


Abstract
The aim of this study was to investigate the diagnostic accuracy and impact on patient management of the new integrated PET/CT modality in patients with suspected iodine-negative, differentiated thyroid carcinoma (DTC). Methods: Forty patients with DTC and a suggestion of iodine-negative tumor tissue underwent PET/CT examination (370 MBq 18F-FDG, coregistered PET/CT whole-body images). As the first step of analysis, PET and CT images were scored blindly and independently by 2 nuclear medicine physicians and 2 radiologists. A 5-point scale was used. The second step consisted of a consensus reading, during which a virtual side-by-side fusion of PET and CT images was initially evaluated and afterward the “real” fusion (i.e., coregistered) PET/CT images were also scored with the same 5-point scale. The imaging results were compared with histopathologic findings and the course of disease during further follow-up examinations. Results: One hundred twenty-seven lesions in 40 patients were evaluated. Diagnostic accuracy was 93% and 78% for PET/CT and PET, respectively (P = 0.049, per-patient analysis). In 17 (74%) of 23 patients with suspicious 18F-FDG foci, integrated PET/CT added relevant information to the side-by-side interpretation of PET and CT images by precisely localizing the lesion(s). In tumor-positive PET patients, PET/CT fusion by coregistration led to a change of therapy in 10 (48%) patients. Futile surgery was prevented in an additional 3 patients. Conclusion: Integrated PET/CT is able to improve diagnostic accuracy in a therapeutically relevant way in patients with iodine-negative DTC. By precisely localizing tumor tissue, image fusion by integrated PET/CT is clearly superior to side-by-side interpretation of PET and CT images.
Differentiated thyroid cancer (DTC) occurs in 3–5 per 100,000 people and represents about 1% of all malignant tumors (1). In most cases, prognosis is favorable and treatment consisting of primary surgery and ablative radioiodine administration achieves a 10-y survival rate of 80%–90% (2). However, special subgroups of patients demonstrate a less favorable course of disease with much lower survival rates. Risk factors are an age of >45 y, histopathologic grading, and poor radioiodine accumulation (3,4). Those patients without sufficient radioiodine uptake in the tumor cells have a significantly lower survival rate if distant metastases are present (3).
Low expression of the sodium-iodine symporter seems to be one main reason for the lack of iodine uptake that may be present at primary diagnosis or that develops during the further course of disease (5). Patients with DTC may have only iodine-negative tumor lesions or both iodine-negative and iodine-positive tumor tissue (6). Consequently, the presence of iodine-negative tumor tissue decreases the accuracy of iodine scintigraphy, which is routinely used for staging and restaging patients. This can lead to the situation in which tumor tissue is not detected by iodine scintigraphy and will remain without further treatment (7).
PET with 18F-FDG has been able to improve the diagnostic work-up of these patients with iodine-negative DTC (6,7). Studies on the value of 18F-FDG PET for DTC have concentrated on patients in whom radioiodine scintigraphy is negative but metastatic spread is associated with an increase of thyroglobulin (TG) level or unclear morphologic findings. It has been shown that 18F-FDG PET is the most accurate method in this situation, and sensitivities and specificities range between 85% and 94% (7–11). For the treatment of iodine-negative tumor tissue, surgery is the only curative therapy option. Exact localization of 18F-FDG tumor foci is mandatory for successful resection of cancer in these cases.
Integrated PET/CT is a new imaging modality that might have advantages over the diagnostic work-up by PET alone or by separate PET and morphologic imaging. We hypothesized that the diagnostic accuracy of integrated PET/CT would be significantly higher than that of PET alone or of side-by-side PET and CT. The more accurate definition of tumor location should also result in better decision making for therapy.
MATERIALS AND METHODS
Patients and Design of Study
We included patients with histopathologically proven DTC who were suspected of having iodine-negative tumor tissue. Each patient had to meet the following inclusion criteria: elevated TG level in the euthyroid and also the hypothyroid state (>3 ng/mL) or morphologically suspected tumor disease (sonography, CT, MRI), l-thyroxin withdrawal for 4 wk before 131I whole-body scintigraphy, low-iodine diet during this period, thyroid-stimulating hormone increase of >30 mU/L, performance of evaluable γ-camera 131I whole-body scintigraphy meeting high-quality requirements, decision of a nuclear medicine physician (not involved in data evaluation) that no pathologic accumulation of radioiodine could be found on whole-body scintigraphy, previous total thyroidectomy, and radioiodine ablation. Exclusion criteria were as follows: positive test for TG antibodies, administration of CT contrast medium within the previous 6 mo, positive iodine urine test performed on the day of scintigraphy, pregnancy, or an age of <18 y.
This was a prospective study. The findings of PET, CT, and fused imaging were compared with histopathology (tumor grading (4)) or clinical follow-up results as a gold standard. The evaluation of imaging was performed directly after imaging, and the results were used for further clinical decision making. All patients were informed about the study and had given written consent according to the Declaration of Helsinki. The ethical committee and the radiation safety committee had given approval.
