


Abstract
Anomalous coronary arteries (ACAs) may be clinically silent and totally benign or associated with catastrophic and fatal presentations. It has been postulated that the proximal course of an ACA is a decisive factor in risk stratification and surgical approach. Particularly, a course between the aorta and pulmonary trunk carries a high risk of major adverse events. We sought to evaluate the anatomic course of documented ACAs by transesophageal echocardiography (TEE) and to study their functional importance using stress–rest 99mTc-sestamibi (99mTc-MIBI) myocardial perfusion SPECT. Methods: From a cohort of patients undergoing coronary angiography in our department between January 1997 and April 2003, we selected 14 with ACAs but without CAD (9 men and 5 women; mean age, 50.7 ± 14.6 y). All patients underwent TEE and stress–rest 99mTc-MIBI myocardial perfusion SPECT. Results: TEE correctly identified the origin of all ACAs and revealed an anomalous course between the great vessels in 5 patients. At exercise myocardial perfusion SPECT, 4 of 14 patients demonstrated a reversible myocardial perfusion defect. All these patients had an anomalous course between the aorta and pulmonary artery. Conclusion: In this study, 4 of 5 (80%) anomalous courses between the aorta and pulmonary artery were associated with the finding of a reversible perfusion defect on stress–rest SPECT. An integrated evaluation of anatomic course and hemodynamic importance could be useful in the management of ACA.
The incidence of congenital coronary anomalies in the general population is reported to be between 0.46% and 1.55% (1–4). Coronary anomalies may occur in conjunction with complex congenital heart diseases or as isolated abnormalities, and their clinical manifestations vary widely. On the one extreme, they may be clinically silent, totally benign, and discovered by chance; on the other extreme, they may cause angina pectoris, syncope, arrhythmias, myocardial infarction, and sudden cardiac death, resulting in significant morbidity and mortality even among young adults (5).
An anomalous coronary artery (ACA) that courses between the aorta and pulmonary trunk, either within or outside the aortic wall, is associated with sudden cardiac death, often occurring during or immediately after strenuous physical activity (6). In these cases, it is postulated that marked augmentation of cardiac output causes the aorta and right ventricular outflow tract to dilate, leading to torsion or kinking of the ACA. To our knowledge, no reported studies have confirmed this pathophysiologic hypothesis. Little information is available about stress-induced ischemia in patients with ACA.
The ability of stress–rest 99mTc-sestamibi (99mTc-MIBI) myocardial perfusion SPECT to provide myocardial perfusion data offers a unique opportunity to evaluate the functional importance of ACAs on myocardial perfusion during stress. Knowledge of this functional importance can be useful in assessing prognostic value and in planning corrective surgery.
Detecting a vessel course on the basis of only a coronary angiogram may be difficult. In fact, this technique provides only a silhouette of the ACA and does not reliably delineate its course in relation to the aorta or pulmonary trunk. Transesophageal echocardiography (TEE) is a noninvasive method allowing tomographic visualization of the proximal tract of coronary arteries. The origin of a coronary artery from an anomalous aortic location or a proximal anomalous course of a coronary artery can therefore reliably be identified with TEE, and numerous reports in the literature have documented its usefulness in such cases (7,8).
We sought to evaluate the anatomic course of cases of ACA that had been documented by TEE and to study the functional importance using stress–rest 99mTc-MIBI myocardial perfusion SPECT in order to more correctly manage these anomalies.
MATERIALS AND METHODS
We considered only major ACAs (9,10) (capable of causing relevant clinical consequences) of origination and course present in our database and did not consider anomalies of intrinsic coronary arterial anatomy (e.g., coronary hypoplasia or myocardial bridge) or of coronary termination (e.g., fistulas or anomalous collateral vessels).
Study Population
Nineteen consecutive patients with coronary arteries of confirmed anomalous origin or course were identified from the cohort of those undergoing coronary angiography in our department from January 1997 to April 2003. Coronary angiography was performed because of chest pain or electrocardiography (ECG) signs of ischemia.
