


Abstract
The aim of this first-in-man study was to demonstrate the feasibility, safety, and tolerability, as well as provide dosimetric data and evaluate the imaging properties, of the bombesin analogue BAY 864367 for PET/CT in a small group of patients with primary and recurrent prostate cancer (PCa). Methods: Ten patients with biopsy-proven PCa (5 with primary PCa and 5 with prostate-specific antigen recurrence after radical prostatectomy) were prospectively selected for this exploratory clinical trial with BAY 864367, a new 18F-labeled bombesin analogue. PET scans were assessed at 6 time points, up to 110 min after intravenous administration of 302 ± 11 MBq of BAY 864367. Imaging results were compared with 18F-fluorocholine PET/CT scans. Dosimetry was calculated using the OLINDA/EXM software. Results: Three of 5 patients with primary disease showed positive tumor delineation in the prostate, and 2 of 5 patients with biochemical relapse showed a lesion suggestive of recurrence on the BAY 864367 scan. Tumor-to-background ratio averaged 12.9 ± 7.0. The ratio of malignant prostate tissue to normal prostate tissue was 4.4 ± 0.6 in 3 patients with tracer uptake in the primary PCa. Mean effective dose was 4.3 ± 0.3 mSv/patient (range, 3.7–4.9 mSv). Conclusion: BAY 864367, a novel 18F-labeled bombesin tracer, was successfully investigated in a first-in-man clinical trial of PCa and showed favorable dosimetric values. Additionally, the application was safe and well tolerated. The tracer delineated tumors in a subset of patients, demonstrating the potential of gastrin-releasing-peptide receptor imaging.
- prostate cancer
- GRP receptor imaging
- gastrin-releasing peptide
- 18F-radiolabeled bombesin analogue
- dosimetry
Prostate cancer (PCa) is one of the leading causes of death among men in the Western world (1). Screening methods in the diagnostic process include a prostate-specific antigen blood test followed by digital rectal examination. However, these screening methods do not allow the primary location of the carcinoma cells to be determined with high accuracy or possible metastases to be diagnosed. In recurrent PCa, the location of tumor tissue may be relevant to further therapy planning. Although local recurrence can be treated with reoperation or local radiation therapy with curative intent, patients with distant metastases are commonly referred for systemic therapy. Therefore, there is a great need for sensitive and specific imaging to detect primary and recurrent tumors, as well as metastases.
PET/CT is a highly sensitive hybrid imaging modality that allows examination of the whole body (2). The poor performance of the most commonly used tracer in cancer, 18F-labeled glucose (18F-FDG), for the detection of PCa is due to the relatively slow growth of well-differentiated PCa and consequently low glucose metabolism (3,4). This drawback has led to the development of other PET tracers such as 11C-choline and 18F-choline, which have been reported to be potentially useful for the detection of PCa lesions and are in routine clinical use (5–7). However, the fact that radiolabeled choline analogues cannot differentiate between benign hyperplastic prostate cells and malignant carcinoma cells may limit their diagnostic value. Hence, much effort has been put into developing new prostate carcinoma–specific PET tracers with high diagnostic sensitivity and specificity.
One of these specific targets worth investigating is the gastrin-releasing-peptide receptor (GRPr), a G-protein–coupled receptor belonging to the family of bombesin receptors (8). In 1989, it was discovered that bombesin stimulates the growth of human PCa cells (9). An extensive in vitro autoradiographic GRPr evaluation in prostate tissue showed a high receptor density in cells of primary invasive PCa and in high-grade prostatic intraepithelial neoplasias (10). It was further discovered that these receptors are overexpressed rarely and, if expressed, then only in low density in benign prostatic hyperplasia and normal prostate tissue (10).
