


Abstract
Estrogen receptor alpha (ERα) and progesterone receptor (PR) are important steroid hormone receptor biomarkers used to determine prognosis and to predict benefit from endocrine therapies for breast cancer patients. Receptor expression is routinely measured in biopsy specimens using immunohistochemistry, although such testing can be challenging, particularly in the setting of metastatic disease. ERα and PR can be quantitatively assayed noninvasively with PET. This approach provides the opportunity to assess receptor expression and function in real time, within the entire tumor, and across distant sites of metastatic disease. This article reviews the current evidence of ERα and PR PET imaging as predictive and early-response biomarkers for endocrine therapy.
More than 230,000 women in the United States are predicted to be diagnosed with breast cancer in 2015, making it the most common malignancy among women (1). Most of these patients will be diagnosed with curable breast cancer, although 5%–9% will have metastatic disease at presentation (1). When breast cancer has spread to distant organs, it is mainly incurable and the goal of therapy is palliative. Treatment of metastatic breast cancer is indefinite; therefore, therapies that maximize quality and quantity of life are preferred.
The systemic therapy decision for a specific patient is based on the estrogen receptor alpha (ERα), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) status of the patient’s breast cancer (2). At present, receptor testing from tissue obtained from a metastatic biopsy is the standard method of ascertaining the receptor status. If tissue from a metastatic site is not available, receptor status is inferred from the primary breast tumor. For those with tumors expressing ERα or PR (>75% of all breast cancers), endocrine therapy is the preferred treatment for the first several lines of therapy. However, only 50%–75% of patients with ERα-positive breast cancer will respond to first-line endocrine therapy, and the response rate decreases with additional lines of therapy, with only 25% responding beyond the first line (3).
A variety of challenges exist in determining the hormone receptor status of a metastatic tumor. First, the location of the metastatic disease may not be amenable to biopsy (e.g., brain or bone), and the treating clinician will be forced to assume that the receptor status in the metastatic disease is the same as in the primary breast tumor. However, this assumption is problematic because the receptor status can differ 25%–40% of the time between primary breast tumors and metastatic lesions (3–5). Second, even when a bone biopsy can be performed, issues with sample processing of bone (specifically decalcification) can generate false-negative ERα or PR results (6). With a false-negative result, the clinician could be led away from using less toxic endocrine therapy to treat the patient. Finally, there is the issue of both intratumor and intertumor heterogeneity (7). Tumor heterogeneity is of particular relevance, because patients generally have more than one site of metastatic disease. Furthermore, not all cancer cells in a tumor will be the same. A biopsy samples only a small portion of one lesion; it is not feasible to sample each individual metastatic lesion. Thus, practitioners must assume that the one biopsy represents all of the cancer. These issues underscore the need to develop standard methods of measuring tumor heterogeneity. One method under development that can better assess tumor heterogeneity is imaging using receptor-targeted radiopharmaceuticals.
Noninvasive imaging is a useful approach for visual assessment and quantitative measurement of steroid hormone receptors both in primary breast cancer and across metastatic sites of disease. The techniques used for steroid receptor imaging have focused predominately on 18F-based radiopharmaceuticals and PET alone or, more recently, in combination with CT (PET/CT) for improved anatomic colocalization. PET imaging has an advantage over other nuclear medicine techniques, such as planar imaging or SPECT, because of its excellent sensitivity to quantify radioligand binding down to picomolar concentrations (8).
Although steroid receptor PET imaging agents have not yet been approved by the U.S. Food and Drug Administration, several factors make them attractive candidates for successful translation, implementation, and acceptance into clinical use for breast cancer patients. Patient preparation for steroid receptor imaging is simpler than for conventional PET/CT imaging with 18F-FDG because fasting and measurement of blood glucose levels before scanning are not necessary. As with 18F-FDG PET/CT, patients are injected intravenously with the steroid receptor imaging agent and imaged approximately 1 h later using static emission data acquisition. The SUV of the steroid receptor imaging agent in a lesion of interest, calculated as radioactivity in the volume of interest (kBq/mL) divided by the injected dose per kilogram of body weight (MBq/kg), has been validated through correlation with in vitro receptor expression assays such as 3H-radioligand binding assays and immunohistochemistry (9–11). Although more sophisticated uptake measures using dynamic image acquisition and pharmacokinetic modeling have been reported, they have not been proven superior to simpler SUV measurements (10). Ease of patient preparation, image acquisition, and analysis are important factors to keep in mind when evaluating new molecular imaging agents for potential use in clinical practice.
