


Abstract
Graft infection is a serious complication to vascular surgery. The aim of this study was to assess 18F-FDG uptake in vascular grafts in patients with or without symptoms of graft infection. Methods: In all 2,045 patients examined by PET/CT at our clinic, 16 patients with synthetic aortic grafts were identified and reevaluated for 18F-FDG accumulation. Clinical and biochemical data were obtained from patient records. Results: High 18F-FDG uptake was found in 10 of 12 grafts in the patients who underwent open surgery and in 1 of 4 grafts in patients who underwent endovascular aneurysm repair. On the basis of biochemical and clinical data, it was concluded that 1 of the 16 patients had a graft infection at the time of investigation. Conclusion: 18F-FDG uptake in vascular grafts was found in the vast majority of patients without graft infection. The risk of a false-positive diagnosis of graft infection by 18F-FDG PET/CT is evident.
Postoperative infection in synthetic vascular grafts is a serious complication to vascular surgery, with an incidence of 1%–3% (1). Leukocyte scintigraphy is a diagnostic cornerstone, with a sensitivity and specificity of more than 90% (2,3).
18F-FDG PET/CT has developed into a widely used diagnostic modality primarily for malignant diseases. 18F-FDG uptake also accumulates in infectious lesions (4,5) and in inflammatory lesions such as large-vessel arteritis (6). Consequently, PET/CT theoretically has a potential to visualize vascular graft infections, as illustrated in several case reports (7–10) and in 2 systematic evaluations (11,12).
However, synthetic grafts provoke a chronic low-grade inflammation (13–15). This chronic inflammation constitutes a potential site for 18F-FDG uptake and, therefore, a risk for false-positive results.
This study was performed to assess 18F-FDG activity in synthetic abdominal aortic grafts during 18F-FDG PET/CT scans in patients with or without graft infection. We report the results on 18F-FDG accumulation in all 16 identified patients with synthetic abdominal aortic grafts out of our total of 2,045 patients.
MATERIALS AND METHODS
Patients
All 2,045 patients examined by 18F-FDG PET/CT at the Karolinska University Hospital, from the installation of the integrated PET/CT scanner in May 2006 until February 2008, were matched with the national Swedish registry for vascular surgery for abdominal aortic repair procedures, which resulted in 20 matches. Four patients had been examined before surgery and were therefore excluded. The examinations of the remaining 16 patients were reevaluated, and clinical and biochemical data were obtained from patient records.
Integrated PET/CT Examination
Examinations were performed using a PET scanner (Biograph 64 TruePoint; Siemens Medical Solutions) with an axial field of view of 21.5 cm. After 1 h of rest, 4 MBq of 18F-FDG per kilogram of body weight were administered intravenously. Sixty minutes later, examination started with a low-dose CT scan to correct the ensuing PET images for photon attenuation and scatter. PET examination was performed and followed by CT examination before and during intravenous injection of ioversol (Optiray; Tyco Healthcare Deutschland GmbH) contrast enhancement (350 mg of iodine/mL, 1 mL/kg body weight). The CT scan was performed using a continuous-spiral 64-detector-row technique with a tube voltage of 120 kV, pitch of 0.8, slice thickness of 1.2 mm, and rotation speed of 0.5 s/revolution. PET acquisition was made during 3 min at each bed position.
Image Analysis and PET Measurements
Examinations were reviewed by 2 radiologists aware of the clinical data, and a consensus was reached.
Examinations were reviewed in 3 orthogonal views. Fused PET/CT images were used to correlate PET signal with morphologic findings.
A 3-grade arbitrary scale was used to indicate high, low, or no 18F-FDG accumulation within the graft. CT examinations were reviewed to identify graft wall thickening, edema, or gas surrounding the graft or any other signs of graft infection.
In all examinations, 1 cm or larger circular regions of interest (ROIs) were drawn at 5 different levels of the descending and suprarenal abdominal aorta. The average mean standardized uptake value (SUVmean) of all ROIs was considered the mean blood-pool activity, and PET signal below this level was excluded when the radiologists reviewed the images. The target-to-background ratio (TBR) was calculated by dividing the maximum SUV (SUVmax) in the graft material with the mean blood-pool activity.
RESULTS
Of the 16 patients with synthetic abdominal aortic grafts, 4 patients had undergone the endovascular technique (EVAR). Fifteen of the patients experienced uneventful postoperative recoveries. The mean time between surgery and PET/CT was 6 y. Table 1 describes patient characteristics.
Clinical Characteristics of Patients
Table 2 illustrates the primary reasons for referral to PET/CT, the primary diagnosis obtained by PET/CT, and the results of the reevaluation.
