


Abstract
Fever of unknown origin (FUO) was originally defined as recurrent fever of 38.3°C or higher, lasting 2–3 wk or longer, and undiagnosed after 1 wk of hospital evaluation. The last criterion has undergone modification and is now generally interpreted as no diagnosis after appropriate inpatient or outpatient evaluation. The 3 major categories that account for most FUOs are infections, malignancies, and noninfectious inflammatory diseases. The diagnostic approach in FUO includes repeated physical investigations and thorough history-taking combined with standardized laboratory tests and simple imaging procedures. Nevertheless, there is a need for more complex or invasive techniques if this strategy fails. This review describes the impact of 18F-FDG PET in the diagnostic work-up of FUO. 18F-FDG accumulates in malignant tissues but also at the sites of infection and inflammation and in autoimmune and granulomatous diseases by the overexpression of distinct facultative glucose transporter (GLUT) isotypes (mainly GLUT-1 and GLUT-3) and by an overproduction of glycolytic enzymes in cancer cells and inflammatory cells. The limited data of prospective studies indicate that 18F-FDG PET has the potential to play a central role as a second-line procedure in the management of patients with FUO. In these studies, the PET scan contributed to the final diagnosis in 25%–69% of the patients. In the category of infectious diseases, a diagnosis of focal abdominal, thoracic, or soft-tissue infection, as well as chronic osteomyelitis, can be made with a high degree of certainty. Negative findings on 18F-FDG PET essentially rule out orthopedic prosthetic infections. In patients with noninfectious inflammatory diseases, 18F-FDG PET is of importance in the diagnosis of large-vessel vasculitis and seems to be useful in the visualization of other diseases, such as inflammatory bowel disease, sarcoidosis, and painless subacute thyroiditis. In patients with tumor fever, diseases commonly detected by 18F-FDG PET include Hodgkin's disease and aggressive non-Hodgkin's lymphoma but also colorectal cancer and sarcoma. 18F-FDG PET has the potential to replace other imaging techniques in the evaluation of patients with FUO. Compared with labeled white blood cells, 18F-FDG PET allows diagnosis of a wider spectrum of diseases. Compared with 67Ga-citrate scanning, 18F-FDG PET seems to be more sensitive. It is expected that PET/CT technology will further improve the diagnostic impact of 18F-FDG PET in the context of FUO, as already shown in the oncologic context, mainly by improving the specificity of the method.
Fever of unknown origin (FUO) was defined in 1961 by Petersdorf and Beeson as recurrent fever of 38.3°C or higher, lasting 2–3 wk or longer, and undiagnosed after 1 wk of hospital evaluation (1). The last criterion has undergone modification and is now generally interpreted as no diagnosis after appropriate inpatient or outpatient evaluation (2). Following these guidelines will eliminate from consideration most short-lived viral pyrexias and other benign transient causes of fever.
In 1991, Durack and Street proposed a new system for the classification of FUO: classic FUO in nonimmunocompromised patients, nosocomial FUO, neutropenic FUO, and FUO associated with HIV infection (3). The diagnostic and therapeutic approach in immunocompromised patients is conceptually different from that in patients with “classic” FUO and is not dealt with specifically in this review.
THE CLINICAL PROBLEM
Prolonged, undiagnosed fever is usually an atypical manifestation of a more common disease rather than a manifestation of an exotic illness. The diseases underlying FUO are numerous, and infections account for 13%–43% of them. Most patients with FUO have autoimmune or collagen vascular disease or a neoplasm—responsible for up to 54% of all cases. In 10%–40% of patients with FUO, the underlying disease remains undiagnosed (3–8).
There is general agreement that every successful strategy in the diagnostic work-up of FUO has to take into account the symptoms and clinical history of the patient. In a prospective multicentric study, repeated physical investigations and thorough history-taking combined with standardized laboratory tests and simple imaging procedures were successful in the diagnosis in approximately one third of all FUO patients enrolled (5).
Nevertheless, there is a need for more complex or invasive techniques if this strategy fails. Endoscopy, biopsy, high-resolution CT, MRI, and nuclear medicine techniques may be used in these cases. Imaging will be helpful only if a focal pathologic cause is responsible for the fever.
Searching for the focus of fever with radiotracers seems to be attractive for several reasons:
Radionuclide imaging allows the detection of focal pathologic changes early in the disease course even in the absence of a morphologic correlate.
Scintigraphy will show positive findings in several autoimmune diseases that are usually not detected by conventional procedures.
In lesions that are suggested to be biologically inactive by other methods, radioactive tracers with a specific uptake in inflammatory or tumor tissue may show a positive signal, thus providing strong arguments for the activity of the process.
Radionuclide imaging is usually performed as a whole-body procedure allowing delineation of both the location and the number of foci, even at sites that are clinically not suspected.
Although methods that use in vitro or in vivo labeled white blood cells (WBCs) have a high diagnostic accuracy in the detection and exclusion of granulocytic abnormalities, these methods are of only limited value in FUO patients in establishing the final diagnosis because of the rather low prevalence of granulocytic processes in this clinical setting. WBCs are more suited to the evaluation of a focus in occult sepsis (9).
67Ga-Citrate is a γ-emitter that can image acute, chronic, granulomatous, and autoimmune inflammation and infection, as well as various malignant diseases. Therefore, 67Ga-citrate was long considered to be the tracer of choice in the evaluation of FUO. The percentage of 67Ga-citrate scans contributing to the final diagnosis was generally found to be higher than that reported for labeled WBCs (9).
It has long been recognized that 18F-FDG accumulates not only in malignant tissues but also at sites of infection and inflammation and in autoimmune diseases, but a systematic assessment of this method in diagnosing nonneoplastic conditions has been undertaken only in the past decade. This review describes the impact of 18F-FDG PET in the diagnostic work-up of FUO as reported in the literature.
MOLECULAR BASIS OF 18F-FDG UPTAKE IN TUMOR AND INFLAMMATORY CELLS
Physics and Metabolism of 18F-FDG
18F-Labeled FDG is a structural analog of 2-deoxyglucose with a half-life of 110 min.
Three mechanisms of transport are responsible for the uptake of glucose and 18F-FDG into mammalian cells. The first, passive diffusion, is of minor importance for human tissues. The second, active transport by a Na+-dependent glucose transporter (GLUT), is of importance in kidney epithelial cells and in the intestinal tract. The third mechanism, and the most important pathway for 18F-FDG to enter the cell body of almost all human cells, is mediated by the facultative GLUT-1 through GLUT-13 (10).
Once 18F-FDG has entered the cell, it is subsequently phosphorylated to 2′-FDG-6 phosphate by the hexokinase enzyme. In contrast to glucose-6-phosphate, 2′-FDG-6 phosphate is not a substrate for the enzymes of the glycolytic pathway or the pentose–phosphate shunt. The content of the enzyme glucose-6-phosphatase, which could reverse the initial phosphorylation of 18F-FDG, is low in many tissues and tumors. In these tissues, 2′-FDG-6 phosphate is trapped because it cannot be metabolized, nor can it diffuse back into the extracellular space. In other organs with high concentrations of the enzyme, such as the liver, uptake of 2′-FDG-6 phosphate decreases after a rapid initial accumulation. Similar kinetics are also observed in leukocytes (9,11,12).
Biodistribution
After intravenous application, 18F-FDG is preferably taken up in tissues with high glucose consumption. The tracer is filtered in the kidney glomeruli, and only a small amount is reabsorbed by the renal tubular cells. Rapid clearance of 18F-FDG from the intravasal compartment results in a high target-to-background ratio within a short time, and imaging can therefore start as early as 30–60 min after injection.
A high accumulation of 18F-FDG is regularly seen in the brain, especially in the cortex and the basal ganglia. Cardiac uptake is infrequently noted and often patchy. Accumulation of 18F-FDG activity in the urine interferes with visualization of pelvic and, sometimes, abdominal abnormalities. Circumscribed or diffuse gastrointestinal uptake may result from smooth muscle peristalsis. Uptake of 18F-FDG in the reticuloendothelial system, especially in the bone marrow, varies. In patients with fever, bone marrow uptake is usually high, probably as a consequence of interleukin-dependent upregulation of GLUTs (9). The peripheral bones are usually free of activity. Physiologic uptake of 18F-FDG in the brain, myocardium, kidneys, and urinary bladder and variable accumulation of 18F-FDG in the bowel hinder interpretation of PET findings in these organs and is a drawback of the method in the context of FUO.
Uptake of 18F-FDG in Tumor Cells
An increased uptake of 18F-FDG has been found in various tumors (13), as can be explained by overexpression of distinct facultative GLUT isotypes and by overproduction of glycolytic enzymes (12). The isotypes involved and overexpressed in the process of malign transformation are GLUT-1, GLUT-3, or GLUT-5 (12–15). This has already been demonstrated in cancers of the gastrointestinal tract (esophagus, colon, and pancreas), lung cancer, head and neck cancer, and thyroid cancer—to name just a few.