We selected 14 (73.7%) of the 19 patients (9 men, 5 women; mean age ± SD, 50.7 ± 14.6 y) without angiographic coronary stenoses to reduce the number of false-positive myocardial perfusion scintigraphy findings (11). Among these 14 patients, 6 had hypertension, 4 had hypercholesterolemia, 1 had diabetes mellitus, 2 had recurrent syncope, 1 had severe mitral regurgitation, 1 had a previous non–Q wave myocardial infarction, and 1 had persistent atrial fibrillation.
Study Protocol
After coronary angiography, all the patients underwent TEE with commercially available 5-MHz transesophageal transducers attached to electronic sector scanners (Sequoia [Acuson] or Sonos 5500 [Hewlett Packard]) to better evaluate the course of ACA with regard to the aorta and pulmonary artery.
In all patients, the functional importance of ACA was assessed through stress–rest 99mTc-MIBI SPECT, performed with 2-d protocols. A dose of 740 MBq of 99mTc-MIBI was intravenously injected at peak exercise, and stress lasted for another minute. Rest scintigraphy was performed the following day with the same dose of radiopharmaceuticals.
Stress and rest images were acquired 45–60 min after 99mTc-MIBI administration. SPECT data were obtained over a 180° orbit from the right anterior oblique 45° view to the left posterior oblique 45° view, using a large-field-of-view γ-camera with high-resolution collimators (Starcam 4000; General Electric Medical Systems). For image acquisition, a 20% acceptance window around the 140-keV photopeak was used. Thirty-two projections were acquired at 30 s per projection, and a 64 × 64 matrix was used.
Exercise stress was performed using a Bruce protocol treadmill test. Accepted endpoints for the exercise test included achievement of 85% of the target heart rate, >2-mm ST-segment depression on the ECG, or typical ischemic chest pain. For terminating the exercise test, the absolute and relative indications we used were those of the practice guidelines of the American College of Cardiology (ACC) and the American Hospital Association (AHA) (12).
Filtered backprojection was performed using a low-resolution Butterworth filter with a cutoff frequency of 0.5 cycles per pixel and an order of 5.0. No attenuation or scatter correction was applied. The transaxial tomographic slices were reoriented into short-axis, horizontal long-axis, and vertical long-axis views.
Vascular territories were assigned on the basis of the 17-myocardial-segment model of the guidelines of the ACC, AHA, and American Society of Nuclear Cardiology: Anterior, septal, and apical segments included the left anterior descending artery territory; lateral segments included the left circumflex coronary artery (Cx) territory; and inferior segments included the right coronary artery (RCA) territory (13). All images were visually interpreted using a semiquantitative method (4-point grading system for perfusion: normal = 0, mildly reduced = 1, severely reduced = 2, and absent = 3) by a consensus of at least 2 experienced observers who had no knowledge of the clinical or TEE findings. A perfusion defect seen on the exercise images was identified as reversible if it resolved at rest; a perfusion defect seen on the exercise images was identified as fixed if it persisted at rest.
