


Abstract
SPECT has traditionally been regarded as nonquantitative. Advances in multimodality γ-cameras (SPECT/CT), algorithms for image reconstruction, and sophisticated compensation techniques to correct for photon attenuation and scattering have, however, now made quantitative SPECT viable in a manner similar to quantitative PET (i.e., kBq⋅cm−3, standardized uptake value). This review examines the evidence for quantitative SPECT and demonstrates clinical studies in which the accuracy of the reconstructed SPECT data has been assessed in vivo. SPECT reconstructions using CT-based compensation corrections readily achieve accuracy for 99mTc to within ±10% of the known concentration of the radiotracer in vivo. Quantification with other radionuclides is also being introduced. SPECT continues to suffer from poorer photon detection efficiency (sensitivity) and spatial resolution than PET; however, it has the benefit in some situations of longer radionuclide half-lives, which may better suit the biologic process under examination, as well as the ability to perform multitracer studies using pulse height spectroscopy to separate different radiolabels.
- SPECT (single-photon emission computed tomography)
- quantification
- scatter correction
- attenuation correction
- validation
Quantitative emission tomography is a powerful investigative tool in clinical practice and biomedical research. The two principal forms of emission tomography using radionuclide-labeled compounds are SPECT and PET. Although PET has a tremendous sensitivity advantage and higher spatial resolution over conventional SPECT, mostly because of the methods of collimation used in each, SPECT arguably has some advantages over PET. The physical half-lives for many SPECT radionuclides are generally longer and more aligned with the biologic half-lives of physiologic processes of interest; radiotracers are readily available and do not require relatively close proximity to a medical cyclotron and a rapid distribution network; there is the potential for simultaneous multitracer studies with different radionuclides examining different biologic pathways in a single imaging session; and the systems are of lower cost and have a much greater installed base worldwide. As the γ-camera/SPECT component in a SPECT-only system is the same as that in a combined SPECT/CT system, we will use the terms SPECT and SPECT/CT interchangeably. In doing so, we emphasize that the SPECT acquisition and performance are independent of whether the system has a CT scanner attached.
Since the inception of PET, PET systems have been designed to produce reconstructed images that are inherently quantitative (i.e., the reconstructed data are in units of radioactivity per unit volume [kBq⋅cm−3]) because the correction for photon absorption is relatively straightforward to apply and in early 2-dimensional scanners the amount of scattered radiation detected was low enough (<5%) to be ignored. In SPECT, however, these corrections have been more challenging, and to this day much of the SPECT imaging performed is without correction for photon absorption (attenuation) or scattered radiation. Put simply, the dogma has arisen that PET is quantitative and SPECT is not, as is demonstrated by the following recent example from this journal (1): “…PET is superior to SPECT in both sensitivity and spatial resolution. Furthermore, PET enables quantitation of tissue radioactivity concentrations.”
Today, however, 3-dimensional PET systems record a large fraction of scattered events (from 35% to >50% of all detected coincident events) such that the scatter correction required is on the same order as, or even greater than, that required in SPECT. Although various strategies have been proposed to produce quantitative SPECT data, such as combined use of transmission radionuclide sources (e.g., 153Gd or 241Am) with simultaneous emission imaging to directly measure emission photon absorption (2,3), it has been the relatively recent introduction of combined SPECT/CT scanners that has given renewed impetus to this goal. The CT data complement the SPECT data by providing information about the density of the body tissues, which can be used in algorithms that aim to correct for photons that have been Compton-scattered or attenuated within the body. Although the data from CT are not absolutely essential for producing quantitative SPECT images, the ready availability of coregistered datasets of SPECT and CT has certainly assisted in the ability to apply corrections for scattered and attenuated photons more easily.
In this review, we will concentrate on the latest developments to achieve quantitative SPECT reconstruction based on the conventional NaI(Tl) γ-camera, whether used with or without a combined CT system. We do not consider the recently introduced solid-state (cadmium zinc telluride) SPECT systems in this discussion.