Four different isoenzymes of hexokinase are known and show a pronounced tissue-specific distribution. In malignant cells, type II hexokinase and to a lesser extent type I hexokinase are overexpressed regardless of whether the tissue of origin expresses these enzymes (16). It has been shown that increased transcription of the hexokinase gene is, at least in part, responsible for this overproduction (16).
The tumoral stroma (microenvironment) plays another critical role in uptake of 18F-FDG by tumors. It is now acknowledged that tumor cells and their stroma coevolve during tumorigenesis and progression. The tumor microenvironment influences growth of the tumor and its ability to progress and metastasize. Stroma consists of cells, an extracellular matrix, and extracellular molecules. Among the identified cells are fibroblasts, glial cells, epithelial cells, adipocytes, inflammatory cells, immunocytes, and vascular cells (17). Many of these stromal elements contribute to tumoral 18F-FDG uptake, as was recognized nearly 15 years ago by Kubota et al. (18).
Uptake of 18F-FDG in Inflammatory Cells and Granulation Tissue
In vitro studies of 18F-FDG metabolism in inflammatory cells have used mixed preparations of WBCs or pure preparations of neutrophils and mononuclear cells. The labeling efficiency in WBCs ranged from 40% to 80% (19–23). In mixed preparations, cell labeling was predominately due to granulocytic uptake, accounting for 78%–87% of the activity. Optimal labeling efficiency occurred at 37°C. The uptake increased within the first 60 min and was inversely proportional to the glucose concentration in the labeling medium (19,21). When neutrophils were stimulated by the chemotactic peptide n-formyl-methionyl-leucyl-phenylalanine for a relatively short time of 60 min, a significant increase in 18F-FDG uptake, compared with that in nonstimulated cells, was observed (19,21). The labeling of WBCs with 18F-FDG is not very stable, and an elution of 27%–35% within the first 60 min has been reported (19,21).
Activated lymphocytes in acute inflammatory tissues showed an increased uptake of 18F-FDG in both in vitro and in vivo models (22). In an animal model of bacterial infection induced by inoculation with Escherichia coli, autoradiographs showed that the highest 3H-FDG uptake was in the area of inflammatory cell infiltration surrounding the necrotic region (23).
Substantial uptake of 18F-FDG by inflammatory cells is, at least in neutrophils, a postmigratory event of activated cells and not dependent on an ongoing chemotactic stimulus. This fact was demonstrated in a comparative study with 111In-leukocytes and 18F-FDG of neutrophil function in patients with acute lobar pneumonia or bronchiectasis. Neutrophil emigration was evident in bronchiectasis patients but not in pneumonia patients, whereas 18F-FDG uptake was selectively increased in pneumonia patients but not in bronchiectasis patients (24).
Autologous leukocytes labeled with 18F-FDG have been studied in vivo in healthy volunteers. The scintigrams reflect the normal physiologic distribution of leukocytes in the liver, spleen, and bone marrow, and the distribution of labeled cells is broadly similar to that reported for 111In-leukocytes. Some uptake in the brain indicates elution of 18F-FDG from the labeled cells. Kinetic analysis shows that about a quarter of the activity may have been released from leukocytes in vivo over 6 h, a finding that fits well with the in vitro data (20). Although labeling leukocytes with 18F-FDG is far from ideal, the feasibility of this approach has recently been demonstrated using PET/CT technology in a small series of patients (21).
The molecular basis of 18F-FDG uptake in WBCs and elements of granulation tissue and granulomas exhibits striking similarities to the metabolism of 18F-FDG in tumors. GLUT-1 together with GLUT-3 is the most important isotype for understanding 18F-FDG uptake in WBCs, especially after stimulation. Overexpression of GLUT-1 after stimulation with cytokines or mutagens has been demonstrated in elements of both inflammatory tissues and granulation tissues (25–28).
GLUT-1 is located predominantly in the plasma membrane but can also be found within intracellular vesicles (27). After stimulation, the intracellular GLUT-1 pool can be translocated to the cell membrane, thus increasing the glucose transport capacity within a relatively short time (28). The late (>24 h) increase in 18F-FDG uptake by stimulated inflammatory cells in vitro is due to a gene-dependent de novo synthesis of GLUT-1 (25–27,29–34). In addition, neutrophils and macrophages also show an overproduction of the hexokinase II enzyme during the respiratory burst (30).
GLUT-3 has a high affinity for glucose and can be found in a wide range of tissues, especially in the kidney, the placenta, and the neurons in the brain, where GLUT-3 ensures a constant glucose supply even at low extracellular glucose concentrations (10). In macrophages, the GLUT-3 affinity for glucose was found to be enhanced during the respiratory burst (35). In an animal model, inflammatory tissue showed a high expression of GLUT-1 and GLUT-3 (36).
Influence of Elevated Serum Glucose Levels and Insulin
Very high serum glucose levels (more than 900 mg/dL) were shown to substantially impair tumor uptake of 18F-FDG in an animal model (37). It has also been reported that, during hyperglycemia, the level of 18F-FDG uptake in tumors decreased significantly to approximately half that during the fasting state in nondiabetic patients with bronchial carcinoma or with head and neck cancer (38,39). Similar results were reported for pancreatic cancer patients (40).
Zhao et al. (41) determined the effects of modest hyperglycemia (150–180 mg/dL), induced by a glucose load, on 18F-FDG uptake in inflammatory lesions of infectious and noninfectious origin and in malignant tumors in rats. These investigators found that 18F-FDG uptake in both types of inflammatory lesions was significantly impaired by hyperglycemia whereas uptake of 18F-FDG in tumors was not significantly altered.
These observations were partly explained by altered expression of facultative GLUT isotypes in the hyperglycemic state. Glucose loading significantly decreased the expression of GLUT-1 (inflammatory lesions of noninfectious origin) and GLUT-3 (inflammatory lesions of infectious origin), whereas the expression levels of GLUT-1 and GLUT-3 in the tumor were not significantly affected (42).
In another study, 18F-FDG uptake in a mesothelioma cell line significantly decreased as the glucose level increased from 50 to 200 mg/dL. 18F-FDG uptake by peripheral blood mononuclear cells, on the other hand, exhibited little change between the same glucose concentrations but also decreased as the concentration of glucose exceeded 250 mg/dL (43).
The results of in vitro studies do not necessarily predict the reaction of inflammatory or malign tissues in vivo. Besides serum glucose concentration, a variety of other factors influence 18F-FDG uptake in vivo, such as the nature of the lesion, cytokine expression, the status of angiogenesis, hypoxia, and necrosis, and the results of modest hyperglycemia may therefore not be predictable in an individual patient.
These uncertainties should not lead automatically to the exclusion of patients with modest diabetes and suspected infection or autoimmune disease from an 18F-FDG study. Zhao et al. (42) concluded from a large retrospective clinical data set that below a level of 250 mg/dL, elevated glucose concentrations do not have a negative effect on 18F-FDG uptake in inflammatory cells, contrary to observations in malignant disorders.
Insulin loading significantly decreased the level of 18F-FDG uptake in tumors and in infectious and inflammatory lesions in an animal study (41,42). Because insulin loading did not significantly affect the expression of GLUT-1 and GLUT-3 in these lesions, a different mechanism has to be considered.
One probable explanation is that hyperinsulinemia increases the level of glucose uptake in GLUT-4–rich organs such as the heart, fat, and muscles by translocation of GLUT-4 from intracellular vesicles to the membranes and therefore shifts uptake from the inflammatory lesions to these tissues (41,42).
ROLE OF 18F-FDG PET IN PATIENTS WITH FUO
Studies of 18F-FDG PET in FUO
Only a few publications have directly addressed the problem of imaging FUO with 18F-FDG PET (44–51). The few data currently available are far from fulfilling the criteria of an evidence-based medicine.
In contrast to earlier studies with 67Ga-citrate or labeled WBCs in FUO patients, most publications about the role of 18F-FDG PET have used a uniform definition of undiagnosed fever (revised Petersdorf's criteria). However, some studies were retrospective, represented only a selected group of patients, or evaluated both patients with classic FUO and patients with postoperative sepsis (45,49,51).
Prospective studies on a cohort of consecutive patients are rare (44,46–48). To our knowledge, only 2 studies have compared 67Ga-citrate with 18F-FDG PET on a head-to-head basis (44,47) and only 1 study has used a structured protocol in the diagnostic workup of FUO. In that study, 18F-FDG PET or 67Ga-citrate scanning was used as a second-line procedure (47,52). The timing of 18F-FDG PET in the diagnostic process in other studies was less clear (44–46,48–51).
