


Abstract
The aim of this study was to examine the prevalence, distribution, and topographic relationship of vascular 18F-sodium fluoride uptake and arterial calcification in major arteries. Methods: Image data obtained from 75 patients undergoing whole-body 18F-sodium fluoride PET/CT were evaluated retrospectively. Arterial radiotracer uptake and calcification were analyzed qualitatively and semiquantitatively. Results: 18F-sodium fluoride uptake was observed at 254 sites in 57 (76%) of the 75 study patients, and calcification was observed at 1,930 sites in 63 (84%) of the patients. Colocalization of radiotracer accumulation and calcification could be observed in 223 areas of uptake (88%). However, only 12% of all arterial calcification sites showed increased radiotracer uptake. Conclusion: Our data indicate the feasibility of 18F-sodium fluoride PET/CT for the imaging of mineral deposition in arterial wall alterations. 18F-sodium fluoride PET/CT may provide relevant information about the morphologic and functional properties of calcified plaque.
The formation and progression of atherosclerotic plaque are dynamic processes involving multiple pathophysiologic mechanisms, including inflammation, apoptosis, necrosis, and calcification. The composition and inflammatory state of plaque determine its stability and, therefore, the risk of clinical events (1–4).
Vascular calcification is a common phenomenon and possibly the most prominent feature of atherosclerosis (1,5). There is accumulating evidence that calcification in atherosclerotic plaque is an active, complex process exhibiting remarkable similarities to the formation of new bone (1,6). Cell types, signaling pathways, and metabolic compounds participating in bone formation have been found to be associated with plaque and arterial calcification (6–9). Pathologic mineralization can also occur through passive precipitation if physiologic inhibitors are no longer able to prevent mineral deposition (10).
Morphologic imaging techniques mainly provide information about structural aspects of calcified atherosclerotic lesions, such as the extent of plaque and the degree of stenosis, but fail to identify active calcification of plaque (11). For the reasons mentioned earlier, we postulated that 18F-sodium fluoride PET/CT may have the potential to visualize ongoing mineral deposition in atherosclerotic plaque.
Therefore, the purpose of the present study was to assess the prevalence, location, and relationship of increased 18F-sodium fluoride uptake and arterial calcifications and lesions.
MATERIALS AND METHODS
Study Population
From all subjects for whom whole-body 18F-sodium fluoride PET/CT had been performed for the exclusion of bone metastases at the University Medical Center Hamburg-Eppendorf between December 2008 and July 2009, subjects were selected according to the following criteria. For inclusion, whole-body image data had to be digitally available for retrospective analysis. Subjects with systemic inflammatory disease, a history of vasculitis, a cardiovascular event in the preceding 3 mo, or chemotherapy in the preceding 2 mo were excluded. On the basis of these criteria, 75 subjects were included. Treatment with statins was recorded for all patients (12). A history of cardiovascular events (myocardial infarction or cerebrovascular insult) was obtained for every patient. All subjects had given written informed consent for the retrospective evaluation of their data.
Image Acquisition and Reconstruction
PET and CT were performed with a PET/CT hybrid system (Gemini GXL 10; Philips). 18F-sodium fluoride was injected intravenously at a dose of 350 ± 50 MBq. During the 60-min uptake period, patients were hydrated orally with water. Imaging started with nonenhanced, low-dose CT of the whole body (120 kV, 80 mA). Next, PET of the whole body was performed for 90 s per bed position at the head and thorax and 60 s at the legs. Overlap between consecutive bed positions was 50%. Transverse PET slices were reconstructed into a 144 × 144 matrix with the iterative 3D line-of-response reconstruction algorithm of the system software. The low-dose CT was used for PET attenuation correction. The voxel size was 4 × 4 × 4 mm. The spatial resolution in the reconstructed PET images was about 8 mm in full width at half maximum.
