


Abstract
Patients with differentiated thyroid carcinoma (DTC) are treated with 131I therapy after total thyroidectomy or surgical resection of recurrent tumor. However, some recurrent DTC lesions are not iodine-avid, which affects further treatment planning. The aim of this study was to evaluate the clinical benefit of 18F-FDG PET/CT performed concurrently with 131I therapy in DTC patients with intermediate to high risk. Methods: We retrospectively enrolled 286 DTC patients at 2 Korean medical centers who comprised 2 different patient groups: 28 patients who underwent adjuvant 131I treatment after curative surgical resection of recurrent tumor and 258 patients with intermediate to high risk who underwent 131I ablation after total thyroidectomy. 131I therapy and 18F-FDG PET/CT scanning were performed on the same day. Administration of l-thyroxine was withheld from all enrollees for 4 wk before 131I treatment. Results: In 39 patients (14%), 18F-FDG PET/CT detected additional recurrent or metastatic lesions that were not detected on the posttherapy 131I scan, and the treatment plan was changed for 30 patients (10%) based on such findings. Among the 28 patients receiving 131I treatment after resection of recurrent tumor, PET/CT detected additional lesions in 46%, and treatment was changed in 43%. Assessing a subgroup of stage T3–T4N1 patients with tumor size > 2.0 cm, among 258 patients undergoing 131I ablation after total thyroidectomy, we found that 25% had additional positive PET/CT results, and treatment changed for 17%. In contrast, 8% of stage T3–T4N1 patients with tumor size ≤ 2.0 cm, 6% of stage T1–T2N1 patients, and 3% of stage T3–T4N0 patients had additional positive PET/CT findings. Conclusion: 18F-FDG PET/CT performed concurrently with 131I therapy detected additional lesions in 14% of DTC patients and was particularly helpful for detecting additional lesions in patients undergoing 131I therapy after resection of recurrent tumor or in stage T3–T4N1 patients with tumor size > 2.0 cm.
The standard treatment protocol for differentiated thyroid carcinoma (DTC) is complete surgical resection of tumor lesions, followed by 131I therapy (1). 131I treatment has been shown to be beneficial in reducing cancer recurrence and cancer-specific mortality (2,3). However, in certain patients with DTC, the tumor cells lose their ability to trap iodine, including 131I. These iodine-negative tumor cells are not curable with 131I treatment. They are more aggressive and are associated with a poorer prognosis than tumors that can uptake iodine (4–6). The early detection of iodine-negative DTC lesions is important, because it triggers an adjustment in the treatment strategy: surgical resection, external-beam radiation therapy (EBRT), or multikinase inhibitor therapy will be selected rather than 131I treatment.
18F-FDG PET/CT is useful for the detection of recurrent DTC lesions, especially in patients with iodine-negative tumors and elevated serum thyroglobulin levels (6–10). Furthermore, recent studies showed that 18F-FDG PET can detect DTC lesions more accurately under thyroid-stimulating hormone (TSH) stimulation than under TSH suppression (11–13). Because 131I treatment is performed in the context of an elevated serum TSH level, concurrent 18F-FDG PET with 131I treatment could be beneficial for detecting recurrent DTC lesions, especially iodine-negative lesions, and for planning further treatment. However, there has been only one study to evaluate the role of 18F-FDG PET performed concurrently with 131I treatment under TSH stimulation (14).
In this study, we evaluated the usefulness of 18F-FDG PET/CT performed concurrently with 131I therapy for detecting DTC lesions in patients with intermediate to high risk at 2 Korean medical centers. Moreover, we evaluated the relationship between tumor factors and positive PET/CT findings to find which patient group would benefit most from this strategy.
MATERIALS AND METHODS
Patients
We reviewed the electronic medical records of all DTC patients who underwent 131I treatment at 2 Korean medical centers (Cheonan Soonchunhyang University Hospital [CSUH] and Jeju National University Hospital [JNUH]). Of these patients, we retrospectively enrolled 286 patients who underwent 18F-FDG PET/CT concurrently with 131I treatment. The enrolled patients comprised 2 different patient groups: those who underwent 131I ablation after total thyroidectomy and those who underwent adjuvant 131I treatment after intended curative surgical resection of recurrent neck lesions. Among the former group, only those with intermediate to high risk were enrolled, according to the guidelines of the American Thyroid Association (1). Patients with a history of malignant tumor other than DTC were excluded from the study. No patient had gross residual tumor lesions after an operation. The interval between an operation and 131I treatment ranged from 1 to 6 mo (median, 3 mo). The therapeutic 131I dose ranged from 3.7 GBq (100 mCi) to 7.4 GBq (200 mCi). In all patients, replacement of l-thyroxine (T4) was discontinued for 4 wk before 131I treatment, and patients received replacement l-triiodothyronine (T3) for the first 2 wk of this period. Additionally, all patients were on a low-iodine diet for at least 2 wk before the 131I therapy. Recombinant human TSH was not used in all patients. 18F-FDG PET/CT scanning was performed just before the 131I treatment, on the same day. At both medical centers, serum TSH, thyroglobulin, and antithyroglobulin antibody levels were measured in the collected blood samples on the day of 131I treatment using an electrochemiluminescence immunoassay. At the time of 131I treatment, all patients had serum TSH levels > 30 IU/mL. Whole-body 131I scans were obtained at 3–5 d and at 7–9 d after 131I treatment. All patients signed a written informed consent form for the 18F-FDG PET/CT and 131I treatment, and this study was approved by the Institutional Review Board of both medical centers.