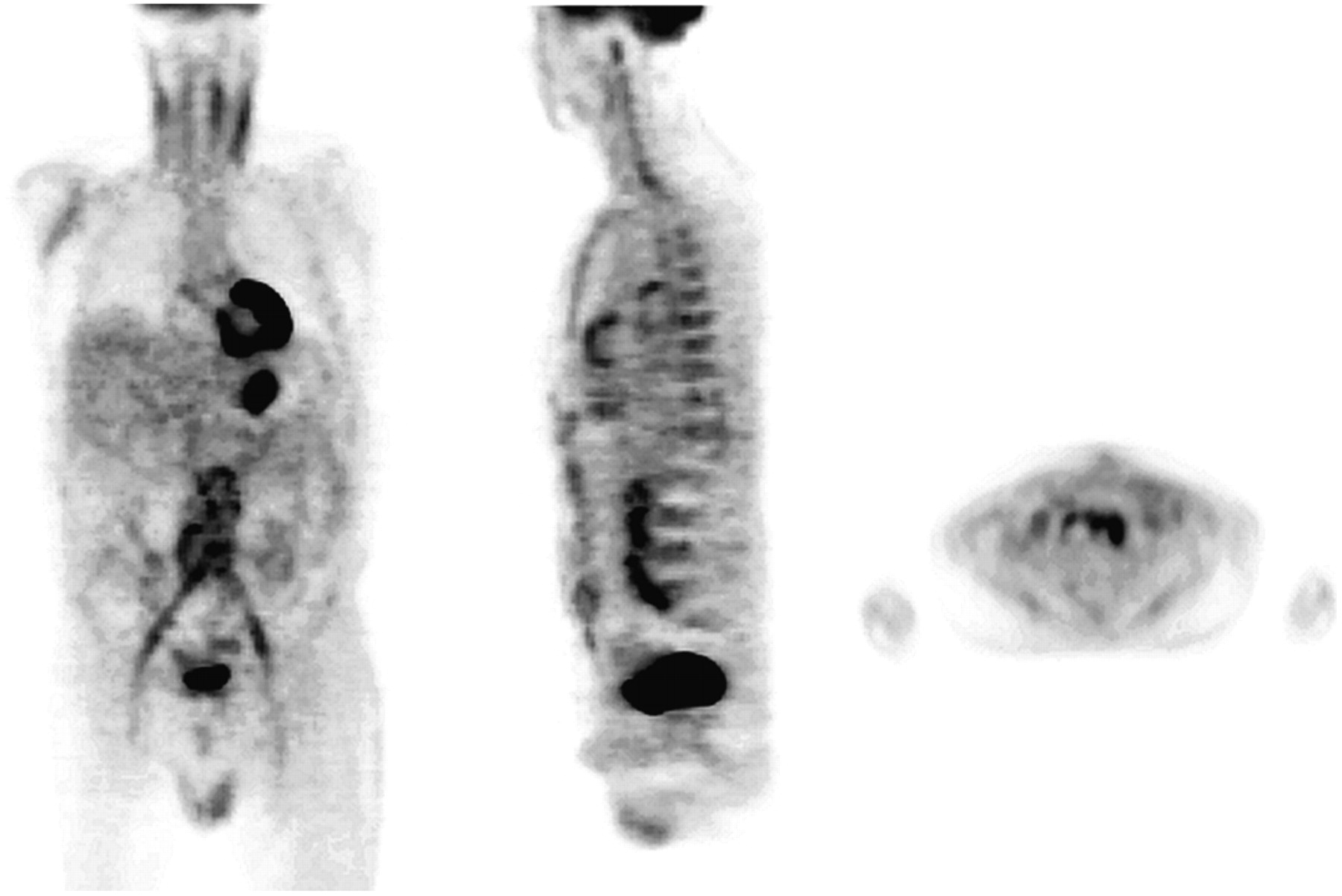
Calculations of formal sensitivities and specificities in FUO patients are difficult and even misleading for a variety of reasons. First, a final diagnosis and therefore a true gold standard for the diagnostic impact of a procedure are typically missed in a substantial number of patients. Second, a negative result on a scan is generally not helpful in the diagnostic work-up of FUO even if the result may formally be true-negative (9,44–51). Third, pathologic accumulations of 18F-FDG often are not adequately followed up if radiologic procedures show no obvious morphologic substrate; hence, the pathologic 18F-FDG accumulations often have to be reviewed as false-positive findings (Fig. 1) (44,47).
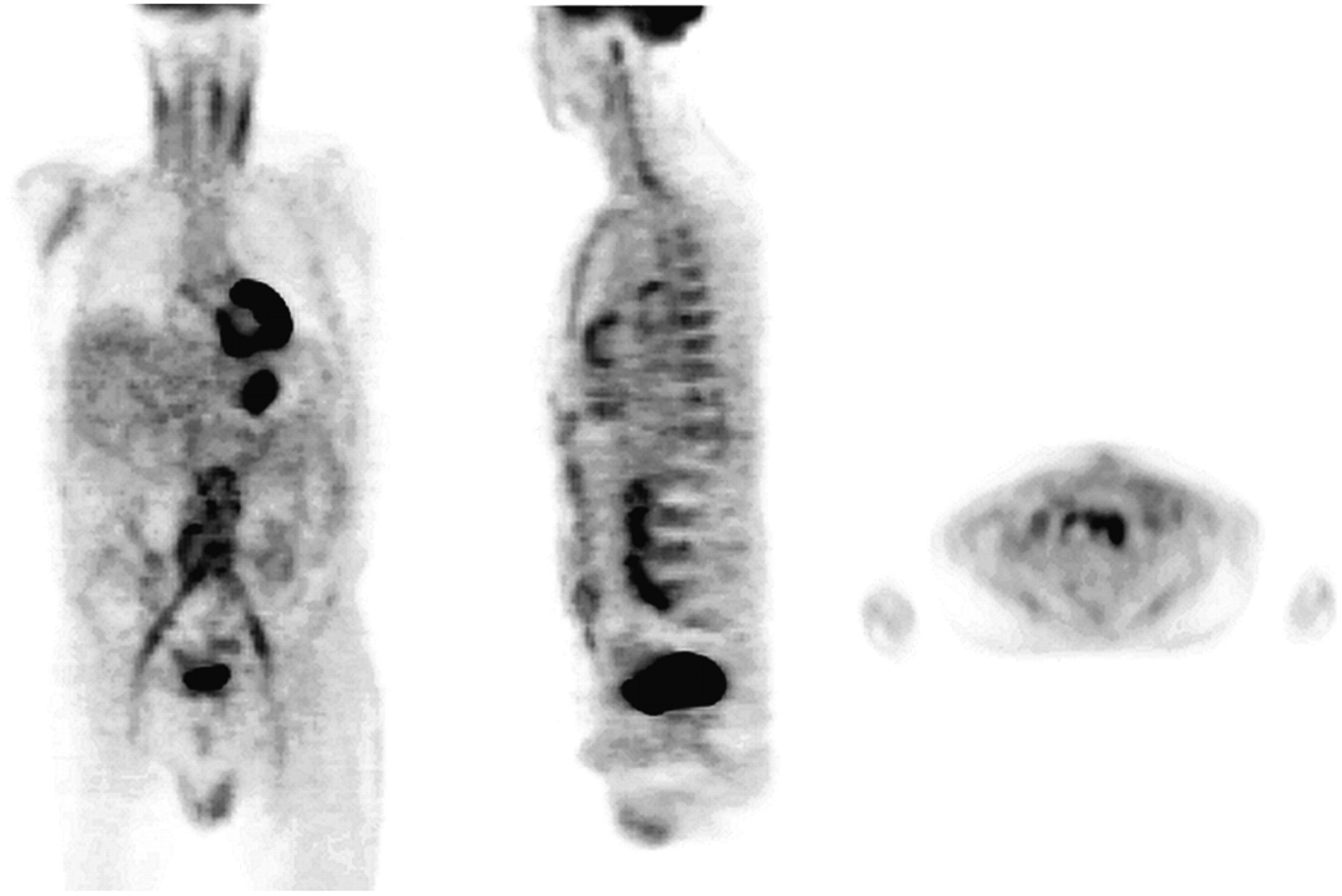
18F-FDG PET (from left to right: coronal, sagittal, and transversal slices) of 65-y-old patient with long-standing FUO 6 y after revision of aortic aneurism, which was replaced by vascular graft. PET scan demonstrates elevated uptake in graft extending to adjacent tissue. Infection of graft was subsequently proven during diagnostic work-up.
In the assessment of a method of diagnosing FUO, it seems most useful to ask how often this technique essentially helped to establish the final diagnosis (9). Not unexpectedly, the percentage of 18F-FDG PET scans helpful in the diagnostic process in patients with FUO, as reported in the literature, varies between 25% and 69%, reflecting the wide range of possible causes of fever. Comparison of these studies is also difficult because of the heterogeneity of the patient populations, differences in PET technique, and differences in the number of undiagnosed patients.
