


Abstract
18F-FDG PET may assist decision making in ischemic cardiomyopathy. The PET and Recovery Following Revascularization (PARR 2) trial demonstrated a trend toward beneficial outcomes with PET-assisted management. The substudy of PARR 2 that we call Ottawa-FIVE, described here, was a post hoc analysis to determine the benefit of PET in a center with experience, ready access to 18F-FDG, and integration with clinical teams. Methods: Included were patients with left ventricular dysfunction and suspected coronary artery disease being considered for revascularization. The patients had been randomized in PARR 2 to PET-assisted management (group 1) or standard care (group 2) and had been enrolled in Ottawa after August 1, 2002 (the date that on-site 18F-FDG was initiated) (n = 111). The primary outcome was the composite endpoint of cardiac death, myocardial infarction, or cardiac rehospitalization within 1 y. Data were compared with the rest of PARR 2 (PET-assisted management [group 3] or standard care [group 4]). Results: In the Ottawa-FIVE subgroup of PARR 2, the cumulative proportion of patients experiencing the composite event was 19% (group 1), versus 41% (group 2). Multivariable Cox proportional hazards regression showed a benefit for the PET-assisted strategy (hazard ratio, 0.34; 95% confidence interval, 0.16–0.72; P = 0.005). Compared with other patients in PARR 2, Ottawa-FIVE patients had a lower ejection fraction (25% ± 7% vs. 27% ± 8%, P = 0.04), were more often female (24% vs. 13%, P = 0.006), tended to be older (64 ± 10 y vs. 62 ± 10 y, P = 0.07), and had less previous coronary artery bypass grafting (13% vs. 21%, P = 0.07). For patients in the rest of PARR 2, there was no significant difference in events between groups 3 and 4. The observed effect of 18F-FDG PET–assisted management in the 4 groups in the context of adjusted survival curves demonstrated a significant interaction (P = 0.016). Comparisons of the 2 arms in Ottawa-FIVE to the 2 arms in the rest of PARR 2 demonstrated a trend toward significance (standard care, P = 0.145; PET-assisted management, P = 0.057). Conclusion: In this post hoc group analysis, a significant reduction in cardiac events was observed in patients with 18F-FDG PET–assisted management, compared with patients who received standard care. The results suggest that outcome may be benefited using 18F-FDG PET in an experienced center with ready access to 18F-FDG and integration with imaging, heart failure, and revascularization teams.
Coronary revascularization may be beneficial for patients with ischemic cardiomyopathy; however, there are significant perioperative risks (1–3). 18F-FDG PET has been shown to be the most sensitive noninvasive means for the prediction of left ventricular functional recovery after coronary revascularization (4).
Observational studies have suggested that 18F-FDG PET can help identify patients at high risk for cardiac events (4–14). The randomized controlled PET and Recovery Following Revascularization (PARR 2) trial demonstrated a trend toward reduction of cardiac events with 18F-FDG PET–assisted decision making, compared with standard care, but overall was inconclusive regarding the primary outcome (15).
Gould noted several factors that may bias randomized trials (16). With the PARR 2 study, although imaging acquisition and interpretation were standardized, access to 18F-FDG, prior experience performing and using 18F-FDG PET, and integrating 18F-FDG PET into clinical practice were variable. Prompted by these factors, as well as new drug submission requirements of Health Canada to provide data on 18F-FDG produced in Ottawa, we undertook a post hoc substudy of PARR 2.
The hypothesis of this post hoc substudy was that management assisted by 18F-FDG PET achieves a better clinical outcome than standard care without 18F-FDG PET at a site with (1) ready access to 18F-FDG; (2) expertise; and integration between the (3) imaging, (4) heart failure, and (5) revascularization teams, in patients with severe left ventricular dysfunction and suspected coronary artery disease. We call this substudy Ottawa-FIVE: 18F-FDG PET Imaging of Myocardial Viability in an Experienced Center with Access to 18F-FDG and Integration with Clinical Management Teams. FIVE also refers to the 5 key elements enumerated above.