ESTROGEN RECEPTOR IMAGING
16α-18F-fluoro-17β-estradiol (18F-FES) is the most studied radiopharmaceutical to quantify ERα and has been reported for nearly 1,000 patients participating in clinical trials as of 2013 (12). This radioligand was developed in the 1980s (13), with the first-in-human study published in 1988 by Mintun et al. (9). 18F-FES displays a favorable tissue biodistribution profile with comparable binding affinity to ERα, as does 17β-estradiol (14). 18F-FES uptake (as measured by SUV with imaging) strongly correlates with ERα expression—as measured by radioligand binding in fresh tissue and by immunohistochemistry in fixed tissue (9,10)—as shown in Figure 1. Sensitivity and specificity data of 18F-FES imaging for the detection of ERα-positive breast cancer are available in 4 published studies involving 114 patients (9,10,15,16). The overall sensitivity and specificity were 84% (95% confidence interval, 73%–91%) and 98% (95% confidence interval, 90%–100%), respectively (12). Thus, 18F-FES-PET is a good surrogate measurement of ERα expression.
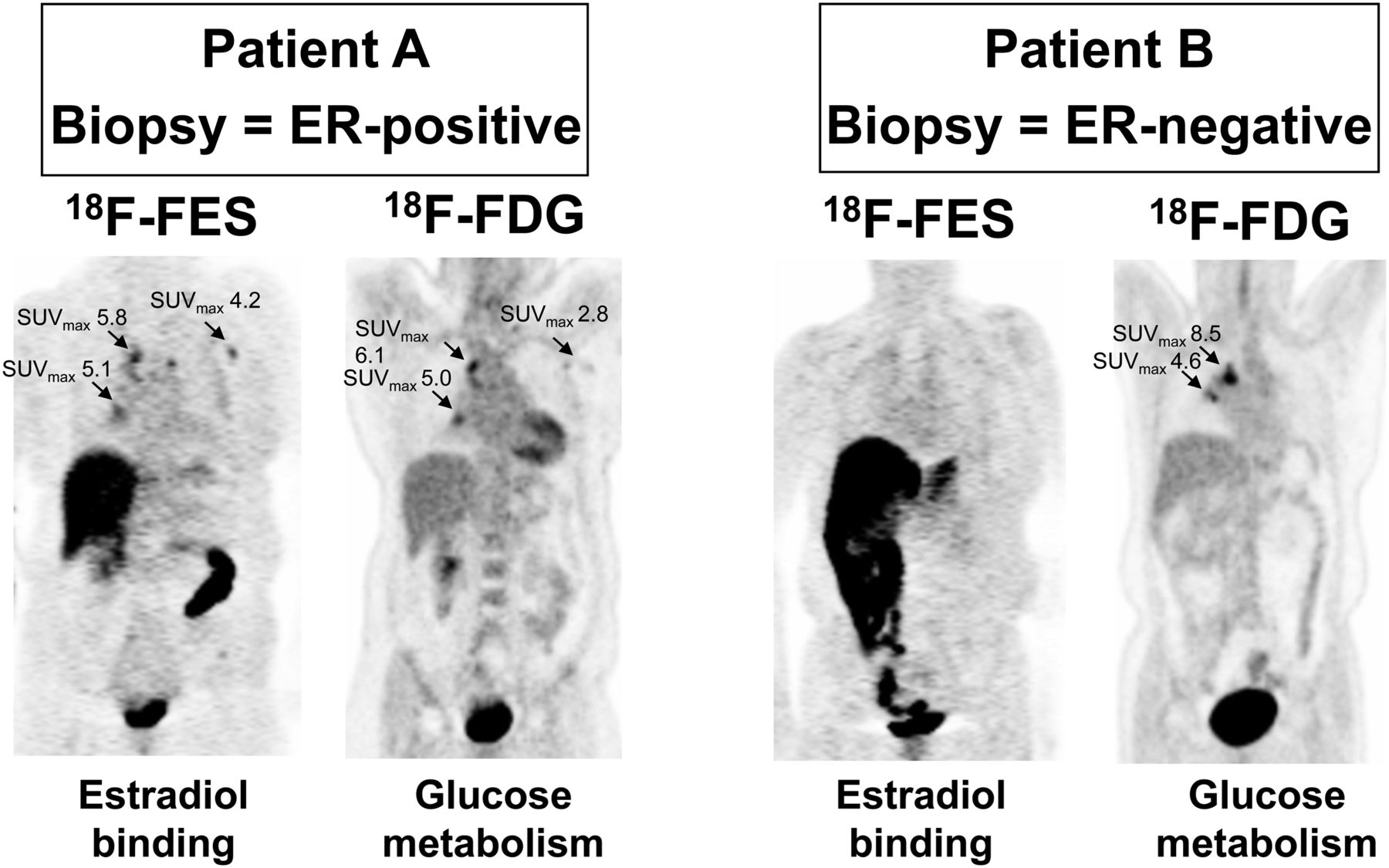
18F-FDG and 18F-FES PET coronal slices are shown for 2 patients in University of Washington 18F-FES trial (22). Both patients have mediastinal nodal metastases from ERα-positive breast cancer. Both had biopsy of metastatic site. ER uptake is shown by 18F-FES in patient A but not in patient B. Patient A has 18F-FES uptake at multiple sites; in fact, sites are more prominent on 18F-FES PET than on 18F-FDG PET and can be seen with well-differentiated breast cancer. Patient B has mediastinal disease clearly seen by 18F-FDG PET but not seen on 18F-FES PET. Biopsy showed ERα-negative breast cancer. 18F-FES values are 1.4 and 1.3. (Reprinted with permission of (22).)
The Cancer Imaging Program of the National Cancer Institute sponsors an investigational new drug exemption from the Food and Drug Administration (IND 79,005) for 18F-FES and freely provides reference materials to the research community to assist investigators with further 18F-FES clinical trials (17). They anticipate that data gained from wider use of 18F-FES may eventually support a Food and Drug Administration new drug application.
18F-FES as a Predictive Biomarker