Imaging
All data were acquired with a combined PET/CT in-line system (Biograph; Siemens Medical Solutions). This camera integrates a PET scanner (Ecat HR+; Siemens) with a dual-section helical CT scanner (Somatom; Siemens) and allows the acquisition of coregistered CT and PET images in one session.
All patients were studied (also for PET/CT) after a 4-wk withdrawal of l-thyroxin (first a 2-wk substitution with triiodothyronine, then complete withdrawal). 131I whole-body scintigraphy was performed 3–4 d after administration of 370 or 1,110 MBq 131I using a standard γ-camera with high-energy collimator. The interval between 131I scintigraphy and PET/CT was 1 wk.
The patients fasted at least 4 h before injection of 370 MBq 18F-FDG. Scanning was started 60–90 min after the injection (5–7 bed positions; acquisition time, 5 min/bed position). Blood glucose levels did not exceed 150 mg/dL (8.3 mmol/L). No intravenous contrast agent was administered. Initially, patients were examined in the supine position with arms elevated, and CT scanning was started at the level of the cervicothoracic region with the following parameters: 40 mAs; 130 kV; slice thickness, 2.5 mm; pitch, 1.5. The CT scans were acquired during breath holding within the normal expiration position and reached caudally to the midthigh. PET over the same region was performed immediately after acquisition of the CT images (5 min/bed position). Afterward, a second data acquisition set from the base of the skull to the upper thoracic region was initiated with the patient's arms positioned next to the body. For this second part of the examination, the same parameters were used for CT and PET. The CT data were used for attenuation correction, and images were reconstructed as 5-mm slices applying a standard iterative algorithm (ordered-subset expectation maximization).
Interpretation
Images were interpreted at a workstation equipped with fusion software (Syngo; Siemens) that provides multiplanar reformatted images and enables display of the PET images (with and without attenuation correction), CT images, and fused PET/CT images in any percentage relation.
Analysis of images was performed as a multistep image interpretation (12). During the first step of analysis, PET and CT images were scored blindly and independently by 2 nuclear medicine physicians and 2 radiologists. For this purpose, a 5-point scale was used: a score of 0 indicated that the lesion was normal; a score of 1 indicated that the lesion was probably normal; a score of 2 indicated that the lesion was equivocal; a score of 3 indicated that the lesion was probably abnormal; and a score of 4 indicated that the lesion was abnormal.
The second step of data analysis consisted of a consensus reading by both groups. During the consensus reading, first a virtual (meaning mental) fusion of PET and CT images was scored on the 5-point scale; afterward, the “real” fusion (i.e., coregistered) PET/CT images were also scored with the same 5-point scale. The 5-point interpretation was applied to every lesion as well as to the patient. If no consensus was achieved, the results were to be part of a special-case analysis.
A lesion was categorized as 0 or 1 if it did not follow the physiologic 18F-FDG uptake patterns and was not thought to represent a tumor site. These lesions showed uptake of low intensity or were located at the anatomic regions of organs or structures that can be associated with nontumoral 18F-FDG uptake, such as blood vessels, a field of recent surgery, vocal cords (symmetric uptake), salivary glands, and brown fat tissue. Lesions categorized as 3 or 4 had focal uptake of high intensity and were assigned to one of the anatomic areas described below. If readers could not decide whether a lesion was benign or malignant on the basis of the previous criteria, the lesion was classified as 2.
Interpretation of separate PET and CT images, of side-by-side PET and CT images, and of fused PET/CT images also included the anatomic localization of 18F-FDG uptake sites. The following regions were used for anatomic assignment of tumor lesions: midline of neck (upper, medium, lower third), cervicolateral (upper, medium, lower third), pretracheal/prelaryngeal, lateral to the trachea, retrotracheal/retrolaryngeal, supraclavicular, mediastinal (upper, medium, lower third), hilar, lung (upper, medium, lower third, ventrally/dorsally located), and bone as appropriate.
A lesion was considered as true-positive if the score was 2–4 and if histopathology was positive or if it showed progression at follow-up sessions. A finding was considered as true-negative (score of 0–1) if histology was negative or if follow-up examinations did not show any pathologic result in the region of concern for at least 18 mo. A lesion was considered as false-positive if the score was 2–4 and if histopathology was negative or if it showed no progression at follow-up sessions. A finding was considered as false-negative if the score was 0–1 and if histology was positive or if follow-up examinations showed growth of the lesion(s). Follow-up examinations were performed every 3–6 mo and consisted basically of measurement of TG levels and sonography of the neck. In the case of elevated TG levels but no suspicious findings on sonography, additional investigations were performed as indicated: bone scintigraphy with 99mTc-methylene diphosphonate, CT of the thorax, CT/MRI of the neck and mediastinum, or repeated PET/CT. If sonography revealed suggestive lesions, it served as the further follow-up method to determine whether progression was present. If suspected tumor lesions were visualized, or better visualized, by only one of the imaging modalities, definition of progress or nonprogress was met by analyzing exclusively this single modality. In the case of different tumor sites, several imaging modalities were used as appropriate for the specific region.
