


Abstract
We evaluated the potential of 18F-fluoromethyldimethyl-2-hydroxyethyl-ammonium (FCH) PET/CT in the detection of recurrent disease or distant metastases and correlated its diagnostic accuracy with prostate-specific antigen (PSA) levels in prostate cancer patients with biochemical evidence of recurrence. Furthermore, the influences of androgen deprivation therapy (ADT) and its duration on 18F-FCH PET were assessed in this study. Methods: This prospective study included 250 prostate cancer patients with PSA relapse who underwent 18F-FCH PET/CT. At the time of 18F-FCH PET/CT imaging, the mean PSA level was 46.9 ± 314.7 ng/mL and 55.2% (138/250) of patients were receiving ADT. Overall, ADT was performed on 67.2% (168/250) of patients after initial treatment. Imaging was performed on an integrated PET/CT system. Acquisition started 1 min after intravenous injection of 18F-FCH (4.07 MBq/kg of body weight) with dynamic PET images in the pelvic region during 8 min (1 min/frame) followed by a static semi–whole-body acquisition. The final diagnosis of positive PET lesions was based on histopathology or a consensus of clinical findings, additional imaging, or follow-up imaging modalities. Results: 18F-FCH PET/CT was able to correctly detect malignant lesions in 74% (185/250) of patients but was negative in 26% (65/250). In 28% of patients, only 1 lesion was detected (69/250); from these, 65.2% (45 patients) had a local recurrence, 18.8% (13 patients) a single lymph node, and 15.9% (11 patients) a solitary bone metastasis. The sensitivity of the 18F-FCH PET was significantly higher (P = 0.001) in patients with ongoing ADT (85%; confidence interval, 80%–91%) than in patients without ADT (59.5%; confidence interval, 50%–69%). 18F-FCH PET sensitivity was 77.5%, 80.7%, 85.2%, and 92.8% for the trigger PSA levels of more than 0.5, 1.0, 2.0, and 4.0 ng/mL, respectively. Scan sensitivity was 33% in patients with a trigger PSA level of less than 0.3 ng/mL and 77% in patients with a trigger PSA level of greater than 0.3 ng/mL, respectively (P = 0.001). Using a binary logistic regression analysis model, we showed trigger PSA and ADT to be the only significant predictors of positive PET findings. Conclusion: 18F-FCH PET/CT proved its potential as a noninvasive 1-stop diagnostic modality enabling us to correctly detect occult disease in 74% of patients and to differentiate localized from systemic disease. In patients with biochemical recurrence, it also guides to an optimal treatment approach after initial treatment. Trigger PSA and ADT are the 2 significant predictors of 18F-FCH–positive PET lesions. ADT seems not to impair 18F-FCH uptake in hormone-refractory prostate cancer patients.
In Western Europe and North America, prostate cancer is the most common malignancy in men. It accounts for about 33% (232,090) of incidental cases of cancer in men in the United States (1,2).
Radical prostatectomy is the most frequently offered first-line curative treatment approach. Clinical follow-up of such patients is mainly through monitoring the levels of prostate-specific antigen (PSA). Biochemical recurrence—defined as a persistent PSA increase—occurs in 15% to 77% of patients within 5 y after radical prostatectomy (3,4). The accurate differentiation of locally confined versus systemic metastases is of key importance for defining the most appropriate therapeutic approach.
Imaging modalities play an important role in the restaging of prostate cancer. However, their optimal use is still under debate, because the reported sensitivity and specificity of current imaging methods such as bone scintigraphy, CT, MR imaging, and ultrasonography vary remarkably (5,6). Each of these modalities has its own limitations.
PET using 11C- or 18F-labeled choline has recently been used for the assessment of prostate cancer and has shown promising results for the detection of occult disease (7–18).
Age, the various clinical stages of disease, PSA levels, previous biochemical failure, and PSA kinetics have been suggested as predictive parameters for referring prostate cancer patients with biochemical recurrence for choline PET/CT (19,20). However, limited data are available to draw an accurate conclusion on the value of other suggested predictive parameters. The PSA cutoff for the prediction of choline PET/CT positivity has been a subject of controversy (9,14,15,17,21,22). Additionally, the influence of androgen deprivation therapy (ADT) on choline uptake was evaluated in only a few studies with limited patient populations (23,24).
The purpose of this study was to evaluate the potential value of 18F-fluoromethyldimethyl-2-hydroxyethyl-ammonium (FCH) PET/CT in the restaging of prostate cancer patients with biochemical recurrence regarding PSA levels and kinetics. Moreover, the influence of ADT on 18F-FCH PET/CT positivity in a large patient population was assessed.
MATERIALS AND METHODS
Patients
This prospective study was approved by the local ethical committee, and written informed consent was obtained from all patients.
Two hundred fifty consecutive prostate cancer patients (mean age ± SD, 68 ± 8 y) with biochemical evidence of recurrent disease after initial therapy (radical prostatectomy, radiotherapy, or ADT) were enrolled in this study between October 1, 2003, and May 15, 2012.
All patients underwent 18F-FCH PET/CT imaging for the assessment of recurrent disease. Free PSA serum concentration was determined on the day of study (mean, 46.9 ± 314.7 ng/mL; range, 0.2–4,692 ng/mL). The median PSA level was 5.6 ng/mL, and the median Gleason score was 7.
Biochemical recurrence was defined as a PSA value of more than 0.2 ng/mL after radical prostatectomy or a rise by at least 2 ng/mL (with or without short-term ADT) above the nadir PSA after radiotherapy (25).