18F-FDG PET/CT Scans
The 18F-FDG PET/CT scans were obtained using a Gemini PET/CT scanner (Philips) at CSUH and a Biograph 40 scanner (Siemens Medical Solutions) at JNUH. All patients were instructed to fast at least 6 h before the 18F-FDG administration. Patients were intravenously injected with 18F-FDG (5.18 MBq/kg for the Gemini scanner or 6.29 MBq/kg for the Biograph 40 scanner) 1 h before a PET/CT scan. First, CT images were acquired for attenuation correction without contrast enhancement. Then, PET images were acquired from the skull base to the proximal femur at 2.5 min per bed position for the Gemini scanner and at 2 min per bed position for the Biograph 40 scanner. PET images were reconstructed into a 128 × 128 matrix using an iterative algorithm with an attenuation correction.
Posttherapy 131I Scans
Posttherapy 131I whole-body scans were obtained using a large field-of-view dual-head γ-camera (Xeleris [GE Healthcare] at CSUH and Vertex V60 [ADAC] at JNUH) equipped with a medium-energy parallel-hole collimator. The continuous acquisition mode was used, with a scanning speed of 12 cm/min for the Xeleris camera and 13 cm/min for the Vertex V60 camera. Anterior and posterior whole-body images were acquired, and additional spot images were acquired where abnormal 131I uptake was shown on the whole-body images.
Image Analysis
All 18F-FDG PET/CT and posttherapy 131I whole-body images were visually assessed by 2 experienced nuclear medicine physicians. On posttherapy 131I scans, lesions showing abnormally increased 131I uptake other than remnant thyroid uptake or physiologic uptake were considered positive lesions. All lesions on PET/CT images were classified using a 4-point scale: 1, definitely benign, physiologic 18F-FDG uptake or lesions without abnormal 18F-FDG uptake; 2, probably benign, lesions with mild-to-moderate 18F-FDG uptake showing benign features on the CT images; 3, probably metastatic, lesions with mild-to-moderate 18F-FDG uptake showing indeterminate or malignant features on CT images or lesions with relatively high 18F-FDG uptake in comparison with size; and 4, definitely malignant, lesions with intense 18F-FDG uptake. The lesions with a score of 3 or 4 are classified as positive PET/CT lesions. The locations of positive lesions on both images were classified as thyroid bed, right neck, left neck, mediastinum, and other distant organs. All patients with positive findings on 18F-FDG PET/CT or 131I scans underwent further diagnostic work-up, and findings were determined to be true-positive when the lesions were histopathologically confirmed as recurrent or metastatic lesions of DTC or verified on subsequent follow-up imaging studies including ultrasonography, CT, PET/CT, or 131I scanning. If the true-positive lesions were only positive on 18F-FDG PET/CT and negative on 131I scans, patients were considered to have additional positive lesions on PET/CT. Furthermore, if the classified locations of true-positive lesions on PET/CT scans were incongruent with the positive lesions on 131I scans, the patients were considered to have additional positive lesions on PET/CT. If the classified locations of true-positive lesions on PET/CT and 131I scans were the same, the lesions were considered positive on both PET/CT and 131I scans, and the patients had no additional PET/CT lesions.
All enrolled patients were classified as having additional positive lesions on 18F-FDG PET/CT, the same positive lesions on PET/CT and 131I scans, positive lesions on 131I scans with negative PET/CT findings, and negative findings on both PET/CT and 131I scans. We calculated the ratios of patients with additional positive lesions on PET/CT and the ratio of patients with treatment change due to PET/CT findings. The treatment change was defined as abandonment of further 131I treatment or thyroid hormone suppression therapy in favor of surgical resection, EBRT, or multikinase inhibitor therapy. Afterward, tumor stage and size, patients’ age, and serum thyroglobulin level were evaluated as predictive factors for positive findings on PET/CT. The frequency of additional PET/CT lesions was compared among patients grouped according to the tumor stage and size and patients’ age using the χ2 and Fisher exact tests. Furthermore, the Mann–Whitney test was performed to compare the serum thyroglobulin level between patients with positive and negative PET/CT findings. All statistical analyses were performed with SPSS software (SPSS), and P values less than 0.05 were considered statistically significant.
RESULTS
Patient Characteristics
Characteristics of the enrolled 286 patients are summarized in Table 1. Of these patients, 258 (90%) underwent 131I ablation after total thyroidectomy. The remaining 28 patients (10%) underwent adjuvant 131I treatment after intended curative surgical resection of recurrent lesions. Distant metastatic lesions were found in 13 patients (5%) on 18F-FDG PET/CT or posttherapy 131I scans.