Interpretation of side-by-side PET and CT and of fused PET/CT images also included a special analysis of anatomic localization of 18F-FDG uptake sites in addition to the categorization. Localizations with 18F-FDG accumulation scored 2 or higher were related to a definite anatomic structure on CT images during side-by-side analysis. For definite comparison of feasibility for localizing lesions, the location of lesions as demonstrated by side-by-side interpretation was compared with the lesion location on fused images. For verification of the localization accuracy, surgical reports and histology as well as imaging procedures during follow-up were used as the gold standard.
Additional information obtained by integrated PET/CT images was considered as diagnostically relevant if one or more of the following criteria were met: anatomic location of suspicious lesion was not truly indicated by side-by-side interpretation but by fused imaging, new tumor sites were diagnosed by fused imaging, or false-positive lesions were identified as true-negative by fused imaging. A finding was considered as therapeutically relevant if it resulted in the prevention of surgery or if reduction of tumor volume could be enhanced by extension of surgical resection to areas that would not have been included in a standard resection. Lymph node dissection of the lateral and central cervical compartment was considered as the standard surgical procedure.
Statistical Analysis
The sensitivity, specificity, negative predictive value, positive predictive value, and accuracy of PET alone and PET/CT were calculated on the basis of the true-positive and true-negative findings as described in the same anatomic region with a lesion-based and a patient-based analysis. The McNemar test (χ2 test) was used for comparison of the sensitivity and specificity of PET alone with those of fused PET/CT (and for calculation of localizing accuracy comparing side-by-side PET and CT with fused PET/CT) with a confidence level of 95% (P < 0.05 was considered significant).
RESULTS
No patient refused to enter the study, but 2 patients had to be excluded because of a positive iodine urine test.
Forty patients were included in the study (23 papillary and 17 follicular cancers). The patient characteristics are given in Table 1. After total thyroidectomy, 6 patients were suspected of having iodine-negative tumors because oxyphilic tumor cells were present in the primary tumor. Thirty-four patients were included because of elevated TG levels and negative iodine scintigraphy. All of these patients underwent previous total thyroidectomy and ablative radioiodine treatment. Histology and clinical follow-up served as the gold standard in 17 and 23 cases, respectively. There were 19 tumor-positive and 21 tumor-negative patients as classified by the gold standard. Thirteen patients had either local recurrence or lymph node metastases without distant metastatic disease. Five patients showed both lymph node and distant metastases (lung, bone), and 1 patient demonstrated exclusively lung metastases. No patient study was excluded from primary analysis because of disagreement on the consensus reading. For the evaluation of lymph nodes and local recurrence, 70 lesions were analyzed, as shown in Table 2. For the evaluation of distant metastases, 57 lesions were scored, as shown in Table 3.
Patient Characteristics
Comparison of PET/CT and PET in Interpretation of Lymph Nodes and Local Soft-Tissue Recurrence on a Lesion Basis
Comparison of PET/CT and PET in Interpretation of Distant Metastases on a Lesion Basis
Sensitivity, specificity, positive and negative predictive values, and diagnostic accuracy on a per-patient basis are given in Tables 4 and 5.
Detection of Local Disease/Lymph Node Metastases (T and N Staging) and Distant Metastases (M Staging) as well as Overall Parameters on a Per-Patient Basis
Probabilities for Different Imaging Modalities on a Per-Patient Basis
PET and PET/CT
Comparing PET and fused PET/CT images, 47 lesions were classified as true-positive in a group of 19 tumor patients. Thirty-two true-negative lesions were found in 21 tumor-negative patients.
False-negative findings on PET were observed in 3 of 4 patients with lung metastases. In these 3 patients, 37 lung metastases that had a diameter of <5 mm were identified on CT images of PET/CT. These 3 patients with lung metastases showed additional regional disease (1 with lymph node metastases, 2 with local recurrences) accumulating 18F-FDG with high intensity. One of the 4 patients with iodine-negative lung disease showed a true-positive PET finding indicating 2 solid lung metastases, which were removed surgically.
False-positive findings on PET and PET/CT (also side-by-side PET and CT) were found in 2 patients (total of 5 lesions) revealing 18F-FDG uptake in bilateral hilar lymph nodes due to sarcoidosis and in acute inflammatory cervical lymph nodes. PET showed an additional 3 false-positive patients who were also false-positive with side-by-side PET and CT.
