% in 16 patients (80%). Mean RPA was significantly greater in the target vessels (46% ± 14%) than in reference vessels (12% ± 18%; P < 0.0001). Doppler flow velocity measurements showed abnormal vasodilation capacity (CFR < 2.5) in 14 patients (70%). Mean CFR was significantly lower in the target vessels than in the reference vessels (2.3 ± 0.5 versus 3.1 ± 0.6; P < 0.0001). A significant inverse correlation was seen between the summed reversible score and the coronary reserve ratio (y = 9.05x − 9.9; r = 0.70; P < 0.005). Conclusion: Reversible perfusion defects seen on SPECT images are often associated with angiographically unrecognized occult atherosclerotic changes and an abnormal vasodilation capacity of the coronary circulation. The tendency to dismiss abnormal exercise perfusion findings as false-positive in these patients may be unjustified.
The accuracy of myocardial perfusion scintigraphy in the detection of coronary artery disease has been evaluated in several studies using coronary angiography as the gold standard (1–3). Therefore, abnormal perfusion findings in patients without significant coronary artery narrowing at coronary angiography have been considered false-positive. Several factors have been reported to affect the specificity of radionuclide perfusion imaging. These include the type of acquisition and the criteria for interpretation and analysis. Factors frequently associated with false-positive stress perfusion findings are the female sex, angina with normal coronary arteries (syndrome X), left bundle branch block, cardiomyopathy, and mitral valve prolapse (4–8). Coronary angiography is a well-established and useful technique for clinical assessment of patients with coronary artery disease. Whether a coronary angiogram may represent a true gold standard for perfusion imaging studies is still a matter of debate. Recent work with intracoronary sonography and Doppler flow measurements has emphasized the limitations of coronary angiography in assessments of the extent and severity of coronary disease, particularly in the early phases of atherosclerotic coronary involvement (9–13). In this study, we sought to assess the significance of abnormal scintigraphic findings in patients with angina and normal coronary angiography findings by evaluating coronary anatomy and vasodilator capacity with intracoronary sonography and Doppler flow velocity measurements.
MATERIALS AND METHODS
Patients
We studied 20 consecutive patients (9 men, 11 women; age range, 40–79 y; mean age ±SD, 58.9 ± 10 y) referred for coronary angiography because of chest pain, abnormal exercise electrocardiography findings, and abnormal myocardial perfusion findings. The patients had a mean left ventricular ejection fraction of 60% ± 13%. The clinical history included stable angina in 13 patients (65%), unstable angina in 3 (15%), and non–Q wave myocardial infarction in 5 (25%). Associated risk factors included diabetes in 3 patients (15%), dyslipidemia in 6 (30%), hypertension in 10 (50%), and smoking in 2 (10%). Patients were selected if the performing angiographer and another angiographer not involved with the study agreed that the angiography findings were normal, with smooth borders, or indicated only minimal irregularity by visual analysis. The presence of significant coronary artery narrowing (>30% diameter stenosis by quantitative analysis), vessel ectasia, myocardial bridging, slow flow, or any other abnormal findings excluded subjects from the study. Patients with intramyocardial conduction abnormalities (left bundle branch block), cardiomyopathy, or mitral valve prolapse were also excluded. At the time of the study, many patients received antianginal medications and antiplatelet agents. Only 3 patients were receiving therapy for their dyslipidemia. No major changes in medications occurred during the study. Intracoronary sonography and Doppler studies were performed immediately after angiography and after the patients gave informed consent, according to the approved clinical protocol of the local ethical committee.
99mTc-Sestamibi SPECT
Myocardial perfusion SPECT was performed with a 2-d stress–rest protocol. Each patient received 800–925 MBq 99mTc-sestamibi (reconstituted from Cardiolite kits [Du Pont Merck Pharmaceuticals, Wilmington, DE]) intravenously either at baseline or during exercise stress testing. The images were acquired 1 h after injection using a rotating single-head gamma camera (Prism 1000XP; Picker, Cleveland, OH) equipped with a low-energy high-resolution parallel-hole collimator. Sixty images were obtained on a 64 × 64 matrix for 15 s, throughout a 180° arc, beginning at the 45° right anterior oblique projection and ending at the 45° left posterior oblique projection. Transaxial reconstruction was achieved using a standard backprojection algorithm and a Butterworth filter with a cutoff frequency of 0.21 Nyquist (0.18 cycles per centimeter) and an order of 4. The transaxial sections were then used to generate oblique sections reoriented along the horizontal and vertical long and short axes of the left ventricle. The images were analyzed by 3 experienced readers who did not know the results of the coronary angiography and intravascular sonography studies, using the datasets of the stress–rest images. Disagreements were resolved by consensus. For each study, the observers evaluated 8 short-axis, 8 vertical long-axis, and 8 horizontal long-axis slices together with the polar map of the left ventricle image. A perfusion abnormality on the stress image showing partial or complete normalization on the rest image was designated as a reversible defect indicating inducible myocardial ischemia. A semiquantitative score was used to describe the extent and severity of the perfusion defects on the basis of a 13-segment model of the polar plot of the ventricular wall and a 5-point scale ranging from 0 (normal uptake) to 4 (no uptake). The summed reversible defect score was then computed by subtracting the rest score from the summed stress score of all segments (14,15). The septal and anterior myocardial segments were matched to the left anterior descending coronary artery; the inferior, inferoapical, and posterior myocardial segments were matched to the right coronary artery; and the lateral myocardial segments were matched to the left circumflex coronary artery.