Characteristics of Study Subjects (n = 286)
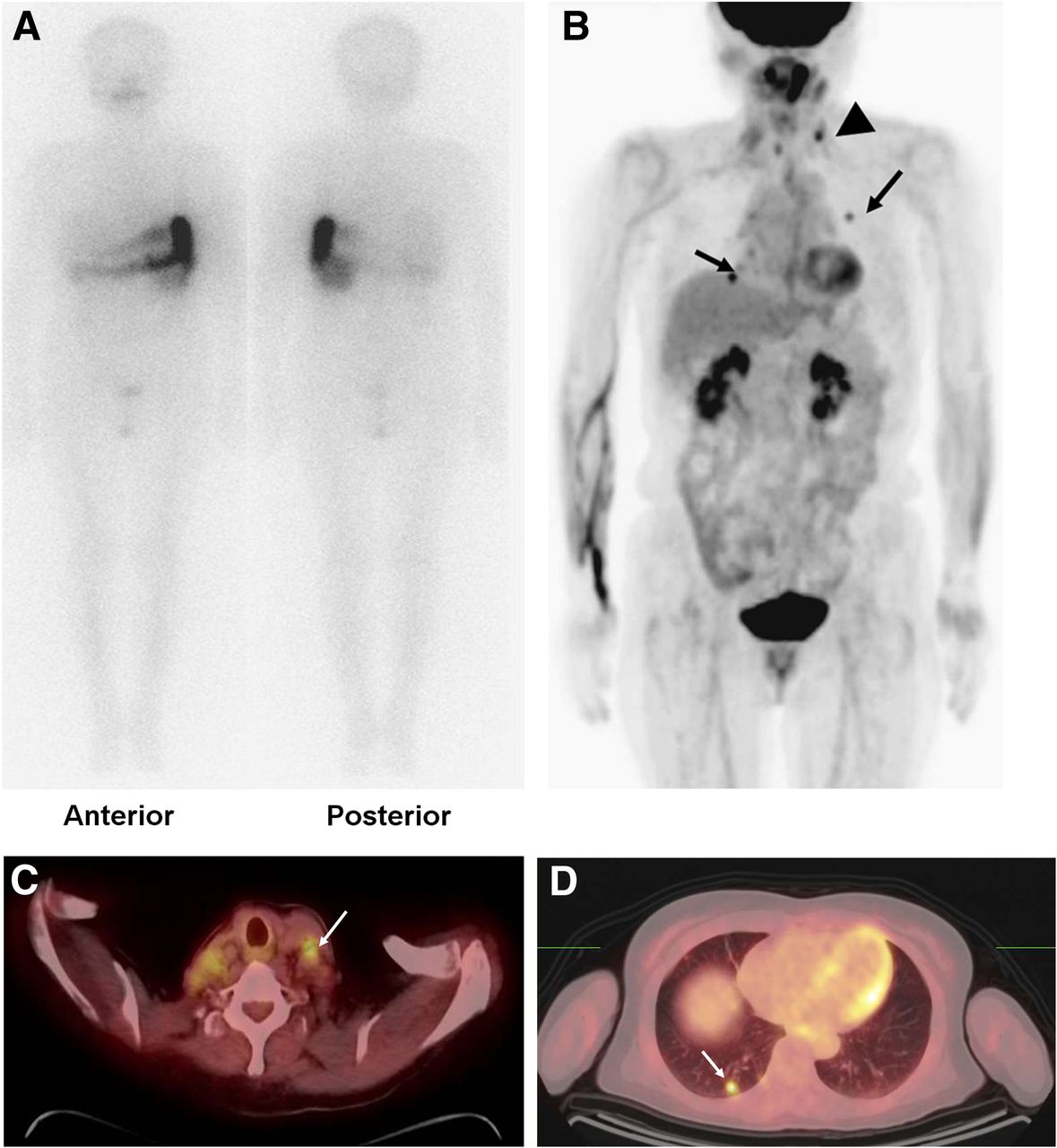
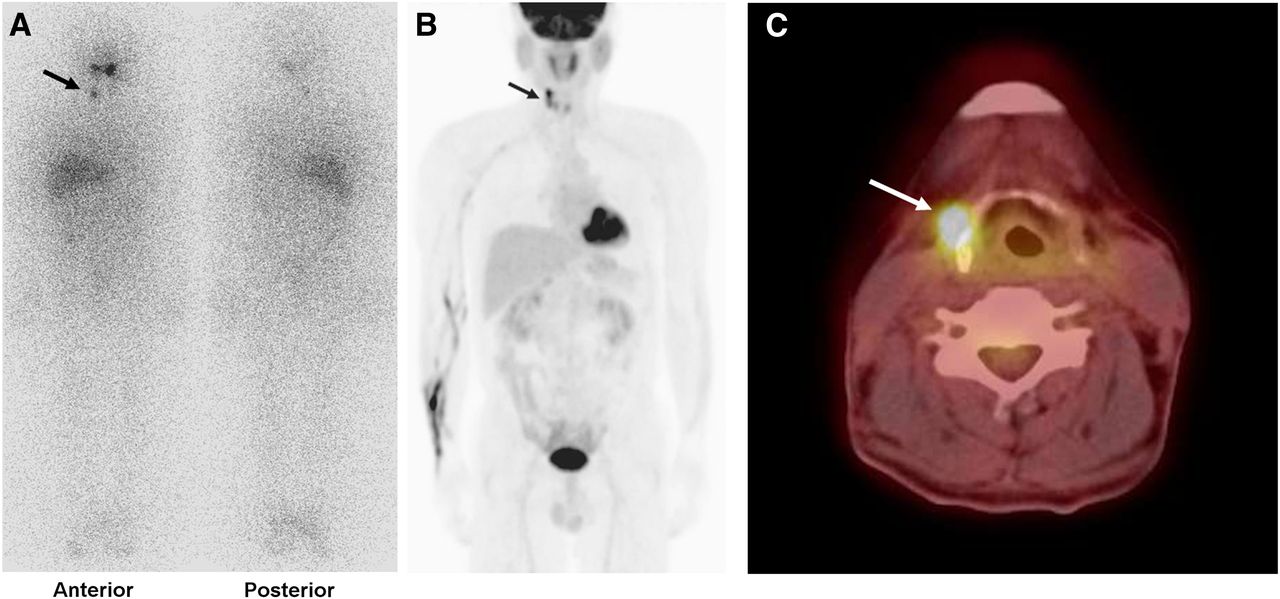
18F-FDG PET/CT showed positive lesions in 50 patients (17%) among the enrolled 286. This group of 50 patients includes 39 (14%) with additional positive lesions on the 18F-FDG PET/CT scan that were not observed on the posttherapy 131I scan (Fig. 1): in the neck lymph nodes (n = 27), neck lymph nodes and lungs (n = 4), thyroid bed recurrent lesions (n = 3), thyroid bed recurrent lesions and neck lymph nodes (n = 2), neck and mediastinal lymph nodes and lungs (n = 1), mediastinal lymph nodes and lungs (n = 1), and lungs (n = 1). Of these 39 patients, 24 (62%) had only lesions with a score of 3, and the remaining 15 patients (38%) had at least 1 lesion with a score of 4. PET/CT findings led to treatment change in 30 patients (10%) from further 131I treatment to surgical resection, EBRT, or multikinase inhibitor therapy.