QUANTIFICATION IN EMISSION TOMOGRAPHY
The requirements for producing quantitative data in emission tomography are the same for PET as for SPECT. The main features are a reconstruction algorithm that behaves in a linear fashion in terms of the reconstructed radioactivity concentration, an algorithm to compensate for photon absorption within the body, an algorithm to remove scattered radiation from the data, and the ability to calibrate the reconstructed data in kBq⋅cm−3. There are several other factors that may influence the quantitative accuracy of reconstructed PET or SPECT data, including a decreased apparent radioactivity concentration in objects less than approximately 3 times the spatial resolution of the system and therefore affected by the partial-volume effect, counting rate losses due to dead time within the instrumentation, radioactive decay during the acquisition process, and corrections and normalizations for spatial and temporal variations in detector response. A subtle final point is that PET reconstruction has traditionally been performed with voxel values in units of radioactivity per unit volume (kBq⋅cm−3), that is, an image of radioactivity concentration, whereas SPECT has tended to be reconstructed as a count-based image. The difference is accentuated when a zoom is applied during reconstruction: the image reconstructed as a radioactivity concentration with or without a software zoom will represent those data with a constant numeric value per voxel; that is, the concentration of radioactivity is independent of the zoom applied. Conversely, the count-conserving algorithm in SPECT will keep the total number of reconstructed events constant and, as the object reconstructed with increasing zoom appears larger because of the magnification applied in software, the value contained in each voxel will be decreased as the total number of counts is held constant. This difference can probably be traced back to the “PET is quantitative, SPECT is not” dogma. Conversion between these two situations is, of course, relatively straightforward, even after reconstruction.
