


Abstract
Graft infection after prosthetic vascular reconstruction is an uncommon but severe complication. The clinical presentation is often subtle and nonspecific and may occur long after surgery. Although defining a prosthetic vascular graft infection can be difficult, early diagnosis and treatment are important because of the relatively high rates of amputation and death. The present study assessed the role of PET/CT using 18F-FDG for the diagnosis of vascular graft infections. Methods: Thirty-nine patients (35 men and 4 women; age range, 44–82 y) with suspected vascular graft infection underwent 18F-FDG PET/CT. The performance of PET/CT for the diagnosis of an infectious process and its localization to the graft or soft tissues was assessed. The final diagnosis was based on histopathologic findings and microbiologic assays obtained at surgery or on clinical and imaging follow-up. Results: PET/CT detected foci of increased 18F-FDG uptake suspected as infection in 27 patients and localized these findings to the graft in 16 patients. Vascular graft infection was confirmed in 14 of these patients (88%). PET/CT excluded graft involvement in 11 patients, and in 10 (91%) of these 11, long-term follow-up further confirmed that the infectious process was limited to surrounding soft tissues only. No abnormal 18F-FDG uptake was found in any of the 12 patients with no further evidence of infection. PET/CT had a sensitivity of 93%, specificity of 91%, positive predictive value of 88%, and negative predictive value of 96% for the diagnosis of vascular graft infection. Conclusion: 18F-FDG PET/CT is a reliable noninvasive imaging modality for the diagnosis of vascular graft–related infection. The precise anatomic localization of increased 18F-FDG uptake provided by PET/CT enables accurate differentiation between graft and soft-tissue infection.
Graft infection is an uncommon but potentially severe complication after prosthetic vascular reconstruction. The overall frequency of this complication ranges from 0.5% to 5% and occurs, as a rule, a few months after surgery. Delay in the treatment of an infected vascular graft can lead to life-threatening complications such as sepsis or hemorrhage (1), with limb amputation and death occurring in more than 50% of patients (2,3). The clinical presentation is often subtle and nonspecific (2). When the vascular graft is surrounded by an abscess on CT or MRI, the diagnosis of a prosthetic vascular graft infection is obvious. However, in most cases, conventional imaging findings are nonspecific and diagnosis can be difficult (1,4).
PET using 18F-FDG is a well-accepted clinical tool for the routine assessment of cancer. 18F-FDG is a tracer of increased intracellular glucose metabolism and therefore taken up by malignant, as well as infectious and inflammatory, processes (5). Initial studies have reported a high sensitivity for 18F-FDG PET in the diagnosis of infection and inflammation (5–7). PET, however, often lacks the ability to define the precise anatomic location of a site of abnormal 18F-FDG accumulation.
PET/CT provides precise registration of metabolic and structural imaging data, obtained in the same session, on a single device, and has the potential for improving diagnosis and correctly localizing infectious processes in general and specifically when involvement of a prosthetic graft is suspected. The purpose of the present study was to assess the role of PET/CT using 18F-FDG for the diagnosis of a clinically suspected vascular graft infection.
MATERIALS AND METHODS
Patient Population
Thirty-nine consecutive patients with a suspected prosthetic vascular graft infection were prospectively evaluated using 18F-FDG PET/CT. The study included 35 men and 4 women, with a mean age of 68 y (range, 44–82 y). These patients had a total of 69 grafts (range, 1–4 grafts per patient), including 31 femoropopliteal, 20 aortobifemoral, and 18 other prosthetic vascular grafts. For 40 vascular grafts, infection was suspected on the basis of clinical signs including local pain and swelling, cellulitis, the presence of a pus-secreting surgical wound or abscess at the site of surgical scarring, bacteremia, and systemic fever (Table 1). The other 29 vascular grafts were not suspected of being infected. The clinical characteristics of the patient population and reasons for referral are presented in Table 1. The Institutional Review Board of the hospital approved the study, and each patient signed an informed consent form.