RESULTS
Coronary Angiography Findings
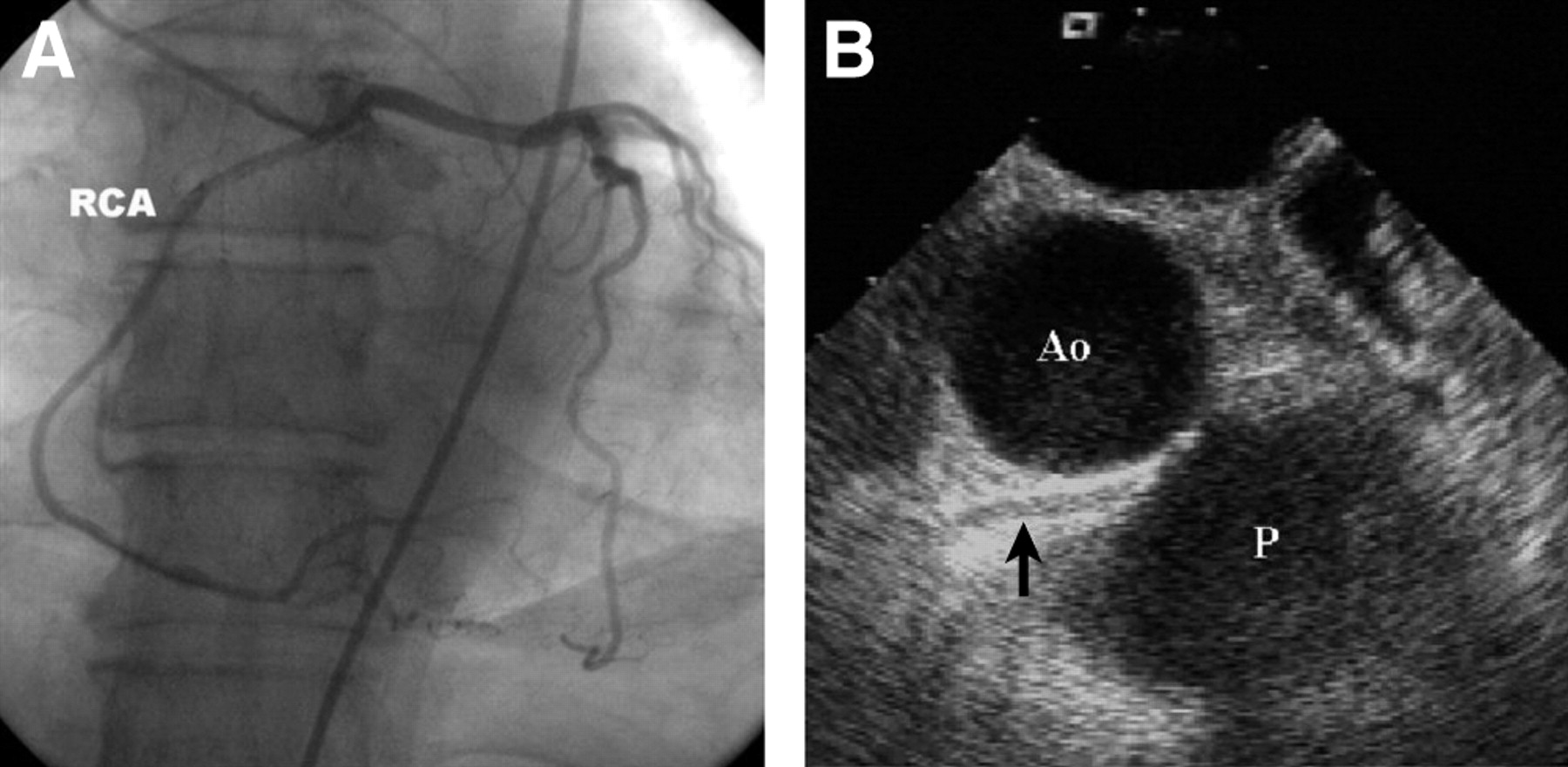
In 4 patients, the RCA originated from the left sinus of Valsalva: In 3 of 4 the RCA coursed between the great vessels (Fig. 1A), and in 1 of 4 the RCA was posterior to the aorta. In 1 patient, the left coronary artery originated from the right sinus of Valsalva and coursed between the aorta and pulmonary artery. The Cx originated from the right sinus of Valsalva in 3 patients (in 2 of 3 the Cx coursed posteriorly to the aorta, and in 1 of 3 anteriorly, to reach its normal location). The Cx originated from the proximal portion of the RCA in 2 patients. One patient had a single coronary artery arising from the right coronary sinus and coursing with the Cx posterior to the aorta and with the left anterior descending coronary artery between the great vessels. Three patients had an RCA originating higher than normal on the ascending aorta (Table 1).