Coronary Angiography
Coronary angiography was performed using the Judkins technique and the right femoral artery approach. All angiograms were filmed at 25 frames per second in multiple pairs of orthogonal views using a monoplane multidirectional isocentric radiologic system (Integris 2000 Cardiac; Philips Medical Systems, Best, The Netherlands), and images were interpreted semiquantitatively by 2 experienced angiographers. Quantitative coronary analysis was performed using the diameter of the contrast-free diagnostic catheter for calibration of image magnification. The vessel diameter, the minimal lumen diameter, and the percentage of diameter stenosis were measured at any narrowing site of the investigated vessels using an automatic edge detection computer-assisted analysis system (QCA; Philips).
Intracoronary Doppler Velocity Measurements
After administration of 3000–5000 IU intravenous heparin, adjusted for body weight, an 8-French guiding catheter was used to cannulate the ostium of the coronary arteries and a 0.014-in. floppy intracoronary Doppler guidewire (Flowire; Cardiometrics Inc., Mountain View, CA) was advanced distally into a major branch of the coronary artery system and positioned to obtain the best-quality phasic signal of blood flow velocity. Doppler flow velocities were continuously displayed on the Doppler sonography instrument (Flowmap; Cardiometrics) and recorded on a videotape. Spectral variables were calculated including the average peak velocity and the ratio of the average diastolic to the average systolic peak velocities. Maximal hyperemia was induced by intracoronary bolus injection of adenosine (12 μg for the right coronary artery and 18 μg for the left coronary artery). The coronary flow velocity reserve (CFR) was calculated as the ratio between hyperemic average peak velocity and basal average peak velocity, as previously described (9–12). According to other studies (9–12) and our own experience (12), a CFR less than 2.5 was considered to be abnormal. All measurements were repeated in at least 2 major coronary arteries per patient. Each vessel was classified, according to perfusion scans, as supplying abnormal territories (target vessel) or normal segments (reference vessel). When measurements from more than 1 vessel supplying normal segments were available, the mean value of CFR was used. The ratio of the CFR of the target vessel and the reference vessel (coronary reserve ratio) was calculated as an index of the relative vasodilation capacity of the affected territory (16,17).
Intracoronary Sonography
After flow velocity measurement, the Doppler guidewire was left in place and used to advance the sonography catheter as far distal as possible in each vessel. Intracoronary nitroglycerine, 0.1–0.3 mg, was administered to avoid spasm and to achieve maximum vasodilation of the epicardial vessels. Imaging was performed using intravascular sonographic 2.9- or 3.2-French monorail catheters with polyethylene sheaths (Boston Scientific Corporation, Watertown, MA) incorporating a single-element 30-MHz transducer rotating at 1800 rpm. The intracoronary sonograms were obtained with a Sonos intravascular imaging system (Hewlett-Packard, Palo Alto, CA) and recorded on a videotape for offline analysis. During the study, the imaging catheter was slowly withdrawn manually under fluoroscopic guidance and cross-sectional images of the distal, mid, and proximal sections of the vessel were obtained. During pullback, stop frames were taken at every 5–8 mm of vessel until plaque formation or an abnormality of the coronary wall was found. Atherosclerotic changes in the arterial wall, significant plaque formation, and intimal thickening were defined according to the guidelines for classification and analysis of intracoronary sonograms of the Working Group of Echocardiography of the European Society of Cardiology (13). Stop frames were obtained every 3 mm at the plaque site for quantitative analysis. The lumen area (LA) was determined by computer-assisted planimetry of the lumen–vessel wall interface. The vessel area (VA) was measured by planimetry of the area bounded by the middle echolucent zone (media) and the inner echoreflective adventitial interface. The plaque area (PA) was then calculated as VA − LA, and the cross-sectional relative PA (RPA) was calculated as RPA = PA/VA × 100 and used as an index of the plaque burden at the site of maximal atherosclerotic involvement. A significant plaque burden was defined according to previous publications as a plaque involving more than 40% of the VA (13).
Statistical Analysis
The reproducibility of Doppler velocity signals and dimension measurements from intracoronary sonograms was previously evaluated in our laboratory, yielding mean interobserver and intraobserver variabilities of 7.1% and 4.2%, respectively, which are in keeping with previous reports (9–11,13). Data were expressed as mean values ± 1 SD. Where appropriate, the 2-tailed unpaired t test, the χ2 test, and ANOVA were used to assess statistical significance, with P < 0.05 considered significant. Regression coefficients were obtained using linear regression analysis.
RESULTS
Exercise perfusion images showed mild to moderate reversible perfusion defects in all patients. The median value of the summed reversible score was 3 (range, 1–6). Intracoronary sonograms were obtained in 45 vessels (2.25 vessels per patient). According to perfusion mapping, 20 vessels were classified as supplying underperfused segments (target) and 25 were classified as supplying normal territories (reference).