The patients were divided into 2 groups (PSA doubling time ≤ 10 mo and PSA doubling time > 10 mo), because this cutoff is supposed to provide the most statistically significant prediction of time to distant disease progression (4). Patient characteristics are shown in Table 1. Overall, prostate surgery or radiotherapy (independent of ADT) was performed on 70.8% (177/250) and 43.2% (108/250) of patients, respectively. ADT was performed on 67.2% (168/250) of patients. At the time of 18F-FCH PET/CT imaging, 55.2% (138/250) of patients were receiving ADT. Chemotherapy and bisphosphonate therapy was performed on 8.8% (22/250) and 14% (35/250) of patients, respectively. At least a 3-mo interval was allowed between radiotherapy, chemotherapy, and 18F-FCH PET/CT.
Patient Characteristics and Treatment History
PET/CT Imaging
18F-FCH was synthesized on site (IASOcholine; IASON GmbH) as described by Vassiliev et al. (26).
Imaging was performed on an integrated 4-slice PET/CT system (Discovery LS; GE Healthcare) that consisted of a full-ring PET scanner with a 14.6-cm transverse field of view and an in-plane resolution of 4.8 mm in full width at half maximum. PET scans were acquired in 2-dimensional mode and were reconstructed with a standard ordered-subset expectation maximization iterative algorithm (2 iterative steps). Routinely, acquisition started 1 min after intravenous injection of 18F-FCH (4.07 MBq/kg of body weight) with dynamic PET images of the pelvis during 8 min (1 min/frame) to overcome the effect of urinary bladder activity.
Depending on the patient’s size, 6–7 bed positions with an acquisition time of 4 min/bed position were used from the thigh to the base of the skull (10 min after injection).
Unenhanced CT was performed for localization and attenuation correction (140 kV, 0.5 s/rotation, 5.0-mm reconstructed section thickness, 0.5-mm overlap) with a low-beam current modulation (80–120 mA) in the 40% (100/250) of patients who already had undergone contrast-enhanced CT within 2 wk before 18F-FCH PET/CT.
In all other patients (150/250), contrast-enhanced CT with a high-beam tube-current modulation (120–330 mA, 0.5 s/rotation, 5.0-mm reconstructed section thickness, 0.5-mm overlap, 512 × 512 matrix, pitch index of 1.5) was performed.
The reformatted, transverse, coronal, and sagittal views were used for interpretation.
Image Interpretation and Data Analysis
18F-FCH PET scans were interpreted by 2 nuclear medicine specialists who were aware of the patient’s history. They had access to the CT and PET/CT images for morphologic localization and correlation of PET lesions. The images were read sequentially within a maximum interval of 3 d using advanced PET/CT review software (AW-4.4; GE Healthcare).
A lesion was considered abnormal when focal tracer accumulation was greater than background activity. Semiquantitative analysis of abnormal uptake of radiotracer was performed using the maximum standardized uptake value (SUVmax). To determine the SUVmax, a volume of interest covering the entire abnormal lesion was drawn.
The diagnosis of malignant lymph nodes (LNs) on PET studies was based on the visual assessment of focal increased 18F-FCH uptake corresponding to the CT findings. LNs with increased 18F-FCH uptake were considered positive even if they were smaller than 10 mm. LNs without abnormal tracer uptake were considered benign even if they were larger than 10 mm. Faint 18F-FCH uptake in inguinal LNs was interpreted as reactive (9,12,18) and was excluded.
Whether bone lesions were considered malignant depended on their anatomic localization or characteristic morphologic changes.
The final interpretations were made in consensus by 2 nuclear medicine specialists and a board-certified radiologist.
Final Diagnosis
Local Recurrence and LNs
In 4.4% (11/250) of patients, the final diagnosis of local recurrence or positive LNs on PET studies was based on histopathologic findings. Lesions with increased 18F-FCH uptake were considered to be malignant if showing persistent or increased uptake in follow-up PET studies corresponding to morphologic changes on CT or if, under treatment, showing decreased 18F-FCH activity that correlated with clinically regressive findings.
Bone Metastases
Lesions were considered to be bone metastases if they were positive both on 18F-FCH PET and on CT, with corresponding positive uptake in an additional bone-seeking modality (i.e., 18F-fluoride PET/CT or bone scanning) or positive findings on MR imaging. Discrepancies between 18F-FCH PET and CT required further verification on clinical and 18F-FCH PET/CT follow-up examinations after at least 6 mo (range, 6–24 mo). Persisting lesions with increased 18F-FCH uptake, corresponding malignant morphologic changes on CT, or clinical evidence of disease progression were considered to indicate malignancy.
Statistical Analysis
SPSS statistical software system (version 16; SPSS Inc.) was used for data analysis. Univariate analysis was done for frequency and descriptive analysis. Independent t testing was used for comparison of quantitative variables between different groups, and χ2 testing was done for comparison of ratios between the groups. ANOVA was done for comparison of multiple groups. Logistic regression analysis was done for prediction of PET positivity using different variables. A P value of less than 0.05 was considered significant in all comparisons.
RESULTS
18F-FCH PET was positive in 74% (185/250) of patients and negative in 26% (65/250). Forty-five patients (18%) had local recurrence (Fig. 1), and 33 patients (13.2%) had LN recurrence only. Bone metastases only (Fig. 2) were found in 24 patients (9.6%). Overall, 38% (95/250) of patients had local recurrence, 37.6% (94/250) had LN metastases, and 28% (70/250) had bone metastases. Only 40% (38/95) of patients with LN metastases had local recurrence as well.