The reconstruction algorithm of choice today in emission tomography is based on one of the statistical iterative methods, as opposed to the classic analytic reconstruction methodology of filtered backprojection, with many applications using the block-iterative, ordered-subset maximum-likelihood expectation maximization algorithm (OSEM) (4). This approach has numerous attractive features, including the ability to model physical characteristics of the acquisition process in the reconstruction to enhance image quality and accuracy, and the ability to better control the signal-to-noise characteristics of the final image. Most reconstruction software today includes optional scatter and attenuation correction and, increasingly, depth-dependent resolution recovery (sometimes referred to as point-spread function correction or, alternatively, high definition).
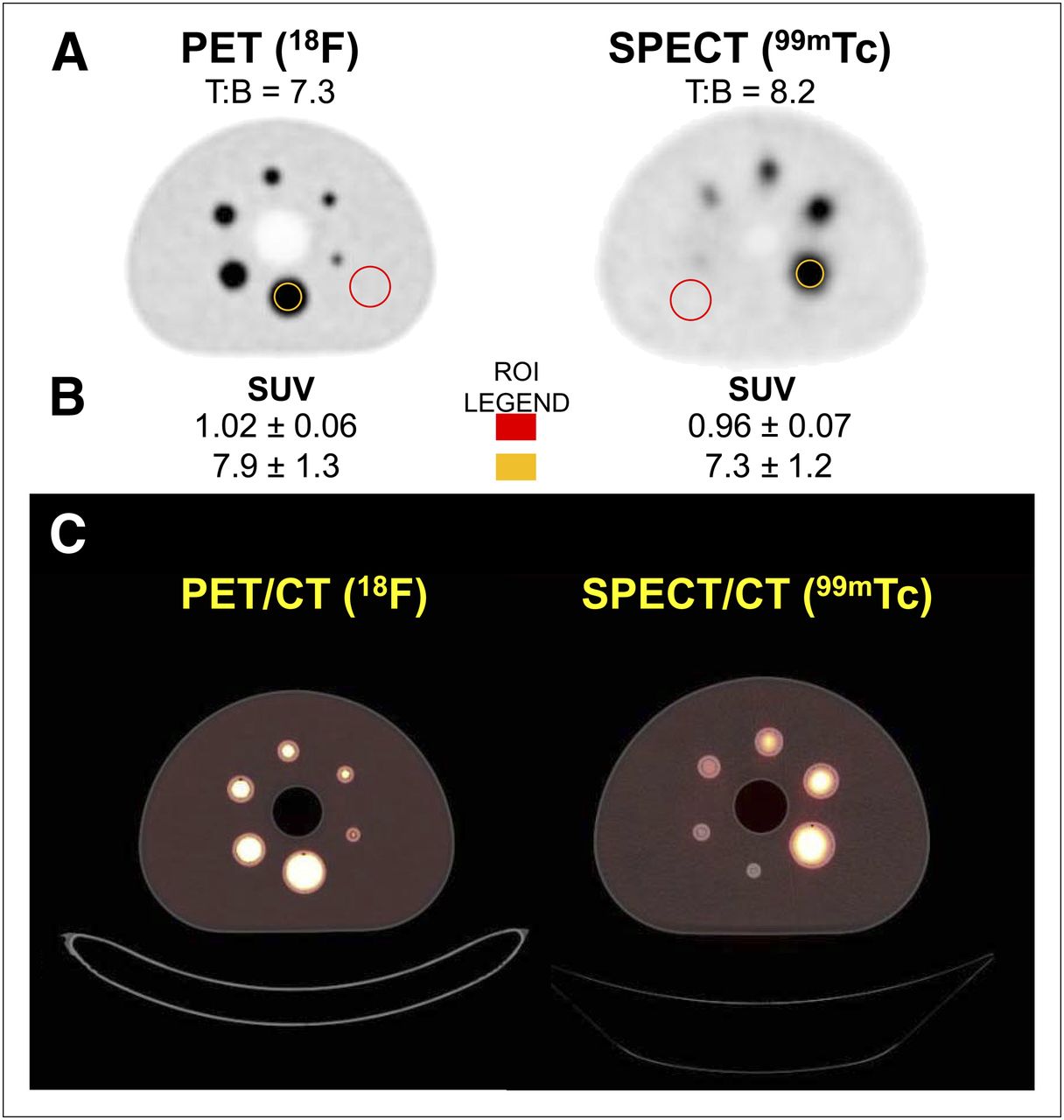
Once the quantitative accuracy of the SPECT image reconstruction in kBq⋅cm−3 has been established, it is then possible to review the data by applying parameters such as a standardized uptake value (SUV) using knowledge of the administered amount of radioactivity, delay from injection until scanning for radioactive decay correction, and patient weight/volume. An example comparing the quantitative accuracy of PET and SPECT images expressed as an SUV is shown in Figure 1.

Comparison of quantitative PET (18F) and SPECT (99mTc) images in IEC body phantom containing 6 fillable spheres. (A) PET and SPECT figures alone. (C) Same images fused with corresponding CT. T:B indicates actual target-to-background ratio for each experiment between concentration of radioactivity in spheres and in general compartment of phantom. (B) Quantitative results. Mean SUV within red region of interest (ROI) in general background should be 1.0. Yellow ROI indicates SUV50 for largest (37-mm-diameter) sphere in both cases. Standard deviation quoted refers to variability about mean within ROI. Results are for single slice through phantom corresponding to central section through largest sphere. In this example, PET SUV50 is slightly overestimated (7.9 [measured] vs. 7.3 [actual]) by about 8% whereas SPECT images are underestimated by about 11% (7.3 [measured] vs. 8.2 [actual]), probably because of partial-volume-effect losses caused by poorer spatial resolution in SPECT than in PET. Table 1 presents results for all spheres.