Image Analysis
PET, CT, and PET/CT fusion images were evaluated both visually and semiquantitatively with the Extended Brilliance Workstation of the PET/CT system. The analysis was performed on the basis of lesions and on the basis of arterial segments. For the segment-based analysis, the major arteries were subdivided as follows: right and left common carotid arteries, ascending aorta, aortic arch, descending thoracic aorta, abdominal aorta, right and left iliac arteries, and right and left femoral arteries.
CT images were evaluated visually for the presence of abnormal sites of vascular calcification, defined as high-density mural areas. Each lesion was classified with scores on a scale for grading circumferential extent: 0, absent; 1, less than 25% of arterial wall circumference; 2, 25%−50% of arterial wall circumference; 3, 50%−75% of arterial wall circumference; and 4, greater than 75% of arterial wall circumference.
An arterial segment was categorized as having CT-positive results (CT+) if at least one calcified lesion was detected in it; otherwise, it was categorized as having CT-negative results (CT−). A CT+ segment was further classified with the maximum lesion score among all lesions in that segment.
Both attenuation-corrected and non–attenuation-corrected PET images were visually evaluated for focal lesions of increased radiotracer uptake. The locations of these areas in relation to the vascular wall and to calcification detected by CT were determined from PET/CT fusion images. A lesion was excluded from the analysis if it was suspected of being an artifact caused by spatial mismatching of PET and CT (physiologic organ or patient motion) or by activity spillover from extravascular structures. Semiquantitative analysis was performed by obtaining the maximum standardized uptake value (SUVmax). For focal lesions, an individual region of interest was placed around the atherosclerotic plaque. For linear lesions, SUVmaxs were obtained from 4 representative, nonadjacent slices and then averaged. An arterial segment was categorized as having PET-positive results (PET+) if at least one PET lesion was detected in it.
Statistical Analysis
The prevalences of vascular calcification on CT images and increased vascular wall radiotracer uptake on PET images were calculated. The presence and locations of radiotracer uptake and calcification on CT images were tested for association with the patients' clinical characteristics and abnormal vascular findings. Continuous variables were analyzed with the Student t test (2-sided) for unpaired data. For categoric data, P values were computed from contingency tables with the Fisher exact test. Statistical significance was established for P values of less than 0.05.
RESULTS
Patient Characteristics
The 75 recruited patients were 65.2 ± 12.3 (mean ± SD) y old and included 48 women. Nine patients had a history of previous cardiovascular events. Eight patients were receiving statins. The patients were clinically stable and asymptomatic when imaged.
Arterial Wall 18F-Sodium Fluoride Uptake and Calcification
Arterial wall 18F-sodium fluoride uptake was observed at 254 sites in 57 (76%) of the 75 study patients (Table 1). The prevalence was highest in the femoral arteries, followed by the abdominal aorta and thoracic aorta. SUVmaxs ranged from 0.8 to 3.6. All sites of 18F-sodium fluoride uptake were seen on both uncorrected and CT-based attenuation-corrected PET images.
Prevalence, Distribution, and Intensity (SUVmax) of 18F-Sodium Fluoride Uptake
Calcification was seen at 1,930 sites in 63 (84%) of the 75 study patients (Table 2). The prevalence of calcification was highest in the abdominal aorta, followed by the femoral and iliac arteries. The prevalence of 18F-sodium fluoride accumulation was statistically significantly higher in lesions with extensive calcification than in those with only minor mineral deposition (the P value for CT calcification scores of 1 vs. 4 was <0.0001). No statistically significant association between intensity of radiotracer accumulation (SUVmax) and calcification score was found (P = 0.71). For 10 patients (13%), no arterial wall lesions were visualized by either PET or CT. Compared with the PET+ study population, these patients were significantly younger (53.4 ± 12.3 y vs. 69.1 ± 9.8 y; P < 0.0001).
Prevalence, Distribution, and Extent of Calcification in Studied Arterial Walls
No statistically significant correlation was found between prior administration of statins and the presence of vascular 18F-sodium fluoride uptake (P = 0.39) or calcification (P = 0.34). The frequency of arterial calcification was higher in men (93%) than in women (79%) without reaching statistical significance (P = 0.19). The group of patients with vascular radiotracer uptake included more men (85%) than women (71%) without reaching statistical significance (P = 0.26). The presence of both vascular tracer accumulation and calcification was significantly associated with age (P < 0.0001). In all patients with a history of cardiovascular events, at least one site of increased 18F-sodium fluoride uptake was observed (100% vs. 76% of the entire study population; P = 0.10).