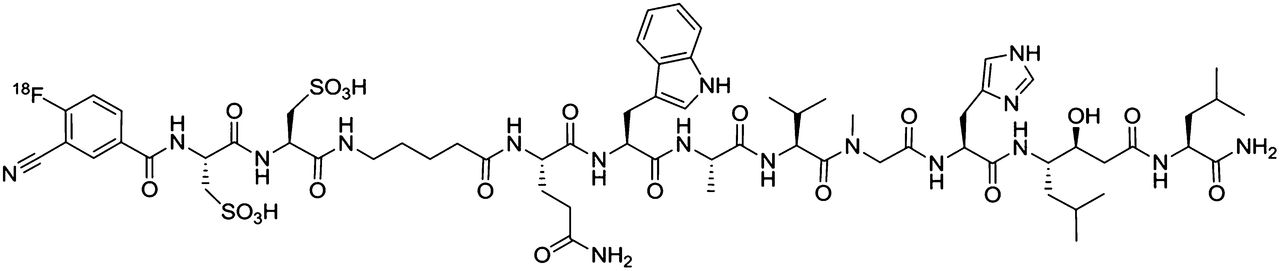
BAY 864367 (3-cyano-4-18F-fluorobenzoyl-Ala(SO3H)-Ala(SO3H)-Ava-Gln-Trp-Ala-Val-NMeGly-His-Sta-Leu-NH2) (Fig. 1) has been identified as a potent synthetic GRPr antagonist that can be directly radiolabeled with 18F and has clearly visualized human PCa (PC-3) xenografts in mice (11). The aim of this first-in-man study was to demonstrate the feasibility, safety, and tolerability, as well as provide dosimetric data and get first hints on the diagnostic value, of the PET tracer BAY 864367 in patients with primary and recurrent PCa.
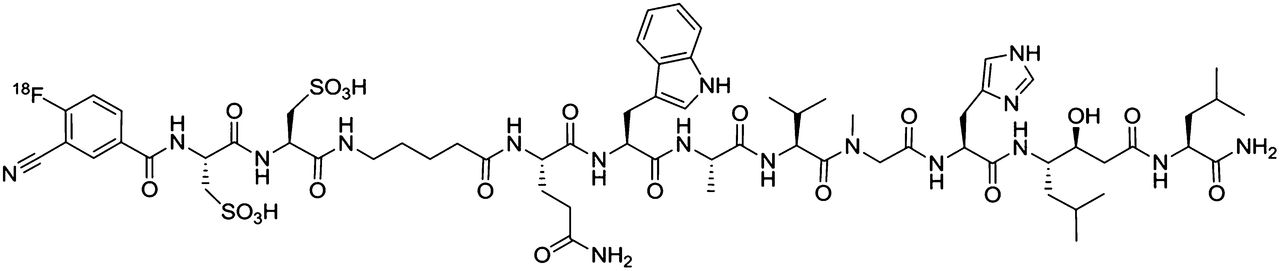
Chemical structure of 18F-BAY 864367.
MATERIALS AND METHODS
Patients
Five patients with biopsy-proven primary PCa and 5 patients with a rising level of prostate-specific antigen after radical prostatectomy were prospectively selected for the study (n = 10). This clinical study met all local legal and regulatory requirements and was performed in accordance with the ethical principles originating from the Declaration of Helsinki and the International Conference on Harmonization guideline E6: “Good Clinical Practice.” Five patients with primary PCa were scheduled for prostatectomy and did not receive any prostate-specific therapy before the BAY 864367 PET/CT scan. All patients gave written informed consent according to our local ethics committee regulations.
Preparation of BAY 864367, Quality Control of BAY 864367, Safety Monitoring, and Data Acquisition
Preparation of BAY 864367, quality control of BAY 864367, safety monitoring, and data acquisition are described in the supplemental materials (available at http://jnm.snmjournals.org).
Data Analysis
Attenuation-corrected images were analyzed visually by 2 experienced nuclear medicine physicians in consensus. Imaging results using BAY 864367 were compared with 18F-fluorocholine PET/CT (n = 9). Whole-body PET/CT scans (from vertex of skull to mid thigh) at 30, 45, 60, 75, 90, and 110 min after injection of 302 ± 11 MBq of BAY 864367 were visually analyzed using the PET/CT COMPARE algorithm of the Advantage workstation (version 4.4; GE Healthcare). In patients for whom pathologic uptake had been identified on visual analysis, a volume of interest was placed over the tumor tissue, normal prostate tissue (in patients with primary PCa), and renal parenchyma. For normalization, another volume of interest was placed over lung tissue at the given time-point and uptake was measured as maximum standardized uptake value (SUVmax).