For the T and N staging, PET alone and PET/CT showed the same sensitivity but PET/CT had a higher specificity (91%) than PET (76%). However, this was not statistically significant (P = 0.2). For M staging, the sensitivity and specificity of PET/CT (100% each) was higher than the probabilities of PET (84% and 95%). The differences were not significant for sensitivity (P = 0.07) and specificity (P = 0.14) on a per-patient basis but were significant on a per-lesion analysis for sensitivity (P < 0.001).
For overall staging, the sensitivity and specificity of PET/CT (95% and 91%, respectively) were also better than those of PET (79% and 76%, respectively). The differences were not significant for sensitivity (P = 0.15) and specificity (P = 0.2). However, diagnostic overall accuracy was significantly better for PET/CT (93%) than that for PET alone (78%) (P = 0.049). When diagnostic accuracy was calculated on a per-lesion basis, there were 121 and 79 true findings (sum of true-positive and true-negative findings of a total of 127 lesions) for PET/CT and PET, respectively. This difference was highly significant (P < 0.0001).
Of the 6 patients with Hürthle cell carcinoma at primary diagnosis, 2 had high 18F-FDG accumulation in lymph node metastases. One patient showed a false-negative finding on PET as well on PET/CT at a site of a mediastinal lymph node metastasis that demonstrated iodine uptake under ablative therapy.
Side-by-Side PET and CT and PET/CT: Therapeutic Relevance
Side-by-side PET and CT interpretation led to discordant results in 73 (57%) of 127 lesions in different anatomic regions (Table 6).
Location and Number of Discordant Findings on Side-by-Side Interpretation of PET and CT Images
Looking at side-by-side PET and CT image and fused PET/CT image interpretation, the location of lesions was tested in 23 patients in whom positive findings were present and the gold standard allowed verification of the exact anatomic location. This group comprised the 15 true-positive 18F-FDG PET tumor patients, 3 patients with lung metastases who also had local 18F-FDG–positive disease, the 3 patients with false-positive PET findings, and also 2 patients with both false-positive PET and PET/CT findings. In this group, side-by-side PET and CT were able to truly localize lesions in only 4 patients, whereas fused PET/CT correctly localized lesions in 21 patients. This difference was highly significant (P < 0.001). In the 18 true-positive PET/CT patients, histology results were available as a gold standard in all but 1 patient, in whom follow-up was used. Side-by-side interpretation could precisely identify the lesion localization in 4 of 18 patients (1 patient with solid lung metastases, 1 patient with a bone metastasis and a lymph node metastasis, 2 patients with lymph node metastases).
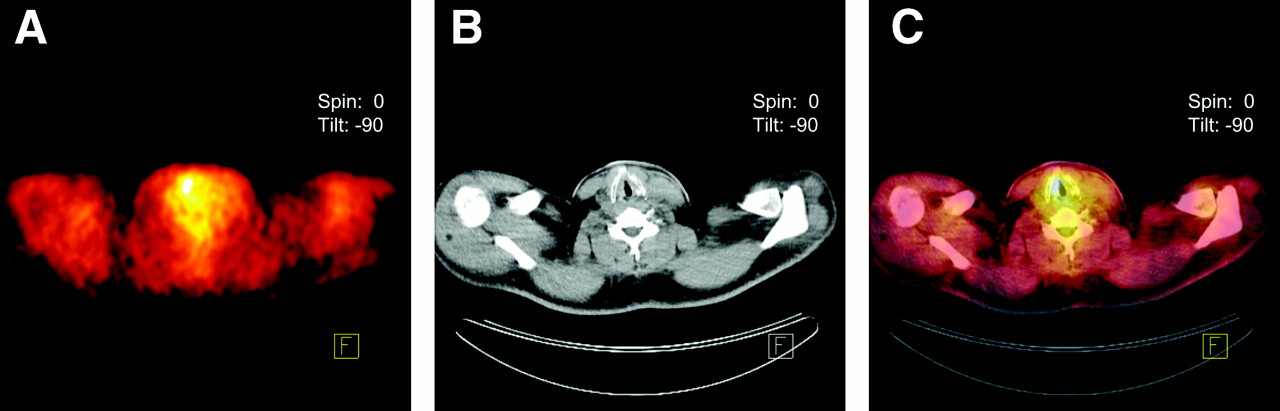
In 17 (74%) of the 23 patients with suggestive 18F-FDG PET findings, fused PET/CT correctly localized the site of the lesion(s), which was not possible by side-by-side interpretation of both methods. This group also comprises the 3 patients with 5 lesions for which fused PET/CT led to a conversion of false-positive findings into true-negative findings. This results in a probability of 60% (3/5) for conversion by fused PET/CT if PET presents a false 18F-FDG–positive patient. These 3 patients did not undergo surgery because PET/CT identified false-positive PET findings (that were also false-positive with side-by-side PET and CT, showing 4 false-positive local findings and 1 false-positive distant finding). One of these 3 patients demonstrated a focal, unilateral cervical 18F-FDG accumulation, with CT showing only normal-sized lymph nodes (misinterpreted as lymph node metastasis). The 18F-FDG accumulation could be identified on PET/CT as uptake in a cervical joint. Furthermore, this young patient revealed intense, unilateral 18F-FDG uptake in the lower abdomen (misinterpreted as distant metastasis by side-by-side PET and CT) that was identified as physiologic ovary accumulation by PET/CT. The second patient was scored as suspicious for local recurrence and supraclavicular lymph node metastasis on side-by-side PET and CT. By image overlay with PET/CT, these findings were truly categorized as benign findings corresponding to unilateral accumulation at the vocal cords (Fig. 1) and to 18F-FDG accumulation at the sternoclavicular joint due to degenerative alterations. The third patient demonstrated an intense 18F-FDG uptake near her tracheostomy that was misinterpreted on side-by-side PET and CT but not on PET/CT. During follow-up of these 3 patients over >2 y, no increase of TG levels was measured, confirming that no recurrent tumor was present at the time of imaging.