Relationship Between 18F-Sodium Fluoride Uptake and Calcification
Of the 600 total segments, 180 (30%) were PET+ and CT+, 160 (∼27%) were PET negative (PET−) and CT+, 10 (∼2%) were PET+ and CT−, and 250 (∼42%) were PET− and CT−. The presence of arterial radiotracer accumulation was strongly associated with calcification within the vessel wall in these segments (P < 0.0001).
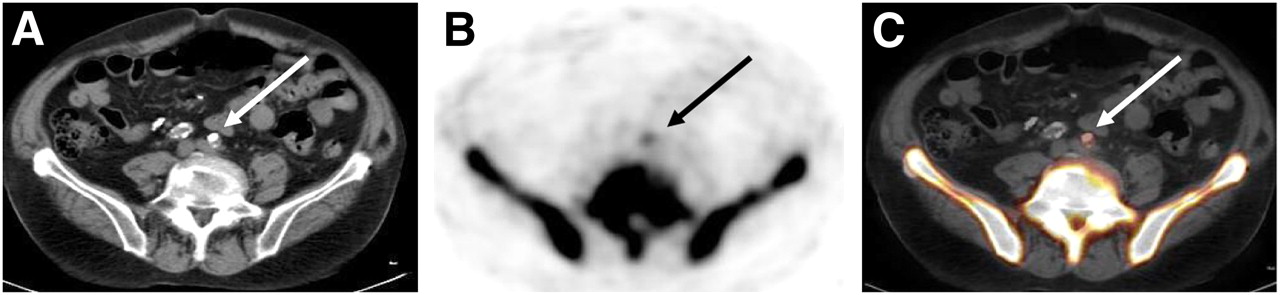
When the spatial correlation between vascular 18F-sodium fluoride uptake and calcification sites in the studied arterial segments was analyzed on a per-lesion basis, only 31 (12%) of the 254 lesions with marked arterial wall 18F-sodium fluoride uptake did not show concordant calcification. For the remaining 223 lesions with uptake (88%), a correspondence of radiotracer accumulation and calcification was observed. However, only these 223 (12%) of the 1,930 total calcification sites showed prominent 18F-sodium fluoride uptake in at least some part of the calcified plaque. Examples of arterial wall calcification coincident with 18F-sodium fluoride uptake are shown in Figures 1 and 2.
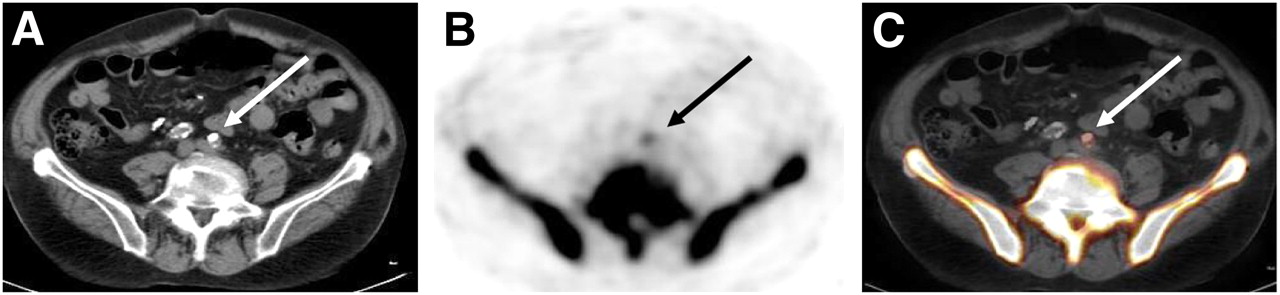
Transaxial 18F-sodium fluoride PET/CT images of common iliac arteries in 67-y-old man. (A) CT image. (B) PET image. (C) Fused PET/CT image. 18F-sodium fluoride accumulation in atherosclerotic lesion was colocalized with calcification. Arrows indicate calcified lesion.