The baseline value of the 18F-FES SUV has been studied as a predictive biomarker to endocrine therapy in several small studies in patients receiving various endocrine therapies for metastatic ERα-positive breast cancer. In all these studies, response was defined by standard clinical criteria based on symptoms and imaging. In early studies from Washington University, Dehdashti et al. (18) studied 11 patients with 18F-FES PET before initiation of tamoxifen therapy. Response was assessed by the treating clinician at 2-mo intervals. The baseline 18F-FES SUV was 2.2 or higher for responders and 1.7 or higher for nonresponders (18). Later, in studying 40 patients with advanced breast cancer before and after tamoxifen therapy, these investigators reported that responders had higher baseline tumor uptake of 18F-FES (SUV, 4.3 ± 6 2.4) than did nonresponders (SUV, 1.8 ± 6 1.3; P = 0.0007) (19). When the SUV cutoff of 2.0 was used, positive predictive value (PPV) was calculated to be 79% and negative predictive value (NPV) 88%, slightly better than in the previous study. Subsequently, the same investigators examined 51 patients receiving an aromatase inhibitor or fulvestrant (20). Baseline SUV of 18F-FES was again noted to be higher in responders (3.5 ± 2.5) than in nonresponders (2.1 ± 1.8). Logistic regression analysis demonstrated a 40% increase in the odds of response for every unit increase in baseline 18F-FES SUV. A prospectively defined cutoff SUV of 2 for 18F-FES was considered positive for ER expression, above which patients were more likely to respond to aromatase inhibitor or fulvestrant therapy. Based on the SUV cutoff of 2.0, PPV and NPV of 18F-FES PET were calculated to be 50% and 81%, respectively (20). Finally, baseline 18F-FES SUV and response at 6 mo were examined in a fourth study at the University of Washington, this one of 47 patients, many of whom had previously received tamoxifen therapy and were scheduled to begin a different salvage endocrine therapy (21). In receiver-operating-characteristic analysis, 18F-FES SUV greater than 1.5 was associated with response to therapy. None of the 15 patients with an SUV less than the threshold of 1.5 responded to hormonal therapy. On the other hand, 11 of 32 with an SUV greater than 1.5 (higher than the threshold) responded. This was statistically significant (P < 0.01). Of note, patients with HER2-positive disease who received trastuzumab were permitted in this study; however, none of these patients were classified as responders (21).