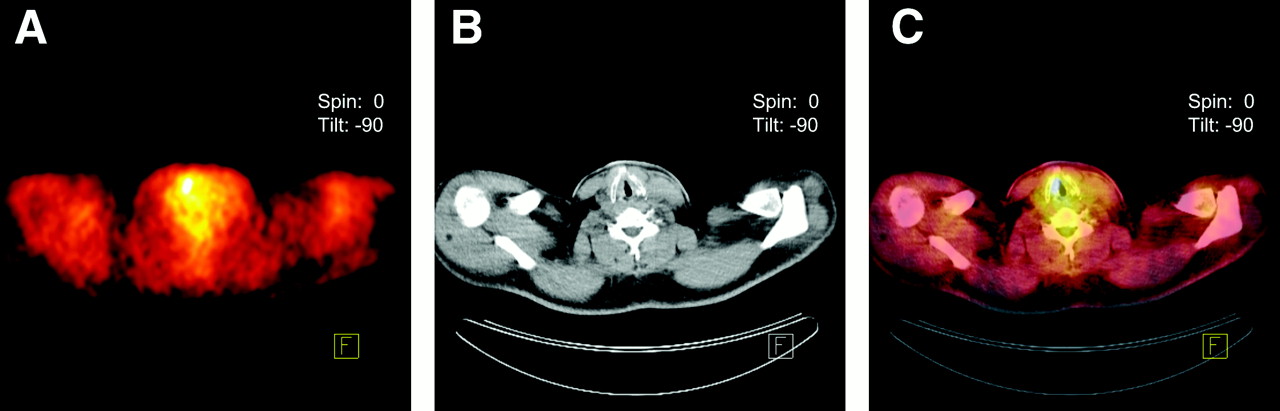
A 56-y-old patient (Hürthle cell pT2 N0 M0, previous lymph node recurrence), with elevated TG level and no iodine accumulation, who showed pathologic 18F-FDG uptake in the right lower cervical region (A). Corresponding CT slices did not reveal any abnormality (B). PET/CT images (C) clearly showed that the PET finding was located on the right vocal cord and corresponded to benign, muscular uptake. No surgery was scheduled and follow-up confirmed this benign finding.
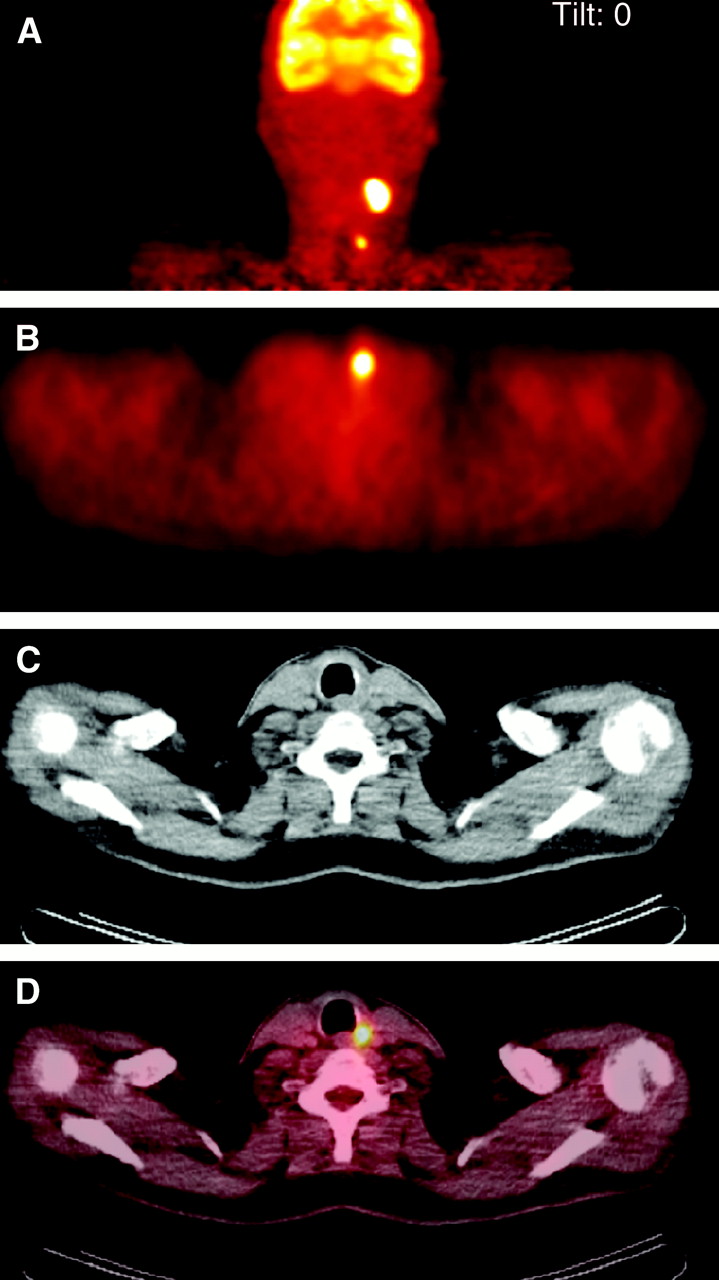
Of 13 patients with lymph node metastases or local recurrence but without distant metastases, 12 were true-positive on 18F-FDG PET. In 2 of these 12 patients, side-by-side interpretation could precisely determine the anatomic location of the lesion. Imaging localization was possible only on fused PET/CT in the remaining 10 patients, of whom CT abnormalities were found in 7 (lymph node enlargement) and no abnormality was found in 3 (Fig. 2). In these 10 patients, the surgical resection of iodine-negative and 18F-FDG–positive tumor tissue was extended to additional regions after PET/CT clearly identified the location of tumor lesions (Table 7). This resulted in a normalization of the TG level after surgery in 5 patients in whom complete tumor volume resection was achieved, as confirmed by control PET/CT. In the other 5 patients, a marked decrease in the TG level and a tumor volume reduction of 50%–90% was observed, as calculated by control PET/CT (4 patients) and MRI (1 patient) measurements.

A 58-y-old patient (oxyphilic, follicular, pT3 N0 M0 G2), who had undergone total thyroidectomy and ablative radioiodine treatment 2 y earlier, presented with markedly elevated TG level but without any iodine accumulation. Sonography-guided fine-needle aspiration biopsy of a suggestive cervical lymph node revealed cells suggestive of tumor. Preoperative PET showed intense 18F-FDG uptake in the suspected, left cervical lymph node as demonstrated on the coronal slice (A). However, PET detected a second tumor focus that was located more caudally. For this second tumor, shown on the transverse PET slice (B), no corresponding abnormality could be localized on CT images (C). Only by fusion of PET and CT images (D) could the second lesion be precisely identified (located between esophagus and dorsolateral trachea) and be removed surgically. Histopathology revealed a 5-mm lymph node metastasis. At 2 y after surgery, the patient had no tumor recurrence.