Our group prospectively compared 18F-FDG PET and 67Ga-citrate SPECT in 20 consecutive patients referred because of FUO (44). We found a sensitivity of 81% and a specificity of 86% for 18F-FDG PET in detecting the cause of the fever and a sensitivity and specificity of 67% and 78%, respectively, for 67Ga-citrate SPECT. Of the 20 patients studied with 18F-FDG, the findings were positive and essentially contributed to the final diagnosis in 11 (55%). No focus of enhanced 67Ga-citrate uptake was missed on the 18F-FDG scans. 67Ga-Citrate SPECT produced negative findings in 1 patient with a pelvic abscess and was nondiagnostic in 3 patients with aortitis clearly shown by PET.
In another prospective study, on 18 patients with postoperative fever, we found a sensitivity of 86% and a specificity of 100% for 18F-FDG PET in detecting infections outside the surgical wound. However, the specificity of 18F-FDG PET in detecting infections within the surgical wound was only 56%, whereas the sensitivity was 100%. Unspecific accumulation of the tracer in granulation tissue at the site of surgical intervention may be the most likely explanation for these findings (46).
Lorenzen et al. (45) reported the results of 18F-FDG imaging in a retrospective series of 16 patients with undiagnosed fever in whom conventional diagnostics had not been conclusive. Pathologic accumulations of 18F-FDG were found in 12 patients (75%) and led to the final diagnosis in 11 patients (69%).
In a prospective study, Blockmans et al. (47) compared the role of 18F-FDG PET with that of 67Ga-citrate scintigraphy in 58 consecutive cases of FUO. In 38 patients (66%), a final diagnosis was established. Forty-six 18F-FDG PET scans (79%) showed abnormal findings, and 24 (41%) of these scans were considered helpful in the diagnosis. In a subgroup of 40 patients, both 18F-FDG PET and 67Ga-citrate scintigraphy were performed. 18F-FDG PET was helpful in establishing the diagnosis in 35% of the patients, whereas diagnostic 67Ga-citrate scanning was helpful in only 25%. All foci of abnormal gallium accumulation were also detected by 18F-FDG PET.
In 35 patients with FUO, Bleeker-Rovers et al. (48) observed that 43% of all PET scans showed abnormal findings. A final diagnosis was established in 19 patients (54%). Of the scans with abnormal findings (representing 43% of all scans), 87% were clinically helpful in this prospective evaluation.
In a large prospective series of 74 patients with classic FUO (50), 53 (72%) of the 18F-FDG PET scans had abnormal findings; 19 scans (36% of those with abnormal findings, or 26% of the total number of scans) were clinically helpful. In the 39 patients with a final diagnosis, 49% of the scans were helpful. A diagnosis was established in 31 (58%) of the 53 patients with abnormal findings and in 8 (38%) of the 21 patients with normal findings.
Jaruskova and Belohlavek (51) published a retrospective evaluation of 18F-FDG PET and 18F-FDG PET/CT results in 124 patients with prolonged febrile temperatures (FUO and postoperative fever). 18F-FDG PET or PET/CT contributed to establishing a final diagnosis in 84% of the 51 patients with positive PET findings and in 36% of all 118 evaluated patients with prolonged fever.
Kjaer et al. (49) prospectively compared, on a head-to-head basis, the diagnostic value of 18F-FDG PET with that of 111In-granulocyte scintigraphy in 19 patients with FUO. A final diagnosis was obtained in 12 (63%) of the patients. In 3 patients (25% of the patients with a final diagnosis), 18F-FDG PET was considered true-positive and helpful in the diagnosis.
In these studies, common causes of FUO detected by PET included a variety of malignancies, especially colorectal cancer, sarcoma, Hodgkin's disease, non-Hodgkin's lymphoma (44–49), and several infectious diseases such as atypical pneumonia, spondylitis, tuberculosis, infected prostheses, and occult abscesses (44–50).
Noninfectious inflammatory diseases were also successfully diagnosed using 18F-FDG PET. An important advantage of 18F-FDG over other radiotracers is its ability to reveal vasculitis in large and medium-sized arteries. Aortitis, usually in the context of giant cell arteritis, was common in all series (44–50). 18F-FDG PET was also judged to be helpful in other autoimmune diseases, such as Still's disease (47,48) and periarteritis nodosa (48). In addition, 18F-FDG PET was helpful in cases of sarcoidosis (44,45,48) and other multisystemic granulomatous diseases. The value of 18F-FDG in the diagnosis of specific entities will be discussed in detail in the next section.
Both our group (44) and Blockmans et al. (47) published data about the diagnostic performance of 18F-FDG PET and 67Ga-citrate scintigraphy when compared on a head-to-head basis. In both studies, all foci of abnormal gallium accumulation were detected by 18F-FDG PET as well, but 18F-FDG PET findings were selectively positive in some patients with negative gallium findings. Most of these patients had vasculitis (44,45), but the use of 18F-FDG PET was also successful in the diagnosis of small abscesses not detected by 67Ga-citrate (44).
The higher diagnostic accuracy of 18F-FDG imaging than of 67Ga-citrate scintigraphy may be explained by the preferable tracer kinetics of the small 18F-FDG molecule, compared with those of the relatively large 67Ga-transferin complex, and by the better spatial resolution of PET systems than of conventional γ-cameras (44).
18F-FDG PET in Patients with Infectious Disease
In a series of FUO patients reported in 2004, infections still remained the most important category (7). Although only parts of these diseases are strictly focal, imaging with radiologic or radionuclide techniques remains an important second-line approach in their diagnosis. The following section gives an overview of some common causes of FUO that can be diagnosed through 18F-FDG PET with a high degree of certainty. Many of these infectious diseases have not been fully evaluated by 18F-FDG PET and PET/CT. In particular, comparative head-to-head studies with other radiotracers are not available.
Focal Infections.
Tahara et al. (53) published data about the use of 18F-FDG PET in detecting abscesses in 2 patients in the late 1980s. Since then, numerous case reports have been published, but data from larger series are rare.
Abdominal and pelvic abscesses, active tuberculosis, bacterial colitis, diverticulitis, and infected vascular grafts can accurately be identified by 18F-FDG PET, with sensitivities generally exceeding 90% (Fig. 1) (44,46,48,54–57). In addition, the method has been highly sensitive in imaging patients at a high risk of infection and of metastatic infectious disease, even when the results of other diagnostic procedures were normal (56,57).
Recently, Mahfouz et al. (57) retrospectively determined the role of 18F-FDG PET in the diagnosis of focal infection in patients with multiple myeloma. In 143 patients, 165 infections were identified. The infections were caused by bacteria, mycobacteria, fungi, and viruses. Most infections involved the upper respiratory tract and the lungs (n = 99) and were easily identified. A substantial part of these infections (e.g., atypical pneumonias) could not be diagnosed by other methods at the time of their appearance, thus confirming earlier observations on FUO patients (44). Successful imaging of pulmonary infection is the domain of 18F-FDG PET and of 67Ga-citrate scanning, whereas simple pneumonia without complications usually shows no uptake of labeled WBCs (9).
Soft-tissue infections, although usually not the focus of radionuclide imaging, can be used to test the paradigms of 18F-FDG PET in infectious disease. All sites of soft-tissue infection were detected by PET in 27 patients in a study by Stumpe et al. (54). Similar data can be drawn from the studies of the Philadelphia and Nijmegen groups (48,55).
Chronic Osteomyelitis.
There is no generally accepted definition for chronic osteomyelitis, a term that has been established on the basis of histologic, clinical, and etiologic factors to describe bone infections (58–61). Chronic osteomyelitis normally results from inadequately treated acute hematogenous osteomyelitis or may follow exogenous bacterial contamination that is due to trauma or surgical procedures. In contrast to acute osteomyelitis, chronic osteomyelitis is characterized predominantly by the presence of lymphocytic and plasmacellular infiltrates and a variable amount of necrotic tissue and osteosclerosis (58–61). Cases of asymptomatic chronic osteomyelitis, especially of the central skeleton, are almost an invariable part of larger series of FUO patients (44–51).
Guhlmann et al. (62) were the first to report a prospective study on the possible role of 18F-FDG PET in the diagnosis of chronic osteomyelitis. They evaluated the results of 18F-FDG PET and antigranulocyte antibody scintigraphy in 51 patients. Patients who underwent bone surgery within the previous 2 y were excluded. In 31 of the patients, histologic findings or the results of bacterial culture were available. Excellent accuracy was found for both techniques (97% for 18F-FDG PET and 92% for antigranulocyte antibody scintigraphy) in the peripheral skeleton (n = 36). In the axial skeleton (n = 15), accuracy was significantly higher for 18F-FDG PET (93%) than for antigranulocyte antibody scintigraphy (80%; P < 0.05).
In another publication by the same group (63), in 31 patients suspected of having chronic osteomyelitis in the peripheral (n = 21) or axial (n = 10) skeleton and with histologic findings available, the overall sensitivity and specificity of 18F-FDG PET were 100% and 92%, respectively. The 1 false-positive case was a patient with a soft-tissue infection of the mandible. Patients with previous bone surgery within the 12 mo before PET were excluded, possibly explaining the low rate of false-positive findings in Guhlmann's studies.