Van Kruchten et al. (12) combined the results of these 4 studies and determined that lack of response to endocrine therapy was predicted by an 18F-FES SUV of less than 1.5 in this heterogeneous group of patients. Using the 1.5 threshold, 96 of 114 patients would have been selected to receive endocrine therapy, and 62 of these would have had a clinical benefit (PPV, 65%). Alternatively, of the 42 patients with an 18F-FES SUV of less than 1.5, 37 derived no clinical benefit from endocrine therapy (NPV, 88%). Van Kruchten et al. also examined a cutoff of 2.0 and found that 31% of patients who responded to endocrine therapy would have been considered 18F-FES–negative using this cutoff and thus potentially would not have received the endocrine therapy to which they responded. Finally, a fifth study of 15 patients showed that 2 of 2 patients with low baseline 18F-FES uptake had progressive disease at 6 mo (22). These data would imply that a cutoff of 1.5 is most appropriate if using 18F-FES PET as a tool to predict response to endocrine therapy; the data further would suggest that patients with disease having 18F-FES SUVs less than 1.5 should potentially receive cytotoxic therapy rather than endocrine therapy. However, before 18F-FES is used in clinical practice, larger studies are needed to further refine and validate the threshold cutoff.
A potential advantage of 18F-FES imaging is visualization of multiple lesions and hence appreciation of the true heterogeneity of uptake across the entire burden of tumor (23). Although 18F-FES can be measured at multiple tumor sites, uptake in the liver is confounded by clearance of the tracer; therefore, 18F-FES cannot measure tumor uptake at this common site of breast cancer metastasis. Because the standard of care is one biopsy sample, little is known about the significance of heterogeneity in predicting response. Further studies are needed to understand the predictive value of knowledge of ER binding at multiple sites.
18F-FES to Monitor Efficacy of Receptor Blockade and Response to Antiestrogen Therapy
Serial imaging is a standard method of evaluating response to treatment, and 18F-FES PET has been evaluated in such a fashion in a few small trials. In the previously discussed trial of 40 patients receiving first-line tamoxifen for metastatic ERα-positive metastatic breast cancer, 18F-FES PET was obtained at baseline and 7–10 d after initiation of therapy. 18F-FES SUV in lesions of responders decreased at the second time point compared with baseline. The decrease in 18F-FES SUV after 7–10 d of tamoxifen was 54.8% ± 14.2% in responders and 19.4% ± 17.3% in nonresponders (P = 0.0003). The mean change in 18F-FES SUV was also higher among responders (−2.5 ± 1.8) than among nonresponders (−0.5 ± 0.6) (19). These results suggest that an early evaluation after introduction of tamoxifen can help determine who will respond by monitoring the efficacy of tamoxifen to block 18F-FES binding to ERα.
A similar approach has also been studied for determining the optimal dose of ERα antagonists needed for complete suppression of 18F-FES uptake in serial imaging. Linden et al. (24) reported a retrospective study of patients with metastatic breast cancer and a prior ERα-positive primary diagnosis undergoing 18F-FES PET/CT before and after the initiation of salvage endocrine therapy. Complete blockade of tumor 18F-FES uptake was observed for all patients treated with tamoxifen (5/5) but for only 36% (4/11) of patients treated with fulvestrant (24). Those authors concluded that the dosing of fulvestrant was insufficient for complete ERα inhibition, but they did not have data on subsequent patient clinical responses to correlate. A subsequent prospective study of 16 patients with ERα-positive metastatic breast cancer treated with the current standard dose of 500 mg of intramuscular fulvestrant was performed to measure ERα availability for 18F-FES binding before and during therapy (25). Residual 18F-FES uptake was observed in 38% (6/16) of patients treated with fulvestrant, which was associated with early clinical disease progression (25). Use of 18F-FES PET/CT for determining optimal ERα inhibition could also be applied to new drug development and evaluation, as reported in a recent scientific meeting abstract for an investigational oral selective estrogen-receptor degrader, ARN-810 (26).