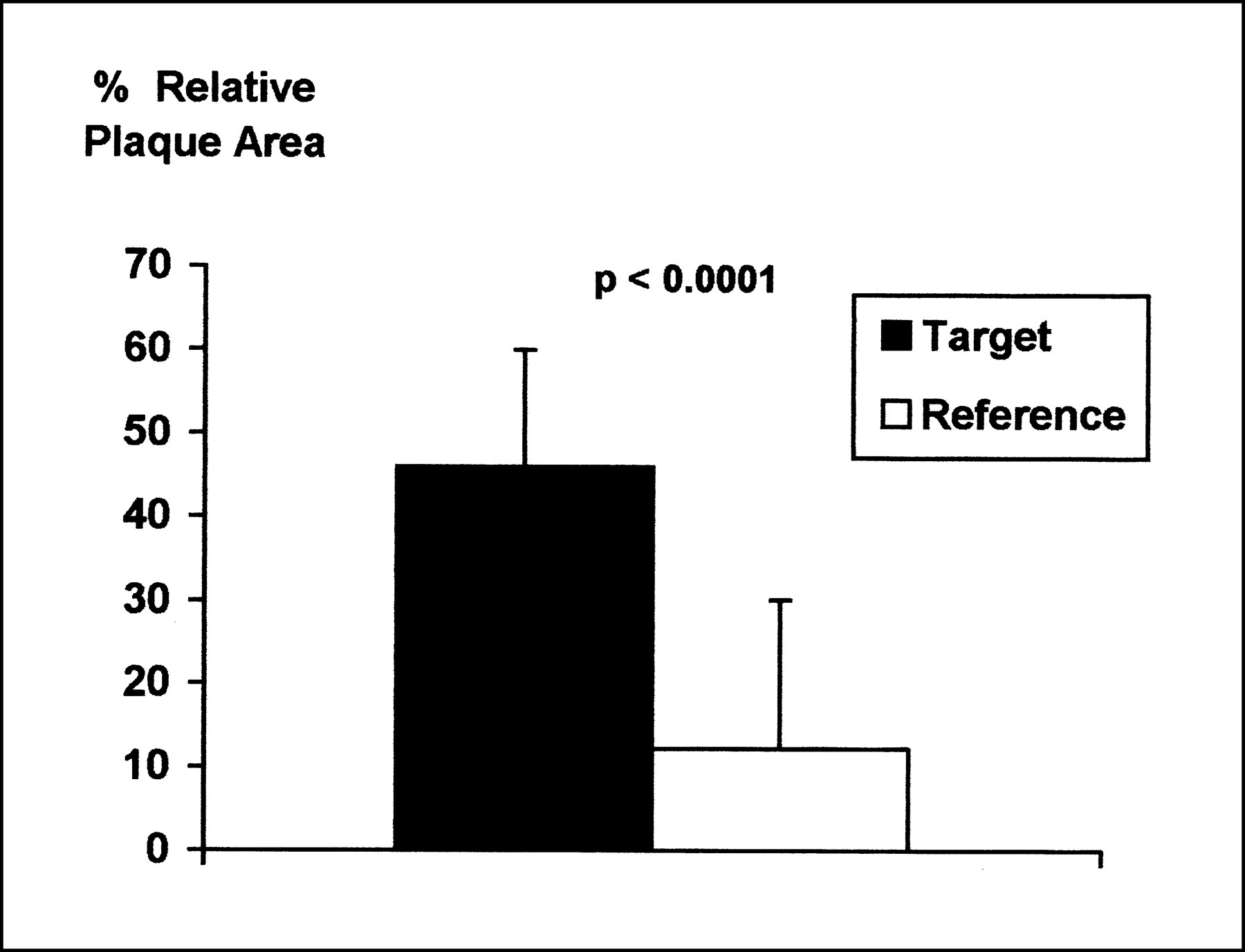
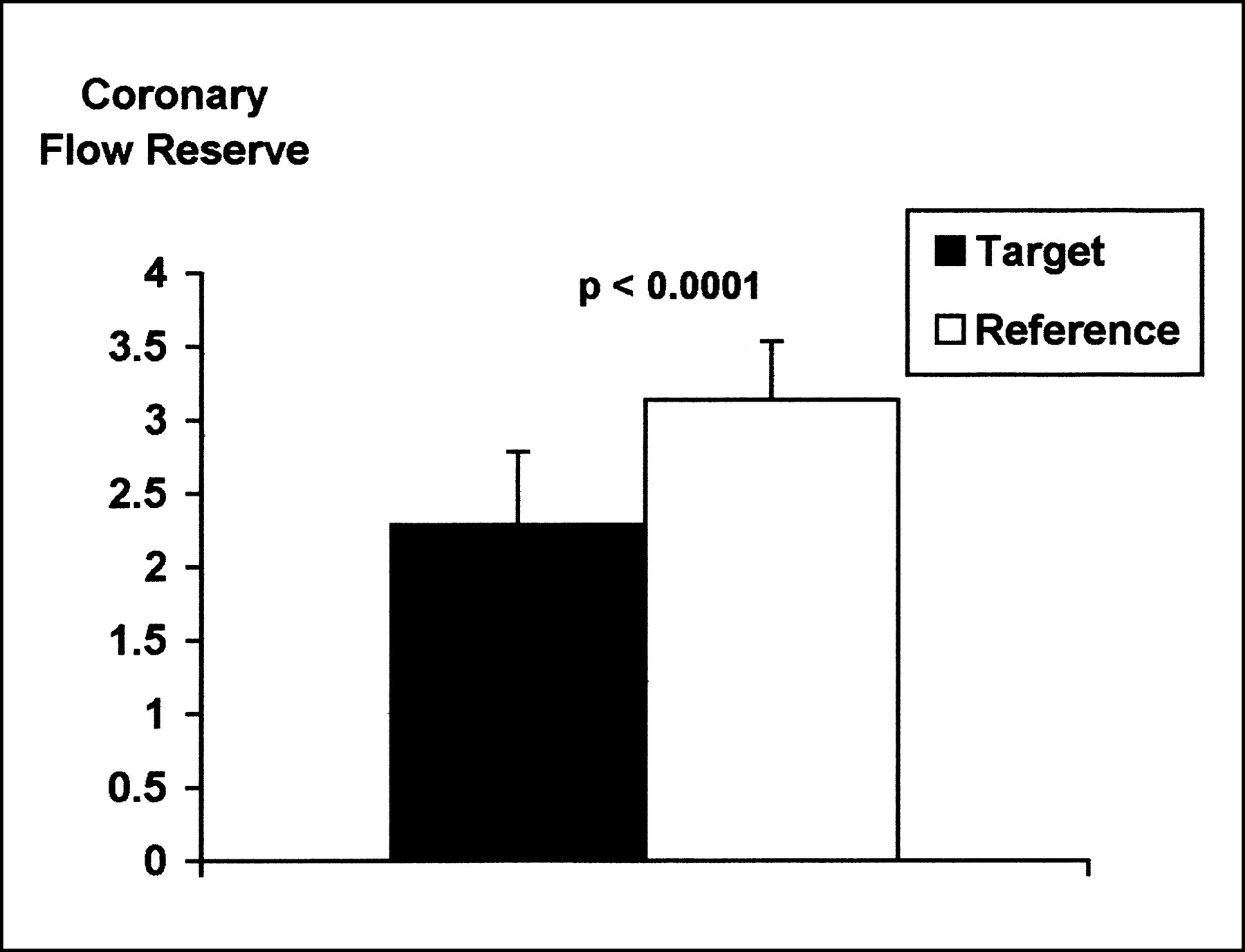
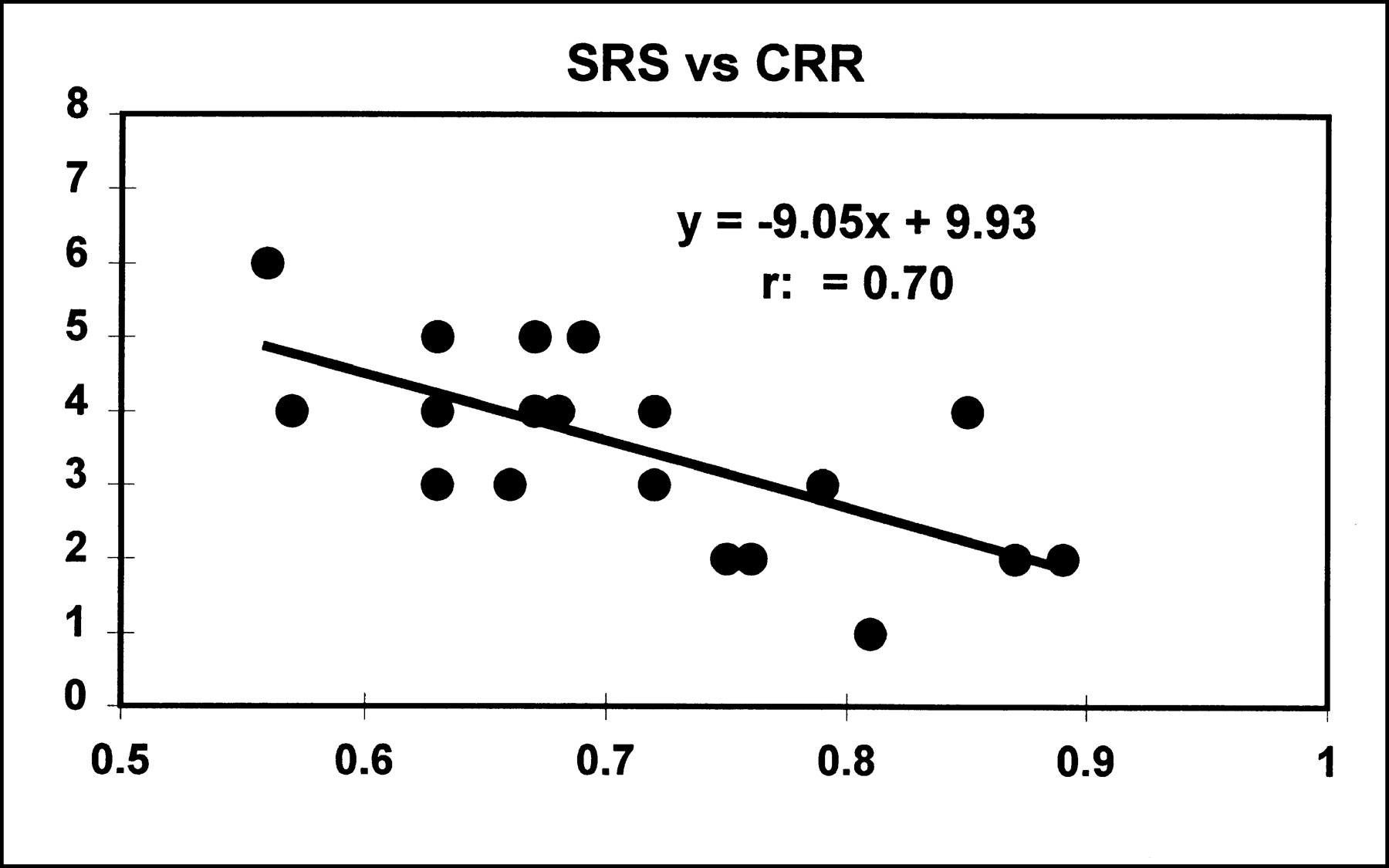
Intracoronary sonograms showed occult atherosclerotic changes unrecognized by angiography in 19 patients (95%). A significant plaque burden (RPA > 40%) was seen in 16 patients (80%). Four patients (20%) showed minor changes, including localized intimal thickening or small, soft, and eccentric plaque formation. Ten patients (50%) had only mild atherosclerosis, with focal plaque formation and an eccentric distribution of mixed (fibroadipous) or soft plaque tissue with no calcifications. Five additional subjects (25%) showed more diffuse changes, including more concentric