Details of Ten 18F-FDG– and Tumor-Positive Patients in Whom PET/CT, but Not Side-by-Side PET and CT, Led to Change in Therapy
In summary, in 10 (48%) of 21 patients with true-positive PET findings, only fused PET/CT revealed residual tumor and could help to enhance tumor volume resection in a relevant way. In 3 additional patients, futile surgery was prevented because of PET/CT. Thus, overall, a change in treatment achieved by fused PET/CT was observed in 13 of the investigated patients.
DISCUSSION
Patients with DTC have a less favorable prognosis if radioiodine-negative tumor tissue, especially in distant metastases, is present (13). One reason for this may be that these cancers are not detected by routine diagnostic work-up with 131I scintigraphy and they cannot be treated efficiently by radioiodine therapy. Therefore, tumor cells will continue to grow undetected and the chance of cure decreases significantly. The presence of tumor tissue with no 131I accumulation is suspected at the time of primary diagnosis if histopathology reveals the so-called Hürthle cell tumor. More often, the suspicion for iodine-negative tumor cells comes up later during the course of the disease after the ablative treatment with radioiodine has been completed. In this case, TG levels increase, with no suggestive findings on 131I scintigraphy.
It was shown recently that 18F-FDG PET is able to reveal iodine-negative tumor tissue with a diagnostic accuracy that is higher than that of other imaging modalities (7). In our study, the overall sensitivity and specificity for the detection of tumor tissue by 18F-FDG PET were 79% and 76%, respectively. These values are within the range of the diagnostic accuracies that have been reported previously by others demonstrating a sensitivity and specificity of 80%–95% and 70%–85%, respectively (6–11). The lower sensitivity in our group might be explained by the 3 patients with false-negative lung metastases.