Clinical Characteristics of 39 Patients with Suspected Vascular Graft Infection
PET/CT Acquisition and Processing
Patients were instructed to fast, except for glucose-free oral hydration, for 4–6 h before the injection of 185–370 MBq (5–10 mCi) of 18F-FDG. Blood glucose levels were measured before injection. None of the patients were withdrawn from the study because of high blood glucose levels, and no additional glucose-controlling drugs were used. Diabetic patients were instructed to keep to their regular schedule of glucose-controlling drugs. PET and unenhanced CT were acquired consecutively 90 min after the injection of 18F-FDG, using a PET/CT system (Discovery LS; GE Healthcare) combining a third-generation multislice spiral CT scanner with a dedicated full-ring PET scanner with bismuth germanate crystals. The PET and CT devices are mechanically aligned back to back and share a common table. Proper registration of the 2 images is ensured by shared positional information of the table and patient for both the CT and the PET acquisitions. Data obtained from CT were used for low-noise attenuation correction of PET emission data and for fusion with attenuation-corrected PET images. PET images were reconstructed iteratively using ordered-subset expectation maximization software. PET, CT, and fused PET/CT images were available for review, displayed in axial, coronal, and sagittal planes. The PET data were displayed as noncorrected and attenuation-corrected images and also as a rotating maximum intensity projection.
Interpretation and Analysis of PET/CT Images
All studies were reviewed prospectively with knowledge of the patient's clinical history and the results of previous imaging studies. A combined team including a nuclear medicine physician, radiologist, and vascular surgeon interpreted the fused PET/CT images. Foci of increased 18F-FDG uptake were recorded. Focal increased 18F-FDG uptake in the region of any of the vascular grafts, with intensity higher than that of surrounding tissues, was defined as an infectious process. The presence and pattern of increased 18F-FDG uptake at the site of noninfected vascular grafts was assessed and recorded as well. Studies with no 18F-FDG uptake or showing only linear uptake of low to moderate intensity along the graft region were considered negative for the presence of infection. The precise PET/CT localization of the 18F-FDG focus to the soft tissues or the vascular graft was recorded.
The performance of PET/CT for the diagnosis of infected vascular grafts was assessed on a per-graft basis. True-positive PET/CT findings were focal abnormal 18F-FDG uptake localized to the graft, which was further confirmed to be infected. Abnormal 18F-FDG uptake localized to the graft on PET/CT, with no further evidence of graft infection, was classified as a false-positive finding. Negative PET/CT findings showing either no 18F-FDG uptake, mildly increased linear tracer uptake along the whole graft, or focal 18F-FDG uptake localized to soft tissues only, with no further evidence of vascular graft infection, were defined as true-negative. Negative PET/CT findings with further evidence of graft infection were defined as false-negative. Sensitivity, specificity, and negative and positive predictive values were calculated using standard definitions.
A final diagnosis of vascular graft or soft-tissue infection was confirmed by histopathologic findings and microbiologic assays obtained at surgery or by a decision of the referring clinical team based on further imaging workup and clinical follow-up. The diagnostic performance of PET/CT in relation to the presence of diabetes and to blood glucose levels was also assessed.
RESULTS
Thirty-nine patients were evaluated for a clinically suspected graft infection. In 38 patients, the clinical suspicion involved a single graft, whereas in 1 patient, 2 adjacent grafts were assessed. Twenty-seven PET/CT studies demonstrated foci of increased 18F-FDG uptake that were interpreted as positive for infection, and 12 studies showed no abnormal tracer activity. The final diagnosis indicated that the infectious process involved 15 of the 69 grafts.
PET/CT localized the sites of 18F-FDG uptake to vascular grafts in 16 of the 27 patients. Infection of the vascular graft was the final diagnosis in 14 (88%) of the 16 patients with PET/CT findings positive for graft infection. Eleven patients had surgery with microbiologic or histologic confirmation of graft infection. In 3 patients, surgery could not be performed because of the patient's general condition and the presence of other concurrent diseases. In 2 of these patients, the final diagnosis of graft infection was based on new findings on follow-up contrast-enhanced high-resolution CT and the development of pus-secreting fistulae that could be tracked as originating from the graft wall. In the third patient, in whom PET/CT localized 18F-FDG uptake to destructive graft changes consistent with a pseudoaneurysm that expanded significantly on 3 consecutive follow-up high-resolution CT studies, the clinical team concluded that this represented a vascular graft infection. The patient's general status deteriorated, with sepsis nonresponsive to broad-spectrum antibiotics, and died 2 wk after the PET/CT study. In addition to the diagnosis of graft infection, in 1 of the 14 patients who had a new graft adjacent to an older one, PET/CT enabled the differentiation and specific localization of infection to the newer graft, as was further confirmed at surgery.