MATERIALS AND METHODS
Patients
Included in this post hoc substudy were PARR 2 patients (15) recruited at the University of Ottawa Heart Institute after August 1, 2002. This is the date on which local 18F-FDG production was commenced. Thus, patients in the Ottawa-FIVE subgroup met the PARR 2 enrollment criteria: that is, they were patients being considered for revascularization or revascularization work-up, transplantation work-up, or heart failure workup, or they were patients for whom 18F-FDG PET viability imaging might be considered useful by the attending physician for decision making and who met other inclusion criteria. Eligible patients were included in PARR 2 if they were older than 18 y; had an ejection fraction of 35% as documented by radionuclide angiography, left ventricular angiography, or echocardiography; had known or highly suspected coronary artery disease based on coronary angiography; had previous revascularization; had a previous myocardial infarction verified by chart review; or had stress perfusion imaging positive for scarring with or without ischemia based on a clinical imaging report of a defect described as at least moderate and fixed or reversible, respectively. Patients were not enrolled in PARR 2 (or included in the Ottawa-FIVE post hoc subgroup analysis) if they met one or more exclusion criteria for PARR 2: that is, patients in whom a therapy decision had already been determined such that the attending physician would in no way alter management based on any potential viability imaging findings, who had already had 18F-FDG viability imaging, who had comorbidities that would likely affect survival over the study duration, who had experienced a myocardial infarction less than 4 wk previously, who had already been identified to be unsuitable for revascularization, who required emergency revascularization, who had severe valvular disease that required surgery, who were geographically inaccessible, or for whom informed consent could not be obtained. Patients in the Ottawa-FIVE subgroup were randomized in PARR 2 to 18F-FDG PET–assisted management (group 1) or standard care (group 2).
Imaging
Patients underwent radionuclide angiography at baseline. Radionuclide angiography was performed using a standard electrocardiogram-gated equilibrium 99mTc-red blood cell blood-pool imaging protocol. The ejection fraction was measured from the left anterior oblique 45° acquisition. Nongated PET perfusion imaging was acquired at rest with a standard protocol using 82Rb or 13N-ammonia as described previously (15,17,18). For 18F-FDG imaging, nondiabetic patients were studied after an oral glucose load, whereas an insulin-euglycemic clamp was used for those with diabetes (5,15,18,19). Full details of PET protocols are provided elsewhere (5,15,18,19).
PET Data Analysis and Interpretation
An automated method of image analysis (myoPC; University of Ottawa Heart Institute) was applied to the perfusion/18F-FDG PET data to yield quantified measures of the extent and severity of scarring and mismatch as previously described (15,17,18). These parameters were included with clinical parameters in a previously derived model that yielded a point estimate and 95% confidence interval for predicted left ventricular function recovery after revascularization (15,17). Patients were classified as having a low, moderate, or high likelihood of recovery, if adequate revascularization could be achieved. The likelihood of recovery was considered low when the upper confidence limit of the predicted ejection fraction change was 3% or less; the likelihood was considered high when the lower confidence limit for predicted change was above 3%; and the likelihood was considered moderate for those with confidence limits between the high and low cut-points (15,17). Physicians experienced in reading PET data also reviewed the images to confirm the model's classification of the likelihood of recovery. Physicians considered the extent of scarring and mismatch in their interpretation. Differences between the model and the interpreting physician were settled by consensus with another experienced imaging physician. A report detailing the extent of viable myocardium as a percentage of the left ventricle, and the likelihood for recovery, was delivered to the attending physician or surgeon. The physician or surgeon then decided whether to proceed with revascularization (or revascularization work-up in those without recent angiography).
18F-FDG PET–Assisted Management Arm
When 18F-FDG PET identified significant viable myocardium, revascularization or revascularization work-up was recommended depending on whether the patient had undergone recent angiography. When PET identified predominantly scar tissue, no revascularization was the recommendation. Once the PET report was available, the physician or surgeon considered the imaging data in the context of the individual patient and decided whether to proceed with revascularization or revascularization work-up.
Standard Care Arm
Standard care proceeded without 18F-FDG PET being available to the physician. An alternative test for viability definition could be considered.
We were aware that some patients could have vessels unsuitable for revascularization. Such patients who were identified before recruitment were excluded from enrollment. Patients who were directed to undergo angiography but were subsequently considered to have unsuitable anatomy continued to be followed in their respective arms on an intention-to-treat basis. For both arms, once initial testing and evaluation were completed, the physician or surgeon would then consider the imaging data in the context of the individual patient and decide whether to proceed with revascularization (or revascularization work-up in those without recent angiography). The management plans were reviewed and recorded at 8 wk after randomization. Revascularizations directed by initial work-up (with or without PET) were considered protocol revascularizations. Their associated hospital stays were not counted as events.