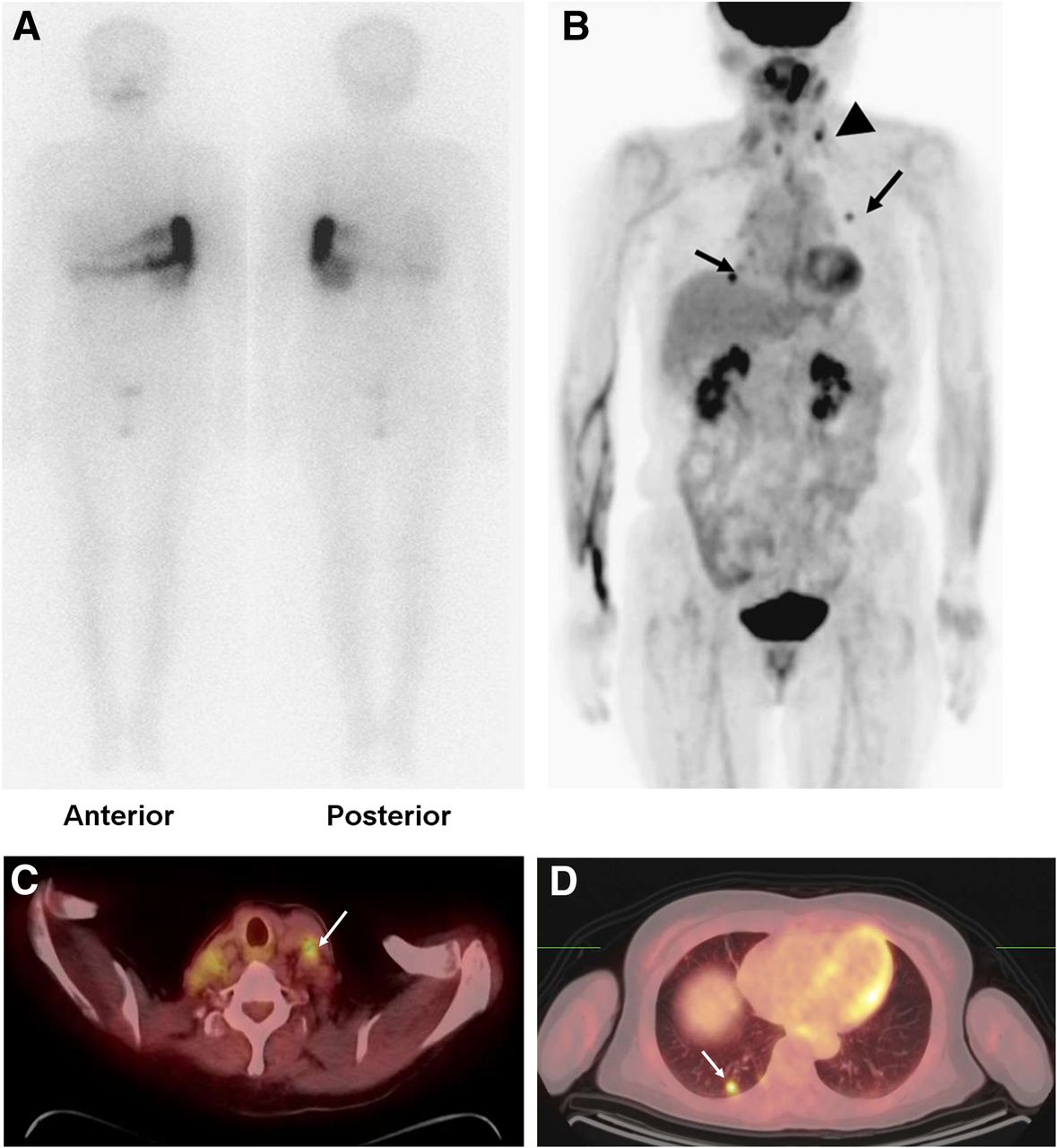
A 72-y-old woman with papillary thyroid cancer underwent 131I ablation (3.7 GBq) 4 mo after total thyroidectomy (histopathologic stage, T3N1). Posttherapy 131I scan (A) showed no abnormal 131I uptake, suggesting remnant thyroid uptake or metastatic lesion. However, maximal-intensity-projection image (B) and transaxial images (C and D) of 18F-FDG PET/CT showed areas of increased focal uptake in left neck region (arrowhead) and in lung (arrow), suggesting multiple metastatic lesions. Neck lesion was histopathologically diagnosed as metastatic lesion.
In 15 patients (5%), both 18F-FDG PET/CT and posttherapy 131I scans showed positive lesions. The same lesions were found on both PET/CT and 131I scans in 11 patients (Fig. 2), and the remaining 4 patients had additional lesions on PET/CT. Additionally, of the entire study sample, 8 patients (3%) had positive lesions only on the posttherapy 131I scan.