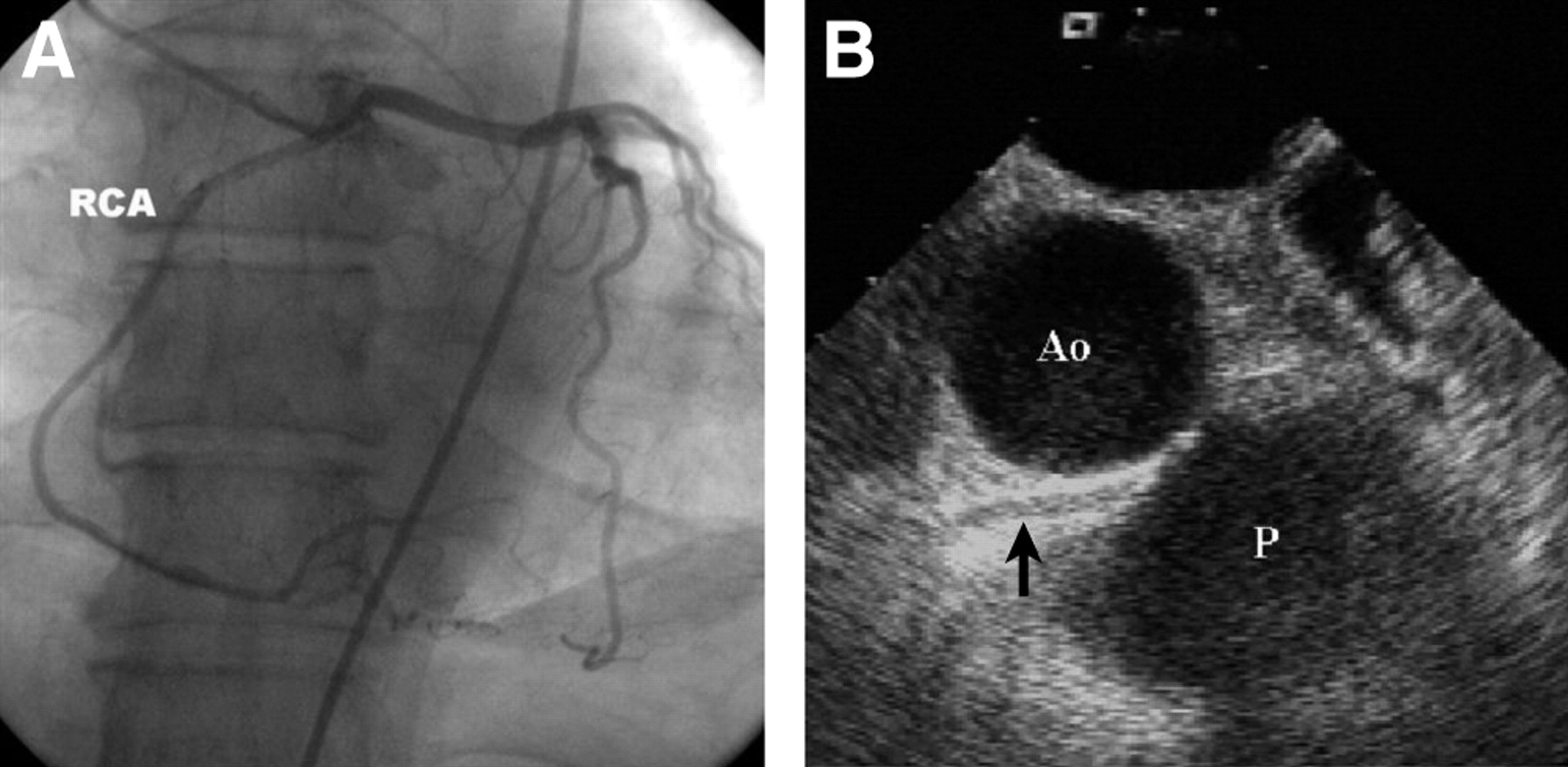
(A) Coronary angiography (anteroposterior projection) of patient 1. The RCA originates in the left main trunk from the left sinus of Valsalva. (B) TEE (basal view, short axis at 35°) shows that the anomalous RCA (arrow) courses between the aorta (Ao) and the pulmonary artery (P).