Cardiac Event Variable Definitions and Measurement
The primary event of interest was the occurrence of any of the following within 1 y of randomization: cardiac death, myocardial infarction, or nonelective hospitalization due to a cardiac cause such as unstable angina or heart failure. Events were assessed by telephone interview every 3 mo and are based on the best available data as of January 2009. All events were reviewed and verified by an adjudication committee unaware of the treatment allocation scheme. The definition of each variable and the timing of its measurement have been described previously (15,17). Cause of death was determined from the death certificate and included death presumed to be tachyarrhythmic or death from other cardiac cause. Specific definitions of cardiac death and nonfatal myocardial infarction have been previously described (15,17).
Cardiac hospitalization was defined as hospitalization due to a cardiac cause such as unstable angina, worsening heart failure, or nonprotocol revascularization and was at the discretion of the attending physician (15,17). Elective admissions for procedures such as implantation of a cardioverter–defibrillator for primary prevention were not counted as events. Hospitalizations were reviewed and verified by an adjudication committee as cardiac versus noncardiac hospitalization.
Statistical Analysis
This analysis is considered a post hoc subgroup analysis because it was not prespecified in the protocol. Even though the direct access to 18F-FDG occurred partway through the study (August 1, 2002), the randomization process ensures that the substudy patients were equally likely to be assigned to either arm. Continuous measures are presented as means ± SD. Wilcoxon rank sum testing for independent samples was performed to identify any significant differences between groups. Categoric measures are presented as frequencies with percentages. The Fisher exact test was used for comparisons between groups. Because the primary objective of this substudy was to determine whether the Ottawa-FIVE group, compared with the standard care group, gained significant benefit from 18F-FDG PET–guided therapy, multivariable Cox proportional hazards models of primary outcome were used to assess the independent prognostic value of the 18F-FDG PET–guided therapy, and the Ottawa-FIVE subgroup including the 2-way interaction. The whole PARR 2 population was used for the modeling with the interaction—the appropriate way to show evidence of a different treatment effect in the Ottawa-FIVE group, compared with the rest of the PARR 2 treatment effect. The 2 separate subgroup analyses may show different effects of the treatment within each group, but the interaction test is needed to show that any group effects are significantly different from each other (20). To prevent overfitting of the multivariable Cox proportional hazards model, only baseline characteristics included in Tables 1 and 2 with P values less than 0.20 based on univariable Cox proportional hazards models of primary outcome in the overall PARR 2 population were considered (i.e., creatinine, ejection fraction, prior coronary artery bypass grafting, age, sex, diabetes, angina, and dyspnea). With the use of stepwise selection methods, these were added to control for confounding, resulting in the final model given in Table 1. Because the model with the interaction requires the full population of PARR 2, there is an inherent power advantage. Hazard ratios for the subgroup comparisons were created using the appropriate contrasts (i.e., various specifications of the level of the first 3 variables) in the final model. A P value of less than 0.05 was considered statistically significant. Statistical calculations were performed using SAS software (SAS Institute Inc.).
Multivariable Cox Proportional Hazards Model for Subgroup Analysis of Primary Outcome for PARR 2
RESULTS
Ottawa-FIVE Baseline Characteristics
There were 111 patients, with 56 randomized to the PET arm and 55 to the standard arm (Table 2). Two patients in the PET arm dropped out. Thus, complete follow-up was available in 109 (98%) of 111 patients. There were no statistically significant differences in baseline parameters between the groups. Three patients (2 in the PET arm and 1 in the standard arm) with left ventricular dysfunction who initially seemed to meet the inclusion criteria were found to have an ejection fraction greater than 0.35 on the radionuclide ventriculography done at the time of enrollment. Although these patients were randomized inappropriately, they were followed and included in the intention-to-treat analysis.
Baseline Characteristics
Ottawa-FIVE PET Viability and Revascularization
In the PET arm 55 patients underwent PET. The PET image quality was considered good in all cases except one (fair quality); 19, 21, and 15 patients had large, medium, and small amounts of viable myocardium, respectively. Twenty-five patients (45%) underwent protocol revascularization (22 coronary artery bypass grafting and 3 percutaneous coronary intervention). No late revascularizations were performed in this group. In the standard arm, 24 patients (44%) underwent protocol revascularization (17, coronary artery bypass grafting; 7, percutaneous coronary intervention). Three patients underwent late revascularization in this group.