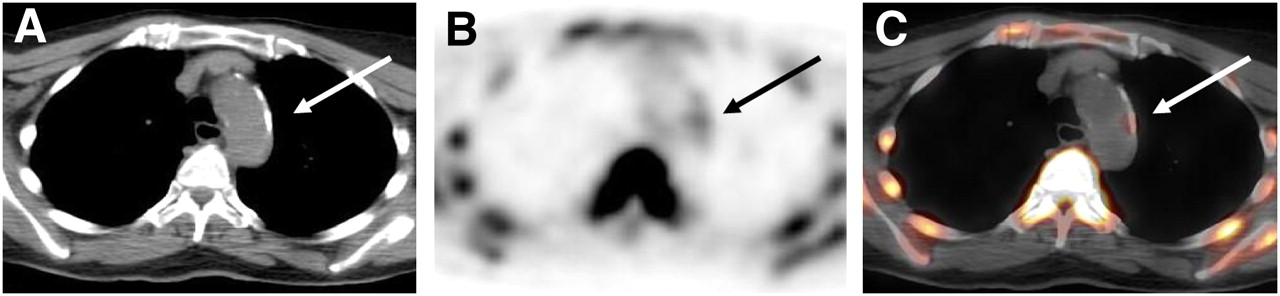
Transaxial 18F-sodium fluoride PET/CT images of aortic arch in 76-y-old woman. (A) CT image. (B) PET image. (C) Fused PET/CT image. 18F-sodium fluoride uptake in atherosclerotic lesion coincided with calcification. Arrows indicate calcified lesion.
DISCUSSION
Our results indicate the feasibility of using 18F-sodium fluoride for the in vivo functional imaging of atherosclerotic lesions. The arterial wall 18F-sodium fluoride distribution was consistent with established atherosclerotic topography, with increased uptake in the thoracic aorta and at the carotid bifurcation.
Both active and passive mechanisms of calcium deposition may explain arterial calcification. Plaque mineralization may be caused by passive calcium precipitation associated with areas of advanced tissue degeneration or necrosis, which can frequently be observed in advanced atherosclerotic lesions (1,10). There is growing evidence that plaque calcification is an active process akin to bone formation. Atheromatous lesions and fibrocalcific plaques express proteins and possess cell types (i.e., chondrocytes, osteoblasts, and osteoclasts) and signaling pathways normally associated with bone and may contain bonelike tissues (6–9). Although the precise mechanism of 18F-sodium fluoride uptake is not fully known yet, one may assume that it indicates ongoing active mineral deposition in atherosclerotic lesions. Plaques still accumulating 18F-sodium fluoride might not represent stable, nonprogressive stages of disease.
With regard to the colocalization of tracer accumulation and calcification sites, the results of the present study differ substantially from the findings of studies of other tracers, such as 18F-FDG (13–15). Although existing studies are difficult to compare because of differences in inclusion criteria, in the portion of the arterial vasculature evaluated, and in data analysis, most of them reported no colocalization of radiotracer uptake and calcification. Using 18F-FDG, Dunphy et al. (14) and Ben-Haim et al. (15) found colocalization in less than 2% of cases and in 7% of sites, respectively. Bucerius et al. (16) observed no 18F-fluoromethylcholine uptake in completely calcified lesions, and Kato et al. (17) found 11C-choline uptake in less than 1% of calcification sites. In the present study, the correlation of radiotracer uptake and arterial wall calcification indicated that 88% of the lesions with 18F-sodium fluoride uptake showed concordant calcification. Unlike 18F-FDG or choline derivatives, 18F-sodium fluoride may provide new insights into the functional properties of calcified lesions.