The data in Figure 1 were acquired using the novel in-line SPECT/CT system developed in our department and consisting of a dual-head γ-camera (SKYLight) combined with a single-slice helical CT scanner (PQ5000) (5) and a state-of-the-art lutetium oxyorthosilicate–based PET/CT scanner with time-of-flight capability and an extended axial field of view (Biograph mCT/64) (6). The test object used was the International Electrotechnical Commission (IEC) body phantom with spheric inserts as described in the latest National Electrical Manufacturers Association PET evaluation test procedures (7) except that in this case the largest 2 spheres, instead of containing nonradioactive water, were filled with the same radioconcentration of activity as were the other spheres. The ratio for the radioconcentration was 7.3:1 for PET and 8.2:1 for SPECT. Scans were acquired under typical clinical imaging conditions. The SPECT data were reconstructed using an OSEM algorithm (4) with attenuation and scatter correction based on the CT data. No partial-volume-effect correction or point-spread-function resolution recovery was applied to the SPECT data. Further details of the processing and system calibration can be found in an article by Willowson et al. (8). The PET data were reconstructed using 3-dimensional OSEM, including time-of-flight weighting and point-spread-function resolution recovery. The amount of radioactivity introduced into the phantom in total was approximately 300 MBq for SPECT and 100 MBq for PET. These values, plus the volume of water in the phantom (stored as the patient weight), were entered into the acquisition protocol along with other pertinent information required, for use later in display and analysis. SUV was calculated as the mean of spheric volumes of interest defined by the CT scan for each sphere, to which was applied a threshold of 50% of the maximum value within the volume of interest (SUV50). The results are shown in Table 1.
SUVs for Compartments of IEC Phantom for SPECT and PET
Although the SUV measured in a large background ROI in both cases was within 5% of the expected value of 1.0, both systems suffered from underestimation of SUV50 in some (PET) or all (SPECT) spheres because of the finite spatial resolution of the systems. As noted previously, the SPECT spatial resolution is poorer than PET and thus would be expected to suffer larger underestimation when being used quantitatively in objects less than approximately 3 times the system spatial resolution. This is seen even for the largest (37 mm in diameter) sphere in SPECT, whereas partial-volume effect losses do not become significant (>5% underestimated) in the PET data until the sphere diameters are less than 17 mm. The spatial resolution for this PET system is approximately 4.6 mm isotropic near the central axis. The SPECT reconstructed spatial resolution, on the other hand, is approximately 15 mm in full width at half maximum.
Attenuation and Scatter Correction
It is not the intention of this review to detail the various approaches to scatter correction or attenuation correction in SPECT, as these have largely been discussed previously (9–11); however, the incorporation of both is a necessity for quantitative SPECT reconstruction. The use of CT data for the purpose of attenuation correction in SPECT was reported nearly 30 y ago by Moore (12) and predated the introduction of radionuclide transmission scanning schemes. Attenuation correction can readily be performed after reconstruction in SPECT using the algorithm of Chang (13) modified to use the measured body density (attenuation map) from the CT data, or the correction can be directly included in the iterative reconstruction algorithm. The scatter correction method that we have the most experience with, transmission-dependent scatter correction (14), has been implemented by several groups and found to give accurate results in a range of imaging situations (15–19). The simpler energy-based method known as the triple-energy-window approach (20) has also demonstrated accurate quantification (21) and is now offered by several γ-camera vendors. More sophisticated approaches that model the scatter have also been shown to give excellent results (22–25); however, they often rely on more intensive computing resources and specialized software.
Today, the intimate temporal and spatial integration of CT and emission tomographic devices has enhanced diagnostic accuracy and patient throughput (26–29). To these documented benefits we are now ready to add the ability to perform quantitatively accurate image reconstruction in SPECT using the CT data as the basis for the attenuation and scatter corrections.
Interestingly, the range of radionuclides investigated quantitatively with SPECT is already quite broad, including 99mTc, 111In, 123I, 131I, 177Lu, 186Re, and 201Tl.