Zhuang et al. (64) investigated 22 patients with possible chronic osteomyelitis (axial skeleton, n = 11; peripheral skeleton, n = 11). 18F-FDG PET correctly diagnosed all 6 patients with chronic osteomyelitis. There were 2 false-positive findings, resulting in a sensitivity, specificity, and accuracy of 100%, 87.5%, and 91%, respectively. The 2 false-positive findings were caused by recent osteotomy.
Kälicke et al. (65) reported the results of 18F-FDG PET in 15 histologically confirmed cases of infection (8 with chronic and 7 with acute osteomyelitis). 18F-FDG PET yielded true-positive results in all 15 patients. However, the absence of negative findings in this series may raise questions about selection criteria.
De Winter et al. (66) prospectively evaluated the feasibility of dual-head γ-camera coincidence imaging in 24 patients with a possible chronic orthopedic infection. The investigators consecutively performed 18F-FDG imaging with a dedicated PET camera and a dual-head γ-camera coincidence device. The final diagnosis was obtained by microbiologic proof in 11 patients and clinical follow-up in 13 patients. The sensitivity and specificity were 100% and 86%, respectively, for 18F-FDG dedicated PET and 89% and 96%, respectively, for 18F-FDG dual-head γ-camera coincidence imaging. The same group published a prospective study of 60 patients in whom chronic osteomyelitis, spondylodiskitis, or infection of a total-joint prosthesis was suspected (67). Microbiologic and histopathologic findings were available for 42 patients. All 25 infections were correctly identified. There were 4 false-positive findings; in 2 of these cases, surgery had been performed less than 6 mo before the study. The sensitivity and specificity for the 33 patients with a suspected infection of the axial skeleton were 100% and 90%, respectively. The sensitivity and specificity for the 13 patients with a suspected infection of the peripheral skeleton were 100% and 86%, respectively.
Our group published a prospective analysis of 29 consecutive patients (68) who were studied because of possible chronic osteomyelitis and underwent combined 111In-WBC imaging and 18F-FDG PET with a coincidence camera. In 4 patients, bone surgery had been performed within the last 6 mo. Of the 34 regions with suspected infection, 13 were localized in the axial skeleton and 21 in the peripheral skeleton. Chronic osteomyelitis was proven in 10 of the 34 regions and subsequently excluded in 24 of the 34 regions. The final diagnosis was established by histologic and culture results in 18 regions and by MRI and clinical follow-up results in 16 regions. The sensitivity of PET was 100% and the specificity 95%. The results of 111In-WBC imaging were inferior, especially in the axial skeleton.
Infection of an orthopedic prosthesis (mainly of the hip or the knee) may cause prolonged monosymptomatic fever in some patients (51). As recently published (69), 18F-FDG PET allows reliable prediction of periprosthetic inflammatory tissue reactions. However, reliable differentiation between abrasion-induced and bacterial inflammation is not always possible by 18F-FDG PET. Because of the high sensitivity of this technique, a negative PET result in the context of FUO eliminates the need for further investigations or revision surgery. In contrast, a positive result does not always allow differentiation between inflammation and infection.
18F-FDG PET in Patients with Noninfectious Inflammatory Diseases
Noninfectious inflammatory diseases comprise a large variety of autoimmune and connective tissue diseases, as well as vasculitis syndromes, granulomatous disorders (sarcoidosis, Crohn's disease), and “miscellaneous” diseases such as subacute thyroiditis and other endocrine disorders (7,70–72). Noninfectious inflammatory diseases encompass 15%–30% of all causes of FUO (7).
Vasculitis Syndromes.
Vasculitis is defined as blood vessel inflammation with leukocytic infiltration in the vessel wall and reactive damage to mural structures and surrounding tissues. According to the Chapel Hill Consensus Conference of 1992, vasculitides are classified according to the size and type of vessels that most commonly are affected by the disorder (73).
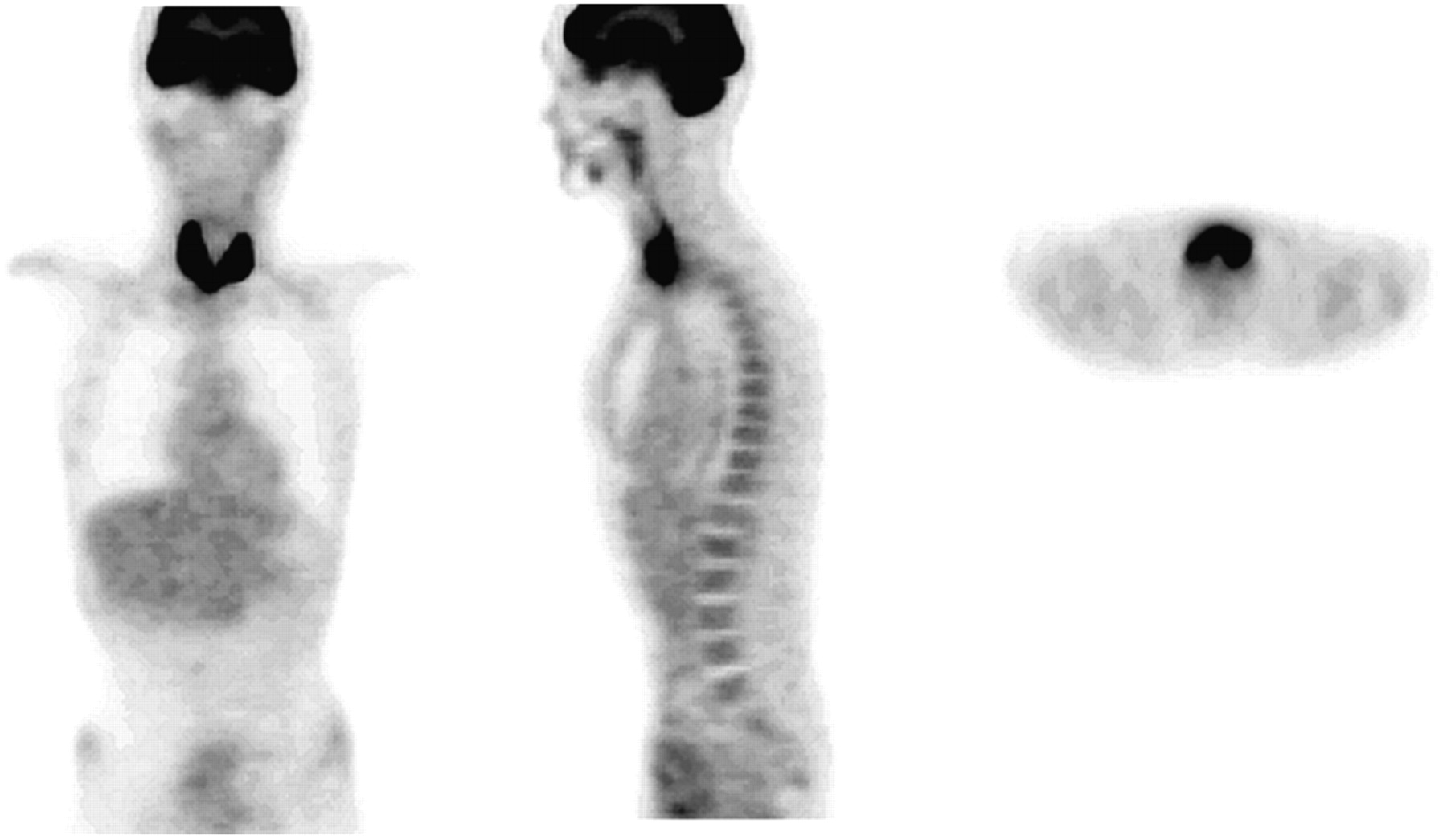
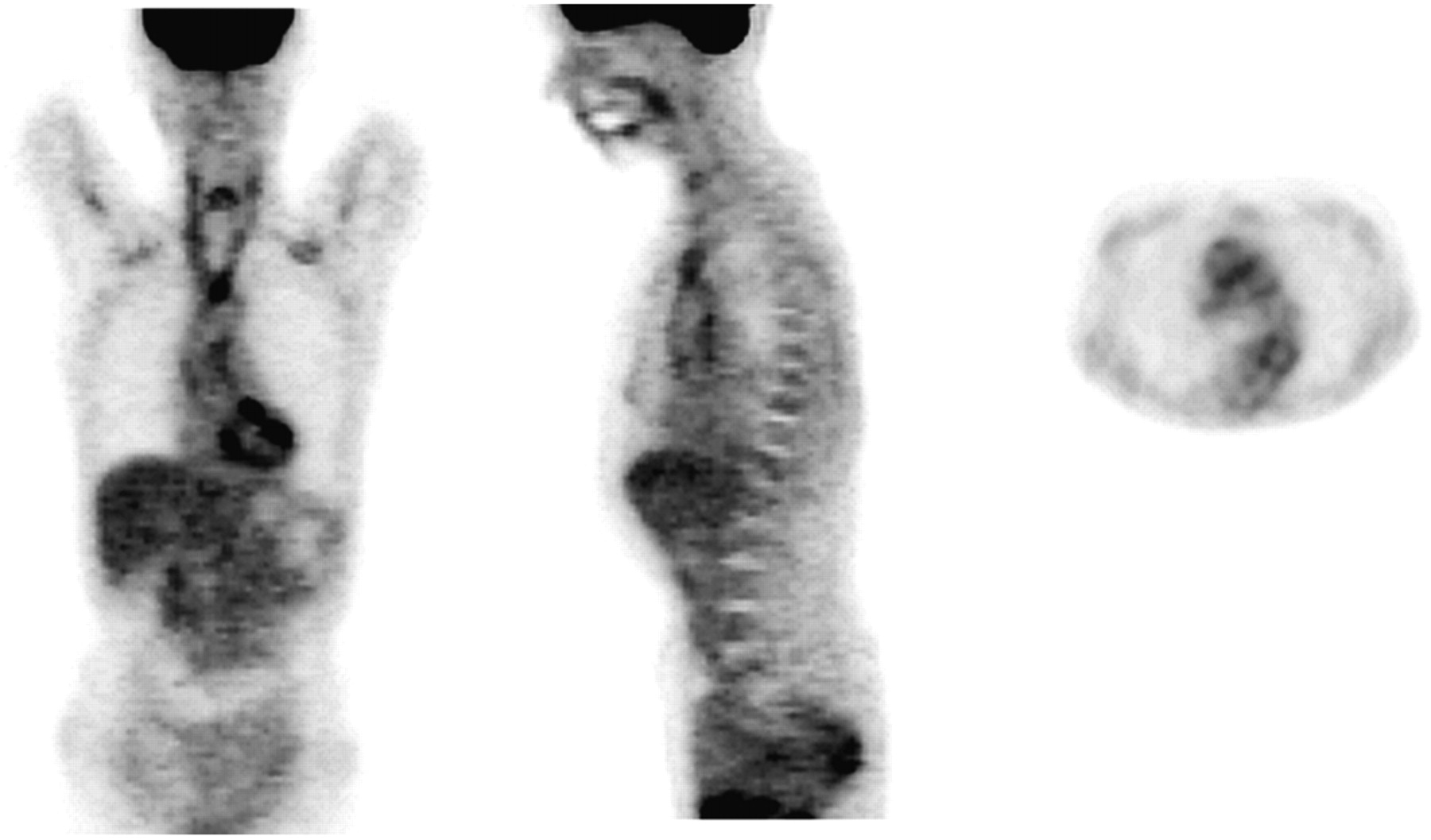
Large-vessel vasculitis, especially giant cell arteritis (GCA) with or without polymyalgia rheumatica, represents up to 17% of all cases of FUO in elderly patients (Fig. 2) (7,72). GCA is almost always confined to older white patients. Many cases can easily be detected by their typical symptoms, but some patients experience nonspecific symptoms, which may include FUO, malaise, weight loss, and an elevated erythrocyte sedimentation rate. In patients with Takayasu's arteritis, the “pulseless” phase of the disease is generally preceded by similar unspecific symptoms.

18F-FDG PET (from left to right: coronal, sagittal, and transversal slices) of 52-y-old patient with FUO. PET demonstrated elevated uptake in wall of thoracic aorta and supraaortal branches. Atypical GCA was diagnosed subsequently. After medication with glucocorticoids had begun, fever resolved and systemic signs of inflammation normalized.