Summary
Thus, through its investigation in clinical trials, 18F-FES appears to be a predictive biomarker for identifying patients with ERα-positive metastatic breast cancer who will respond to endocrine therapy, as well as a useful tool to assess the pharmacodynamics of endocrine therapy at early times. Larger studies are necessary to better determine and validate the 18F-FES SUV threshold above which clinicians can report response to therapy; these studies will also aid in better determining the sensitivity and specificity of baseline 18F-FES SUVs to predict response (27). Such a study is about to open through the Eastern Cooperative Oncology Group/American College of Radiology Imaging Network (ECOG/ACRIN) consortium (NCT02398773), which will enroll patients receiving first-line endocrine-based therapy for ERα-positive metastatic breast cancer.
PROGESTERONE RECEPTOR IMAGING
As with ERα, prognostic and predictive information can be gained from knowledge of PR status. Therefore, PR is routinely assayed along with ERα as part of the standard immunohistochemical analysis of newly diagnosed breast cancers and their recurrences (28). Because ERα and PR expression in breast cancer are strongly associated, ERα-negative, PR-positive tumors are uncommon and may be caused by a false-negative ERα immunohistochemical result (29). However, endocrine therapy remains an option for patients with ERα-negative, PR-positive breast cancers.
PR is a classic estrogen-regulated gene, the expression of which depends on a functional ERα-signaling pathway (30). Thus, PR is a pharmacodynamic or early-response biomarker: “a downstream biomarker that can be used as a surrogate measure of response to treatment-induced modulation of the upstream signaling components” (31). For example, an increase in PR protein as measured on repeat biopsy shortly after initiating tamoxifen that resulted from its partial agonist activity correlated with prolonged time to progression and improved survival (32). Supporting this notion is the observation that patients with metastatic ERα-positive, PR-positive breast cancer are the most likely to benefit from endocrine therapy (33).
The most promising PET agent for imaging PR is 21-18F-fluoro-16α,17α-[(R)-(1′-α-furylmethylidene)dioxy]-19-norpregn-4-ene-3,20-dione (18F-FFNP). This radioligand was developed in the 1990s and fulfills several important criteria for effective steroid receptor imaging (34,35). It has a high relative binding affinity to PR and a low nonspecific binding and thus a high binding selectivity index (34,35). Recently optimized and automated synthesis methods result in a final product with good yield (≤77%), high radiochemical purity, and high specific activity (48,100–314,500 MBq [1,300–8,500 mCi]/μmol) (36). Tissue biodistribution studies in estrogen-primed female rats demonstrated high PR-selective uptake in the uterus and ovaries (34). Importantly, 18F-FFNP exhibits minimal defluorination, evidenced by low bone uptake, and is less prone to metabolism by dehydrogenases, which was the major factor in the unsuccessful application of an earlier PR imaging agent, 21-18F-fluoro-16α-ethyl-19-norprogesterone (18F-FENP), in humans (37).
18F-FFNP to Monitor Response to Endocrine Therapy
The hypothesis that changes in PR as seen on imaging can be an early-response biomarker of treatment-induced changes in an upstream ER-signaling pathway has been tested in preclinical breast cancer models (38,39). These studies show that an early decrease in tumoral 18F-FFNP uptake predicts responsiveness to fulvestrant and estrogen-deprivation therapy. Decreases in 18F-FFNP uptake occurred before changes in tumor growth. Furthermore, monitoring ERα function through imaging PR with longitudinal 18F-FFNP PET was more predictive of response to estrogen-deprivation therapy than was 18F-FES PET or 18F-FDG PET (39). These preclinical data provide the proof of principle to support further translational studies in breast cancer patients.