PET/CT was false-positive for the diagnosis of an infected vascular graft in 2 of the 16 patients. Both patients had an infected hematoma, adjacent to and surrounding the graft, which resolved after antibiotic therapy.
In 11 patients, PET/CT localized the abnormal 18F-FDG uptake to soft-tissue processes adjacent to but not involving the vascular graft. Ten of these 11 patients showed no further evidence of graft infection on long-term follow-up ranging from 12 to 14 mo. These 11 patients were treated with antibiotics, and wound debridement was performed when indicated. The final diagnosis of an infectious process involving only the soft tissues was based on microbiologic sampling and clinical and further imaging workups. In 1 patient, considered through PET/CT to have a soft-tissue infection, an infected vascular prosthesis was diagnosed histologically at surgery.
In addition, in 2 of the 27 patients with positive findings, PET/CT also revealed osteomyelitis, the first case in the foot and involving the calcaneus, and the second case in the above-knee amputation stump.
In all 12 patients with negative PET/CT findings, no further evidence of graft infection was found on clinical and imaging follow-up of 12–24 mo (10 patients) or on histologic and microbiologic assays performed at graft removal surgery (2 patients).
The performance of PET/CT for the diagnosis of vascular graft infection had a sensitivity of 93%, specificity of 91%, positive predictive value of 88%, and negative predictive value of 96%.
No abnormal 18F-FDG uptake was seen in any of the 29 grafts not clinically suspected of being infected, and no further evidence of infection was seen in any of these grafts on long-term follow-up.
Ten of the 54 noninfected grafts showed a mild to moderate increase in linear 18F-FDG uptake along the graft on PET/CT. These grafts had been implanted 1–24 mo before the PET/CT study, as compared with 1 mo to 10 y for those showing no 18F-FDG uptake. Seven of the 10 grafts showing linear uptake were made of Gore-Tex (W. L. Gore and Associates) and 3 of Dacron (Invista, Inc.), as compared with 30 vs. 11, respectively, for those showing no 18F-FDG activity.
Eight of the 39 patients (21%) had type 2 diabetes mellitus. An infected graft was the final diagnosis in 2 of these 8 patients. PET/CT correctly localized the infection to the graft in 1 of the 2 patients. PET/CT indicated soft-tissue infection and soft-tissue infection with osteomyelitis in 2 additional patients, both without further evidence of graft involvement on histologic or clinical follow-up. No infection was evident in 4 diabetic patients with negative PET/CT findings. Blood glucose levels at the time of the study ranged from 3.3 to 18.3 mmol/L (60–330 mg/dL). Glucose levels exceeded 11.1 mmol/L (200 mg/dL) in 2 of the 39 patients. These included one patient with PET/CT results positive for soft-tissue infection not involving the graft and osteomyelitis, and another patient with negative PET/CT results and no further evidence of infection.
DISCUSSION
Graft infection is a severe complication of vascular reconstructive surgery, with high morbidity and mortality (2,4). Accurate diagnosis is challenging and relies on a combination of clinical symptoms and imaging findings. CT is considered the procedure of choice in the diagnosis of graft infection, with persistent opacity and perigraft soft-tissue fluid and gas having been described as features associated with graft infection. However, changes in soft-tissue density may be compatible with either infection or hematoma, fibrosis, and postoperative changes. The sensitivity of CT can reach 100%, but its specificity is impaired by the presence of extragraft infection sites (4,8,9). The value of MRI for the diagnosis of infected vascular grafts is unclear (4). Radionuclide imaging applying labeled white blood cells has been used for the assessment of suspected prosthetic graft infection, particularly in the early stages of disease. Infections localized in the vicinity of the graft can, however, account for false-positive results (10–12).