Biodistribution studies were performed using the Fusion tool of PMOD (version 3.3; PMOD Technologies). Volumes of interest were placed in the liver, gallbladder, kidneys, spleen, muscles, bladder, and lung tissue in the image series at the given time points as described above (15 min at each time point). Activity was measured in kBq/cm3. Activity on the last PET scan was assumed to remain in the organs. After 10 half-lives of 18F, total elimination was assumed. Activity/cm3 was multiplied by the organ weight, given in OLINDA/EXM (version 1.0) (12). The resulting time–activity curves were incorporated using the trapezoidal integration. The remaining fraction was calculated by subtracting the organ-normalized accumulated activities from the whole-body accumulated activity, which for 18F is 2.601 h (13). Effective doses were calculated for each patient with the help of OLINDA/EXM, version 1.0.
Histopathology
At study entry, all patients with primary PCa were scheduled for prostatectomy. The entire prostate samples were histopathologically analyzed to further confirm the imaging localization of tracer uptake (in 3 patients). Despite giving initial consent and contrary to their urologists’ treatment plan, 2 patients decided on radiotherapy rather than prostatectomy. However, in both patients a 12-core needle biopsy had been performed and the results were correlated with the respective imaging results.
RESULTS
Patient Demographics
Ten patients with prostate adenocarcinoma were included in the study. The mean age of the patients was 69 y (range, 63–77 y). Five patients had biopsy-proven primary PCa. The other 5 patients had a chemical relapse of prostate-specific antigen ranging from 5 to 214 μg/L before imaging with BAY 864367. Patient demographics are summarized in Tables 1 and 2.
Patient Characteristics and Imaging Findings
Scan and Patient Information and Tumor Activities
Safety
The injection of 302 ± 11 MBq (range, 282–317 MBq) of BAY 864367 was well tolerated. Safety data did not show any alteration in the sequential pre- and postdosing blood values, electrocardiograms, urine testing, and physical examination. No patient reported any discomfort with regard to the injection.
Imaging Results and Correlation with Histopathology and 18F-Fluorocholine PET/CT Scans
Three (patients 1–3) of 5 patients (patients 1–5) with primary PCa showed positive delineation on BAY 864367 PET scans and concordance with the biopsy results (Fig. 2). The fourth patient of our clinical trial was a 74-y-old man with biopsy-proven adenocarcinoma of the prostate (Gleason score 3 + 4). BAY 864367 scanning revealed no tumor localization in the prostate. 18F-fluorocholine PET/CT showed tracer accumulation in both lobes of the prostate. Prostatectomy identified multifocal infiltration of an adenocarcinoma in both lobes. In patient 5, BAY 864367 PET scanning did not show a suspected malignant lesion in the prostate. However, core-needle biopsy revealed tumor infiltration at the right basal prostate (Gleason score 4 + 4). 18F-fluorocholine PET/CT showed tracer accumulation in both lobes of the prostate. The Gleason score of patients with primary PCa was between 7 (4 + 3) and 9 (5 + 4) (mean, 8.2 ± 0.8).

Results from 63-y-old patient (patient 3). (A) Axial slice of CT image of pelvis. (B) Axial slice of fused PET/CT image of prostate, showing BAY 864367–positive PCa mainly in right apical lobe. (C) Corresponding histopathology slice with simultaneous staining of antibodies targeting cytokeratin 5 and 14, P63, and AMACR/P504S (mirrored horizontally).
All patients with recurrent PCa (patients 6–10) experienced a prostate-specific antigen relapse. The mean Gleason score at the time of initial diagnosis was 8.4 ± 0.9 (range, 4 + 3 to 5 + 4). Two of 5 patients with recurrent PCa showed a suggestive lesion on BAY 864367 PET/CT images. One patient (patient 8) showed focal uptake in the fourth left lateral rib (SUVmax, 2.8). On 18F-fluorocholine PET/CT, focal uptake was seen in the identical anatomic site. In patient 9, BAY 864367 PET/CT scanning showed a positive lymph node dorsal to the right external iliac vein (SUVmax, 13.2; Fig. 3). On 18F-fluorocholine PET/CT scanning, focal radionuclide uptake in the fifth and sixth thoracic vertebral bodies was seen. However, the bone lesions were considered false-positive since they were negative on follow-up 18F-fluorocholine PET/CT 1 y later. The lymph node that had shown BAY 864367 uptake persisted morphologically at that time and was therefore considered true-positive.