Results Demonstrating Quantitative Accuracy in SPECT
Although physicists often use phantoms in controlled experiments to demonstrate and refine the accuracy of image formation, we recognize that the situation when imaging the living human is very different and, hence, the excellent results often obtained in phantom experiments may not be as easy to replicate in humans. Therefore, in this paper we will predominantly discuss published validation work on SPECT studies in humans. For a summary of the accuracy of phantom experimental validation of quantitative SPECT, the reader is referred to Table 1 of the paper by Shcherbinin et al. (30) and Table 2 in the recently published MIRD pamphlet no. 23 on SPECT-based internal radionuclide dosimetry (31). Errors of up to approximately 20% in the estimation of the radioactivity concentration for a range of radionuclides are reported in these papers. As SPECT/CT is the most convenient method for acquiring data suitable for producing quantitative SPECT images today, we will predominantly focus on reports using this multimodality device. In vivo validation of the quantitative accuracy of reconstructed images is challenging in the living human, but there are a limited number of imaging scenarios in which this can be achieved. Several of these are discussed below.
List of Potential Uses for Quantitative SPECT
99mTc
Our group has published 2 papers using 99mTc and SPECT/CT with in vivo validation in the clinical setting. The first demonstrated the accuracy of image reconstruction using 99mTc-macroaggregated albumin in a lung perfusion scan, where it is assumed that close to 100% of the radiopharmaceutical is trapped in the lungs after intravenous injection of a calibrated amount of the radiopharmaceutical (8). This study allowed us to examine the accuracy of the total radioactivity within the images, but not the radioactivity concentration, and found that the total radioactivity in 12 subjects was estimated to be, on average, in error by −1% (range, −7% to +4%). The second clinical validation was in subjects undergoing left ventricular ejection fraction measurements with 99mTc-labeled erythrocytes. The radioconcentration of 99mTc in a peripheral venous whole-blood sample at the time of the SPECT scan was measured in a γ-counter and compared with the concentration of the radiolabeled blood pool in the images reconstructed with CT-based attenuation and scatter correction (32). The accuracy was similar to the previous report, with the average error in estimated radioconcentration being +1.3% and the range being −6.3% to +4.9%. Our scatter correction approach (transmission-dependent scatter correction) uses software that has been developed in house. In yet another in vivo setting, Zeintl et al. have published the accuracy of quantitative 99mTc SPECT measuring the radioconcentration of urine in the bladder of subjects undergoing 99mTc-methylene diphosphate bone scans (33). Their reported average error was +1.1%, similar to what we have reported. Their approach used commercially available reconstruction software with attenuation and scatter correction.
123I
Kim et al. have examined the accuracy of quantitative 123I SPECT using transmission-dependent scatter correction and attenuation correction in the setting of brain imaging, initially in phantoms (16,17). After validating the approach, the same group applied these techniques with 123I-iodoamphetamine for the measurement of regional cerebral blood flow in a multi-institutional setting (34). They measured the accuracy in phantoms and validated the SPECT regional cerebral blood flow results against those obtained with 15O-H2O PET. Across a range of different SPECT cameras, without coacquired CT scans for attenuation or scatter correction, they found a variation of about ±5% in quantitative accuracy in phantoms. However, there was an overall average underestimation of −12%, which they attributed to septal penetration by higher-energy photons and the inability of their attenuation and scatter correction algorithms to estimate photon absorption due to the head holder or scanning couch. They found a slight underestimation in regional cerebral blood flow by iodoamphetamine SPECT, compared with 15O-H2O PET (−6.1 mL⋅100 g−1⋅min−1; r = 0.88). Impressively, their quantitative SPECT methodology has been applied in more than 25,000 patients in more than 130 centers in Japan to date (34).
201Tl
We have investigated the accuracy achieved with 201Tl for the imaging of brain malignancy. Although not able to validate the results in vivo in this situation, testing in an anthropomorphic striatal brain phantom (Radiology Support Devices) using the same methodology as for 99mTc but with adjusted parameters for 201Tl gave results within ±4% of the true values for several different radioconcentrations. This method was subsequently applied to human subjects with suspected recurrent brain malignancies, and a correlation was found between lower SUV and prolonged survival (35). Iida et al. have also used quantitative 201Tl SPECT in dynamic myocardial perfusion imaging to extract the uptake and washout kinetics of the tracer in dogs and compared their results against those for 51Co-microspheres (36). This was one of the first reports of fully quantitative kinetic analysis in SPECT of the myocardium and underlines the potential of new applications for quantitative SPECT.