During PARR 2, 10 patients in the Ottawa-FIVE population underwent implantable cardioverter–defibrillator insertion (5 in the PET arm and 5 in the standard arm). During the trial, the American College of Cardiology and American Heart Association published guidelines that recommended implantation of a cardioverter–defibrillator for primary prevention in severe left ventricular dysfunction (21). Therefore, a recommendation was sent to the attending physicians of enrolled patients to consider device therapy if the patient met appropriate criteria.
Ottawa-FIVE Coronary Anatomy
Among the 82 patients with recent (pre- or postrandomization) angiography available for review, 75 (91%) had 2-vessel, 3-vessel, or left main disease with 50% stenoses: 39 (91%) of 43 patients in the PET arm, compared with 36 (92%) of 39 patients in the standard arm (P = not statistically significant). Distal stenosis of 50% in at least 2 distal segments was reported in 12 PET arm patients (28%) and 11 standard arm patients (28%) (P = not statistically significant). Distal disease in the left anterior descending coronary artery was reported in 7 PET arm patients (16%) with angiography and 5 standard arm patients (13%) with angiography (P = not statistically significant). A small number of patients (4, or 4.9%) did not have a significant stenosis at the time of the postrandomization angiogram despite meeting 1 or more inclusion criteria (3 patients in the PET arm and 1 in the standard arm). This rate was similar to that in the main PARR 2 trial (3.3%). As with PARR 2, because our goal was to determine the added value of 18F-FDG PET among patients being assessed for viability and these patients had been referred for such, and because these patients met the inclusion criteria set and had been randomized, these patients were included in this intention-to-treat analysis. Other testing included stress or viability testing in the 3 mo before randomization in 25 patients in the PET arm and 25 patients in the standard arm. Thirty patients in the standard arm also had testing after randomization. A total of 43 patients had at least 1 stress or viability imaging test in the standard arm.
Ottawa-FIVE Outcomes
There is an interaction between 18F-FDG PET–guided therapy and the Ottawa-FIVE subgroup indicator in the multivariable Cox proportional hazards model such that there was a statistically significant effect on the primary outcome (P = 0.016). In this adjusted model, other independent predictors of outcome were left ventricular ejection fraction, sex, serum creatinine, and prior coronary bypass grafting (Table 1). Even after these parameters had been added to the model, the interaction of 18F-FDG PET–guided therapy and the Ottawa-FIVE subgroup was still statistically significant. If the patients with an ejection fraction of more than 35% on radionuclide ventriculography at the time of enrollment are excluded, the interaction is still significant (P = 0.02).
Ottawa-FIVE Cardiac Events
Thirty-two first events were identified. Among first events, 6 were cardiac deaths, 4 were myocardial infarctions, and 22 were cardiac hospitalizations. Ten patients (19%) experienced the composite events in the PET arm, compared with 22 (41%) in the standard arm. The unadjusted and adjusted hazard ratios for the composite event in the PET arm (group 1), compared with the standard arm (group 2), were 0.37 (95% confidence interval, 0.17–0.78; P = 0.009) and 0.34 (95% confidence interval, 0.16–0.72; P = 0.005), respectively (Fig. 1A). Overall, in total, there were 4 cardiac deaths (7.5%) in the PET arm and 8 (14.8%) in the standard arm. The study was not powered to compare mortality in the 2 arms. There were 2 noncardiac deaths, 1 in the PET arm and 1 in the standard arm.