Results from 64-y-old patient who showed biochemical failure 11 y after initial diagnosis and extended prostatectomy. (A) Maximum-intensity projection 90 min after injection of 306 MBq of BAY 864367 (with arrow marking lymph node). (B) Axial slice of fused PET/CT images, showing bombesin-positive lymph node (arrow) dorsal to right external iliac vein. (C and D) Maximum-intensity projection of diagnostic 18F-fluorocholine PET and fused choline PET/CT slice showing no choline uptake in iliac lymph node. Unit of scale bar is g/mL (SUV).
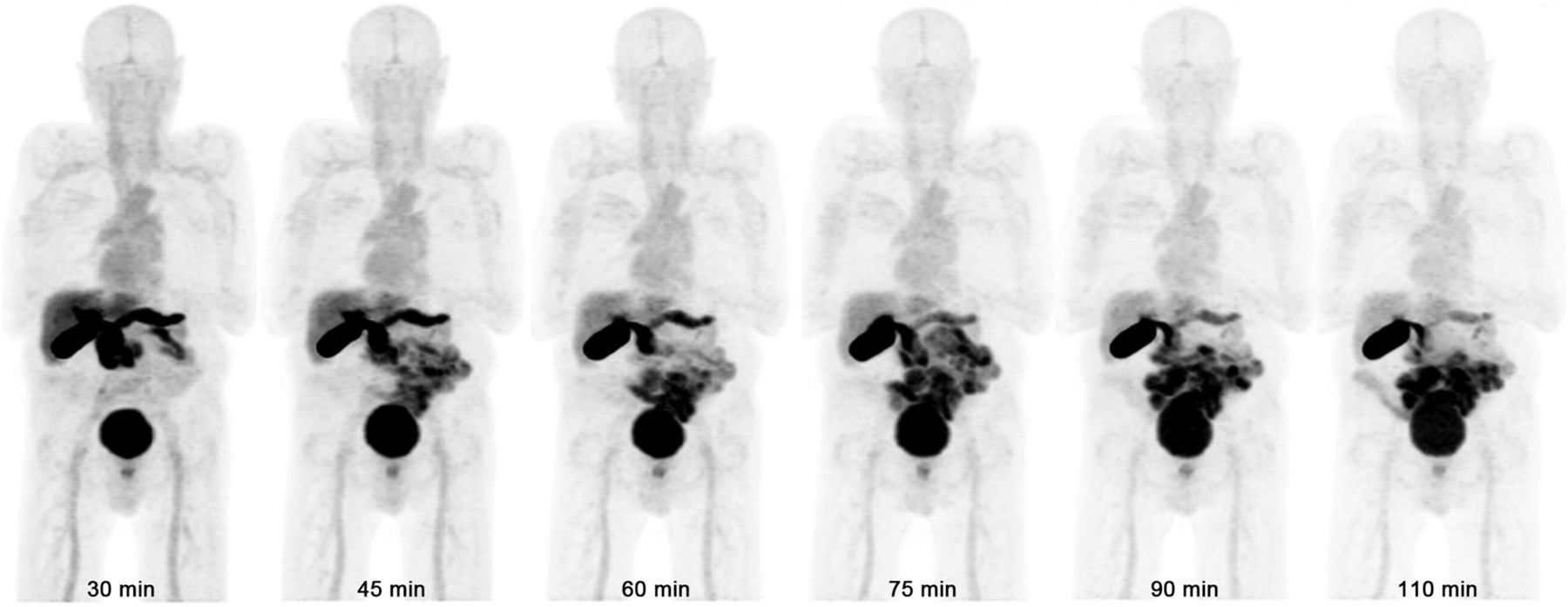
In the other 3 patients with recurrent PCa, BAY 864367 PET/CT remained negative, whereas 18F-fluorocholine PET/CT showed suggestive lesions in all of them. On the 18F-fluorocholine scan, focal uptake was seen dorsal to the left ureter for patient 6 and in the prostate compartment for patient 7, both being suggestive of a local recurrence. In patient 10, who had an advanced state of PCa, 18F-fluorocholine PET/CT revealed multiple osseous and lymph node metastases (BAY 864367 PET/CT is shown in Fig. 4). Detailed information about the imaging results is given in Tables 1–3.