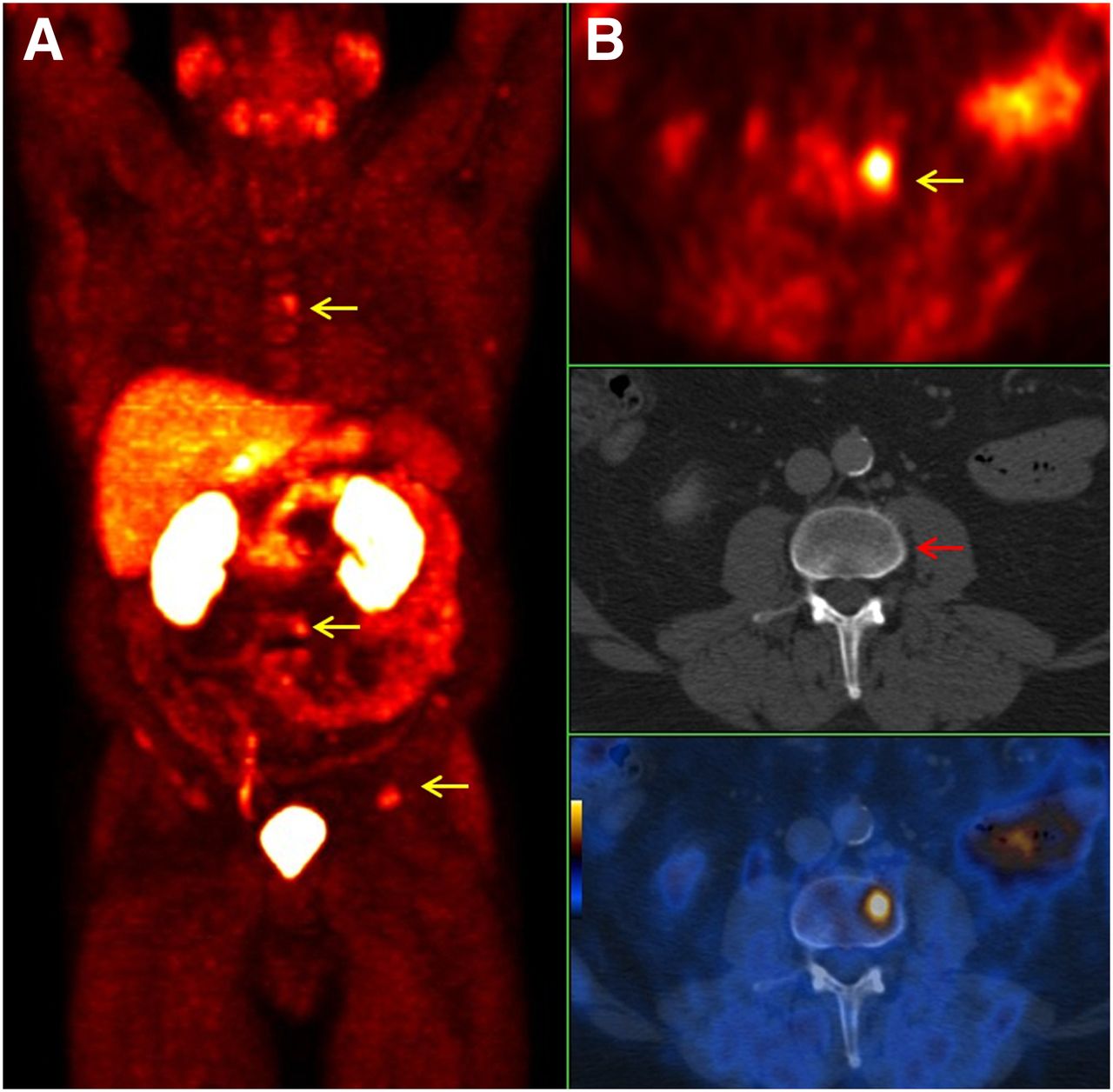
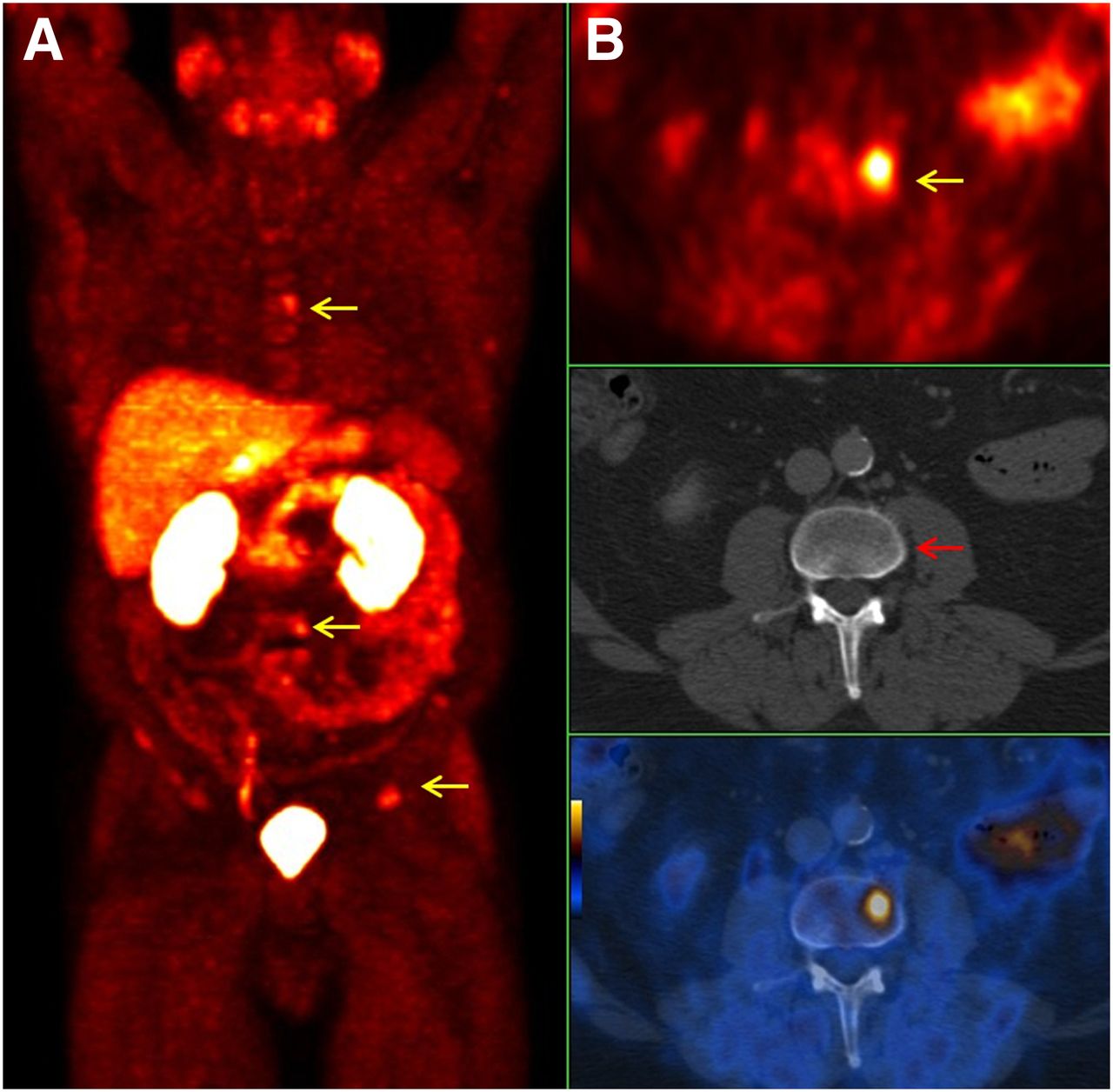
A 70-y-old prostate cancer patient (pT2a, R0, Gleason score of 7, primary PSA level of 16.1 ng/mL) with increasing PSA level of 9.71 ng/mL 13 y after radical prostatectomy. (A) Dynamic 18F-FCH PET images (top: 1 min after injection; bottom: 8 min after injection) showing pathologic increased uptake (arrow) 1 min after injection. (B) Transaxial 18F-FCH PET/CT images from pelvis 4 min after injection (top: 18F-FCH PET; middle: CT; bottom: PET/CT) showing pathologic increased uptake (arrow) on prostate bed (local recurrence).
A 64-y-old prostate cancer patient (pT3a, N0, R0, Gleason score of 7, primary PSA level of 1.34 ng/mL) with increasing PSA level of 4.7 ng/mL 3 mo after radiotherapy. (A) 18F-FCH PET maximum-intensity projection showing multiple foci of pathologic increased 18F-FCH uptake on skeleton (arrows). (B) Transaxial 18F-FCH PET/CT images (top: 18F-FCH PET; middle: CT; bottom: PET/CT) showing early bone marrow metastasis (L3) with pathologic increased uptake (left lateral part, yellow arrow) and no morphologic changes on CT (red arrow).
In 28% of patients (69/250), only a solitary malignant lesion was detected on 18F-FCH PET (65.2% [45 patients] with local recurrence, 18.8% [13 patients] with LN metastases, and 15.9% [11 patients] with bone metastases). Most of these patients (92.6%) had a trigger PSA level of less than 20 ng/mL. Mean SUVmax was 6.4 ± 2.6, 5.9 ± 2.9, and 8.9 ± 6.2 ng/mL in patients with local recurrence, LN metastases, and bone metastases, respectively. If contrast-enhanced CT was performed, PET positivity was significantly higher than when unenhanced CT was performed (81.2% vs. 69.1%, P = 0.04).