It was noticed early (44) and confirmed by others later (45,47–51) that patients with vasculitis of the large arteries represent a substantial portion of all cases of FUO that can be detected by 18F-FDG PET even the absence of abnormalities on 67Ga-citrate scanning. These data indicate that vasculitis remained largely undiagnosed in earlier series of FUO patients who were evaluated with conventional radiotracers (Fig. 2) (9).
Blockmans et al. (74) were the first to systematically evaluate the use of 18F-FDG PET, in a series of 5 patients with polymyalgia rheumatica, 6 patients with GCA, and 23 age-matched control subjects. Increased 18F-FDG uptake in large thoracic vessels was noted in 4 of 5 patients with polymyalgia rheumatica and in 4 of 6 patients with GCA, compared with 1 of 23 control subjects (P < 0.001). Since then, numerous reports about vasculitis in the large arteries have been published, mainly in the context of GCA but also in patients with Takayasu's arteritis (75–88).
From these data, some preliminary conclusions about the value of 18F-FDG PET in the diagnosis and follow-up of large-vessel vasculitis can be drawn:
18F-FDG PET is sensitive (77%–92%) and highly specific (89%–100%) in the diagnosis of large-vessel vasculitis in untreated patients with elevated inflammatory markers (82,85–88).
18F-FDG-uptake, if semiquantitatively scored, correlates well with markers of disease activity, especially in GCA (81,84,87).
18F-FDG PET cannot reliably be used to diagnose or monitor inflammation of the temporal artery. In a study performed by Brodmann et al. (83) to determine the role of 18F-FDG PET as a noninvasive technique for the diagnosis of Horton's disease, 22 patients with a clinical diagnosis of GCA and a positive hypoechogenic halo on duplex sonography underwent 18F-FDG PET. All patients with positive sonographic findings in the large arteries (thoracic and abdominal aorta and subclavian, axillary, and iliac arteries) also had increased 18F-FDG uptake. However, 18F-FDG was false-negative in blood vessels smaller than 4 mm.
18F-FDG PET is highly effective in determining the extent of disease in the whole body. In a prospective series of 15 patients (GCA, n = 14; Takayasu's arteritis, n = 1) with pathologic large-vessel uptake on 18F-FDG PET, we compared the PET findings with MRI findings (80). MRI confirmed the PET findings in all patients. The results of both modalities were broadly comparable, but 18F-FDG PET identified more regions involved in the inflammatory process. Thus, whole-body 18F-FDG PET can be used as the investigation of choice if vasculitis of the large arteries is suspected, because the chance of a positive finding may be higher with PET than with MRI.
18F-FDG PET appears to be a reliable, noninvasive method of monitoring disease activity and response to therapy. In a prospective series of GCA patients, 18F-FDG PET was more reliable than MRI in monitoring disease activity during immunosuppressive therapy (80). Normalization of 18F-FDG uptake during follow-up clearly correlated with clinical improvement and normalization of laboratory findings, whereas MRI performed at similar intervals on the same patients showed improvement in only a minority of the vascular regions that had initially shown vessel wall thickening.
In summary, 18F-FDG PET has a strong potential in the diagnosis of atypical GCA in FUO patients by demonstrating extratemporal disease and in the diagnosis of early Takayasu's arteritis. The diagnosis of both diseases at early stages with PET allows early treatment, which may prevent progression to the later catastrophic complications.
The role of 18F-FDG PET in the diagnosis of other vasculitides is less clear. Vasculitis of medium and small vessels (especially in Churg-Strauss syndrome, Wegener's disease, and panarteritis nodosa) is usually detected only if large vessels are also involved (89) or if inflammatory damage is present in the adjacent tissue (82). Systematic studies are not available.
Other Noninfectious Inflammatory Diseases.
Cases of sarcoidosis, a multisystem granulomatous disease of unknown etiology, have been included in publications about FUO patients (44,48,50). These patients show an elevated uptake in mediastinal and hilar lymphatic nodes, extending sometimes into the pulmonal parenchyma even in the absence of typical radiologic features (44,48,50). Despite several case reports about the use of 18F-FDG PET in sarcoidosis, no prospective studies of larger series are available. 18F-FDG PET cannot distinguish sarcoidosis from diseases such as Hodgkin's disease or non-Hodgkin's lymphoma, but in the context of FUO this drawback is of minor importance.
Adult-onset Still's disease is another systemic inflammatory disorder of unknown etiology and pathogenesis. There is no single diagnostic test for this disease; rather, the diagnosis is based on clinical criteria such as fever, skin rash, lymphadenopathy, and hepatosplenomegaly. On 18F-FDG PET, uptake is high in the bone marrow, the spleen, and affected lymphatic nodes (47,48). The utility of radionuclide imaging in FUO patients with adult-onset Still's disease may be limited mainly to cases in which a septic disease has to be excluded.
Atypical Crohn's disease is a well-known cause of FUO (1–8,5,1). In a prospective study, Neurath et al. (90) compared the diagnostic accuracy of 18F-FDG PET, hydro-MRI, and 99mTc-anti-CD66 immunoscintigraphy. Forty-five detected foci were accessible to endoscopic verification. In these patients, 18F-FDG PET had a sensitivity of 85.4% and a specificity of nearly 90%.