One limitation of 18F-FDG PET, especially in the region of the neck, is the possibility of false-positive 18F-FDG accumulations leading to the diagnosis of lymph node metastases and, consequently, to the potential scheduling of a futile operation (14). In our study, specificity for detecting lymph node metastases could be increased by PET/CT in comparison with PET alone and side-by-side PET and CT (from 76% to 91%). Three patients (60% of the cervical false-positive findings) were identified on PET/CT as having a physiologic or nontumoral cervical 18F-FDG accumulation that was classified as lymph node metastases by PET alone and side-by-side PET and CT.
Although sensitivity on a per-patient basis for lymph node metastasis detection was equal for PET and PET/CT, sensitivity for M staging was increased from 84% to 100% on PET/CT. This was achieved in 3 patients by PET/CT detection of small and miliary lung metastases that were not diagnosed by PET alone. This confirms the findings of previously reported studies showing that 18F-FDG PET is not able to adequately assess miliary lung metastases smaller than 6 mm. It is unclear whether this is generated from motion artifacts on inspiration and expiration or from a lower metabolic activity of the lung metastases (15).
One important aspect of our study was evaluation of the therapeutic relevance of PET/CT. In clinical routine, treatment of DTC is dominated by the combination of surgical tumor removal and subsequent application of radioiodine (16). Whereas this approach is almost optimal for patients with iodine-accumulating tumors, it is inappropriate if only iodine-negative tumors are present. In this case, complete surgical removal of iodine-negative tissue is the only curative treatment option. Furthermore, it seems important to diagnose and remove iodine-negative tumor tissue as early as possible because prognosis of this tumor subgroup is essentially worse than that of most DTCs (13). Therefore, it is crucial to be able to precisely localize an iodine-negative and 18F-FDG PET–positive tumor to enhance complete resection and cure of the patient (17–19). For this purpose, additional morphologic imaging is necessary to help localize the 18F-FDG–positive focus.
To determine whether PET/CT would be helpful in this situation, we performed a second analysis and compared it with a side-by-side interpretation of PET and CT images. This side-by-side interpretation revealed that 57% (73/127) of all scored lesions in different anatomic regions were discordant. One reason for this is a positive PET finding without a corresponding CT finding—for example, when the lymph nodes of the affected area are not enlarged or when CT images show an abnormality at a different anatomic region. In this situation, it is not possible to precisely localize the suspected tumor tissue for surgical resection. In our study, this situation was observed in 17 patients (74% of PET patients with suggestive lesions) in whom PET/CT could correctly localize the tumor, as confirmed by histopathology and follow-up. In this group, 3 patients were identified as having benign findings that prevented futile surgical treatment. In ten 18F-FDG–positive tumor patients, the surgical resection of iodine-negative tumor tissue was extended to additional regions after PET/CT clearly identified the location of tumor lesions that were not localized by side-by-side PET and CT. This resulted in an efficient tumor volume reduction by surgery. If only standard lymph node resection of the lateral and central compartment of the neck had been performed in this group, a relevant amount of 18F-FDG–positive tumor tissue would have been unnecessarily retained.
One limitation of our study seems to be that CT was performed without a contrast agent. However, in patients with DTC, CT is generally done without the application of a contrast agent to avoid blockage of iodine uptake. This also applies to patients in whom iodine-negative tissue is suspected, because iodine-negative and iodine-positive tissue may coexist in one patient. Another aspect is that diagnosis of lymph node metastases by morphologic imaging, including MRI and contrast-enhanced CT, is defined predominantly by the size of the nodes. Therefore, we strongly believe that, in patients with nonenlarged lymph nodes but positive 18F-FDG accumulation, the optimal strategy is fusion of images gained by integrated PET/CT irrespective of the use of a contrast agent. Another limitation of the study is that the minimal time for follow-up of patients was 18 mo. Although 18F-FDG avidity is a predictor of reduced survival (20), this study did not determine the outcome of therapy.