Clinical Presentation and Angiographic, Transesophageal Echocardiographic, and Scintigraphic Findings
TEE Findings
TEE correctly identified all anomalous origins of coronary arteries and identified an anomalous course between the great vessels in 5 cases (Fig. 1B). To evaluate any abnormalities of left ventricular function, we obtained a complete scan of ventricular chambers. In 13 patients, TEE showed a good left ventricular ejection fraction (mean, 60% ± 2%), without regional abnormalities. In only 1 patient, hypokinesis of the proximal segment of the lateral left ventricular wall, with a preserved ejection fraction, was identified.
Stress–Rest Myocardial Perfusion Scintigraphy Findings
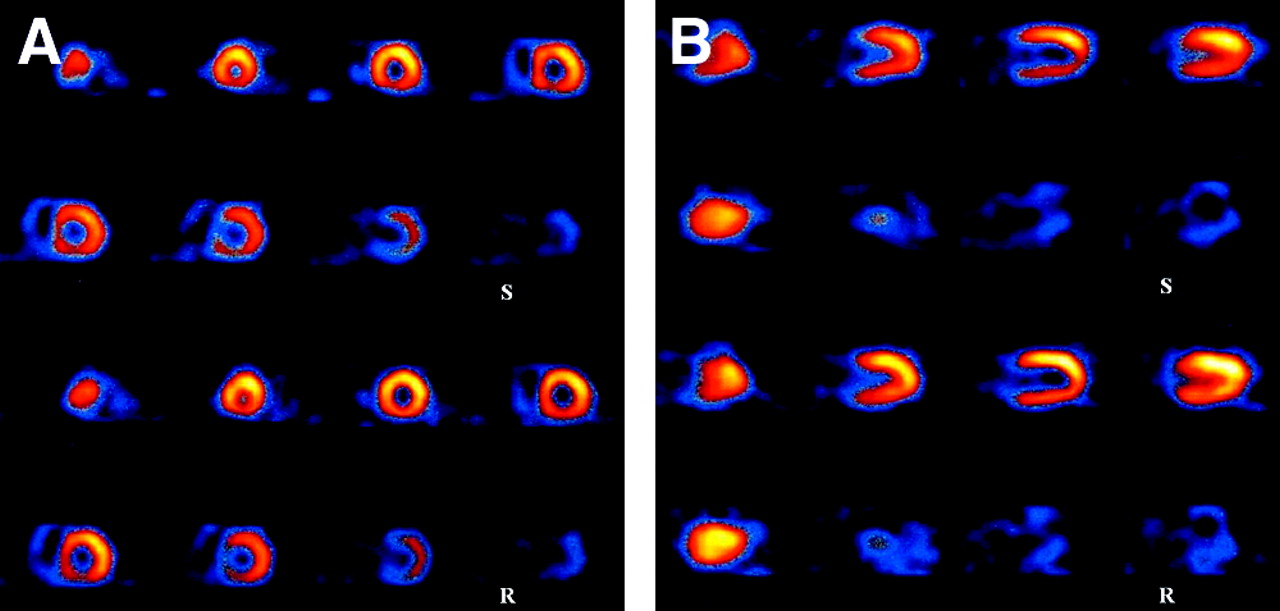
Stress–rest 99mTc-MIBI SPECT was performed on all 14 patients with documented ACA. No patient experienced myocardial infarction or ventricular fibrillation during the test. Four (28.6%) of the 14 patients precociously interrupted the stress; the other 10 (71.4%) reached their target heart rate. Normal perfusion with no ECG sign or symptom of ischemia was observed in 5 patients, and a reversible myocardial perfusion defect was detected in 4 (Fig. 2), all of whom had a coronary artery with an anomalous course between the great vessels (2 had reversible ST-segment depression, 1 complained of transient chest pain, and 1 experienced dyspnea during effort). Another patient, who had a Cx with an anomalous origin from the right coronary sinus, had a small fixed perfusion defect in the proximal segment of the posterolateral left ventricular wall. This patient had experienced a previous posterolateral non–Q wave myocardial infarction. At coronary angiography, the patient was seen to have insignificant stenosis (less than 50% of the lumen diameter) in the Cx, and TEE showed the course of the ACA to be posterior to the aorta, with hypokinesis of the proximal segment of the lateral wall (ejection fraction, 55%). The small entity of ischemia may be considered a consequence of coronary artery or microvascular dysfunction combined with insignificant coronary artery stenosis. In fact, the patient was referred only because of dyspnea and had no chest pain or other clinical or instrumental signs of myocardial ischemia.

