


Abstract
Previous studies have suggested that early changes in blood flow (BF) in response to neoadjuvant chemotherapy and evaluated with 15O-water are a surrogate biomarker of outcome in women with breast cancer. This study investigates, in the triple-negative breast cancer subtype, the prognostic relevance of tumor BF changes (ΔBF) in response to chemotherapy, assessed using a short dynamic 18F-FDG PET acquisition. Methods: Forty-six consecutive women with triple-negative breast cancer and an indication for neoadjuvant chemotherapy were prospectively included. Women benefited from a baseline 18F-FDG PET examination with a 2-min chest-centered dynamic acquisition, started at the time of 18F-FDG injection. Breast tumor perfusion was calculated from this short dynamic image using a first-pass model. This dynamic PET acquisition was repeated after the first cycle of chemotherapy to measure early ΔBF. Delayed static PET acquisitions were also performed (90 min after 18F-FDG injection) to measure changes in tumor glucose metabolism (ΔSUVmax). The association between tumor BF, clinicopathologic characteristics, and patients’ overall survival (OS) was evaluated. Results: Median baseline tumor BF was 21 mL/min/100 g (range, 6–46 mL/min/100 g) and did not significantly differ according to tumor size, Scarf–Bloom–Richardson grade, or Ki-67 expression. Median tumor ∆BF was −30%, with highly scattered values (range, −93% to +118%). A weak correlation was observed between ΔBF and ∆SUVmax (r = +0.40, P = 0.01). The median follow-up was 30 mo (range, 6–73 mo). Eight women developed recurrent disease, 7 of whom died. Low OS was associated with menopausal history (P = 0.03), persistent or increased tumor vascularization on the interim PET (ΔBF cutoff = −30%; P = 0.03), non–breast-conserving surgery (P = 0.04), and the absence of a pathologic complete response (pCR) (P = 0.01). ΔBF and pCR provided incremental prognostic stratification: 3-y OS was 100% in pCR women, 87% in no-pCR women but achieving an early tumor BF response, and only 48% in no-pCR/no-BF–response women (ΔBF cutoff = −30%, P < 0.001). Conclusion: This study suggests the clinical usefulness of an early user- and patient-friendly 2-min dynamic acquisition to monitor breast tumor ΔBF to neoadjuvant chemotherapy using 18F-FDG PET/CT. Monitoring tumor perfusion and angiogenesis response to treatment seems to be a promising target for PET tracers.
Breast cancer includes different molecular entities (1). Triple-negative breast cancers (TNBCs) are defined by the lack of hormone receptor expression and no overexpression of human epidermal growth factor receptor 2 (2,3). This subtype is characterized by an aggressive clinical course marked by high rates of metastases and poor outcome (2). Neoadjuvant chemotherapy aims to improve rates of breast conservation (4) but also offers an opportunity to evaluate early biomarkers of tumor response. The identification of biomarkers, either molecular or otherwise, that could distinguish between highly responsive and nonresponsive tumors early is of critical importance to tailor treatments to tumor response in individual patients.
Previous studies found that early changes in tumor glucose metabolism, assessed with 18F-FDG PET/CT after the first or second course of neoadjuvant chemotherapy, can indicate breast cancer response early (5,6), especially in the aggressive TNBC subtype (7,8).
Beyond tumor glucose metabolism, the ability to induce angiogenesis is another hallmark of cancer cells: the presence of functional vasculature is essential for the growth of solid tumors. In addition to their cytotoxic action, conventional chemotherapeutic agents exert effects on tumor vasculature, indirectly by interrupting proangiogenic support secondary to tumor cell kill and directly by affecting endothelial cell function (9). In the era of precision medicine, one of the challenges facing the field of tumor response monitoring is to find predictive biomarkers to identify tumors with angiogenic resistance. In such tumors, standard treatments may require the adjunction of a pure angiogenic inhibitor (10).
Previous studies have demonstrated that early changes in tumor blood flow (BF) measured by 15O-water PET or in the flow component extracted from 1-h dynamic 18F-FDG PET scans (K1) were associated with pathologic tumor response and outcomes among women with locally advanced breast cancer (11–13). Patients with persistent or incremental increases in 18F-FDG K1 were more likely to relapse or die. Kinetic 18F-FDG measurements were found more useful than static SUV measurements (14).