and calcified lesions. Plaque formation was observed more frequently in the target vessel than in the reference vessels of each patient (70% versus 15%; χ2 = 9.97; P < 0.0001). Mean RPA was significantly greater in the target vessels (46% ± 14%) than in the reference vessels (12% ± 18%; P < 0.0001) (Fig. 1). Measurements of Doppler flow velocity showed abnormal vasodilator capacity during adenosine infusion (CFR < 2.5) in 14 patients (70%). Again, mean CFR was significantly lower in the target vessels than in the reference vessels (2.3 ± 0.5 versus 3.1 ± 0.6; P < 0.0001) (Fig. 2). A significant inverse correlation was present between the summed reversible score and the coronary reserve ratio (y = 9.05x − 9.9; r = 0.70; P < 0.005) (Fig. 3), indicating that abnormal perfusion scans were actually associated with significant heterogeneity of the coronary vasodilation capacity. Typical intravascular sonography, myocardial perfusion, and coronary angiographic findings from a study patient are shown in Figure 4.

Mean RPA at site of maximum plaque concentration by intravascular sonography as estimate of plaque burden in target vessels and reference vessels.

Mean Doppler CFR in target vessels and reference vessels.

Relationship between summed reversible defect score (SRS) by exercise 99mTc-sestamibi scintigraphy and ratio of CFR of target and reference vessels (coronary reserve ratio [CRR]).