18F-FDG PET has been suggested for the diagnosis and assessment of infectious processes (6,13). A few reports have given sparse data on the role of 18F-FDG PET in the diagnosis of vascular graft infection (14,15). In a study aimed to investigate the value of 18F-FDG PET in the detection of aortic graft infection, Fukuchi et al. showed that although highly sensitive, PET performance was hampered by a lack of specificity (16). Despite high sensitivity, nuclear medicine procedures in general and PET in particular are limited by their inability to define the precise anatomic location of tracer activity. Correlation of functional data provided by PET with anatomic imaging such as CT or MRI may be required to accurately localize the site of infection, critical for defining the structures involved by the disease process. Visual side-by-side correlation or coregistration of separately performed PET and CT of the lower limbs is not accurate enough for localizing a focus of increased 18F-FDG uptake to the graft or the surrounding soft tissues. Minimizing registration errors is a challenging task (17,18), especially in the limbs. The small size and close proximity of anatomic structures, and the effect of even slight positional changes, may lead to inaccurate localization and subsequent faulty diagnosis.
Combined PET/CT is performed in the same setting on a single device without changing the patient's position, allowing for correct fusion of both sets of images (17). Hybrid imaging therefore has the ability to accurately localize the focus of increased tracer uptake to the infected anatomic site. Because increased 18F-FDG uptake has been described at sites of postsurgical inflammatory changes, in scar tissue and native vessels (19), differentiation of these causes of increased tracer activity from abnormal uptake within the graft is also important. Treatment of an infected vascular graft consists in its surgical removal—thus, the high importance of accurate diagnosis. False-positive results may lead to unnecessary surgery, whereas failure to diagnose graft infection can result in high-risk morbidity.
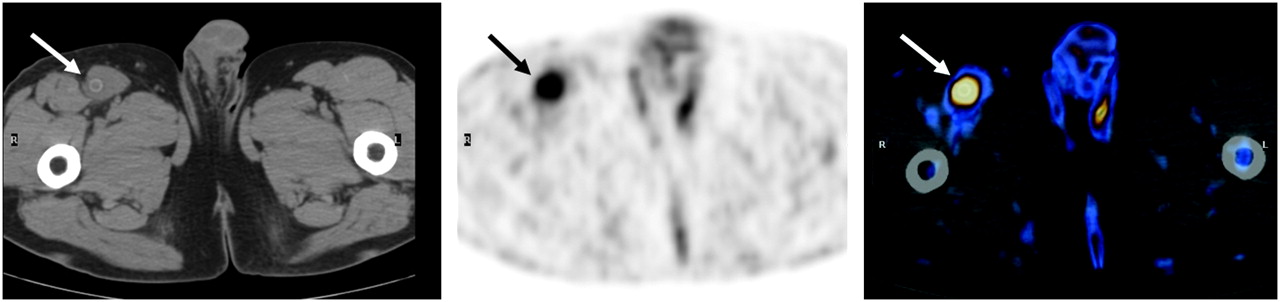
In the current study, whereas foci of increased 18F-FDG uptake were found in 30 of 39 patients with suspected vascular graft infection, PET/CT localized the suggestive lesions to only 16 grafts, thus indicating their involvement in the infectious process with a specificity of 91% (Fig. 1). In 1 of these patients, in whom 2 femoropopliteal bypass grafts were inserted within 5 y, PET/CT enabled the infection to be localized to 1 of the 2 adjacent implants, subsequently resulting in more accurate surgical planning.

A 54-y-old man who had received right femoropopliteal bypass graft 3 mo previously. Infection was clinically suspected because of fever and local pain in right groin. 18F-FDG PET (center) demonstrates focus of increased tracer uptake in right groin (arrow), localized by PET/CT (right) to right femoropopliteal vascular graft as seen on CT (left, arrow). Graft was considered to be involved by infectious process. Diagnosis was confirmed at surgery, and infected graft was removed.