Because of the short half-life of 15O-water, an on-site cyclotron is required and very few nuclear medicine centers have one. Moreover, 18F-FDG PET kinetic analysis requires an acquisition of 1 h. There is, thus, an impetus for clinically practical methods capable of estimating kinetic parameters from PET studies. Mullani et al. developed a first-pass model for the in vivo calculation of BF with PET. This model was applied to the evaluation of tumor BF using 18F-FDG and demonstrated good correlations with BF measured with 15O-water (15).
The present study investigated the clinical and prognostic relevance of early changes in tumor perfusion in response to neoadjuvant treatment, using baseline and interim short dynamic 18F-FDG PET/CT acquisitions. We focused on women with TNBC, which is a challenging tumor subtype because of its high clinical aggressiveness.
MATERIALS AND METHODS
Patients and Study Design
From February 2009 to October 2014, 260 women referred to our institution for clinical stage II or III invasive breast cancer with an indication for neoadjuvant chemotherapy were consecutively and prospectively evaluated. Only women with TNBC were included. This population overlaps those of previous articles published by our team (7,16). Patients with high glycemia (>9 mmol/L), unwilling to undergo the complete PET examinations or with suspected metastasis on baseline 18F-FDG PET, were excluded. The institutional review board approved this prospective study as a current care study. The medical team documented the nonopposition of the patient in source documents and in the information note provided to the patient (the requirement to obtain signed consent was waived).
Most women underwent sequential chemotherapy with anthracyclines (FEC100, 3 courses every 3 wk) followed by taxanes (3 courses every 3 wk). This systematic switch was done in conformance with institutional guidelines and not based on PET response monitoring. Few of the women, included at the beginning of the study, underwent 6 cycles of FEC100. One month after the last course of chemotherapy, the tumors were surgically removed and examined by a pathologist. Radiotherapy was performed according to standard recommendations. Patients were followed up every 3 mo during the first 2 y, every 6 mo for the following 3 y, and then once per year.
Pathologic Analysis
Pretreatment core biopsies from the primary tumor were used to determine the histologic type and the tumor Scarf–Bloom–Richardson grade (17). The following immunohistochemical markers were examined: estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 expression. All immunostaining was performed on an automated immunostainer (Ventana XT). Estrogen receptor and progesterone receptor status were considered negative if the tumor showed less than 10% of positive cells. Human epidermal growth factor receptor 2 status was graded according to the HercepTest scoring system (18). In cases of 2+ scores, fluorescent in situ hybridization was used according to criteria of the American Society of Clinical Oncology/College of American Pathologists (18).
Pathologic complete response (pCR) was defined as no residual invasive cancer in the breast and nodes, though in situ breast residuals were allowed (ypT0/is ypN0) (19).
18F-FDG PET/CT Procedures
A first 18F-FDG PET scan was done at baseline. Two different PET/CT imaging systems were used: a Gemini GXL PET/CT scanner from February 2009 to December 2010 and a Gemini TF PET/CT scanner from December 2010 to October 2014 (Philips). Patients were instructed to fast for at least 6 h before the intravenous injection of 5 MBq/kg of 18F-FDG for Gemini GXL studies and 3 MBq/kg for Gemini TF studies.
18F-FDG was injected using an automatic PET infusion system (Intego; Medrad) at a rate of 1 mL/s. Simultaneously with the injection, the first chest-centered emission acquisition with the patient in the prone position, using a breast imaging coil, was run in the list-mode for 2 min, followed by a low-dose CT scan. Reconstructions of 5- and 10-s frames were extracted from this dynamic first-pass acquisition. Sixty minutes after the 18F-FDG injection, a whole-body PET scan was obtained. Finally, 90 min after the injection, a PET scan restricted to the chest (2 bed positions) with patients in the prone position was obtained. Emission data were corrected for dead time, random, and scatter coincidences and attenuation before reconstruction with the row action maximum-likelihood algorithm.
A few days before the second course of chemotherapy, a second 18F-FDG PET scan was acquired with the same early dynamic first-pass acquisition and late chest-restricted PET static acquisition.
First-Pass Model for Measurement of Tumor BF (Supplemental Fig. 1).