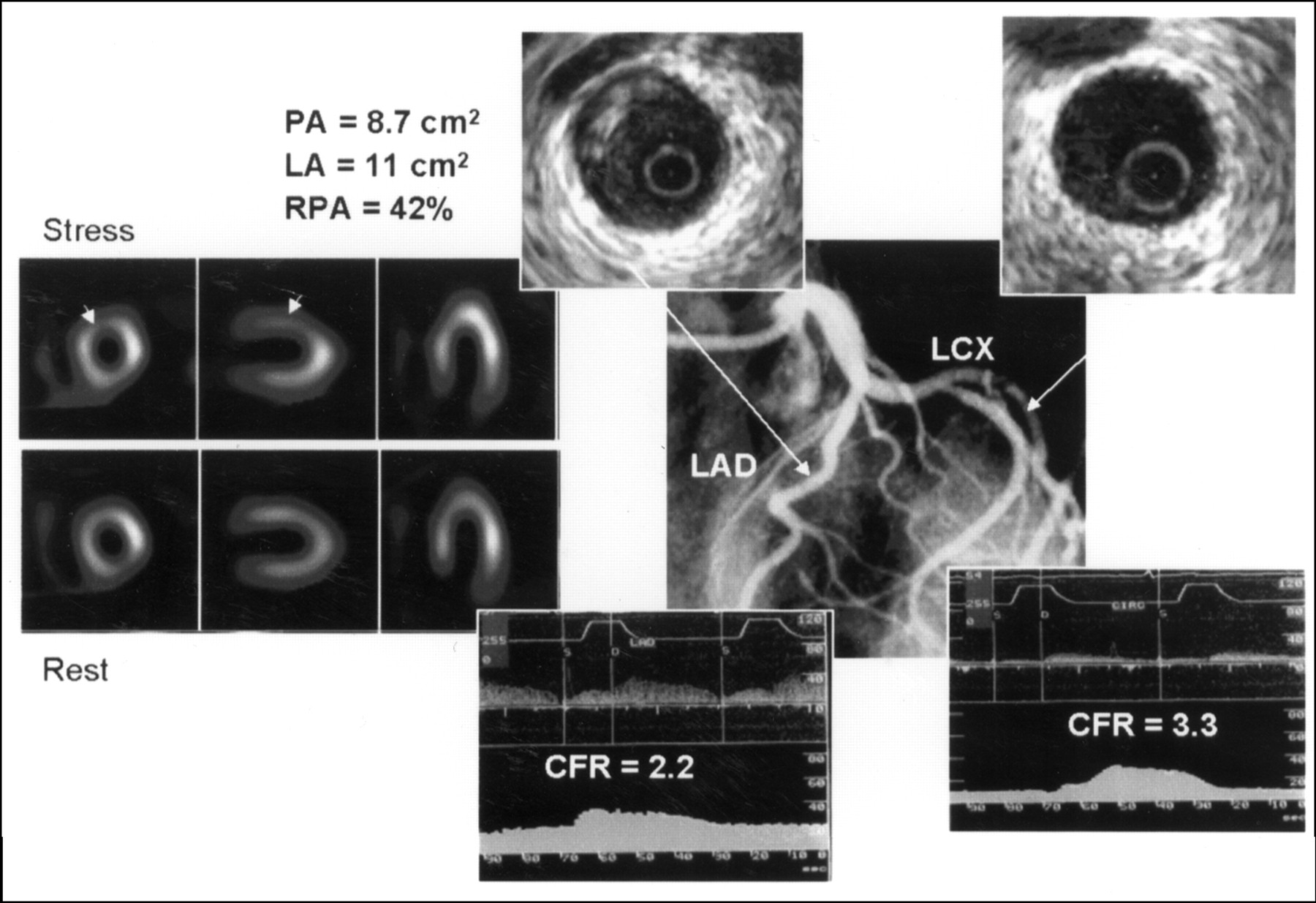
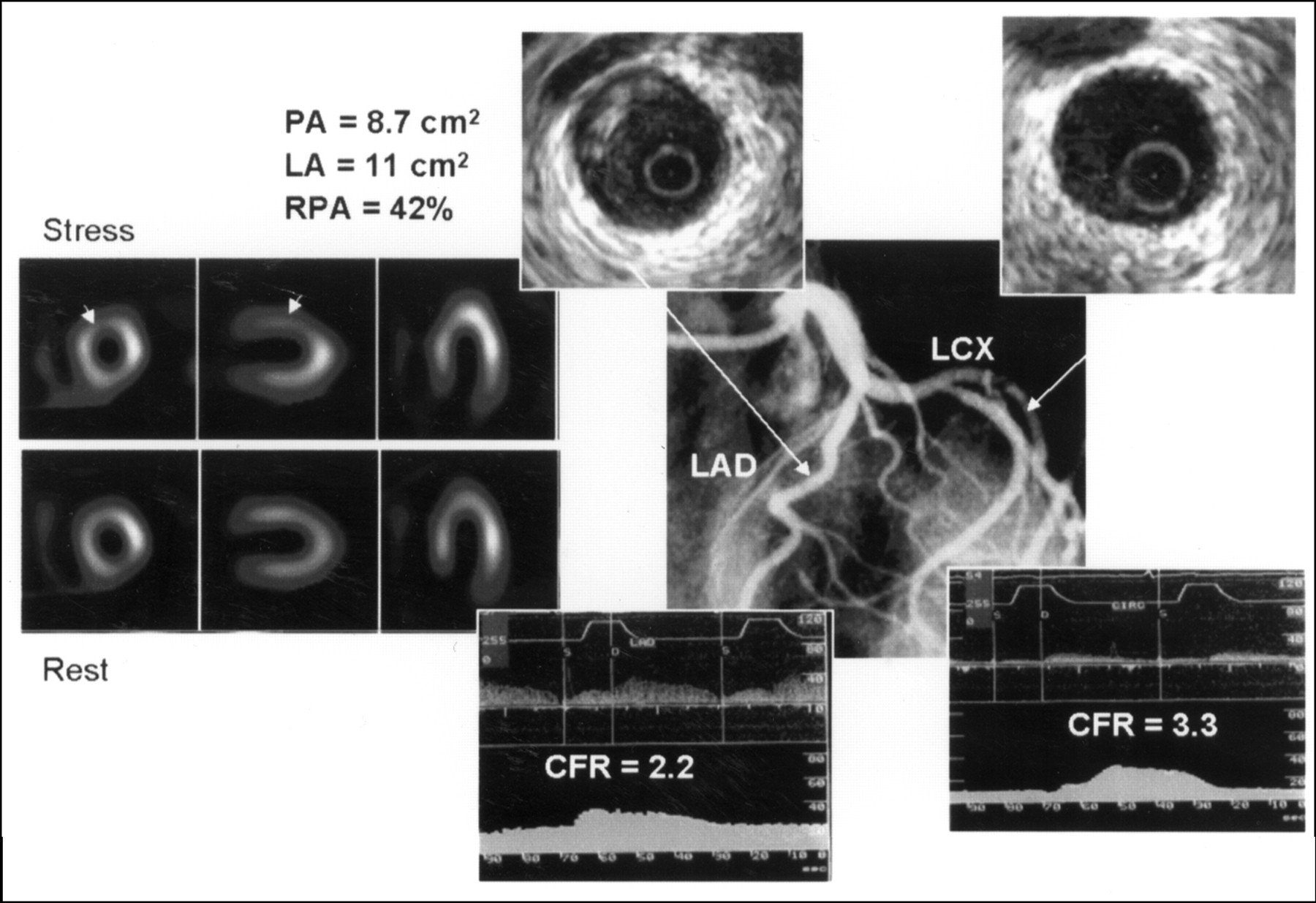
Findings from exercise myocardial scintigraphy (left middle image), coronary angiography (right middle image), intravascular sonography (top 2 images), and Doppler flow velocity measurement (bottom 2 images) for 56-y-old woman with chest pain on exercise and reversible perfusion defect of anterior left ventricular wall (arrows). Intravascular sonography shows eccentric soft plaque, missed by angiography, involving mid left anterior descending (LAD) artery. This finding is associated with relative reduction of CFR in territory of LAD artery. LA = lumen area; LCX = left circumflex artery.