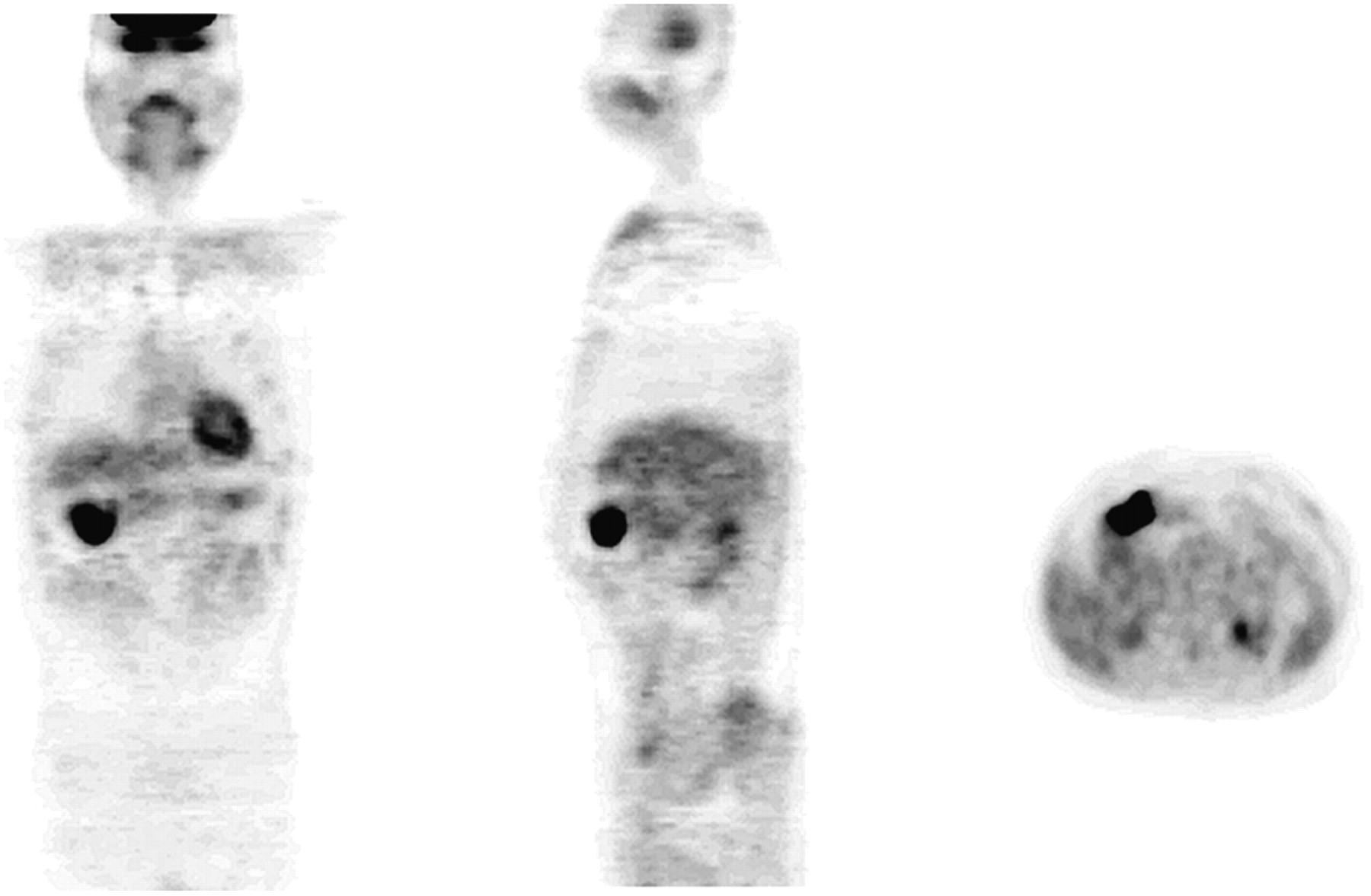
Subacute thyroiditis was relatively common in one published series of FUO patients (7). Usually, the disease can easily be diagnosed by typical clinical features such as neck pain, fever, malaise, myalgia, fatigue, and prostration. In atypical cases, FUO may be the only symptom. 18F-FDG PET usually detects painless subacute thyroiditis through a high focal or, more often, elevated diffuse uptake in the thyroid (Fig. 3).
18F-FDG PET (from left to right: coronal, sagittal, and transversal slices) of 45-y-old patient with FUO (coronal view). High uptake in thyroid (maximum standardized uptake value, 14.3) was found. Subacute, painless granulomatous thyroiditis was subsequently proven cytologically. After glucocorticoid medication had begun, fever disappeared within 2 d.
18F-FDG PET IN PATIENTS WITH TUMOR FEVER
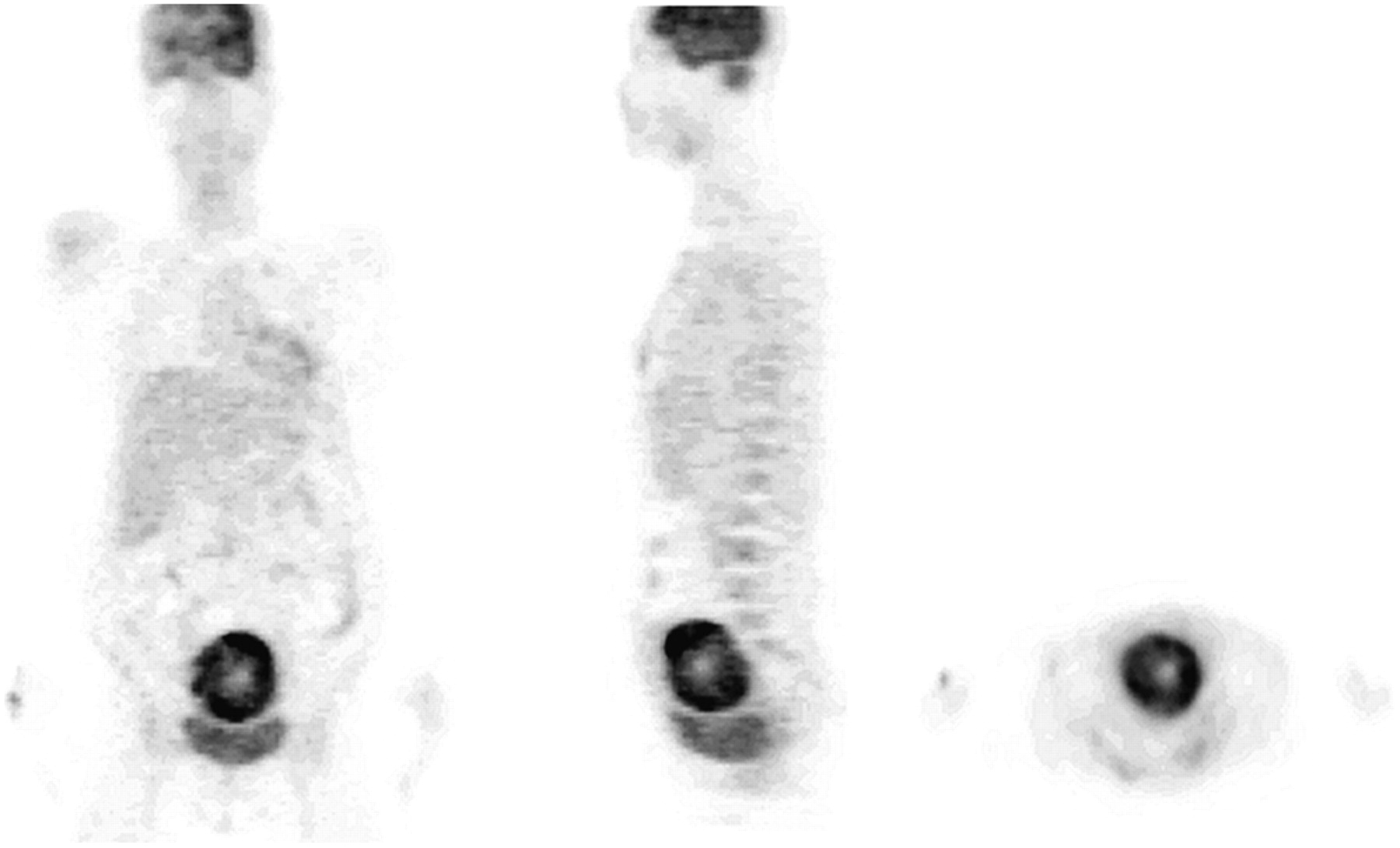
Tumors are common in elderly FUO patients. The relative importance of tumors as a cause of FUO is declining, probably because of the easy detection of solid tumors and enlarged lymph nodes by ultrasonography and CT (70). In a population-based study from Denmark, patients with FUO had an increased risk for hematologic malignant disease; sarcoma; and cancers of the liver, brain, kidney, colon, and pancreas (91). Many of these tumors, especially Hodgkin's disease and aggressive non-Hodgkin's lymphoma, but also colorectal cancer, pancreatic cancer, and sarcoma, are diseases commonly detected by 18F-FDG PET (13) and were found consistently across several series of FUO patients imaged by this method (Figs. 4 and 5) (44,48–51). An extended review of the role of 18F-FDG PET in oncology is not intended in this section. For further particulars, we refer the reader to the many excellent reviews published within the last few years.