The concept and method for measuring tumor BF from the first pass of 18F-FDG has been explained in a previous paper from our institution (20). Briefly, it is based on the first-pass model of Mullani et al. (15,21) hypothesizing that during the early period of the first transit of a highly extracted tracer through the tumor, the venous concentration of the tracer can be considered zero; the first-pass extraction fraction of 18F-FDG in tumor tissue is high, close to those of 15O-water (15); and so as to minimize the error in flow measurement due to the statistical quality of the data, the numerator and the denominator are determined at their maximum values—this peak count time (Tm) was defined on the arterial time–activity curve as the end of the first pass of the tracer in the volume of interest drawn inside the ascending aorta (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). A volume of interest encompassing the primary tumor was also manually drawn. Mixed functional and anatomic contouring was used to delineate the breast tumor. Tumor BF at baseline (BF1) and after the first cycle of chemotherapy (BF2) were then calculated in mL/min/100 g of tumor, using the following equation:
Q(Tm) is the amount of the tracer in tumor tissue at time Tm; E is the tumor first-pass extraction fraction of 18F-FDG, which is assumed to be equal to 1 (15); and Ca(t) is the arterial concentration of the tracer at time t.
The tumor BF response to chemotherapy was calculated:
Tumor Glucose Metabolism Measurements
A spheroidal volume of interest encompassing the primary tumor was manually drawn on the chest-restricted acquisitions obtained at 90 min after tracer injection to measure the SUV maximal index at baseline (SUV1max) and after the first course of chemotherapy (SUV2max). Measured SUVmax was corrected for body surface area and glycaemia, as detailed in our previous studies (22,23). The metabolic response to treatment was calculated as follows:
The ratio between baseline tumor glucose metabolism and perfusion (SUV1max/BF1) was calculated.
Statistical Analysis
Continuous variables are expressed as medians and ranges or means and SD. The study endpoints were the oncologic outcomes of relapse-free survival and overall survival (OS). Relapse-free survival was defined as the time from date of breast cancer diagnosis (biopsy) until the first evidence of disease recurrence (local, regional, or distant). Alive patients without progression were censored at the last follow-up. OS was defined as the time from diagnosis until the date of death or, if alive, the date of the last clinical follow-up.
The Pearson correlation coefficient (r) between ∆SUVmax and ΔBF was calculated. Receiver-operating characteristic curves were used to compare the predictive values for pCR.
Univariate Cox proportional hazards models were calculated to compute the hazard ratios with their 95% confidence intervals (CIs). All P values were 2-sided and considered significant when no greater than 0.05.
Median follow-up with its 95% CI and survival curves were calculated using the Kaplan–Meier method. Survival outcomes were compared using log-rank tests.
WinSTAT software (Microsoft) and Systat software (Systat Inc.) were used.
RESULTS
Patients’ Characteristics (Supplemental Table 1)
Among the 260 women evaluated, 57 (22%) had TNBC. Eleven women were then excluded: 1 of them because of uncontrolled glycaemia, 5 because of unexpected stage IV upstaging, and 5 because the first-pass dynamic acquisitions was not performed for different reasons (e.g., technical problems, refusal). In the remaining 46 patients finally included in the study, 6 missed the second PET scan.
Patients’ characteristics are detailed in Supplemental Table 1. Briefly, the median age was 46 y (age range, 26–85 y). The median primary tumor size, assessed with breast ultrasound or mammogram, was 3.6 cm (range, 1.5–6.7 cm). On ultrasound scanning, 32 of 46 women had lymph node involvement (based on sonographic features of the lymph nodes). Almost all the tumors were invasive ductal carcinoma (45/46), and one was an invasive lobular carcinoma.
The median value of tumor BF1 was 21 mL/min/100 g (range, 6–46 mL/min/100 g). Tumor size, Scarf–Bloom–Richardson grade, mitotic count, and Ki-67 tumor expression were not associated with BF1 values and the SUV1max/BF1 ratio.
Median tumor ∆BF was −30% (range, −93% to +118%). Thirty percent of the women (12/40) experienced increased tumor BF after the first cycle of treatment.
Compared with ∆BF, median tumor ∆SUVmax showed less scattered values (median ∆SUVmax = −50.0% [range, −87 to +15%]). A weak correlation was observed between ∆SUVmax and ΔBF (r = +0.40; P = 0.01) (Fig. 1).