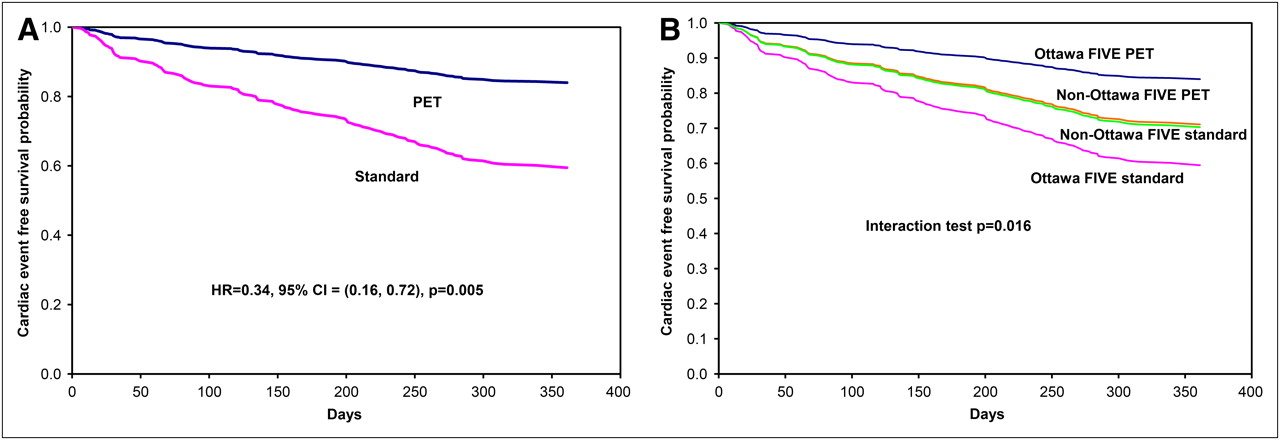
(A) Adjusted survival curves for PET and standard arms in Ottawa-FIVE substudy. (B) Adjusted survival curves for PET and standard arms in Ottawa-FIVE and rest of PARR 2. CI = confidence interval; HR = hazard ratio.
Comparison of Ottawa-FIVE to the Rest of PARR 2
Compared with other patients in PARR 2, the Ottawa-FIVE population had lower baseline left ventricular ejection fraction (25% vs. 27%, P = 0.04) and a greater proportion of women (24% vs. 13%, P = 0.006). The Ottawa-FIVE population also tended to be older (64 ± 10 y vs. 62 ± 10 y, P = 0.07) and to have less prior coronary bypass grafting (13% vs. 21%, P = 0.07) than the rest of the PARR 2 population (Table 3). At 1 y, among the patients in the rest of PARR 2, there was no significant difference between the rate of the composite primary outcome events in the PET arm (group 3) and the standard arm (group 4) (adjusted model hazard ratio, 0.97; 95% confidence interval, 0.64–1.47; P = 0.879). This result is in contrast to the Ottawa-FIVE substudy groups, in which a significant difference was observed. Figure 1B illustrates the observed effect of 18F-FDG PET–guided therapy in the 4 subgroups in the context of adjusted survival curves from the Cox model (interaction test, P = 0.016). The comparisons of the PET and standard arms of Ottawa-FIVE to those similar arms in the rest of PARR 2 demonstrated a trend toward statistical significance (standard arms [group 2 vs. 4]: adjusted hazard ratio, 1.48; 95% confidence interval, 0.87–2.49; P = 0.145; PET arms [group 1 vs. 3]: hazard ratio, 0.51; 95% confidence interval, 0.26–1.02; P = 0.057).
Comparison of Baseline Characteristics of Ottawa-FIVE Patients with Remainder of PARR 2 Patients
DISCUSSION
This post hoc subgroup analysis of the PARR 2 trial suggests that in an experienced center with ready access to 18F-FDG, management assisted by PET may lead to an improvement in clinical outcomes, measured by a reduction in the composite clinical endpoint at 1 y, compared with standard care. These findings were associated with trends toward both an event reduction in the 18F-FDG PET arm and an event increase in the standard arm in the Ottawa-FIVE subgroups, compared with other patients in PARR 2 (although this comparison did not reach statistical significance). Ottawa-FIVE patients were more often female, had a slightly lower ejection fraction, tended to be older, and tended to have less previous coronary artery bypass grafting. Previous observational studies have suggested that patients at high risk of cardiac events can be identified using 18F-FDG PET to define hibernating viable myocardium (4–14). However, these studies were not randomized and could not determine whether clinical decisions guided by 18F-FDG PET data altered patient outcome. The findings of the current substudy support the use of 18F-FDG PET viability imaging in patients with severe ischemic cardiomyopathy. They further support the notion that outcome benefits measured by a composite clinical endpoint may be achieved in a center with cardiac PET experience, ready access to 18F-FDG viability imaging, and integration of imaging with heart failure and revascularization teams. PARR 2 was the largest randomized trial to assess viability imaging and the first to focus on patients with severe left ventricular dysfunction. The trial demonstrated a trend toward outcome benefit, but this trend did not reach statistical significance (15). Randomized controlled trials that evaluate imaging modalities have been few (22) and are difficult to design and implement. PARR 2 is no exception. The results of the current study suggest that the trend toward benefit from a 18F-FDG PET–assisted management strategy over standard care may have been a consequence of the significant results in the Ottawa-FIVE subgroup (Fig. 1) As such, it is possible that PET results were more appropriately applied in the Ottawa-FIVE substudy population than in the rest of PARR 2. Why did this occur?