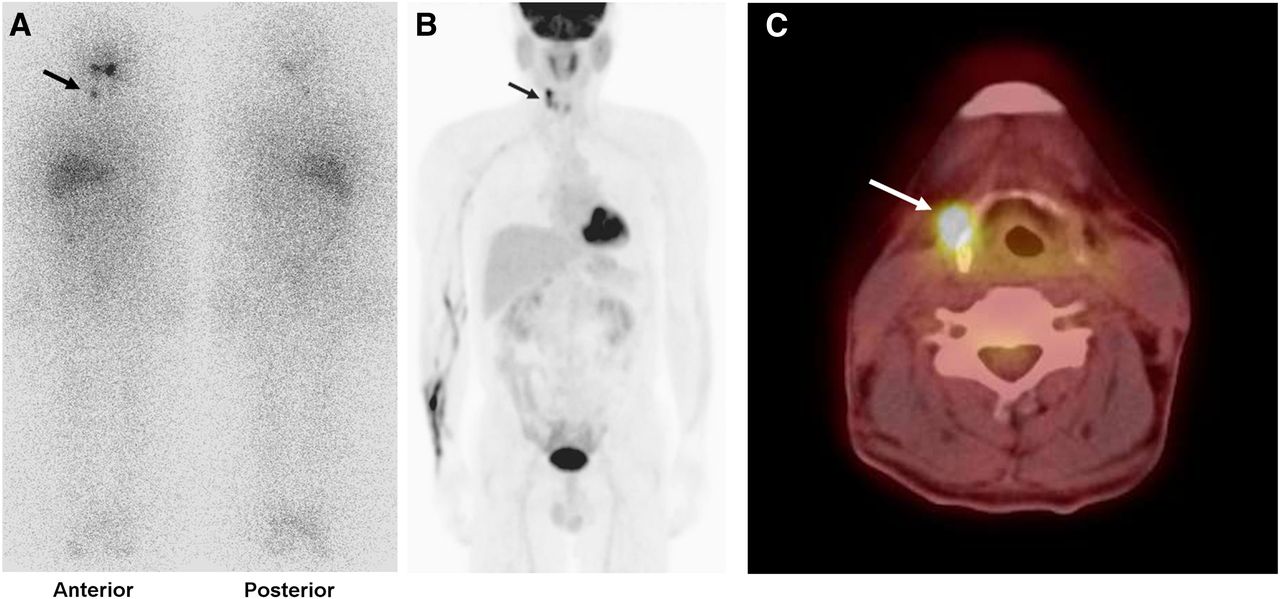
A 61-y-old man with papillary thyroid cancer underwent adjuvant 131I treatment (5.6 GBq) 3 mo after neck lymph node dissection for recurrent cancer. Posttherapy 131I scan (A) showed focus of increased 131I uptake in right neck area (arrow), which also showed increased focal uptake (arrow) on maximal-intensity-projection (B) and transaxial 18F-FDG PET/CT (C) images. Lesion was histopathologically confirmed as metastatic lesion.
18F-FDG PET/CT Findings According to Stage
The ratios of patients with additional lesions on PET/CT and treatment change due to PET/CT findings appeared to follow an upward trend along with a histopathologic stage of the patients (P < 0.0001, χ2 test for trend). 18F-FDG PET/CT findings according to the histopathologic stage are presented in Table 2. In the 28 patients undergoing adjuvant 131I treatment after surgical resection of recurrence, the frequency of additional lesions on PET/CT (46%; P = 0.0001 for stage T3–T4N1 group, P < 0.0001 for stage T3–T4N0 and T1–T2N1 groups) and the frequency of treatment change due to PET/CT findings (43%; P < 0.0001 for all) were significantly higher than in the other patient groups. Furthermore, in 159 patients with stage T3–T4N1, the frequency of additional lesions on PET/CT (13%) and the frequency of treatment change due to PET/CT findings (9%) were higher than in patients with stage T3–T4N0 or T1–T2N1. However, treatment change occurred in less than 5% of patients with T3–T4N0 or T1–T2N1.
Positive 18F-FDG PET/CT Finding and Subsequent Treatment Change According to Stage
18F-FDG PET/CT Findings According to Age and Tumor Size
Because age and tumor size are prognostic factors in DTC (15–17), we analyzed 18F-FDG PET/CT findings accordingly. All 286 patients were classified into 2 groups according to patients’ age at the time of diagnosis of DTC: 90 were 45 y or younger and 196 were older than 45 y at diagnosis. Of those who were 45 y or younger, 14 patients (16%) had additional positive lesions on 18F-FDG PET/CT, compared with 25 (13%) of those who were older than 45 y. There was no significant difference between the 2 groups (P = 0.6).
Furthermore, 258 patients who underwent 131I ablation after total thyroidectomy were divided into 2 groups according to the tumor size: 190 patients had tumor size ≤ 2.0 cm and 68 patients had tumor size > 2.0 cm. The 28 patients who underwent adjuvant 131I treatment after resection of recurrent tumors were excluded from this analysis. Thirteen patients from each subgroup had additional positive PET/CT lesions (7% for patients with tumor size ≤ 2.0 cm and 19% for patients with tumor size > 2.0 cm), and there was a statistically significant difference between the 2 groups (P = 0.008).