Data from PET/CT Examinations
No increased 18F-FDG accumulation in the normal vessel wall of the large arteries in any patient was demonstrated. All 12 patients operated on with conventional open surgery (patients 1–12) displayed elevated 18F-FDG accumulation in the graft material. This accumulation was subjectively high in 10 patients and low in 2 patients (patients 5 and 7; Fig. 1). TBRs ranged from 1.4 to 5.7 (mean, 3.0) (Table 2). TBR was greater than 2.0 in all cases with subjectively high 18F-FDG accumulation and 2.0 or lower in grafts considered to have low 18F-FDG accumulation (Table 2).

CT, PET, and merged PET/CT images in transaxial plane and merged PET/CT images in coronal plane. Top 2 rows illustrate patients who underwent conventional open surgery, and bottom 2 rows illustrate patients operated with EVAR. Normal 18F-FDG accumulation in kidneys (K), ureters (u), liver (L), and bowel segments (B) is indicated in images. Patient 9 illustrates typical appearance of majority of conventional synthetic aortic grafts in material (arrows), with high 18F-FDG accumulation in virtually entire length of graft (SUVmax = 4.4; TBR = 3.4). Marked difference between normal vessel wall and graft is seen at site of proximal anastomosis (arrowhead). Patient 7 illustrates that few patients had low levels of 18F-FDG accumulation in their grafts (SUVmax = 2.8; TBR = 2.0). Patient 13 illustrates the only case of EVAR graft with high 18F-FDG accumulation (SUVmax = 5.4; TBR = 2.8), whereas patient 15 exemplifies low 18F-FDG accumulation seen at the grafts in the other EVAR patients (SUVmax = 2.4; TBR = 1.3).
For the EVAR group, TBR ranged from 1.3 to 2.9, with a mean of 1.8. 18F-FDG accumulation was assessed as high in 1 EVAR graft (patient 13; Fig. 1) and low or absent in 2 grafts (patients 15 and 16; Fig. 1). Figure 2 demonstrates marked 18F-FDG accumulation in a soft-tissue capsule around the aneurysmal sac, but not in the graft itself, in 1 patient (patient 14).
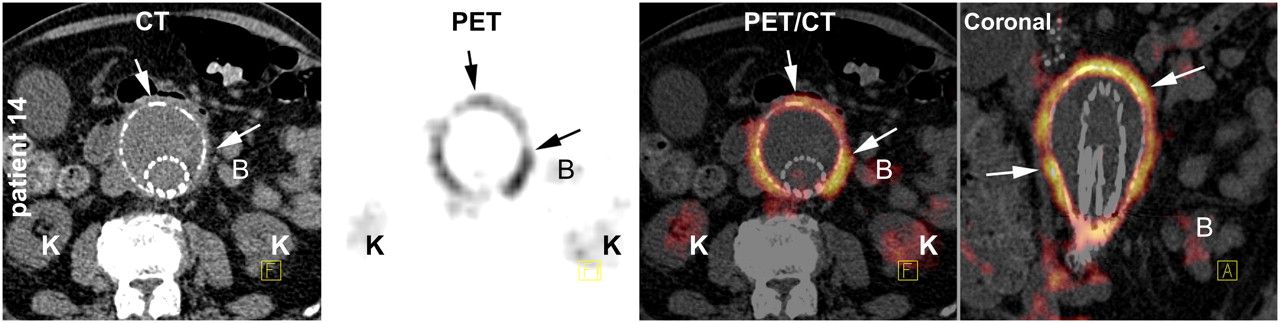
Patient 14 referred for suspected graft infection after presenting with fever 7 mo after EVAR. CT, PET, and merged PET/CT images in transaxial plane and merged PET/CT images in coronal plane illustrate high 18F-FDG accumulation around aneurysmal sac. Results were interpreted as aseptic postoperative inflammation, and patient made full recovery without antibiotic treatment. Normal 18F-FDG accumulation in kidneys (K) and bowel segments (B) is indicated in images.
On the basis of the high 18F-FDG uptake in the aortic graft, leukocyte scintigraphy was performed on patient 3, with a normal imaging result.
Patient 12 presented with fever 5 y after uneventful abdominal aortic aneurysm surgery. Blood cultures tested positive for Staphylococcus aureus. 18F-FDG accumulation was seen throughout the entire graft, with a markedly increased uptake in the ventral distal part of the graft. CT displayed a mass corresponding to the maximal 18F-FDG accumulation. Leukocyte scintigraphy showed increased activity in the same region (Fig. 3), and the radiologic diagnosis was graft infection.

Patient 12, who was referred for suspected graft infection after presenting with fever of unknown origin 5 y after uneventful open surgery and postoperative recovery. Shown are CT, PET, and merged PET/CT images in transaxial plane and merged PET/CT images in coronal plane (top row) and sagittal plane (middle row) and leukocyte scintigraphy in region of aortic graft (bottom row). Normal 18F-FDG accumulation in kidneys (K) and bowel segments (B) is indicated in images. Top row and coronal and sagittal planes illustrate 18F-FDG accumulation (arrows) in area close to proximal anastomosis, which was assessed as noninfected. Middle row illustrates 18F-FDG accumulation close to bifurcation corresponding to soft-tissue mass seen on CT ventral to graft (arrowheads) (not well illustrated on coronal projection [top row on far right] but well illustrated on sagittal projection [middle row on far right]). Bottom row illustrates results of leukocyte scintigraphy, with distinct uptake corresponding to area of graft bifurcation (arrows).