Maximum-intensity projection PET images of serial static PET series from 30 to 110 min after injection of 317 MBq of BAY 864367 (patient 10). All images are displayed at same level of intensity. No pathologic uptake of BAY 864367 is seen.
Lesion-Based Analysis
Biodistribution and Semiquantitative Organ and Tumor Uptake of BAY 864367
An overview of the injected dose of BAY 864367 and the tumor-to-background ratios is shown in Table 2. The mean effective dose was 4.3 ± 0.3 mSv/patient (range, 3.7–4.9 mSv). Activity was secreted over the liver into the bile. Thus, the highest radiation dose was received by the urinary bladder wall, followed by the gallbladder wall and liver (Table 3). Tumor lesions were identified in 5 of 10 patients. The tumor-to-background ratio was 12.9 ± 7.0 (Table 2). The ratio of cancer to normal prostate tissue was 4.4 ± 0.6 in our 3 patients with tracer uptake in the primary PCa. The tumor-to-kidney ratio in all 5 patients with positive tracer uptake in tumor tissue was 4.4 ± 2.9. Tracer uptake (SUVmax) after 1.5 h was 9.1 ± 4.8 (range, 2.4–13.1) in patients with primary PCa (n = 3) and 8 ± 5.2 (range, 2.8–13.2) in patients with recurrent PCa (n = 2); because of the small number of patients, testing for statistical significance was not performed.
DISCUSSION
The aim of this first-in-man study was to demonstrate feasibility and provide dosimetric data for bombesin/GRPr-based imaging using the novel 18F-labeled tracer, BAY 864367, in a clinical trial of PCa patients. In addition, the patients were to be imaged with the current gold standard, 18F-fluorocholine PET/CT, for a direct comparison.
Since the identification of GRPr as a promising target, a plethora of radiolabeled bombesin peptides has been evaluated preclinically (14–32). These were mainly radiolabeled agonists, and a few have progressed to the clinical setting, such as demobesin 4 and 177Lu-AMBA (17,33). However, they showed only limited success, probably because of their limited metabolic stability. Recently, the 18F-labeled BAY 864367 was identified as a potent synthetic GRPr antagonist, and its preclinical evaluation showed specific and effective GRPr targeting in PC-3 tumor–bearing mice, with high tumor uptake, excellent tumor-to-background ratios, and, importantly, excellent metabolic stability (11). To further investigate this promising tracer, an exploratory clinical trial was performed.
PET imaging with BAY 864367 was shown to be safe and well tolerated in 10 patients with biopsy-proven PCa. No adverse events were observed in any of the studied subjects. The effective dose (0.014 mSv/MBq) was favorable and even lower than the reported dose of a recently published 68Ga-labeled bombesin antagonist (0.051 mSv/MBq). Radiation exposure was also lower than the reported doses for 18F-fluorocholine (0.031 mSv/MBq) and comparable to 64Cu-labeled GRPr antagonists (0.019 mSv/MBq) (6,34–36). The dosimetry results of BAY 864367 confirmed a low gastrointestinal radiation dose (Table 4), representing a clear advantage over the literature-known labeled GRPr agonists (16,36,37).
Absorbed Organ Dose (mGy/MBq) and Effective Dose (mSv/MBq) after Injection of 18F-BAY 864367
In 5 of the 10 patients, BAY 864367 displayed accumulation in the malignant prostate tissue. Three of 5 patients with primary PCa showed tumor delineation in the prostate. Although the BAY 864367 uptake rate was high in patients with primary PCa, the detection rate was lower in patients with recurrent disease. Only 2 suggestive lesions of the recurrent disease cases were detected by BAY 864367, whereas 18F-fluorocholine PET/CT depicted suggestive lesions in all 5 patients.