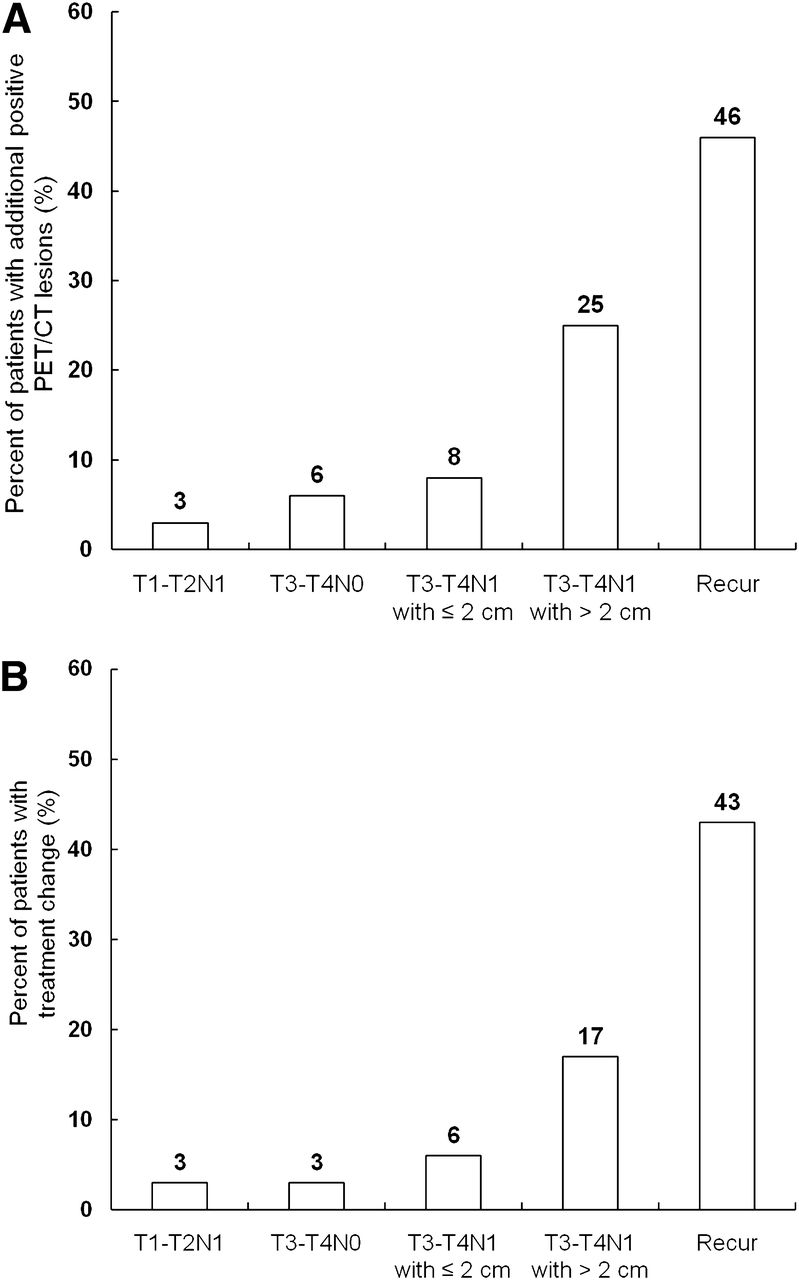
Because we found that the tumor size was a risk factor for positive findings on PET/CT, we performed further subgroup analysis of the 159 patients with stage T3–T4N1. The patients with stage T3–T4N1 were divided into 2 groups according to the tumor size of 2 cm: 106 with tumor size ≤ 2.0 cm and 53 with tumor size > 2.0 cm. In patients with tumor size > 2.0 cm, 13 (25%) had additional positive lesions, compared with 8 patients (8%) with tumor size ≤ 2.0 cm. Furthermore, treatment was changed due to PET/CT findings in 17% (9/53) of patients with tumor size > 2.0 cm, whereas only 6% (6/106) of patients with tumor size ≤ 2.0 cm had treatment change. Stage T3–T4N1 patients with tumor size > 2.0 cm had a significantly higher frequency of positive PET/CT findings than stage T3–T4N1 patients with tumor size ≤ 2.0 cm (P = 0.006), stage T3–T4N0 patients (P = 0.007), or stage T1–T2N1 patients (P = 0.006). Hence, both tumor stage and size can be predictive factors for positive findings on 18F-FDG PET/CT (Fig. 3).

Ratios of patients with additional positive lesions on 18F-FDG PET/CT (A) and ratios of patients with treatment change due to PET/CT findings (B). Stage T3–T4N1 patients with tumor size > 2.0 cm and patients who underwent adjuvant 131I treatment after operation for recurrence had higher frequency of positive PET/CT findings and treatment change than stage T3–T4N1 patients with tumor size ≤ 2.0 cm, stage T3–T4N0 patients, or stage T1–T2N1 patients (P < 0.05). T3–T4N1 with ≤ 2 cm = stage T3–T4N1 patients with tumor size ≤ 2 cm; T3–T4N1 with > 2 cm = stage T3–T4N1 patients with tumor size > 2 cm; Recur = patients who underwent adjuvant 131I treatment after operation for recurrent tumor.
18F-FDG PET/CT Findings and Serum Thyroglobulin Level
Of the total 286 patients, 72 (25%) had positive findings for antithyroglobulin antibody. Serum thyroglobulin level was evaluated in the remaining 214 patients (75%) with negative antithyroglobulin antibody, including 34 of the 50 patients with positive PET/CT lesions and 180 of the 236 patients with negative PET/CT lesions. The mean serum thyroglobulin levels in patients with positive and negative PET/CT lesions were 121.0 ± 203.1 ng/mL (range, 0.4–1000.0 ng/mL) and 7.8 ± 19.0 ng/mL (range, 0.1–167.7 ng/mL), respectively. There was a statistically significant difference in the serum thyroglobulin levels between the 2 groups (P < 0.0001).
Of the 39 patients with additional positive lesions on PET/CT, 13 had positive antithyroglobulin antibody findings. Serum thyroglobulin levels were evaluated in the remaining 26 patients. Furthermore, of the 19 patients with positive lesions on both PET/CT and 131I scans (n = 11) or positive lesions on 131I scan only (n = 8), 4 patients had positive findings for antithyroglobulin antibody, and serum thyroglobulin levels were measured in the remaining 15 patients. Although the serum thyroglobulin level in patients with additional positive lesions on PET/CT (mean value, 138.1 ± 224.6 ng/mL; range, 2.3–1000.0 ng/mL) tended to be higher than that in patients with positive lesions on both PET/CT and 131I scan or positive lesions on 131I scan only (mean value, 48.3 ± 57.0 ng/mL; range, 0.4–184.8 ng/mL), there was no statistically significant difference in the serum thyroglobulin levels (P = 0.1; Fig. 4).