18F-FDG PET (from left to right: coronal, sagittal, and transversal slices) of 62-y-old patient with long-standing FUO. PET revealed accumulation of tracer in right colonic flexura. During diagnostic work-up, adenocarcinoma in this location was diagnosed. Fever disappeared after surgery.
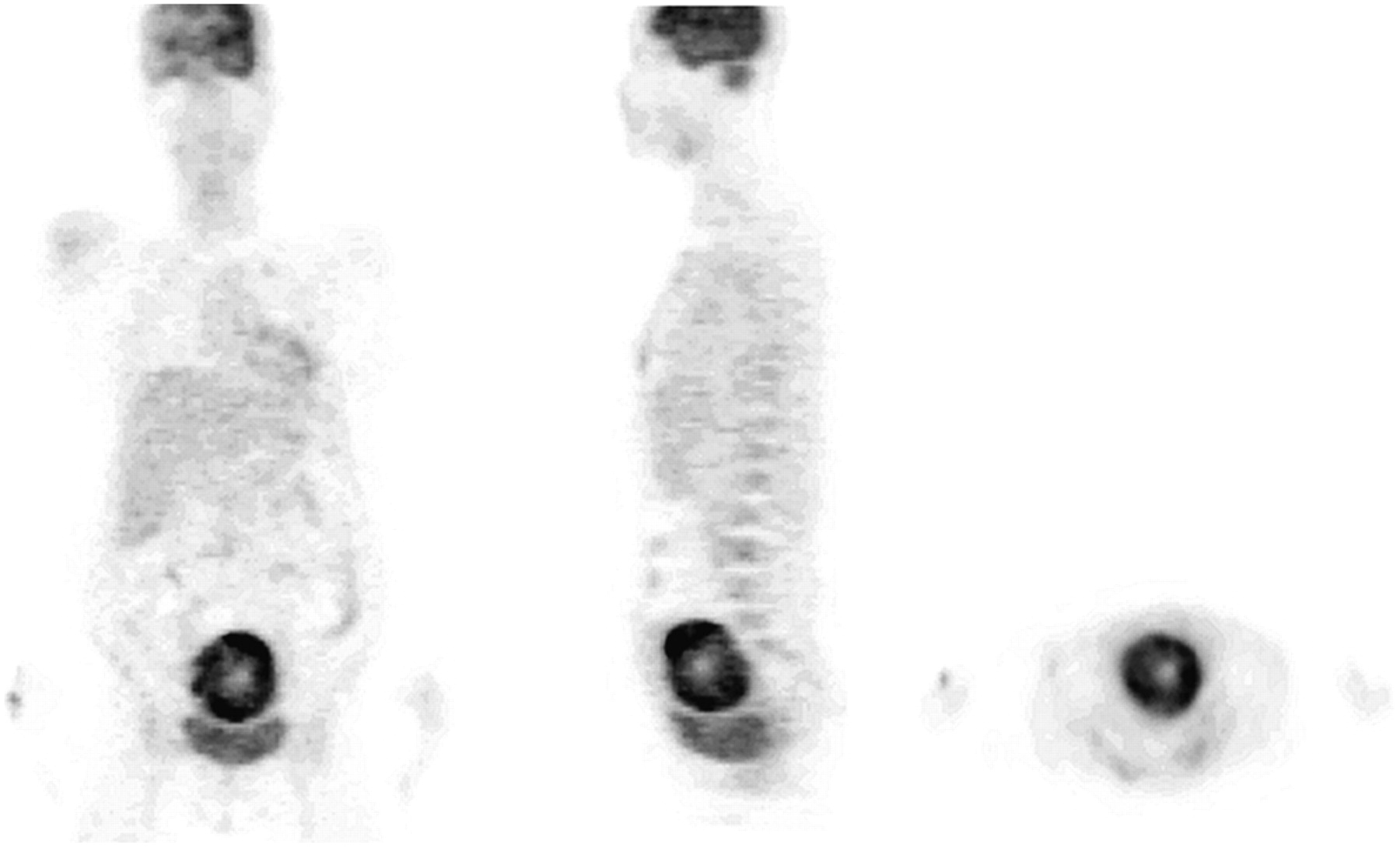
18F-FDG PET (from left to right: coronal, sagittal, and transversal slices) of 52-y-old patient with FUO caused by uterine rhabdomyosarcoma. Ringlike supravesical 18F-FDG uptake (maximum standardized uptake value, 15.8) was clearly higher than usually seen in benign uterine leiomyoma, which had been clinically suggested until PET evaluation was performed. Body temperature normalized after surgery. In addition, right hemispheric uptake in brain was reduced because of vascular stroke 4 y previously.
SUMMARY AND FUTURE PROSPECTS
Although 18F-FDG PET is a state-of-the-art procedure for the assessment of multiple malignancies, it is still not used as a routine procedure in the work-up of FUO. PET has the potential to replace other imaging techniques in the evaluation of these patients. Compared with labeled WBCs, 18F-FDG PET allows diagnosis of a wider spectrum of diseases. Compared with 67Ga-citrate scanning, 18F-FDG PET seems to be more sensitive. In addition, the diagnosis can be obtained much earlier with PET than with any other radiotracer technique.
A negative aspect of 18F-FDG PET is the limited anatomic information provided. It is expected that PET/CT will improve the diagnostic impact of 18F-FDG PET in the context of FUO, as already shown in the oncologic context, mainly by improving the specificity of the method.
Even though the results of previous studies are promising, many challenges remain for further evaluation:
Multicentric studies on a large population of FUO patients using a structured protocol and 18F-FDG PET as a second-line investigation are warranted.
The full impact of 18F-FDG PET in several infectious and noninfectious inflammatory diseases has to be prospectively evaluated in larger series.
Promising results about the use of 18F-FDG–labeled WBCs and 18F-FDG PET/CT are already available (23). In a small series, the method was successful in the diagnosis of soft-tissue, musculoskeletal, and abdominal infections. In a study comparing 18F-FDG–labeled WBCs with 111In-labeled WBCs in infection, the 2 methods showed comparable diagnostic accuracy (92). Whether 18F-FDG–labeled WBCs could have advantages over 18F-FDG PET in FUO patients remains to be determined.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH JANUARY 2008.
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.
- 5.↵
- 6.
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.
- 32.
- 33.
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.
- 60.
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.
- 77.
- 78.
- 79.
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- Received for publication June 22, 2006.
- Accepted for publication October 12, 2006.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The value of 18F-FDG-PET/CT in identifying the cause of fever of unknown origin (FUO) and inflammation of unknown origin (IUO): data from a prospective study
- Combined Parthenolide and Balsalazide Have Enhanced Antitumor Efficacy Through Blockade of NF-{kappa}B Activation
- Undiagnosed cardiac sarcoidosis presenting as complete heart block and ventricular arrhythmia
- 18F-FDG PET and PET/CT in Diagnosis and Treatment Monitoring of Pyrexia of Unknown Origin Due to Tuberculosis with Prominent Hepatosplenic Involvement
- Metabolic Activity of the Spleen and Bone Marrow in Patients With Acute Myocardial Infarction Evaluated by 18F-Fluorodeoxyglucose Positron Emission Tomograpic Imaging
- Advanced Imaging of Cardiac Sarcoidosis
- Diagnostic workup for fever of unknown origin: a multicenter collaborative retrospective study
- Positron Emission Tomography/Computed Tomography for Diagnosis of Prosthetic Valve Endocarditis: Increased Valvular 18F-Fluorodeoxyglucose Uptake as a Novel Major Criterion
- Translational 18F-FDG PET/CT Imaging to Monitor Lesion Activity in Intestinal Inflammation
- Inhibition of Development of Abdominal Aortic Aneurysm by Glycolysis Restriction
- Imaging Infection and Inflammation in Children with 18F-FDG PET and 18F-FDG PET/CT
- Positron-Emission Computed Tomography in Cyst Infection Diagnosis in Patients with Autosomal Dominant Polycystic Kidney Disease
- Subacute Thyroiditis Presenting as a Focal Lesion on [18F] Fluorodeoxyglucose Whole-Body Positron-Emission Tomography/CT
- Evaluation of Metabolic Characteristics and Viability of Lipiodolized Hepatocellular Carcinomas Using 18F-FDG PET/CT
- Potential of Noninvasive Serial Assessment of Acute Renal Allograft Rejection by 18F-FDG PET to Monitor Treatment Efficiency
- Contribution of the 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography to the diagnosis of primary osseous Hodgkin lymphoma
- Idiopathic Pulmonary Fibrosis and Diffuse Parenchymal Lung Disease: Implications from Initial Experience with 18F-FDG PET/CT
- The Role of 18F-FDG PET/CT in the Evaluation of Ascites of Undetermined Origin
- Fever of Unknown Origin: The Role of 18F-FDG PET/CT
- Assessment of Large-Vessel Involvement in Giant Cell Arteritis with 18F-FDG PET: Introducing an ROC-Analysis-Based Cutoff Ratio