PSA Kinetics and PET Positivity
The mean PSA level in patients with negative 18F-FCH PET findings was 2.75 ± 3.8 ng/mL, compared with 8.95 ± 15.4 ng/mL in patients with local recurrence (P = 0.01), 5.8 ± 6.6 ng/mL in patients with LN metastases only (P = 0.12), and 5.4 ± 6.4 ng/mL in patients with bone metastases only (P = 0.20). The mean PSA level was 126.1 ng/mL in patients with distant metastases (i.e., all lesions except local recurrence and locoregional LNs) but 15.2 ng/mL in patients without distant metastases (P = 0.11). The mean PSA level at the time of imaging was significantly higher in patients with triple sites of involvement (i.e., local recurrence, LN metastases, and bone metastases; mean PSA, 391.1 ± 1,241.8 ng/mL) than in patients with only 1 or 2 sites of involvement (mean PSA, 6.71 ± 9.46 and 55.8 ± 179.3 ng/mL, respectively; P < 0.01). Scan sensitivity was 33% in patients with a trigger PSA level of less than 0.3 ng/mL and 77% in patients with a trigger PSA level of more than 0.3 ng/mL (P = 0.001). The 18F-FCH PET sensitivity was 77.5%, 80.7%, 85.2%, and 92.8% for the trigger PSA levels of 0.5, 1, 2, and at least 4 ng/mL, respectively (P < 0.001). In other words, the higher the trigger PSA level, the more positive are the PET results that can be expected (Fig. 3). Interestingly, there was no correlation between trigger PSA level and SUVmax (r = 0.05, P = 0.5).