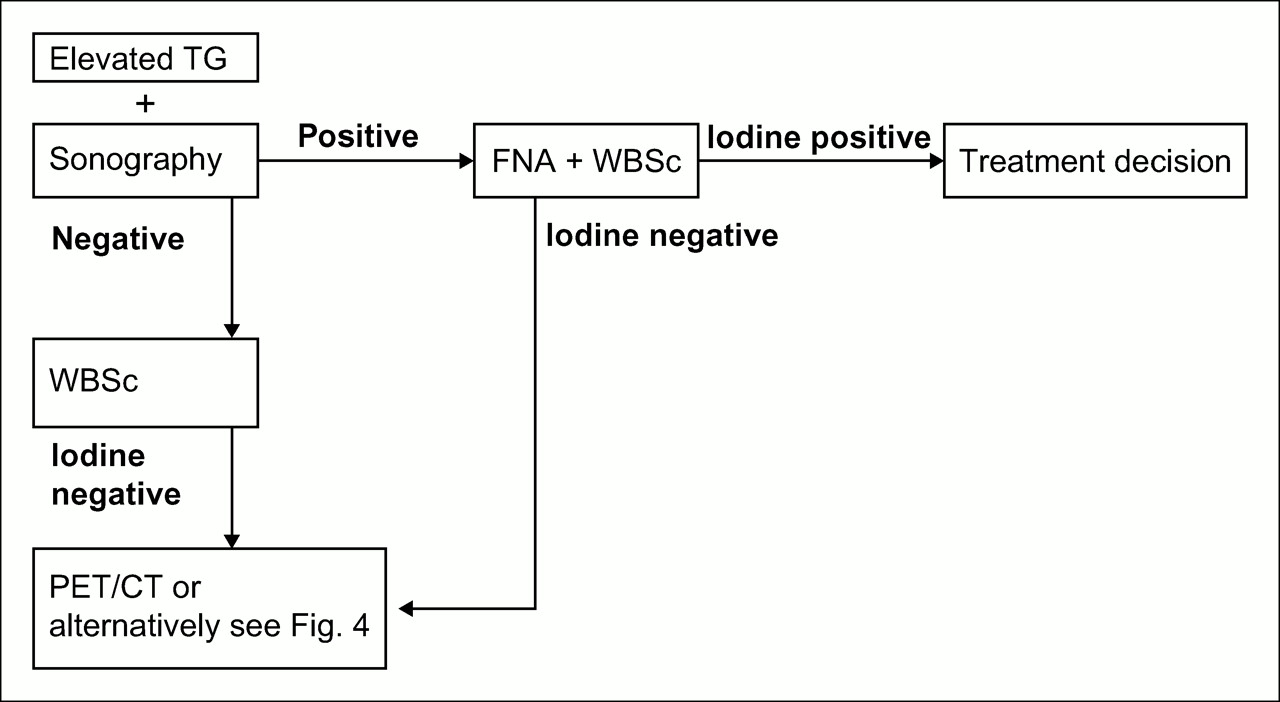
Overall, integrated PET/CT changed the treatment in 48% of patients with a true-positive 18F-FDG PET finding. Additionally, a futile operation was prevented in 3 patients. We consider these results as highly relevant for therapeutic decision making about patients with thyroid cancer and, therefore, would recommend a diagnostic algorithm as shown in Figures 3 and 4. Thereafter, integrated PET/CT would be proposed in all patients in whom iodine-negative tumor tissue is suspected. Alternatively, separated PET and CT could be performed initially, followed by integrated PET/CT only in cases of discordant findings.
Algorithm for clinical use of integrated PET/CT with 18F-FDG in DTC patients. FNA = fine-needle aspiration; WBSc = whole-body scintigraphy.

Alternative to PET/CT following the algorithm in Figure 3.
CONCLUSION
Integrated PET/CT is able to improve diagnostic accuracy in a therapeutically relevant way in patients with iodine-negative DTC. Of tumor-positive PET patients, PET/CT will lead to a change of therapy in about one half. By precisely localizing tumor tissue, image fusion by integrated PET/CT is clearly superior to side-by-side interpretation of PET and CT images.
Acknowledgments
We thank Siemens Medical Solutions for financial support for publishing the color images.
References
- Received for publication June 26, 2005.
- Accepted for publication November 7, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SNMMI Procedure Standard for Scintigraphy for Differentiated Thyroid Cancer
- 68Ga-DOTATOC PET/CT in Patients with Iodine- and 18F-FDG-Negative Differentiated Thyroid Carcinoma and Elevated Serum Thyroglobulin
- Clinical Utility of 18F-FDG PET/CT Concurrent with 131I Therapy in Intermediate-to-High-Risk Patients with Differentiated Thyroid Cancer: Dual-Center Experience with 286 Patients
- Increasing the yield of recombinant thyroid-stimulating hormone-stimulated 2-(18-fluoride)-flu-2-deoxy-D-glucose positron emission tomography-CT in patients with differentiated thyroid carcinoma
- Clinical Value of Integrated [18F]Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography/Computed Tomography in the Preoperative Assessment of Papillary Thyroid Carcinoma: Comparison With Sonography
- Hybrid SPECT-CT and PET-CT imaging of differentiated thyroid carcinoma
- 131I SPECT/CT in the Follow-up of Differentiated Thyroid Carcinoma: Incremental Value Versus Planar Imaging
- 18F-FDG PET/CT in Patients with Suspected Recurrent or Metastatic Well-Differentiated Thyroid Cancer
- Clinical Significance of Small Pulmonary Nodules with Little or No 18F-FDG Uptake on PET/CT Images of Patients with Nonthoracic Malignancies
- Improvements in Cancer Staging with PET/CT: Literature-Based Evidence as of September 2006
- Early Detection of Cancer Recurrence: 18F-FDG PET/CT Can Make a Difference in Diagnosis and Patient Care