The present study had some limitations. First, the lack of synchronization of PET image acquisition with both the cardiac cycle and the spontaneous respiration rate might have affected the visualization of arterial uptake, particularly with regard to the coronary arteries, the ascending aorta, and the aortic arch (18). Second, dynamic and delayed data could provide relevant additional information regarding the nature of arterial radiotracer uptake (19,20). Third, the limited spatial resolution of PET renders images subject to partial-volume effects, which might lead to an underestimation of tracer accumulation in atherosclerotic plaque, especially in smaller arteries. Finally, because of the retrospective nature of the present study, histologic evaluation of the detected plaque could not be performed. Therefore, data concerning the structure, exact composition, and stability of the atherosclerotic lesions are not available. Further prospective studies are needed to determine the prognostic value of tracer uptake and to determine whether it might effectively target therapeutic interventions to influence clinical outcomes.
CONCLUSION
We demonstrated the feasibility of using 18F-sodium fluoride for the imaging of arterial wall alterations. 18F-sodium fluoride PET/CT may provide relevant additional information regarding plaque physiology.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 21, 2010.
- Accepted for publication March 26, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-NaF Uptake on Vascular PET Imaging in Symptomatic versus Asymptomatic Atherosclerotic Disease: a Meta-Analysis
- Vascular Calcification: The Evolving Relationship of Vascular Calcification to Major Acute Coronary Events
- 18F-Fluoride Positron Emission Tomographic Imaging of Penile Arteries and Erectile Dysfunction
- Three-Hour Delayed Imaging Improves Assessment of Coronary 18F-Sodium Fluoride PET
- The Role of Imaging in Measuring Disease Progression and Assessing Novel Therapies in Aortic Stenosis
- Imaging Cardiovascular Calcification
- Clinical Molecular Imaging of Chemokine Receptor CXCR4 Expression in Atherosclerotic Plaque Using 68Ga-Pentixafor PET: Correlation with Cardiovascular Risk Factors and Calcified Plaque Burden
- Clinical Relevance of 18F-Sodium Fluoride Positron-Emission Tomography in Noninvasive Identification of High-Risk Plaque in Patients With Coronary Artery Disease
- 18F-Fluoride Imaging and Other Plaque-Seeking Diagnostic Strategies: Understanding the Reality and Setting the Ground Rules...
- Association Between Osteogenesis and Inflammation During the Progression of Calcified Plaque Evaluated by 18F-Fluoride and 18F-FDG
- Coronary Artery Calcification: From Mechanism to Molecular Imaging
- Evaluation of 68Ga-Glutamate Carboxypeptidase II Ligand Positron Emission Tomography for Clinical Molecular Imaging of Atherosclerotic Plaque Neovascularization
- Noninvasive Molecular Imaging of Disease Activity in Atherosclerosis
- The vulnerable atherosclerotic plaque: in vivo identification and potential therapeutic avenues
- Impact of Personal Characteristics and Technical Factors on Quantification of Sodium 18F-Fluoride Uptake in Human Arteries: Prospective Evaluation of Healthy Subjects
- Radiotracer Imaging of Peripheral Vascular Disease
- 18F-NaF Uptake by Atherosclerotic Plaque on PET/CT Imaging: Inverse Correlation Between Calcification Density and Mineral Metabolic Activity
- 18F-Sodium Fluoride Uptake Is a Marker of Active Calcification and Disease Progression in Patients With Aortic Stenosis
- Radiotracer Imaging of Peripheral Vascular Disease
- Coronary Arterial 18F-Sodium Fluoride Uptake: A Novel Marker of Plaque Biology
- Assessment of Valvular Calcification and Inflammation by Positron Emission Tomography in Patients With Aortic Stenosis
- Feasibility of 11C-Acetate PET/CT for Imaging of Fatty Acid Synthesis in the Atherosclerotic Vessel Wall
- Correlation of Inflammation Assessed by 18F-FDG PET, Active Mineral Deposition Assessed by 18F-Fluoride PET, and Vascular Calcification in Atherosclerotic Plaque: A Dual-Tracer PET/CT Study
- In Vivo Imaging of Mineral Deposition in Carotid Plaque Using 18F-Sodium Fluoride PET/CT: Correlation with Atherogenic Risk Factors