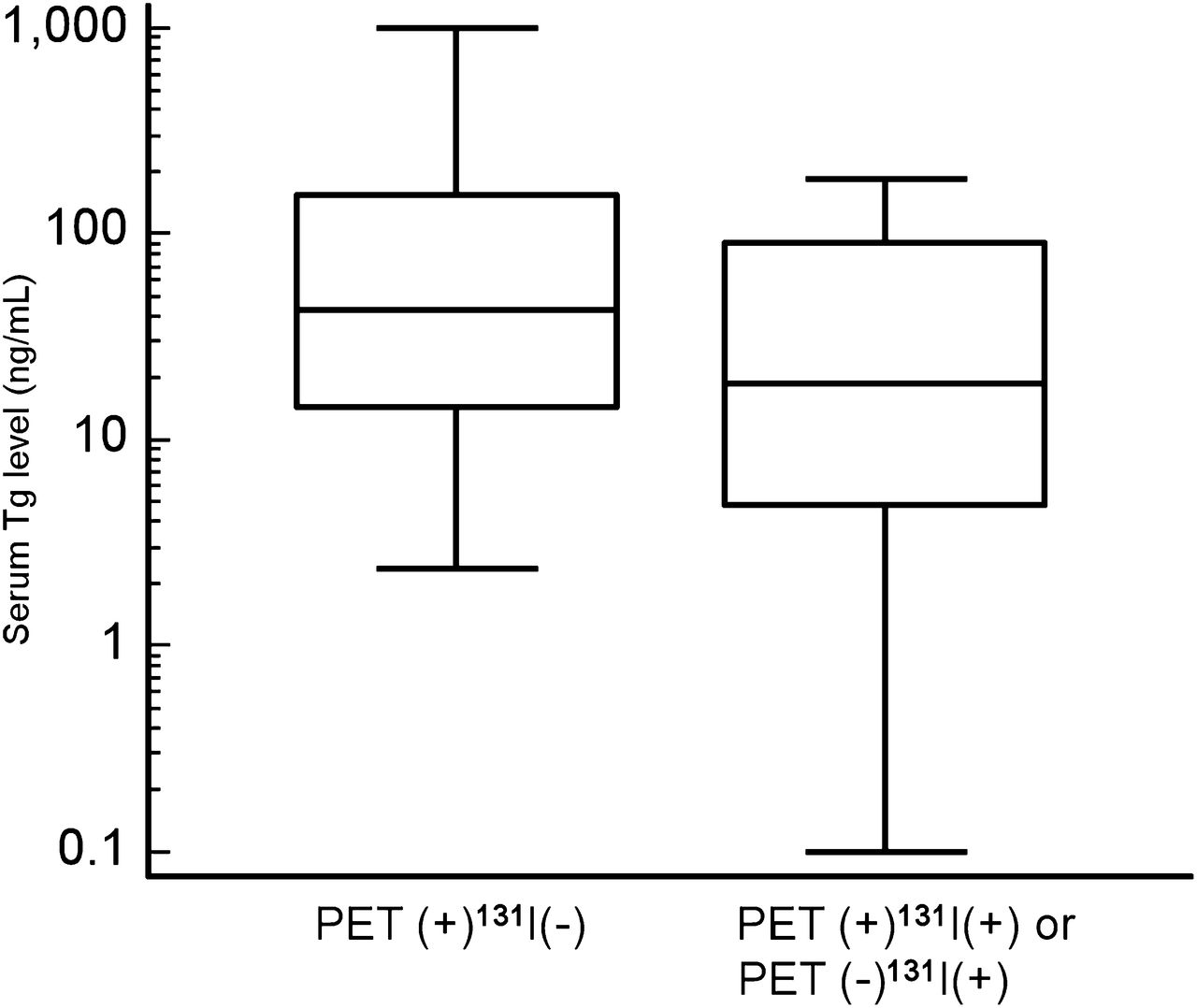
Serum thyroglobulin values in patients with additional positive lesions on 18F-FDG PET/CT (PET(+)131I(−) group) and in patients with positive lesions on both PET/CT and 131I scan or with positive lesions on only 131I scan (PET(+)131I(+) or PET(−)131I(+) group). There was no significant difference in serum thyroglobulin level between the 2 groups (P > 0.05).
DISCUSSION
This study demonstrated that 18F-FDG PET/CT performed concurrently with 131I treatment can detect additional recurrent or metastatic lesions, which were negative on posttherapy 131I scan, in 14% of patients with DTC and influence the treatment plan for these patients. Among patients who underwent adjuvant 131I treatment after operation for recurrence, 46% had additional positive PET/CT findings. Furthermore, of stage T3–T4N1 patients with tumor size > 2 cm who underwent 131I ablation, 25% had additional positive PET/CT findings, suggesting that routine PET/CT performed concurrently with 131I therapy should be considered for patients in this group. Tumor stage and size were predictive factors for positive PET/CT findings; however, age and serum thyroglobulin level were not risk factors for positive PET/CT findings.
To date, 2 studies have reported the usefulness of 18F-FDG PET/CT as an initial staging modality performed with 131I treatment (14,18). Rosenbaum-Krumme et al. (18) performed 18F-FDG PET/CT about 1 wk after the first 131I treatment in 90 patients with high-risk DTC. They found that 29% of patients had positive PET/CT findings, and the treatment strategy for 21% changed. They also showed that age and serum thyroglobulin level were not predictive factors for the presence of positive PET/CT lesions—a result that agrees with our findings. Iwano et al. (14) performed 18F-FDG PET/CT with serum TSH stimulation 3–4 d before 131I ablation in 54 patients with DTC. 18F-FDG PET/CT findings were positive in 33% of enrolled patients, and most of the positive lesions were located in the thyroid bed and cervical lymph nodes. Our study showed that PET/CT found additional lesions in 14% of patients, and treatment was changed in 10% of patients, slightly lower proportions than those previously reported (14,18). This difference could be due to the large numbers of patients with intermediate risk in our study. Moreover, the previous studies enrolled a small number of patients with high risk or advanced stage.