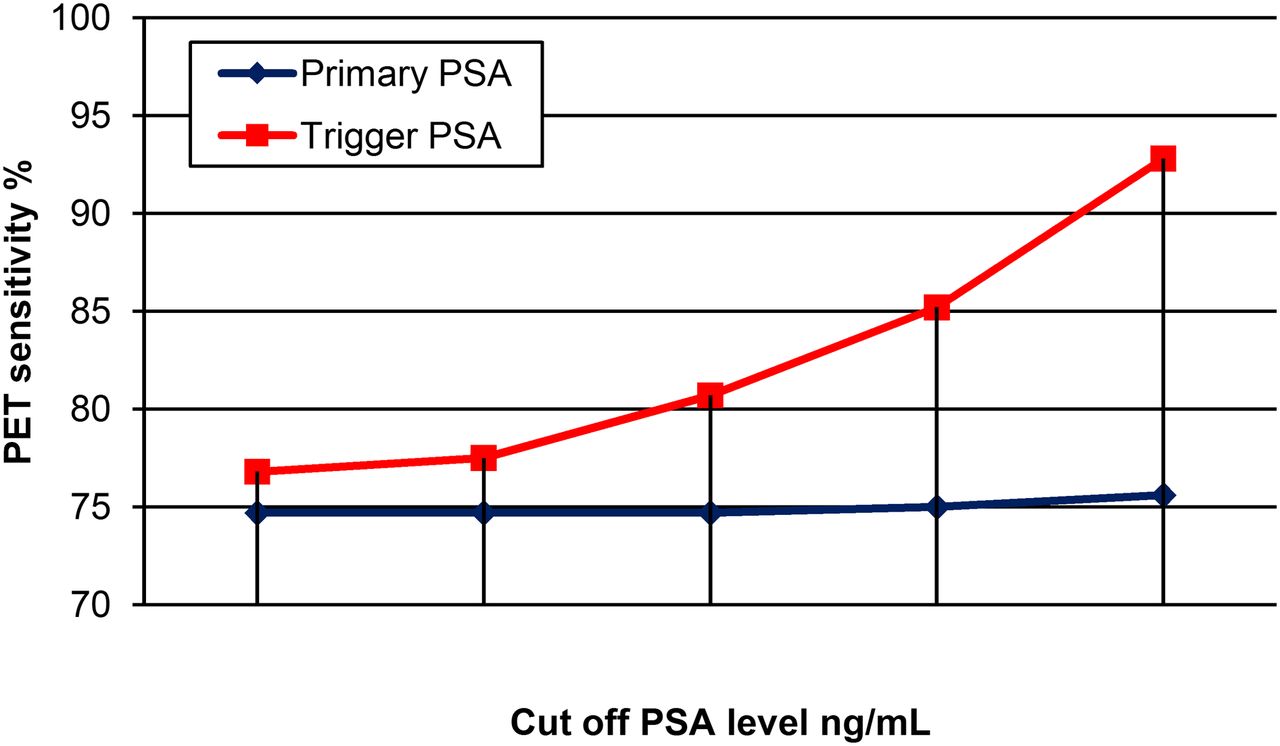
PET sensitivity (vertical axis) with respect to cutoff primary PSA level and trigger PSA level (horizontal axis).
The mean primary PSA level (i.e., at the time of initial diagnosis) was 17.6 ± 23.9 and 35.6 ± 87.7 ng/mL in patients with negative and positive 18F-FCH PET/CT findings, respectively (P = 0.01). The 18F-FCH PET sensitivity was 74.7%, 75.0%, and 75.6% for primary PSA levels of 1.0, 2.0, and 4.0 ng/mL, respectively. No patient had a primary PSA level of less than 1.0 ng/mL in our study.
18F-FCH PET findings were positive in 78.6% and 72.6% of patients with a PSA doubling time of less than or equal to 10 mo and greater than 10 mo, respectively (P = 0.3).
ADT and PET Positivity
The number of patients with and without ADT corresponding to the 18F-FCH PET results is shown in Table 2. At the time of imaging, the mean PSA level was 76.0 ng/mL (range, 0.2–4,692 ng/mL) and 11.8 ng/mL (range, 0.2–378.5 ng/mL) in patients with and without ADT, respectively (P = 0.08). However, the primary PSA level was significantly higher (P = 0.001) in patients with ADT (43.8 ng/mL; range, 1.3–742 ng/mL) than in those without ADT (13.7 ng/mL; range, 1.20–100.3 ng/mL). The sensitivity of 18F-FCH was significantly higher (P = 0.001) in patients with ADT (85%; confidence interval [CI], 80%–91%) than in patients without ADT (59.5%; CI, 50%–69%).
Number of Patients with Positive and Negative 18F-FCH PET Corresponding to ADT
18F-FCH PET showed a sensitivity of 79.3%, 78.9%, and 89.8% in patients undergoing ADT for less than 6 mo, 6–24 mo, and more than 24 mo, respectively (P = 0.18). Also, 62% (28/45) of patients with local recurrence only (P = 0.01), 61% (20/33) with LN metastases only (P = 0.05), and 67% (16/24) with bone metastases only were under ADT whereas 30.8% (20/65) of patients with negative 18F-FCH PET were under ADT (P = 0.001). ADT preoperatively, postoperatively, or at the time of imaging was associated with a higher number of positive 18F-FCH PET studies (P < 0.001).
Additionally, 18F-FCH PET showed a sensitivity of 75.9%, 64.3%, and 76.4% in patients with an interval between initial ADT and PET imaging of less than 6 mo, 6–24 mo, and more than 24 mo, respectively (P = 0.26).
Mean SUVmax (Table 3) was slightly higher in patients with ongoing ADT than in patients without ADT (9.3 ± 5.7 vs. 7.8 ± 4.7, respectively, P = 0.08). Also, mean SUVmax was not significantly different between patients according to the duration of ADT (P = 0.52). The value of SUVmax in patients with only local recurrence or LN or bone metastases and its relation to ADT is shown in Table 4.
18F-FCH PET Sensitivity in Patients With and Without ADT Correlating with Trigger PSA and Tracer Intensity
Comparison of SUVmax in Malignant Lesions With and Without ADT
Risk Stratification and PET Positivity
18F-FCH positivity increased from 58.5% (CI, 43%–74%) in low-risk patients to 67.8% (CI, 59%–76%) in intermediate-risk patients and further to 89.2% (CI, 83%–96%) in high-risk patients (P < 0.001). In low-risk patients (n = 41), 18F-FCH PET was positive in 81.8% and 50% of patients with and without ADT, respectively (P = 0.06). In the intermediate-risk group (n = 116), 18F-FCH PET sensitivity was 78% and 56.4% in patients with and without ADT, respectively (P = 0.01). In high-risk patients (n = 93), 18F-FCH PET sensitivity was 94% and 76.9% in patients with and without ADT, respectively. In addition, 18F-FCH PET was positive in 66.7% of high-risk patients with a PSA level of no more than 1.0 ng/mL under ADT.