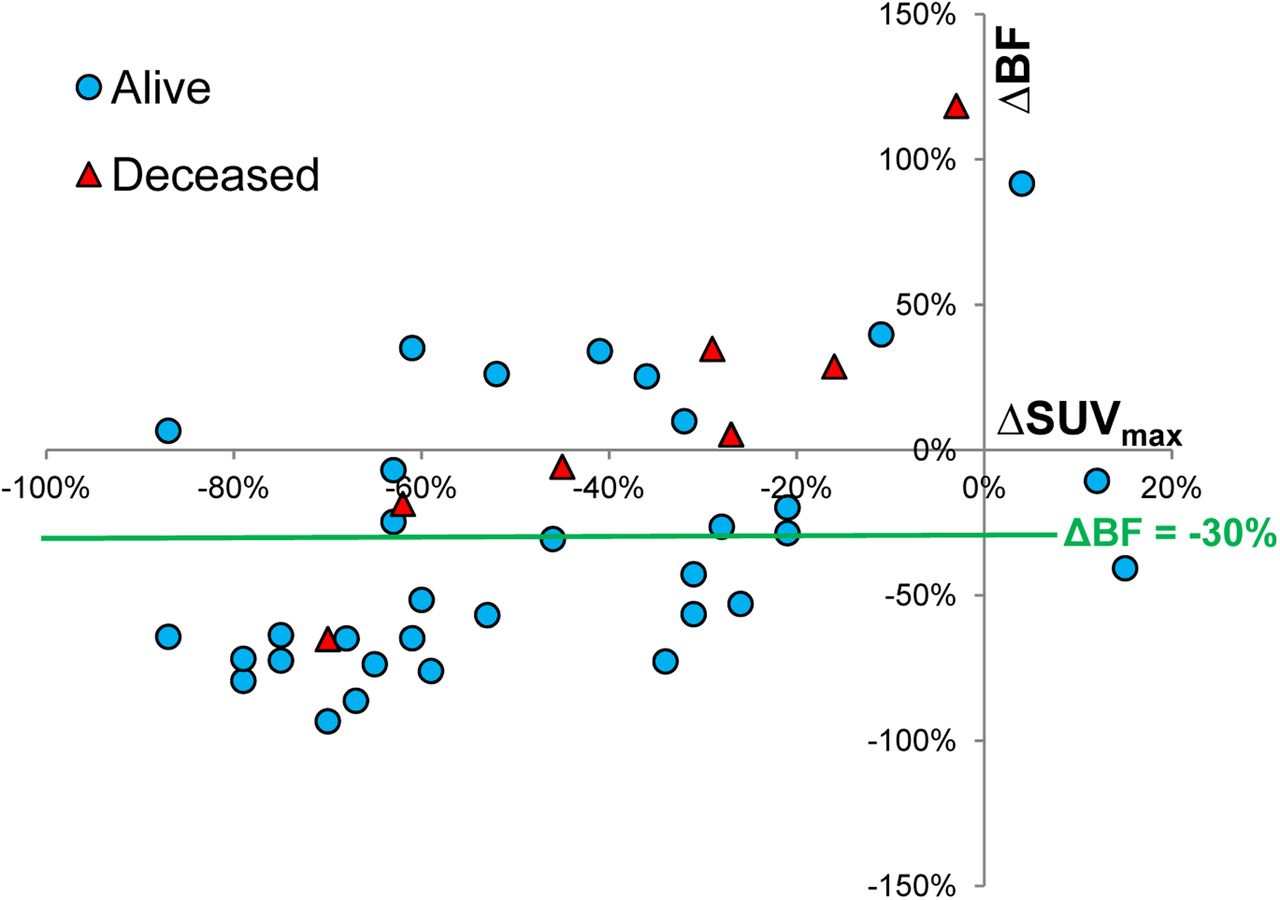
Bivariate scatterplots of tumor BF response (ΔBF) and tumor metabolism response (ΔSUVmax).
The mean (±SD) timeframe between interim PET and surgery was 19 ± 2 wk. Conservative surgery was performed in 65% (30/46) of the women. The pCR rate was 43% (20/46). When receiver-operating-characteristic curve analyses were used, ΔSUVmax predicted pCR with an area under the curve of 0.82 ± 0.07 (P = 0.0007), whereas ΔBF did not reach significance (area under the curve = 0.66 ± 0.09; P = 0.09).