DISCUSSION
The accuracy of myocardial perfusion scintigraphy in the detection of significant coronary artery disease has been reported to be in the range of 85%–98% (1,3). Several factors may affect the specificity of myocardial perfusion scans, including poor-quality imaging, artifacts caused by soft-tissue attenuation and interposition of extracardiac structures, or clinical conditions such as cardiomyopathy, mitral valve prolapse, intramyocardial masses, and conduction abnormalities (4–8). Artifacts related to soft-tissue attenuation and nonuniformity of background activity have commonly been encountered with planar thallium myocardial imaging, in part related to the low physical-energy emission of 201Tl.
Technical improvements in myocardial perfusion tracers and image quality, such as attenuation correction and electrocardiographic gating of tomographic images, have been introduced to attempt to reduce the frequency of artifactual defects (5–7). Nevertheless, reversible perfusion defects have been reported in up to 27% of selected patients with angina and normal findings on coronary angiography (18–22). Perfusion abnormalities have also been described in asymptomatic patients with familial hypercholesterolemia (23) and systemic hypertension (24). The issue of whether abnormal scan findings should represent true perfusion changes or may be interpreted as false-positive remains controversial in nuclear cardiology. Arguments in favor of false-positive results are based on the presence of artifacts, whereas arguments for true coronary flow abnormalities are based on the presence of microcirculatory impairment or endothelial dysfunction. Impairment in coronary vasodilation reserve has been shown in patients with angina and normal coronary angiograms and has been attributed to the presence of coronary microvascular dysfunction (25). Although the evidence of a role for small-vessel disease is good, Wiedermann et al. (26) reported that in most patients presenting with this syndrome, intravascular sonography also shows abnormal epicardial coronary arteries. Early atheromatous plaques and intimal thickening, missed by coronary angiography, were associated with an abnormal (constrictive) response to exercise. This anatomic and physiologic heterogeneity in patients with angina and normal coronary angiography findings has been confirmed in a combined intracoronary sonography and Doppler flow velocity study by Erbel et al. (27). In that study, occult atherosclerosis and plaque formation were found in the left anterior descending and left main coronary arteries of 48% of 44 patients with chest pain and normal coronary angiography findings. Of the 44 patients included in that study, SPECT images were available for only 29 (66%) but showed abnormal findings in 93% of patients with abnormal sonography findings and in only 28% of patients with normal vessels. Only a minority of patients (16%) showed reduced coronary flow reserve in the absence of plaque formation by intracoronary sonography (true microvascular dysfunction). Measurements of coronary flow reserve were obtained with a Doppler catheter positioned in only the proximal left anterior descending artery, using intracoronary papaverine as the hyperemic agent. Measurements were not obtained from other vessels, and the territories corresponding to the location of perfusion defects were not separated from reference territories. Likewise, intracoronary sonograms were obtained from only the left anterior descending and left main coronary arteries. SPECT with 99mTc-methoxyisobutyl isonitrile was performed on only 29 patients (66%) and was visually interpreted and categorized as positive or negative without details on defect size and location.
Our study confirms the observation of Erbel et al. (27) that early signs of atherosclerosis missed by coronary angiography are common in patients with angina and normal coronary arteries. Moreover, we have shown that early signs of atherosclerosis revealed by coronary sonography are more frequent, and usually more advanced, in the coronary territory corresponding to myocardial perfusion defects than in the reference territories.
In addition, with the Doppler guidewire technique we evaluated regional CFR in the bed distribution of either the abnormal scintigraphic segment or the reference regions. A reduction in coronary flow reserve was more frequent in the distribution of perfusion defects than in the reference territory. We also found a significant relationship between the scintigraphic perfusion defect score and the relative impairment of the coronary flow reserve as assessed by the CFR ratio.