Other Radionuclides
Several other radionuclides have been used quantitatively in SPECT, although in vivo validation has not been possible. These include 111In-labeled antibodies and tumor-seeking radiopharmaceuticals (37–39), 131I uptake in tumors (40,41), 177Lu for dosimetry calculations in therapeutic applications (42,43), 186Re in palliative bone cancer therapy (44), and even quantitative bremsstrahlung imaging of 90Y (45).
CLINICAL APPLICATIONS OF QUANTITATIVE SPECT
A list of potential uses for quantitative SPECT is presented in Table 2. Few clinical applications of quantitative SPECT exist today because SPECT has generally been developed without routine application of corrections for attenuated and scattered radiation. The major application of attenuation correction in SPECT to date has been in the area of removing attenuation artifacts in SPECT myocardial perfusion imaging (46,47), but the emphasis has not been on quantitative assessment. Likewise, in our institution we routinely apply attenuation correction to all clinical brain, abdominal, and pelvic soft-tissue SPECT (e.g., 67Ga in infection or [123I or 131I]-MIBG), but again this step is taken to mitigate attenuation artifacts or improve image quality rather than to pursue quantitative reconstruction per se.
CHALLENGES FOR IMPLEMENTING QUANTITATIVE SPECT
The evidence included in this review demonstrates that quantitative SPECT is potentially realizable using 99mTc, especially with today’s current multimodality SPECT/CT scanners. The necessary hardware and software already exist to implement quantitative SPECT and achieve reliable results likely to be, in general, within ±10% of the true value in vivo over a wide variety of imaging conditions. The next step toward more widespread implementation is to introduce routine methodology in the SPECT systems to allow them to be calibrated for the specific radionuclide. In PET, all manufacturers provide procedures that allow the calibration factors for quantitative PET to be incorporated into the reconstruction software—calibration factors that are based on measurements of radioactivity using the site’s own local dose calibrator. It is our experience in PET/CT that accuracy testing in a phantom can readily achieve values within ±5% of the true value for the radioactivity concentration of 18F and 68Ga (kBq⋅cm−3). We believe that the equivalent is needed for SPECT—that is, manufacturer-supplied techniques for calibration of the systems, defined operational limits within which quantitative SPECT can be applied, and routine validation of the technique as part of the regular SPECT quality control program.
Several considerations need to be addressed in the calibration process: first, measurements of system sensitivity, which will vary depending on the radionuclide, thickness of the scintillation crystal, collimator, and pulse height analyzer energy windows used; second, definition of any parameters required for the scatter correction algorithm, which will vary depending on the radionuclide and collimator; third, correction of dead-time losses; fourth, calibration of the pixel dimensions to allow scaling from pixels to unit volume (cm3); and fifth, radionuclide half-life.
QUALITY CONTROL FOR SPECT/CT
Quality control for future quantitative SPECT will mirror that required by PET systems today, namely, a regular check of agreement between the dose calibrator and reconstructed SPECT values for radioactivity. Cross-calibration is slightly simpler for PET systems than for SPECT, because in PET all the radiation has the same photon energy and characteristics (namely 2 × 511-keV annihilation photons), independent of the radiotracer, whereas in SPECT different radiotracers—with different photon energies necessitating different collimators, pulse height analyzer energy windows, and other factors—will require separate calibrations and checking. With the cooperation of and implementation by the manufacturers of the SPECT/CT systems, many of the required parameters (such as for scatter correction) can be predefined and fixed for a particular radionuclide/collimator/pulse height analyzer setting. We envisage that strict adherence to the predetermined operating conditions and regular validation will be essential when quantitative SPECT is deployed. At least one example of such a protocol for a multicenter quantitative SPECT trial has been reported (48,49).