Survival Analysis (Fig. 2; Table 1)
The median follow-up period was 30 mo (range, 6–73 mo). Eight of the 46 women included developed recurrent disease, 7 of whom died. The 3-y relapse-free survival rate was 77.3% (95% CI = 62.9%–91.7%) and the 3-y OS rate was 82.2% (95% CI = 69.0%–95.4%).
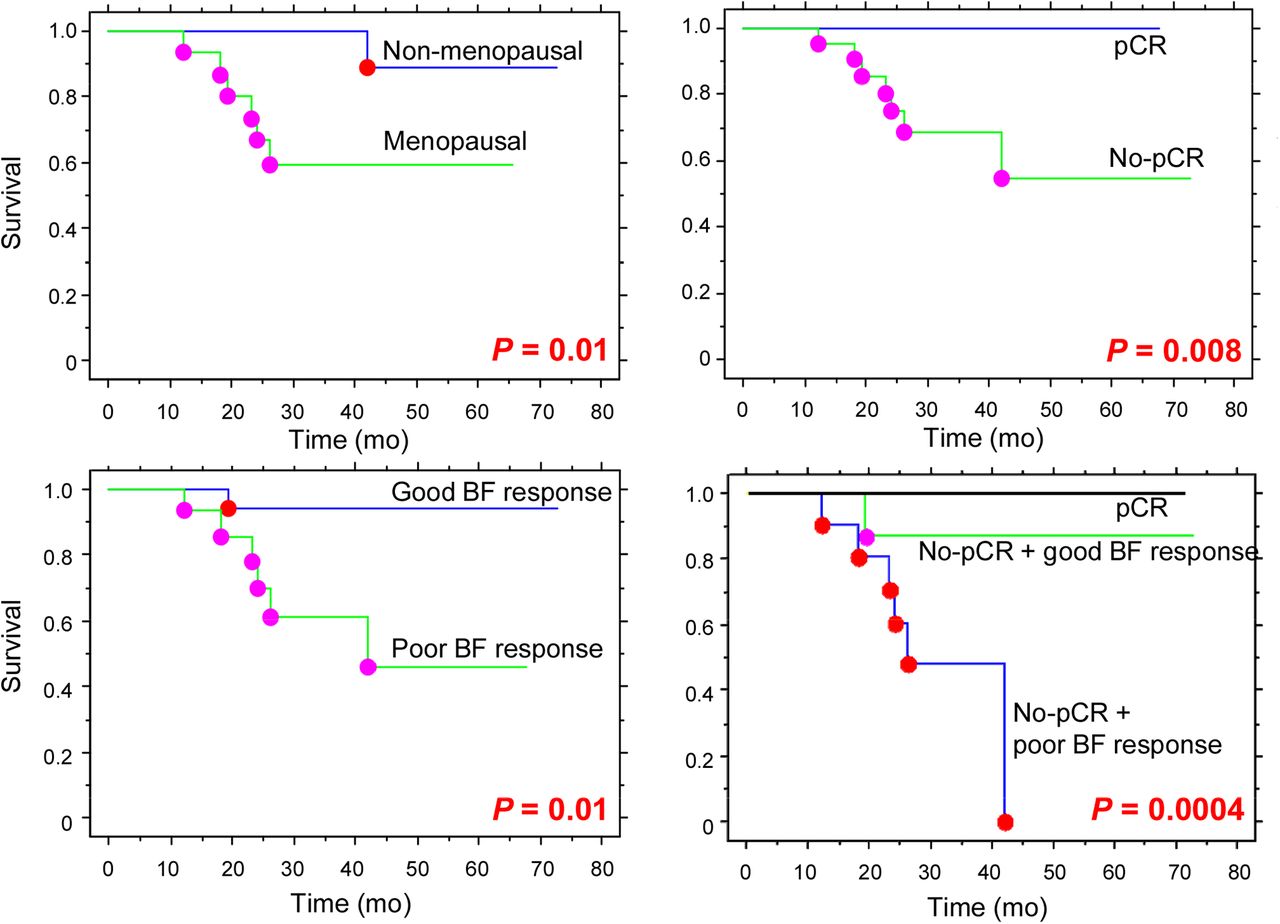
Kaplan–Meier curves showing OS according to menopausal status, histologic response, tumor BF response (ΔBF cutoff = −30%), and association of pathologic response and ΔBF. P values were determined with log-rank test.