The relationship between regional abnormalities of perfusion scans and coronary flow reserve has been investigated in previous studies using different techniques. One of the earlier studies (21) was performed in a few patients with abnormal planar thallium imaging using digital angiography to measure coronary flow reserve and a relatively weak hyperemic agent such as contrast medium. In this study, we used tomographic sestamibi imaging, selective intravascular flow velocity measurements, and intracoronary adenosine as the hyperemic agent. Adenosine testing has been shown to induce a perfusion defect in the same area and to the same extent as the perfusion defect observed at exercise in patients with syndrome X (28) and in patients with coronary artery disease (16,29). Measurement of CFR with Doppler guidewires has been shown to be accurate and reproducible in human studies and to permit selective access to distal vessels and side branches (9,16).
This study provides new evidence supporting the concept that an abnormal scintigraphy finding, rather than being false-positive, may be an early marker of vasomotion changes associated with occult atherosclerosis in patients with angina and normal coronary angiography findings. The pathophysiologic link between early atherosclerotic changes of the epicardial vessels and an abnormal vasodilation capacity of the underlying microvasculature remains elusive. Several complex mechanisms may be involved in the regulation of coronary vasomotion in early atherosclerosis (22,30). Endothelial dysfunction has been found to be associated with the early stages of atherosclerotic involvement of the coronary epicardial vessels in humans (30). In addition, reports show that impairment of endothelium-dependent coronary vasodilation may result in myocardial perfusion defects (31). The small cohort of patients included in this study did not allow an evaluation of the relative influence of coronary risk factors and cholesterol levels on coronary vasomotion and perfusion changes. Among conventional coronary risk factors, serum cholesterol levels have been found to affect vasomotion of human coronary arteries (30,32). Also, short-term cholesterol lowering has been found to possibly decrease the size and severity of perfusion abnormalities revealed by PET in patients with coronary artery disease (32).
The study had some limitations. We studied a relatively small and selected population of consecutive patients with chest pain and angiographically normal coronary arteries who had abnormal stress perfusion findings. Patients with cardiomyopathy, atypical chest pain, or left bundle branch block were excluded. The mean age was 58.9 ± 10 y, and most patients had typical symptoms and coronary risk factors. Consistent evidence of myocardial ischemia was present in most patients and—of particular note—3 patients presented with a history of unstable angina and 5 had a history of non–Q wave myocardial infarction. Therefore, a possible criticism to our observations is that atherosclerotic and vasomotion changes may be a nonspecific finding in a population expected, on the basis of clinical presentation, to have a high prevalence of atherosclerotic disease. However, the close relationship between the distribution of regional perfusion abnormalities and the atherosclerotic and vasomotion changes observed in the related vessel make this possibility unlikely.
Doppler flow velocity and intravascular sonography measurements have few well-known limitations or pitfalls. However, several studies have shown the overall accuracy of these techniques either in patients with overt coronary artery disease or in patients with chest pain and insignificant disease (13,16).
CONCLUSION
Our findings, together with previous observations, suggest that the tendency to dismiss abnormal exercise perfusion findings as false-positive in patients with chest pain, abnormal exercise electrocardiography findings, and normal coronary angiography findings may be unjustified. Angiography is a silhouette technique with substantial limitations. Intracoronary sonography and Doppler flow mapping provide new, accurate tools for evaluating the morphology and function of the coronary circulation that may overcome the limitations of coronary angiography. We therefore suggest examining patients who have abnormal scintigraphy findings and angiographically normal coronary arteries using intravascular sonography and flow mapping to definitively assess the presence or absence of disease. Further studies are required to determine whether the detection of significant occult atherosclerosis and associated vasomotion changes may have prognostic implications that require more attentive consideration of a patient's symptoms and signs and more aggressive treatment of coronary risk factors.
Footnotes
Received Nov. 5, 1999; revision accepted May 5, 2000.
For correspondence or reprints contact: Luca Ceriani, MD, Department of Nuclear Medicine, Ospedale di Circolo and Fondazione Macchi, Viale Borri, 57, I-21100 Varese, Italy.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- False-Positive Stress Echocardiograms: A Continuing Challenge
- The Prevalence of Microvascular Dysfunction, Its Role Among Men, and Links With Adverse Outcomes: Noninvasive Imaging Reveals the Tip of the Iceberg
- Structural Abnormalities of the Coronary Arterial Wall--in Addition to Luminal Narrowing--Affect Myocardial Blood Flow Reserve
- Coronary Microvascular Reactivity to Adenosine Predicts Adverse Outcome in Women Evaluated for Suspected Ischemia: Results From the National Heart, Lung and Blood Institute WISE (Women's Ischemia Syndrome Evaluation) Study
- Stress-Rest Myocardial Perfusion SPECT for Functional Assessment of Coronary Arteries with Anomalous Origin or Course
- Detecting Occult Coronary Disease in a High-Risk Asymptomatic Population
- 99mTc-N-NOET Imaging for Myocardial Perfusion: Can It Offer More Than We Already Have?