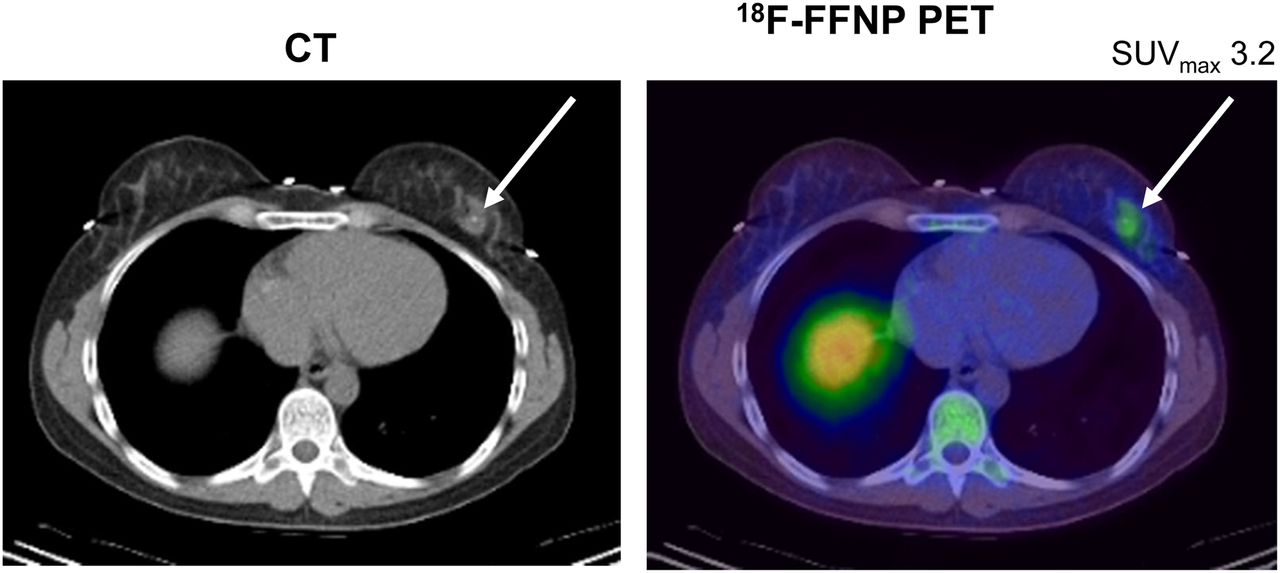
The first-in-human study of 18F-FFNP was published in 2012 and provided safety and dosimetry data on 20 women with breast cancer (Fig. 2) (11). No adverse or pharmacologic effects of the injected mass dose (1.34 ± 1.24 μg) were observed. The whole-body effective dose for 18F-FFNP was 0.020 mSv/MBq, which is similar to that for 18F-FES (0.022 mSv/MBq) and 18F-FDG (0.024 mSv/Bq) (11,40,41). As with 18F-FES, 18F-FFNP is eliminated by hepatobiliary clearance. Thus, evaluation of 18F-FFNP uptake in liver lesions is a potential limitation.

Representative transverse CT (left) and fused 18F-FFNP PET/CT (right) images in patient with PR-positive breast cancer demonstrate focally increased uptake in known cancer in left breast (arrows).
In addition to investigating safety and dosimetry, correlation of 18F-FFNP uptake with in vitro PR measurement via immunohistochemistry was performed by Dehdashti et al. (11). In their patient population with 16 PR-positive and 6 PR-negative primary breast cancers, tumor–to–normal breast tissue uptake ratios of 18F-FFNP were greater in PR-positive cancers (2.6 ± 0.9) than in PR-negative cancers (1.5 ± 0.3; P = 0.001) (11). Dynamic imaging demonstrated rapid 18F-FFNP uptake within the PR-positive tumor and showed no significant washout over the 60-min imaging interval (11). Thus, 18F-FFNP PET can be safely used in patients to assess the PR status of breast cancer.
Investigations into the usefulness of 18F-FFNP PET as an early-response biomarker for endocrine therapy are in progress. The clinical trial NCT02455453 aims to measure 18F-FFNP uptake before and after administration of estradiol for 1 d (estradiol challenge) for postmenopausal patients with ERα-positive breast cancer to determine whether the change in 18F-FFNP uptake is predictive of response to endocrine therapy. Furthermore, preclinical studies have demonstrated that 18F-FFNP uptake of hormone-sensitive mouse mammary tumors increases in response to estradiol treatment (38).