Myocardial stress–rest 99mTc MIBI SPECT images of patient 1: short-axis slices (A) and vertical long-axis slices (B). A stress-induced reversible myocardial perfusion defect is visible in the proximal and middle portions of the inferior wall. S = stress; R = rest.
Among the 4 of 14 patients who did not reach the target threshold, 2 patients (patients 6 and 8), both with a Cx arising from the right sinus of Valsalva, interrupted exercise testing because of the onset of transient upsloping ST-segment depression (1 mm). Patient 6 interrupted exercise testing at 78% of the predicted maximum heart rate (100 W), and patient 8, at 82% (125 W). No perfusion defect was detected on SPECT for either patient. The ECG abnormalities are reasonably attributable to confounders of stress test interpretation and not to the presence of ACA. In fact, patients 6 and 8 had a right bundle branch block and mild left ventricular hypertrophy, respectively. In the other 2 patients (patients 12 and 3) of the 4 who did not reach the target threshold, testing was interrupted because of stress-induced angina. Patient 12 interrupted testing at 81% of the predicted maximum heart rate (75 W), and patient 3, at 68% (100 W). Patient 3 had an anomalous RCA origin coursing between the great vessels and no myocardial perfusion defects on SPECT. Other patients with the same ACA who reached their predicted maximum heart rate showed perfusion defects. Although reported to be high, the sensitivity of stress–rest 99mTc-MIBI SPECT for diagnosing myocardial ischemia depends on the values of maximum heart rate achieved. In patient 3, who showed no ECG sign of ischemia or perfusion defects, one can assume that a higher workload could produce myocardial ischemia, as occurred in other patients with the same ACA. For these reasons, this patient is periodically followed up, and if a new episode of angina occurs, another stress test will be planned. Patient 12 had a high RCA origin and hypertension, and effort caused angina even at presentation. Like other patients with the same ACA who reached the target threshold, he did not show myocardial perfusion defects.
On semiquantitative analysis of the findings of stress–rest myocardial perfusion SPECT (Table 1), 9 of the 14 patients did not show any myocardial perfusion defect (severity score = 0). Of the 2 patients (patients 1 and 2) with an RCA arising from the left sinus of Valsalva and coursing between the great vessels, patient 1 had a reversible perfusion defect on the proximal segment, and patient 2 on the proximal and medium segments, of the inferior wall; both patients had a severely reduced perfusion score (severity score = 2 and 3, respectively). The patient with a left coronary artery arising from the right sinus of Valsalva and a course between the great vessels (patient 5) had a reversible perfusion defect on the distal segment of the anterior wall (severity score = 2). A reversible perfusion defect on the medium and distal segments of the anterior wall (severity score = 3) and on the proximal segment of the inferior wall (severity score = 2) was also found in the patient with a single coronary artery and a left anterior descending coronary artery coursing between the aorta and pulmonary artery (patient 11). Finally, a fixed defect on the proximal tract of the posterolateral wall (severity score = 3) was detected in the patient with a Cx arising from the RCA (patient 9).
DISCUSSION
In this study, we assessed the functional importance of ACAs by stress–rest 99mTc-MIBI SPECT after coronary angiography and TEE evaluations. SPECT images detected reversible myocardial perfusion defects during stress in 4 of 14 patients with ACA. All these patients had an anomalous course between the aorta and pulmonary artery, and a surgical approach was successively planned.