Factors Affecting Survival
Continuous variables were dichotomized according to their median value. Univariate Cox analysis for OS demonstrated that menopausal history, no significant decrease in tumor BF after the first cycle of chemotherapy (ΔBF cutoff = −30%), and non–breast-conserving surgery were associated with worst OS (P = 0.035, 0.037, and 0.046, respectively) (Table 1). Women who died had an average increase in tumor ΔBF (+11.6% ± 56%), whereas those who survived had an average decrease (−30.4% ± 45%). Given the small number of events, the multivariate analysis was not performed.
The Kaplan–Meier curves for OS with dichotomized values of ΔBF, type of surgery after neoadjuvant chemotherapy, and histologic tumor response are shown in Figure 2. Women achieving a pCR had excellent outcome (3-y OS = 100%). In women who did not achieve a pCR, tumor ΔBF could further stratify between women with good or poor outcome: 3-y OS was 87.5% in no-pCR women but who did experience an early tumor ΔBF decrease, whereas OS was only 48.5% in women who achieved neither a pCR nor a ΔBF response (ΔBF cutoff = −30%; P < 0.001).
DISCUSSION
Angiogenesis plays an important role in both growth and metastasis of many cancers and is thus recognized as one of the main hallmarks of oncogenesis (24). In TNBC, the association of an antiangiogenic agent (bevacizumab) with conventional neoadjuvant chemotherapy increases the pCR rate (25) but without any survival benefit demonstrated (26), emphasizing the need for biomarkers of the angiogenic cascade, to better select women who may benefit from antiangiogenic drugs.
Several imaging modalities, which yield different imaging-derived hemodynamic parameters, have been proposed for the noninvasive assessment of tumor vascularity and the response to treatment (27). In the neoadjuvant setting of breast cancer, these modalities demonstrated that maintained tumor BF at therapy midpoint was associated with poorer survival (12,13). Dynamic contrast-enhanced MRI is widely available and frequently used in studies evaluating tumor BF response to treatment (28,29). Dynamic contrast-enhanced–MRI derived biomarkers, particularly those involving tumor kinetic textures, are able to predict tumor histologic response early (28,29). The clinical value of monitoring tumor BF using 15O-water PET has also been evaluated: BF in breast cancer is highly variable and women with persistent or elevated tumor BF on interim PET experienced poorer tumor response and outcomes (11–13), thus paralleling our results in the specific TNBC population. When pharmacokinetic modeling was used, the flow component extracted from 1-h dynamic 18F-FDG PET imaging (K1) yielded a good correlation to 15O-water PET and dynamic contrast-enhanced MRI–measured BFs of breast cancer (30,31). In the neoadjuvant setting, 18F-FDG K1 changes over the first course of treatment provide the same prognostic information as BF changes assessed with 15O-water PET (13).
One main limitation of all these previous studies was that they evaluated tumor BF in all breast cancer subtypes pooled together. Today, this is less relevant than a per-subtype analysis because of the well-known molecular heterogeneity of breast cancer entities (1,32). Other limitations are that 15O-water PET requires an on-site cyclotron and that 18F-FDG PET kinetic complete analysis requires a long and uncomfortable acquisition procedure for the patient (1 h). Further optimization of 18F-FDG kinetic analysis measurements is needed to yield insights into practical alternatives that overcome the limitations of purely static measurements.
To assess tumor BF, we applied a dynamic first-pass model developed by Mullani et al., based on a simple 1-compartment flow model. This model estimates BF using only the first 2 min of data after injection. This short dynamic acquisition is suitable for routine practice (15,21). Tumor BF assessed with this model is linearly correlated with 15O-water–measured BF (r = 0.86) (15) and with breast tumor angiogenesis as measured by immunohistochemistry markers (20).