Access to 18F-FDG
In the Ottawa-FIVE substudy population, the ready access to 18F-FDG meant that its lack was not a limitation to patient enrollment. Any patient could undergo 18F-FDG PET 5 days of the week. In sites without PET, only patients willing and able to travel to a PET center were enrolled, representing a selection bias acknowledged in PARR 2. In sites with PET but with infrequent 18F-FDG shipment, limited access may also have limited enrollment of patients who were more likely to benefit.
Center Experience and Integration with Clinical Teams
In addition to Ottawa, there were 8 other recruiting sites in PARR 2, 5 of which did not have direct access to 18F-FDG PET at any time during the study. Of the 3 remaining sites, 2 were primarily oncology PET centers that each performed approximately 20 PET viability studies in the year before PARR 2. The third PET site acquired PET late during the PARR 2 trial so also did not have significant prior cardiac PET experience. The PARR 2 protocol standardized patient preparation, acquisition protocols, core laboratory processing, analysis, and interpretation, in an attempt to minimize any effect related to differences between sites. However, one may speculate that recruitment in the 3 other PET sites may have been driven by physicians interested in PET and the trial, whereas attending physicians may not have been as familiar with the importance of translating PET findings to clinical practice. As well, direct on-site interaction with the imaging centers may have been more limited. In contrast in the Ottawa-FIVE substudy population, attending physicians had experience implementing PET data in decision making (23). In addition, although not objectively measured, heart failure specialists, interventionalists, and cardiac surgeons often took the opportunity to review the images directly with the imaging experts. Other unmeasured factors may also have played a role, including factors such as how individual sites interpreted the central automated analyses and the quality and expertise associated with revascularization and postoperative care.
The effect of center experience is recognized as an important factor affecting outcomes (24–26). This post hoc subgroup analysis supports the premise that center experience may be one factor in realizing the potential outcome benefits of 18F-FDG PET–guided management.
Patient Population
The consequence of ready access and site experience is that the Ottawa-FIVE substudy may have been able to enroll sicker patients. Ottawa-FIVE patients did have slightly worse left ventricular function, were more often female, and tended to be older. There was a trend toward worse outcomes in the standard arm of the Ottawa-FIVE substudy than in the rest of PARR 2. This trend may also suggest a sicker population. A counterargument may be that in Ottawa, physicians had become dependent on 18F-FDG and that decision making in standard care therefore suffered. However, this argument would not explain why patients in the 18F-FDG PET arm had better clinical outcomes than the rest of the PARR 2 population.
Does this mean that only centers with experience and access to the tracers can achieve outcome benefits? No—only that centers undertaking cardiac 18F-FDG PET should ensure that tracers are as readily accessible as possible, the imaging team has sufficient expertise, and attending physicians are familiar with how to apply the imaging results. These precautions are likely true for all emerging imaging modalities.
Limitations
Ottawa-FIVE was a post hoc subgroup analysis. Hence, Ottawa-FIVE had the inherent limitations of post hoc and subgroup analyses (20,27–29) and should be confirmed in a larger prospective study.
The sample size was sufficient to identify the significant interaction between 18F-FDG PET–guided therapy and the Ottawa-FIVE subgroup in the primary outcome–adjusted model and the associated statistically significant hazard ratios. Post hoc power calculations based on PASS 2005 (NCSS) Cox proportional hazards regression give a power greater than 90% for the interaction and associated hazard ratios.
The overall mortality rate in the PET arm was 7.5%, which was lower than the rate in the standard arm: 14.8%. However, the sample size was too small to have enough statistical power to detect a significant difference. The mortality rate in the PET arm is similar to an annualized mortality rate of 7.9% calculated from the systematic review of observational PET viability studies by Schinkel et al. (4). Of note, the original design of PARR 2 did not consider this select subgroup. Other post hoc analyses have also been performed in PARR 2, including addressing adherence in the main trial (15) and evaluating parameters predicting adverse outcome in the 18F-FDG PET arm alone (30). The Ottawa-FIVE substudy represents an additional subgroup analysis prompted in part by a post hoc evaluation of an experienced site with access to 18F-FDG and submission requirements of Health Canada for data on 18F-FDG produced in Ottawa. The post hoc nature of the analysis, combined with the small sample size and the small number of hard events and the fact that the events were driven primarily by hospitalization, means that the results must be interpreted with caution. Hence, the results would best be confirmed in a larger prospective study. Finally, the fact that the PARR 2 trial did not consider 18F-FDG access, team expertise, or team integration represents a limitation of the main trial design. Future imaging trials should consider these factors.