For several decades, the only method for the premorbid diagnosis of coronary artery anomalies was invasive coronary angiography (14). However, TEE, a well-tolerated but moderately invasive test, can also reliably identify coronary arteries of anomalous origin or of a proximal anomalous course. Up to now, TEE has been used to image coronary anomalies only in small series and case reports (7,8). The largest TEE series in the literature included 9 patients with coronary anomalies previously detected by coronary angiography (7), in which TEE did confirm the origin and initial course of the anomalous vessels. As in our study, the TEE images in that series were acquired and analyzed with prior knowledge of the angiographic findings. Thus, the ability of TEE to identify coronary anomalies in a masked analysis remains unreported. Even in that series, TEE correctly and accurately identified every anomalous origin and course of coronary arteries.
Both identifying the presence of an ACA and defining its proximal course with respect to the aorta and pulmonary artery are essential in distinguishing a malignant from a benign disorder. In fact, most coronary arteries of anomalous origin are benign and myocardial perfusion is normal. For example, an anomalous Cx follows a benign, retroaortic course in most situations and enters the proximal left atrioventricular groove as if originating as a proximal branch of the left main coronary artery. A single coronary artery is rare, with an incidence of approximately 0.024% in the general population (15). It is characterized by a single aortic ostium and, despite a report of sudden death in an infant (16), has limited clinical relevance in adults. It tends to be associated with complex congenital heart disease and is detected long before adulthood (17). In our study, the single coronary artery was detected at coronary angiography, and TEE showed that the left anterior descending coronary artery coursed between the aorta and pulmonary artery and that the Cx coursed posteriorly to the aorta. This patient also had a reversible perfusion defect in the anterior and inferior walls on stress–rest 99mTc-MIBI SPECT.
In contrast, a left main stem with an aberrant origin in the right aortic sinus of Valsalva, and an RCA with an aberrant origin in the left aortic sinus of Valsalva, are the most common anomalies associated with angina pectoris, myocardial infarction, or sudden cardiac death (18), probably because of abnormal myocardial perfusion. For these 2 coronary anomalies, a malignant prognosis is assigned and surgery is recommended (19). The most widely accepted pathophysiologic explanation for the association between these 2 aberrant origins and fatal events is that these ACAs follow an anomalous course between the great vessels to reach their normal location. Thus, the aorta and pulmonary artery impinge on the proximal anomalous vessel, especially during exercise, when the aortic and pulmonary artery dilate in response to increased cardiac output coincident with increased coronary flow demand. This mechanism was also suggested by the results of a perfusion cardiovascular MRI study in 3 patients with ACA (20). Another underlying mechanism assumed to explain stress-induced ischemia in ACA is that, during extreme exertion, certain intervening autocrine dysfunction may induce autonomic or endothelial dysfunction, causing spasm or acute thrombosis at anomalous sites (4). In our study, all 5 of the 14 patients with a coronary artery of documented anomalous course between the aorta and pulmonary artery presented with effort-induced angina, and 1 of 5 had recurrent episodes of syncope. Moreover, in this setting, as in a previous study (21), 4 (80%) of 5 anomalous courses between the great vessels were associated with a reversible myocardial perfusion defect detected by stress–rest 99mTc-MIBI SPECT. This finding, which had not previously been demonstrated to such a large degree, is evidence of the functional importance of these anomalies.
CONCLUSION
We demonstrated a highly sensitive and specific correlation between an anomalous course between the great vessels and a stress-induced myocardial perfusion defect. If further studies on a larger population indicate that perfusion scans show positive findings in all cases in which the coronary course is between the aorta and pulmonary artery, there will probably be no need to perform additional testing such as TEE. Moreover, as seen in this study, stress–rest SPECT will reliably select those patients with ACA who are subject to corrective surgery. At the moment, integrated use of TEE and exercise SPECT should be considered in risk stratification and choice of surgical approach for coronary anomalies.
Footnotes
Received Aug. 12, 2003; revision accepted Dec. 8, 2003.
For correspondence or reprints contact: Leonardo De Luca, MD, Divisione Ospedaliera di Cardiologia, Azienda Policlinico Hospital, Pizza G. Cesare, 11, 70100 Bari, Italy.
E-mail: leodeluca{at}virgilio.it





{kind=link}
{kind=link}