CONCLUSION
Although SPECT is an extremely helpful, widely used clinical imaging modality, it will not achieve its full potential when it is used in a purely qualitative manner. We believe that combined SPECT/CT is a game-changer in numerous ways and provides the impetus for a paradigm shift in SPECT use into the quantitative domain in radionuclide emission tomography—a position occupied exclusively by PET until now. As we have demonstrated in this paper, users should also be aware of the deterioration in quantitative accuracy with decreasing object size when objects below 3 times the spatial resolution of the system are imaged. Nevertheless, cooperation between researchers developing the methodology required for quantitative SPECT and manufacturers will allow its wider introduction for clinical use.
In summary, the time for the clinical implementation of quantitative SPECT has come.
Acknowledgments
We are grateful to Professor Hidehiro Iida of the National Cardiovascular Centre Research Institute in Osaka, Japan, for useful discussions and for providing an update on the Japanese brain imaging studies, and we thank our local colleagues for useful suggestions of potential clinical applications for quantitative SPECT.
Footnotes
Learning Objectives: On successful completion of this activity, participants should be able to (1) review the current status of SPECT imaging, with an emphasis on clinical applications for quantitative interpretations; (2) consider the requirements for quantitative SPECT imaging—instrumentation, software, and image calibration; and (3) acquire knowledge of the capabilities of quantitative SPECT with a view to developing new clinical applications.
Financial Disclosure: Dr. Bailey is an employee of NSW Health, University of Sydney, and an investigator for NHMRC, ARC, Cure Cancer Australia. Dr. Willowson is an employee of the University of Sydney and is supported by the Australian Research Council and the NSW Cancer Council in conjunction with the Cure Cancer Australia Foundation. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, participants can access this activity through the SNMMI Web site (http://www.snmmi.org/ce_online) through January 2016.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication September 11, 2012.
- Accepted for publication December 7, 2012.





{kind=link}
Jump to section
Related Articles
Cited By...
- C-X-C Motif Chemokine Receptor 4-Directed Scintigraphy Using [99mTc]Tc-Pentixatec in Primary Aldosteronism: A Proof-of-Concept Study
- Accuracy Assessment of SUV Measurements in SPECT/CT: A Phantom Study
- Optimization of Number of Iterations as a Reconstruction Parameter in Bone SPECT Imaging Using a Novel Thoracic Spine Phantom
- Multicenter Study of Quantitative SPECT: Reproducibility of 99mTc Quantitation Using a Conjugated-Gradient Minimization Reconstruction Algorithm
- Absolute Quantitation of Cardiac 99mTc-Pyrophosphate Using Cadmium-Zinc-Telluride-Based SPECT/CT
- Radiomics Analysis of Clinical Myocardial Perfusion Stress SPECT Images to Identify Coronary Artery Calcification
- The Prognostic Value of Quantitative Bone SPECT/CT Before 223Ra Treatment in Metastatic Castration-Resistant Prostate Cancer
- Digital Solid-State SPECT/CT Quantitation of Absolute 177Lu Radiotracer Concentration: In Vivo and In Vitro Validation
- Quantitative Bone-Avid Tracer SPECT/CT for Cardiac Amyloidosis: A Crucial Step Forward
- Intra- and Interobserver Agreement of SUV SPECT Quantitative SPECT/CT Processing Software, Applied in Clinical Settings for Patients with Solid Renal Tumors
- A Review of Magnetic Particle Imaging and Perspectives on Neuroimaging
- A Prospective Study of Quantitative SPECT/CT for Evaluation of Lung Shunt Fraction Before SIRT of Liver Tumors
- Harnessing the Power of Molecular Imaging for Precision Medicine
- Repeatability of Radiotracer Uptake in Normal Abdominal Organs with 111In-Pentetreotide Quantitative SPECT/CT