CONCLUSION
This post hoc subgroup analysis of the PARR 2 trial suggests that 18F-FDG PET–guided management reduces the composite of cardiovascular events in patients with ischemic cardiomyopathy in a center with an experienced imaging team; established synergies between cardiac imaging, heart failure, and revascularization services; and ready access to 18F-FDG. Although larger prospective studies may be better suited to address hard events, centers where 18F-FDG can be made readily available should consider its routine use for viability detection in patients with ischemic left ventricular dysfunction. Centers using viability detection methods should ensure imaging expertise, access to tracer, and close communication with the health care team. These measures will facilitate the best use of imaging data toward optimizing patient outcomes.
Acknowledgments
The study was supported by the Canadian Institute for Health Research (grant MCT 37412) and the Heart and Stroke Foundation of Ontario (Grants-in-Aid NA4316 and T5222 and Program Grant PRG6242), supplemented by a University/Government/Industry Program: the Ontario Research and Development Challenge Fund, with MDS Nordion (ORDCF-00May-0710) for part-time coordinator salary support and the Whit and Heather Tucker Research Fellowship in Cardiology at the University of Ottawa Heart Institute for a clinical research fellowship. We thank Carrie Barlow for her assistance in the preparation of the manuscript; May Aung, Kimberly Gardner, Michaela Garkish, Debbie Gauthier, and Patricia Grant for their care of patients undergoing PET imaging; Samantha Mason and Paul Coletta for their assistance with 18F-FDG production; and Francois Benard, Karen Gulenchyn, Terrence Ruddy, Paul Hendry, Roy Masters, and Lyall Higginson for their input into the design and conduct of the study. The other participating sites and details of the participating teams from all sites have been published elsewhere (15). The PARR 2 registration number is NCT00385242 at the National Library of Medicine, National Institutes of Health (http://www.clinicaltrials.gov).
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 13, 2009.
- Accepted for publication August 27, 2009.





{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic importance of extensive coronary calcium on lung cancer screening chest computed tomography
- Hot Spot Imaging in Cardiovascular Diseases: An Information Statement from SNMMI, ASNC, and EANM
- Nuclear cardiology: state of the art
- Appropriate Use Criteria for PET Myocardial Perfusion Imaging
- Myocardial Viability: Survival Mechanisms and Molecular Imaging Targets in Acute and Chronic Ischemia
- Can Functional Testing for Ischemia and Viability Guide Revascularization?
- The Future of Cardiac Imaging: Report of a Think Tank Convened by the American College of Cardiology
- Clinical Value of F-18-Fluorodeoxyglucose Positron Emission Tomographic Imaging of Myocardial Viability Is Dependent on Adherence to Treatment Strategy Based on Imaging Results
- Revascularization in Patients With Severe Left Ventricular Dysfunction: Is the Assessment of Viability Still Viable?
- Communication is key
- Potential Applications of PET/MR Imaging in Cardiology
- Repeatable Noninvasive Measurement of Mouse Myocardial Glucose Uptake with 18F-FDG: Evaluation of Tracer Kinetics in a Type 1 Diabetes Model
- Identification of Therapeutic Benefit from Revascularization in Patients With Left Ventricular Systolic Dysfunction: Inducible Ischemia Versus Hibernating Myocardium
- More Evidence for the Survival Benefit of Coronary Revascularization Versus Medical Therapy in Patients With Ischemic Cardiomyopathy and Hibernating Myocardium
- Randomized Controlled Trials on PET: A Systematic Review of Topics, Design, and Quality
- Imaging-Guided Selection of Patients With Ischemic Heart Failure for High-Risk Revascularization Improves Identification of Those With the Highest Clinical Benefit
- Effects of Radiation Exposure From Cardiac Imaging: How Good Are the Data?
- Cardiac PET: A Versatile, Quantitative Measurement Tool for Heart Failure Management
- Imaging Myocardial Metabolic Remodeling