Summary
Clinical studies of PR PET imaging significantly lag behind those of ERα, and considerable work is still required before 18F-FFNP is ready for translation into clinical practice. Larger-scale investigations are needed into the sensitivity and specificity of 18F-FFNP PET for the detection of PR, and its usefulness as an early-response biomarker for endocrine therapy; these studies should then undergo subsequent validation through multiinstitutional studies. Comparison might also be considered of the performance of 18F-FFNP with 18F-radiolabeled and 11C-radiolabeled Tanaproget (ApexBio), a nonsteroidal progestin analog with in vitro and preclinical data demonstrating a high binding affinity for PR and less cross-reactivity with glucocorticoid and androgen receptors (42–44).
FUTURE DIRECTIONS
Combined ERα and PR Imaging
Information gained from imaging with both 18F-FES and 18F-FFNP could result in the highest predictive power for response to endocrine therapy. A baseline 18F-FES PET examination would determine whether the therapeutic target (ERα) is present in some, most, or all of a patient’s metastatic lesions, thus providing important information about tumor heterogeneity. The strength of ERα imaging with 18F-FES is its high NPV (88%); that is, if the 18F-FES SUV is less than 1.5, patients are very unlikely to have a clinical benefit from endocrine therapy (12). However, the PPV of 18F-FES PET is only 65% (12). Thus, the presence of ERα capable of binding to 18F-FES does not guarantee its function. Baseline and short-follow-up 18F-FFNP PET imaging after endocrine therapy initiation or estradiol challenge may be helpful as a probe of PR expression to confirm a functional ERα-driven pathway. However, a drawback of using 18F radioligands for this approach is the inability to image using more than one radiopharmaceutical at a time, thus requiring repeated longitudinal PET/CT studies, which raises potential concerns regarding radiation exposure. Fortuitously, simultaneous PET/MRI scanners have recently been developed for clinical use that can reduce radiation exposure by eliminating the CT component of the examination and thus be a more suitable modality for serial imaging to assess therapy response.
Steroid Receptor Imaging in the Era of Personalized Cancer Medicine
Evidence is increasing of the complementary role of targeted therapy of growth factor activation and cell-cycle control pathways with endocrine therapy for patients with recurrent or metastatic breast cancer. Indications for this approach have been recently incorporated into clinical practice guidelines (2,45). These treatments include everolimus, an inhibitor of the phosphatidylinositol 3-kinase/mammalian target of rapamycin (PI3K/mTOR) pathway, in combination with exemestane, a steroidal aromatase enzyme inactivator; and palbociclib, a cyclin-dependent kinase 4/6 inhibitor, in combination with fulvestrant or letrozole, a nonsteroidal aromatase inhibitor. The ability of steroid receptor imaging to predict response to these types of combined endocrine and molecular pathway–targeted therapies will need to be investigated.
In this emerging era of precision medicine and big data, we will also need to consider how information gained from molecular imaging is best integrated with “-omics”-level tissue data. For breast cancer, these assays include measuring the overall gene expression pattern for molecular subtyping (46); measuring a subset of 21 genes to quantify the likelihood of distant recurrence in tamoxifen-treated patients with axillary lymph node–negative, ERα-positive primary breast cancer (47); and whole-genome sequencing of metastatic tumor samples to identify gene mutations that respond to medications (48). An approach that incorporates molecular imaging with genomics tissue data may improve the overall clinical usefulness of the individual tests. A multidisciplinary approach, such as a molecular genomics and imaging tumor board, would be the ideal setting for guiding clinical decision making, particularly for patients with progressive metastatic breast cancer.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication September 9, 2015.
- Accepted for publication November 2, 2015.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Biodistribution of 18F-FES in Patients with Metastatic ER+ Breast Cancer Undergoing Treatment with Rintodestrant (G1T48), a Novel Selective ER Degrader
- Building the Bridge: Molecular Imaging Biomarkers for 21st Century Cancer Therapies
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy
- Harnessing Preclinical Molecular Imaging to Inform Advances in Personalized Cancer Medicine
- Introduction and Overview