Two false-positive PET/CT results were related to 18F-FDG uptake in an infected hematoma adjacent to and surrounding the graft. The hematoma could not be separated on the CT component of the study from the graft structure itself. In 14 patients, PET/CT led to the diagnosis of soft-tissue infection sparing the graft (Fig. 2). In all but 1 of these patients, soft-tissue infection was confirmed and the treatment strategy was changed, sparing surgical removal of the graft.

A 68-y-old man who had received left femoropopliteal bypass graft 18 mo previously. Infection was clinically suspected because of fever and infected surgical wound in medial aspect of left distal thigh. Coronal (top left) and transaxial (top right) 18F-FDG PET images show area of increased uptake in medial aspect of left thigh (arrows), localized by PET/CT image (bottom right) to soft-tissue swelling (arrow) adjacent to left femoropopliteal graft as seen on CT (bottom left). Patient responded rapidly to antibiotic therapy, and no vascular graft infection was evident on long-term follow-up of 14 mo.
In addition, in 2 patients PET/CT localized additional foci of abnormal 18F-FDG activity to bone, indicating the presence of osteomyelitis in a diabetic foot and in a femoral stump, as was further confirmed at surgery.
Mildly increased linear 18F-FDG uptake was seen along 10 grafts that had no further evidence of infection. This pattern is considered to be related to a postoperative foreign-body inflammatory reaction and is more frequent in recently implanted grafts (16), as was the case with 7 of the 10 grafts that were only 1–2 mo old in the current study.
Eight of the 39 patients in the study population had diabetes mellitus. Severe vascular diseases and infections are common complications in patients with diabetes and may raise concerns about the performance of PET. The effect of elevated serum glucose levels on the sensitivity of 18F-FDG PET in cancer patients is controversial (20,21). Limited data in the literature suggest that high blood glucose concentrations may not have a negative effect on 18F-FDG uptake in infectious processes (22). In the present study, 1 of 8 diabetic patients, who had normal blood glucose levels at the time of imaging, had a false-negative PET/CT result for localization of an infectious process to the graft. High blood glucose, however, which was found in 2 patients, did not account for false-negative results.
CONCLUSION
The current study demonstrated the feasibility and incremental value of 18F-FDG PET/CT, which may provide a useful tool for the noninvasive diagnosis of vascular graft infection. Studies on larger numbers of patients are needed to further validate the diagnostic performance of PET/CT and its role in the management of patients with this challenging clinical dilemma.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 30, 2007.
- Accepted for publication March 23, 2007.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Skin tumour resulting from late infection of a thoracic aortic prosthetic graft diagnosed by FDG-PET/CT
- The Value of 18F-FDG PET/CT in Diagnosis and During Follow-up in 273 Patients with Chronic Q Fever
- FDG Uptake by Prosthetic Arterial Grafts in Large Vessel Vasculitis Is Not Specific for Active Disease
- Vascular Graft Infections, Mycotic Aneurysms, and Endovascular Infections: A Scientific Statement From the American Heart Association
- 18F-FDG PET/CT for Therapy Control in Vascular Graft Infections: A First Feasibility Study
- Vascular graft infections and role of PET/CT in patients with persistent bacteraemia
- 18F-FDG Uptake in Noninfected Prosthetic Vascular Grafts: Incidence, Patterns, and Changes over Time
- Imaging of Inflammation by PET, Conventional Scintigraphy, and Other Imaging Techniques
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Usefulness of Fluorine-18 Positron Emission Tomography/Computed Tomography for Identification of Cardiovascular Implantable Electronic Device Infections
- Nuclear Medicine Imaging of Infection in Cancer Patients (With Emphasis on FDG-PET)
- Imaging of Inflammation by PET, Conventional Scintigraphy, and Other Imaging Techniques
- Do Hyperglycemia and Diabetes Affect the Incidence of False-Negative 18F-FDG PET/CT Studies in Patients Evaluated for Infection or Inflammation and Cancer? A Comparative Analysis
- Fever of Unknown Origin: The Role of 18F-FDG PET/CT
- High 18F-FDG Uptake in Synthetic Aortic Vascular Grafts on PET/CT in Symptomatic and Asymptomatic Patients