Predictive Factors for PET Positivity
Binary logistic regression analysis was done to predict PET positivity. The variables that were included in the model were PSA level at the time of PET imaging, tumor stage, Gleason score, primary PSA level, ADT at the time of imaging, interval between initial treatment and PET, and PSA doubling time (≤10 mo or >10 mo). The model was able to predict (χ28 = 44.5, P < 0.001) 18F-FCH PET positivity in 82.4% (sensitivity of 91.9% and specificity of 48.4%). The Cox and Snell R2 and the Nagelkerke R2 were 0.26 and 0.41, respectively. The only significant variables in the model were PSA level at the time of PET (odds ratio, 1.25, with 95% CI of 1.07–1.46; P = 0.003) and ADT (odds ratio, 3.71 with 95% CI of 1.25–10.97; P = 0.01). Thus, for every ng/mL of PSA increase at the time of imaging, the chance of having positive PET findings increased by a factor of 1.25. Also, patients undergoing ADT had a 3.71 times greater chance of having positive PET findings. Tumor stage and PSA doubling time were not significant predictors.
DISCUSSION
In prostate cancer, correct determination and localization of cancer relapse is of great importance, particularly for defining the best therapeutic approach. A rise in PSA value after radical prostatectomy or radiotherapy represents biochemical recurrence. In this clinical setting, although pathologic and clinical findings (e.g., PSA levels and kinetics) may be helpful (27), imaging techniques are usually used to identify patients with local recurrence and those with distant metastases. In patients with increasing PSA serum levels after radical prostatectomy, ultrasonography-guided transrectal biopsy is performed as the first procedure for evaluating local recurrence but is only 50% effective (28). The main limitations of this method are false-negative results due to tissue-sampling errors and painfulness as an invasive procedure (28). MR imaging and CT are the most common modalities currently used for the evaluation of LN metastases. The 2 modalities perform equally poorly (29), mainly because of the use of morphologic criteria (Fig. 4). In the last few decades, bone scintigraphy has been used for the evaluation of bone metastases, as the skeletal system is the most important single site of metastasis (85%–90% of prostate cancer patients) (30). Despite its high sensitivity, it suffers from poor specificity, and further imaging modalities therefore are often required to characterize lesions with increased tracer uptake (31).

A 63-y-old prostate cancer patient (pT3a, N0, R1, Gleason score of 9, primary PSA level of 9.0 ng/mL) with increasing PSA level of 22.56 ng/mL; patient underwent radical prostatectomy and radiotherapy of prostate in 2004, and ADT has been ongoing since 2005. (A) 18F-FCH PET MIP (maximum intensity projection) showing multiple sites of pathologic increased tracer in pelvis and retroperitoneum (blue arrow). (B) Transaxial 18F-FCH PET/CT images (top: 18F-FCH PET; middle: CT; bottom: PET/CT) showing LN metastases with pathologic increased tracer uptake in right external iliac region (left, yellow arrow) and common iliac region (right, yellow arrow); However, CT (middle) shows only small nonsuggestive LNs (red arrows)
Considering the mentioned limitations of the current imaging modalities, many recent investigations have assessed the value of 11C- and 18F-choline PET/CT as a single noninvasive modality in the restaging of prostate cancer patients with biochemical recurrence after initial treatment (7,9,12,14,16,17,21,32–35). A sensitivity of between 43% and 95% was reported in previous studies using choline PET/CT in the detection of malignant lesions in recurrent prostate cancer. Moreover, several studies have evaluated the influence of various clinical (e.g., tumor stage, Gleason score, and ADT) and laboratory findings (e.g., PSA level, PSA velocity, and PSA doubling time) on choline PET/CT in patients with rising PSA levels after initial treatment (15,19,20,22,23,31). The promising value of choline PET/CT in the detection of occult malignant lesions in recurrent prostate cancer, as well as predictive factors on choline PET positivity, has been studied over the last few years. However, open issues such as defining a PSA cutoff and the influence of ADT and its interval on choline PET should be addressed in order to define a consensus for performing choline PET/CT on prostate cancer patients with biochemical recurrence.
In our study with a large patient population, 18F-FCH PET/CT showed an overall sensitivity of 74% in the detection of malignant lesions with biochemical recurrence after initial therapy, thus clearly supporting the previous published data concerning the feasibility of this examination in the restaging of prostate cancer patients.
Accurate identification of sites of cancer relapse is of great concern. In patients with local recurrence, radiotherapy has been shown to be effective in 48%–56% in preventing further recurrence for at least 3 y (36).
In those with distant metastases, ADT is the best therapeutic procedure. In our patient population, 18F-FCH PET/CT was able to determine systemic relapse (Fig. 5) in 50.8% (127/250) of patients. In addition, 18F-FCH PET/CT enabled the selection of 28% (69/250) of patients with only 1 malignant lesion. Among these patients, 65.2% had local recurrence (Fig. 3), 18.8% had a single LN metastasis, and 15.9% had a single focus of bone metastasis. Detection of a single lesion may change the treatment options from a systemic approach to local salvage therapy. These data also reinforced the findings previously reported by other authors (19,31).