We found a high frequency of additional positive PET/CT lesions in patients with recurrent DTC (46%) and in patients with stage T3–T4N1 and tumor size > 2 cm (25%). However, only 3%–6% of patients with stage T3–T4N0 or T1–T2N1 had additional PET/CT findings. Recurrence is found in 16%–35% of DTC patients after initial surgery (19,20), and recurrent DTC cells often exhibit negative 131I uptake and positive findings on 18F-FDG PET/CT due to cell dedifferentiation (6,21). Furthermore, T stage, presence of nodal metastasis, and tumor size are prognostic factors for DTC that reflect the aggressiveness of cancer cells (16,17,22,23). A previous study has already shown that glucose transporter 1 expression increased with escalating dedifferentiation and aggressiveness of thyroid cancer cells (24). These findings support the idea that a routine 18F-FDG PET/CT scan can be beneficial for DTC patients with aggressive clinical features or recurrent lesions. We stratified our patients by tumor stage and size to predict risk of positive PET/CT lesions with negative 131I uptake. At our medical centers, 18F-FDG PET/CT has routinely been performed at the same time as 131I treatment in patients who underwent curative operation for recurrence or in patients with stage T3–T4N1 and tumor size > 2 cm.
Until recently, the relationship between cell differentiation in DTC and 131I and 18F-FDG uptake has been explained according to the so-called flip-flop phenomenon; DTC cells with remaining functional differentiation for iodine uptake are known to exhibit low 18F-FDG uptake, whereas dedifferentiated thyroid carcinoma cells with aggressive features show high 18F-FDG uptake with a loss of avidity for iodine uptake (6,25). However, we observed simultaneous uptake on both 18F-FDG PET/CT and 131I scans in some of our patients (Fig. 2). Previous studies have also found simultaneous uptake of 18F-FDG and 131I in metastatic DTC lesions (18,26). On the basis of the results of these studies, Bertagna et al. (27) suggested that iodine and 18F-FDG metabolism in DTC could be, at least partly, unrelated. Nevertheless, most patients with metastatic lesions in our study exhibited positive uptake on only the 18F-FDG PET/CT or the 131I scan.
In our study, 18F-FDG PET/CT was performed just before 131I treatment on the same day to maximize TSH stimulation and minimize inconvenience to patients. A recent metaanalysis showed that PET scans under TSH stimulation significantly improved the detection of DTC metastases and suggested that TSH stimulation should be recommended for DTC patients undergoing PET scanning (28). Because 131I treatment is performed in patients with an appropriately increased serum thyroglobulin level, with concurrent use of 18F-FDG PET/CT with 131I treatment, TSH-stimulated PET/CT images can be acquired without additional preparation. However, even in TSH-stimulated PET/CT images, 62% of patients with additional lesions had lesions with a score of 3. Hence, because many metastatic DTC lesions can still have mild-to-moderate 18F-FDG uptake on TSH-stimulated PET images, a careful analysis of PET/CT images is needed.
Although the serum thyroglobulin levels in patients with additional PET/CT-positive lesions tended to be higher than in patients with positive 131I scan lesions, there was no significant difference in our study. The serum thyroglobulin level is only indicative of the presence of DTC lesions and tumor burden irrespective of tumor differentiation (29–32). Furthermore, some patients with positive PET/CT findings in the present study had low serum thyroglobulin levels of < 10.0 ng/mL with TSH stimulation, suggesting that DTC patients with low serum thyroglobulin levels can also have positive PET/CT findings.
Though pretherapy radioiodine scanning was not performed in our study, the American Thyroid Association recommends pretherapy scanning when the extent of the thyroid remnant cannot be ascertained or when the results would alter the treatment plan or the dose of 131I (1). TSH-stimulated PET/CT imaging can be performed with pretherapy scanning for detecting iodine-negative lesions before 131I treatment. However, there is still a debate whether pretherapy 123I scanning can achieve results comparable to posttherapy 131I scanning (33–35). Therefore, careful consideration is needed to diagnose iodine-negative lesions based on pretherapy 123I scans.
There are several limitations in our study. First, because the present study was retrospectively performed, selection bias could have affected the results. Second, all the patients were Korean. Because dietary patterns and genetic mutation for DTC in Koreans are different from those in other ethnic groups (36,37), further studies are needed to establish concurrent 18F-FDG PET/CT and 131I therapy as a standard procedure in other countries. Third, only planar posttherapy 131I images were obtained in the study, and SPECT was not performed. Further studies that compare PET/CT with SPECT/CT will be needed to confirm the clinical utility of PET/CT. Finally, not all positive PET/CT lesions were histopathologically confirmed, especially distant metastatic lesions. However, because these positive PET/CT lesions were verified by follow-up imaging studies, it could not significantly influence the results.
CONCLUSION
The present study demonstrated that 18F-FDG PET/CT performed concurrently with 131I treatment detects additional iodine-negative metastatic foci in 14% of DTC patients, resulting in a change in further management of many of such patients. Tumor stage and size predict the likelihood of detecting 18F-FDG–avid lesions. Therefore, we recommend concurrent 18F-FDG PET/CT imaging with 131I treatment in DTC patients with recurrent tumors or aggressive clinical features.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported in part by the Soonchunhyang University Research Fund. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 27, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 11, 2012.
- Accepted for publication March 28, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}