This particular finding corresponds to autoradiographic results published by Markwalder and Reubi, showing GRPr expression on a subject base in 4 of 7 metastases (10). Beer et al. analyzed the GRPr expression in PCa and metastases in a large cohort with immunohistochemical staining. This study found less than half of primary PCa samples to have strong GRPr staining intensity. Moreover, they found a significant inverse correlation between GRPr staining intensity and the Gleason score (8), possibly explaining why late, and probably dedifferentiated, metastases are not depicted on BAY 864367 PET/CT. This hypothesis is supported by a study by de Visser et al. (38). They investigated GRPr expression in different stages of PCa using autoradiography with labeled bombesin analogues in 12 different PCa xenograft models. They showed only androgen-dependent cell lines of PCa to have a high density of GRPr, indicating high GRPr expression only in early, androgen-dependent, stages of prostate tumor development and not in later stages (38).
Because of the low number of primary carcinomas (n = 5), our study was not powered to draw conclusions on correlations between Gleason score and tracer uptake. However, 2 of our 3 patients with recurrent PCa, for which the BAY 867548 scanning was negative, already showed a Gleason score of 9 at the time of diagnosis. Analogous to the above studies, BAY 867548 PET/CT was negative because of possible loss of receptors in these 2 patients.
In a recently published study, Kahkonen et al. investigated the use of a 68Ga-labeled peptide (BAY 867548) with high affinity to the bombesin receptor (39). This new tracer showed a high sensitivity and specificity for detection of primary PCa and lymph node metastases. In 10 of 11 patients with primary PCa, the dominant tumor lesions could be detected, and in 2 of 3 patients with a biochemical relapse, the BAY 867548 scan showed local recurrence and lymph node metastases in accordance with 11C-acetate PET/CT. The sensitivity of detection of 10 histologically proven lymph node metastases was 70% (39). These results are remarkably higher than those of the study presented here. The reason for this difference in diagnostic performance remains open, since the receptor properties are the same as in our study. However, the slight structural change between NMeGly for the 18F-compound versus Gly in the 68Ga-compound may contribute to this observation. The structural element NMe is known to greatly affect peptide stability and excretion. On the other hand, the linker in the 18F-compound has two –SO3H groups and probably affects the permeability of the tracer into the cells because the tracer will always be negatively charged at physiologic pH compared with the overall neutral 68Ga-compound (with one DOTA-CO2H adding a negative charge, which is compensated by the protonated nitrogen of the piperidine moiety of the linker). Another reason why the gallium-based tracer published by Kahkonen et al. showed a higher detection rate might be that the patients included in their study had a lower Gleason score (3.7 vs. 8.3) as discussed above. In the light of the data of Beer et al. (8) and the BAY 867548 results, bombesin PET imaging may be better suited to imaging of early PCa, whereas for late stages of the disease there may be a risk of understaging. We therefore see potential for using BAY 867548 for early, androgen-dependent stages of PCa, such as in patients with lower Gleason scores, or in patients under active surveillance. This possibility might be supported by the results of Körner et al., which showed overexpression of GRPr in prostatic intraepithelial neoplasia as early carcinoma in situ in the prostate (40).
CONCLUSION
The 18F-labeled bombesin tracer BAY 864367 is a well-tolerated imaging probe for diagnosing PCa targeting the GRPr. BAY 864367 showed favorable dosimetric values and excretion kinetics and displayed good tumor delineation in a subset of patients with PCa. Future trials must emphasize the biologic behavior of the GRPr as overexpressed mainly in early, hormone-dependent PCa. A possible future trial on a large patient collective might be designed in the setting of active patient surveillance at early stages not amenable to prostatectomy.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. The trial was financially supported by Bayer HealthCare. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the radiopharmacy of ETH, the technologists, and the administrative staff at the University Hospital of Zurich for their help in acquiring the data and freeing up resources.
Footnotes
Published online Feb. 12, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 29, 2014.
- Accepted for publication December 30, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MITIGATE-NeoBOMB1, a Phase I/IIa Study to Evaluate Safety, Pharmacokinetics, and Preliminary Imaging of 68Ga-NeoBOMB1, a Gastrin-Releasing Peptide Receptor Antagonist, in GIST Patients
- Imaging the Distribution of Gastrin-Releasing Peptide Receptors in Cancer
- Will GRPR Compete with PSMA as a Target in Prostate Cancer?
- Bombesin-Targeted PET of Prostate Cancer
- Radiopeptides for Imaging and Therapy: A Radiant Future