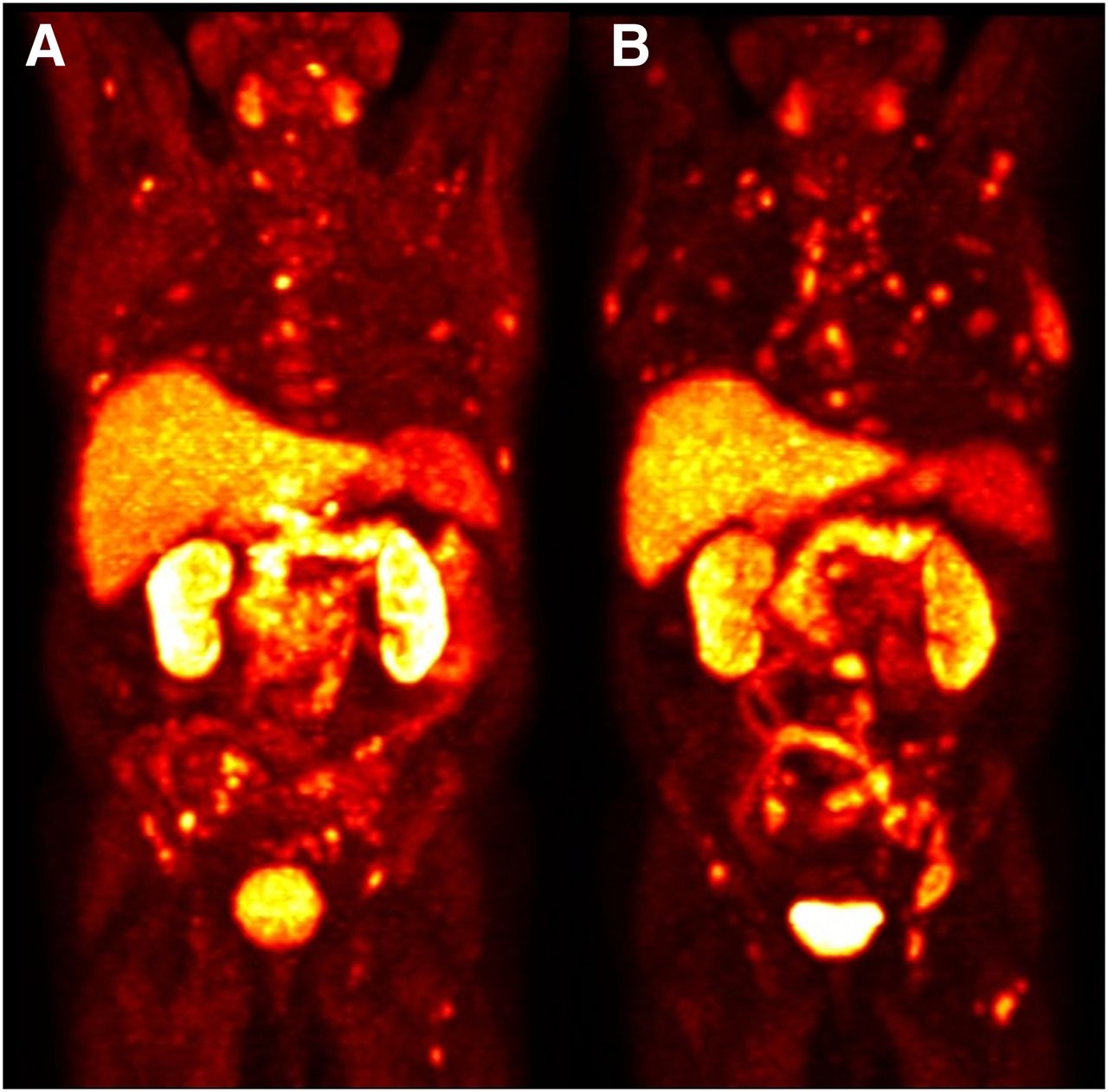
An 80-y-old prostate cancer patient (pT3b, pN0, R1, Gleason score of 7, primary PSA level of 8.9 ng/mL) with increasing PSA level of 28.41 ng/mL; patient underwent radical prostatectomy in 1999 and radiotherapy of prostate in 2000, and ADT has been ongoing since 2004. (A) 18F-FCH PET maximum-intensity projection performed in November 2011 (PSA level: 28.41 ng/mL) showing multiple LN metastases and bone metastases. (B) Follow-up 18F-FCH PET maximum-intensity projection performed in May 2012 after 8 cycles of chemotherapy showing disease progression despite relative constant PSA level of 27.85 ng/mL.
Some groups reported a low sensitivity for choline PET/CT in patients with PSA levels lower than 4–5 ng/mL (14,22) and found a linear relationship between the absolute PSA value and identification of the site of relapse (22). However, recent studies by Giovacchini et al. and Schillaci et al. (19,31) suggested a PSA cutoff of 2.0 and 1.4 ng/mL, respectively, as best for performing choline PET/CT imaging in the assessment of prostate cancer patients with a rising PSA level after initial treatment. In our series, 18F-FCH PET sensitivity was 77.5%, 80.7%, 85.2%, and 92.8% for a trigger PSA cutoff of more than 0.5, 1.0, 2.0, and 4.0 ng/mL, respectively (P < 0.001). In addition, 18F-FCH PET was positive in 66.7% of high-risk patients with PSA levels of no more than 1 ng/mL under ADT. The mean primary PSA level was also significantly higher in 18F-FCH PET–positive patients.
In a recent study, Giovacchini et al. (20) introduced the PSA doubling time as an independent predictor of 11C-choline PET/CT positivity. However, our results showed no significant difference in 18F-FCH PET positivity between patients with a PSA doubling time of less than or equal to 10 mo and those with a doubling time of greater than 10 mo.
Moreover, in our study, different variables were included in binary logistic regression analysis to predict 18F-FCH PET positivity. The model could correctly predict 18F-FCH PET positivity in 82.4%, with a sensitivity of 91.9% and a specificity of 48.4%. The only variables significant in the model were the PSA level at the time of PET (odds ratio, 1.25, with a 95% CI of 1.07–1.46; P = 0.003) and ADT (odds ratio, 3.71, with a 95% CI of 1.25–10.97; P = 0.01). It means that for every ng/mL of PSA increase, the chance of having positive PET findings is increased by a factor of 1.25. Nevertheless, tumor stage and PSA doubling time were not significant predictors.