Using this first-pass model, we evaluated early tumor BF changes in response to chemotherapy in the challenging and aggressive TNBC subtype. Our estimated TNBC BF at baseline averaged 21 mL/min/100 g, which agrees with previous reports using 15O-water PET (11,30,31). The tumor BF response (ΔBF) showed highly scattered values, ranging from −93% to +118%, which weakly correlated with tumor metabolic changes (r = 0.4). Patients whose tumors failed to show a significant decrease in tumor BF after the first cycle of treatment (ΔBF cutoff = −30%) had a higher risk of recurrence and death. These results are consistent with those of Dunnwald et al., obtained in all tumor subtypes pooled together and using 15O-water PET and dynamic 18F-FDG PET (13,14).
In TNBC, pCR at the end of neoadjuvant chemotherapy has demonstrated a crucial endpoint: women who do not achieve pCR at the end of neoadjuvant chemotherapy have a higher risk of relapse and reduced OS (19). We found a 100% 3-y OS in women reaching a pCR. The more accurate exclusion of oligometastatic women by the baseline 18F-FDG PET examination, compared with previous studies using conventional imaging, may explain the excellent prognostic stratification of the pCR as already shown by Groheux et al. (33).
Contrary to ΔSUVmax, ΔBF was not a good predictor of pCR. But interestingly, ΔBF and pCR seemed to provide incremental prognostic stratification in the TNBC subtype: 3-y OS was 100% in pCR women, 87% in no-pCR women but achieving an early tumor BF response, and only 48% in no-pCR/no-BF–response women. We could thus identify a high-risk subgroup of women who experienced neither an early tumor BF decrease after the introduction of chemotherapy nor a pCR at the end of treatment. This study may thus be an important step toward the use of 18F-FDG PET to quantify different aspects of tumor biology and their changes in response to therapy, using a single 18F-FDG injection and 2 short PET acquisitions (early dynamic for tumor BF and late static for tumor glucose metabolism).
Our study has some limitations. First, TNBC is a rare subtype, which explains the small cohort of women: the results are preliminary. Second, the simple 1-compartment flow model used in this study has some intrinsic limitations, already described (15). Briefly, the first pass of 18F-FDG imaging may contain a few trapped components of 18F-FDG that can lead to an overestimation of BF. On the other hand, the first-pass extraction of 18F-FDG, relative to the 15O-water, averaged 0.86, thus suggesting a small underestimation of BF (15). Furthermore, the limited count statistic arising from a short static acquisition has statistical fluctuation that may affect the results.
Persistent cancer cell–derived cytokines may explain the persistent or increased tumor BF in resistant tumors after initiating neoadjuvant chemotherapy (34). But our results leave questions unanswered about the relationship between preserved tumor BF during treatment and the higher likelihood of metastatic failure. The elevated level of tumor BF after initiating treatment may directly facilitate the spread of tumor metastatic cells via the circulation (35) or may be a consequence of a more invasive TNBC phenotype, which could withstand cancer treatment and metastasize. The use of functional imaging modalities in combination with tissue-based genomic profiling will offer a unique opportunity to elucidate the critical biologic pathways that underlie our results. Molecular imaging also holds promises for in vivo imaging of tumor angiogenesis with the development of new specific probes, for example, against integrin (36).
CONCLUSION
This study showed that patients with breast carcinoma exhibiting persistent or even increased tumor vascularization after the first cycle of neoadjuvant chemotherapy experienced worse outcomes. Its great interest lies in the fact that it focused on the particularly aggressive TNBC subtype and demonstrated the prognostic usefulness of an early user- and patient-friendly 2-min dynamic 18F-FDG PET acquisition to monitor tumor BF changes. Imaging biomarkers of breast tumor perfusion may help the physician to better select women with TNBC who may benefit from the adjunction of angiogenic inhibitor drugs.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
This study is part of the PharmImage® project. We thank Mr. Philip Bastable for proofreading the text.
Footnotes
Published online Apr. 21, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 21, 2016.
- Accepted for publication March 14, 2016.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Principles of Tracer Kinetic Analysis in Oncology, Part II: Examples and Future Directions
- Breast Cancer Blood Flow and Metabolism on Dual-Acquisition 18F-FDG PET: Correlation with Tumor Phenotype and Neoadjuvant Chemotherapy Response
- 2-18F-Fluoroethanol Is a PET Reporter of Solid Tumor Perfusion
- Getting the Most out of 18F-FDG PET Scans: The Predictive Value of 18F-FDG PET-Derived Blood Flow Estimates for Breast Cancer