CT examination of patient 14 showed thickening of the wall of the aneurysmal sac, indicating a reaction to the EVAR procedure (Fig. 2). The patient recovered completely without antibiotic treatment.
In the remaining 14 patients (patients 1–11, 13, 15 and 16), no signs of ongoing graft infection were found. No graft infection developed in patients during a 2- to 18-mo (mean, 8 mo) follow-up period after PET/CT examination.
Biochemical analyses of white blood cell (WBC) count and C-reactive protein (CRP), performed before PET/CT examination, were normal or discretely elevated in 13 of 15 patients (Table 1). The significance of discrete elevations in this patient population is low; there were, for example, several patients with malignancies that may well explain these results. Patient 8 had an elevated CRP of 72, and the radiologic and clinical diagnosis was pneumonia. Patient 16 was examined by 18F-FDG PET/CT shortly after EVAR, and CRP decreased over time and normalized shortly after examination. This result was interpreted as a normal postoperative reaction.
DISCUSSION
This study describes 18F-FDG accumulation in synthetic abdominal aortic grafts. Prominent 18F-FDG accumulation in the vast majority of these 16 grafts was demonstrated, although careful reviewing of all case records revealed evidence for only 1 case of graft infection at the time of examination. No other graft infection developed in patients during the 2- to 18-mo follow-up period.
Keidar et al. (12) reported a sensitivity of 93%, specificity of 91%, positive predictive value of 88%, and negative predictive value of 96% for infection in synthetic vascular grafts for 18F-FDG PET/CT in a population of 39 patients with suspected graft infection. In their material, no elevated 18F-FDG accumulation in graft material of any of the 12 patients considered free from graft infection was demonstrated. These results are well within the range of the best results on leukocyte scintigraphy (2,3). However, for reasons unknown, our results disagree with those reported in the study by Keidar et al. (in which SUVmax and TBR were not reported). It is possible that relative differences in intensity, and thus different subjective cutoff values for TBR, may explain the vast differences in results.
Fukuchi et al. (11) also reported a sensitivity of 91% for 18F-FDG PET, compared with a sensitivity of 64% for CT, in 33 patients with suspected graft infections. However, the specificity for 18F-FDG PET was merely 64%, compared with 86% for that of CT, with 8 cases of false-positive findings for 18F-FDG PET and 3 for CT. The patient material reported by Fukuchi et al. (11) is different from ours, but their results appear to be more comparable to those of our study than do the findings of Keidar et al. (12).
The only positive case of graft infection (patient 12) had the highest SUVmax and TBR, suggesting that very high SUVmax and TBR may be more specific for graft infection. Prospective investigations may be able to identify a threshold level for SUVmax or TBR below which graft infection is unlikely.
The chronic aseptic inflammation in synthetic graft material, mediated primarily by macrophages, fibroblasts, and foreign-body giant cells, constitutes a potential base for 18F-FDG uptake, even a long time after the operation (13–15).
In our material, 10 of 12 patients with synthetic abdominal aortic grafts who underwent conventional operations displayed markedly high 18F-FDG uptake in the grafts; 1 of 4 patients displayed the same result after EVAR. No clinical or biochemical evidence for graft infection at the time of examination was observed in any of these patients.
CONCLUSION
It is likely that a large portion of patients with synthetic vascular grafts will display high 18F-FDG accumulation in the graft material during PET/CT examination, even a long time after surgery, without having a graft infection. The basis for this 18F-FDG accumulation may be the chronic inflammation known to occur on the surface of synthetic graft material (13–15). Although not statistically significant, the 18F-FDG accumulation appears to be less prominent in endovascular grafts than in conventional grafts.
On the basis of the data reported here and in the absence of large prospective investigations, we suggest caution when using 18F-FDG PET/CT to diagnose infection in synthetic vascular grafts because of the apparent risk of false-positive results.
Acknowledgments
This study was supported by the SWEDVASC Steering Committee.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 14, 2008.
- Accepted for publication June 9, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Infection Imaging: Focus on New Tracers?
- FDG Uptake by Prosthetic Arterial Grafts in Large Vessel Vasculitis Is Not Specific for Active Disease
- Respective Performance of 18F-FDG PET and Radiolabeled Leukocyte Scintigraphy for the Diagnosis of Prosthetic Valve Endocarditis
- 18F-FDG Uptake in Noninfected Prosthetic Vascular Grafts: Incidence, Patterns, and Changes over Time
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Experiences with Citrate Rather Than Heparin as an Anticoagulant for 18F-FDG Labeling of Leukocytes