In a preliminary study, Fuccio et al. (24) showed that ADT significantly reduces 11C-choline uptake in androgen-sensitive prostate cancer patients. However, there are different aspects concerning the influence of ADT on choline PET/CT in hormone-refractory patients with biochemical recurrence. To our best knowledge, to date there have been only 2 cross-sectional studies in which the authors took this subject into account (19,37). In the first study, Givacchini et al. (19) reported a higher sensitivity (56%) for 11C-choline PET/CT in hormone-resistant patients than in hormone-sensitive patients (44%). In addition, hormone resistance was a significant predictor of 11C-choline PET positivity in a univariate analysis. Similar findings were reported by Castellucci et al. (37) in 102 prostate cancer patients with PSA levels of less than 1.5 ng/mL.
In our study, the sensitivity of 18F-FCH was significantly higher (P = 0.001) in patients with ongoing ADT (85%; CI, 80%–91%) than in patients without ADT (59.5%; CI, 50%–69%). ADT previously, postoperatively, or at the time of imaging was associated with a higher number of positive PET studies (P < 0.001). There was no significant difference between patients with various durations of ADT (i.e., <6 mo, 6–24 mo, and >24 mo) or in patients with different intervals between initial ADT and 18F-FCH PET. In addition, patients with ADT had a 3.71 times greater chance of having positive PET findings. Moreover, mean SUVmax was slightly higher in patients with ongoing ADT than in patients without ADT (9.3 ± 5.7 vs. 7.8 ± 4.7, respectively, P = 0.08).
These results showed that PSA level and ADT were the only significant predictors of 18F-FCH PET positivity. Our findings are in contrast to previously published data (24) indicating that choline uptake will be significantly reduced by ADT. This discrepancy may be related to disease aggressiveness or other factors such as advanced primary tumor stage in hormone-refractory prostate cancer patients.
The results of our study and of recently published data (19,37) assume that ADT does not significantly affect choline uptake in hormone-refractory patients who develop biochemical recurrence. In contrast, choline PET/CT is more likely positive in such patients than in those who respond to ADT. Hence, on the basis of current data, withdrawal of ADT seems unnecessary before choline PET/CT scanning. Nevertheless, further paired studies are needed concerning mechanisms causing inhibition of choline uptake by ADT (38).
One limitation of this study is that, for ethical reasons, confirmation of all detected lesions by 18F-FCH PET/CT was not possible and only 4.4% of lesions were examined by histopathology. Other lesions were proved to be malignant on the basis of a consensus of clinical and follow-up imaging studies. However, malignant lesions in different sites may have responded differently to the therapy, potentially causing a bias in the results of this study.
In addition, prostate cancer patients with recurrent disease may undergo various therapeutic approaches. Although ADT is supposed to have a particular influence on 18F-FCH uptake, different therapy regimes (e.g., radiotherapy, chemotherapy, and bisphosphonate therapy in addition to ADT) may also affect the 18F-FCH PET/CT findings. However, such an analysis was out of the scope of this study and requires evaluation in future studies. Nevertheless, the effect of radiotherapy and chemotherapy on 18F-FCH PET/CT findings seems to be negligible in this study, as at least a 3-mo interval should be considered between completing these therapies and performing 18F-FCH PET/CT.
CONCLUSION
Our study showed that PSA level and ADT were the only significant predictors of 18F-FCH PET/CT positivity in prostate cancer patients with biochemical recurrence.
18F-FCH PET/CT proved its potential as a noninvasive 1-stop diagnostic modality enabling us to correctly differentiate localized from systemic disease and to guide us to the optimal treatment approach in prostate cancer patients with biochemical recurrence. It can also provide useful information even when there is a low rising PSA level of 0.5 ng/mL especially in intermediate- and high-risk patients. The sensitivity of 18F-FCH PET/CT was directly related to the trigger PSA level. However, there was no significant difference in 18F-FCH PET positivity between patients with a PSA doubling time of less than or equal to 10 mo and those with a doubling time of more than 10 mo.
The sensitivity of 18F-FCH PET/CT was significantly higher in patients with ongoing ADT than in those without ADT. Furthermore, ADT did not significantly impair 18F-FCH uptake in malignant lesions.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 4, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 19, 2012.
- Accepted for publication November 29, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Multiphasic 68Ga-PSMA PET/CT in the Detection of Early Recurrence in Prostate Cancer Patients with a PSA Level of Less Than 1 ng/mL: A Prospective Study of 135 Patients
- 11C-Choline PET/CT in Recurrent Prostate Cancer: Retrospective Analysis in a Large U.S. Patient Series
- 64CuCl2 PET/CT in Prostate Cancer Relapse
- 11C- or 18F-Choline PET/CT for Imaging Evaluation of Biochemical Recurrence of Prostate Cancer
- Bombesin-Targeted PET of Prostate Cancer
- Evaluation of Prostate Cancer Bone Metastases with 18F-NaF and 18F-Fluorocholine PET/CT
- Pilot Comparison of 68Ga-RM2 PET and 68Ga-PSMA-11 PET in Patients with Biochemically Recurrent Prostate Cancer
- Prospective Comparison of 18F-Fluoromethylcholine Versus 68Ga-PSMA PET/CT in Prostate Cancer Patients Who Have Rising PSA After Curative Treatment and Are Being Considered for Targeted Therapy
- Dosimetry and First Clinical Evaluation of the New 18F-Radiolabeled Bombesin Analogue BAY 864367 in Patients with Prostate Cancer
- 11C-Choline PET/CT Predicts Prostate Cancer-Specific Survival in Patients with Biochemical Failure During Androgen-Deprivation Therapy
- Clinical and research applications of simultaneous positron emission tomography and MRI