


Abstract
White blood cell scanning with 99mTc-hexamethylpropylene amine oxime (HMPAO) has proven highly sensitive and specific in the diagnosis and follow-up of patients with suspected osteomyelitis. The aim of this prospective study was to evaluate the usefulness of SPECT and transmission CT performed simultaneously using a hybrid imaging device for the functional anatomic mapping of bone and joint infections. Methods: 99mTc-HMPAO scintigraphy was performed on 28 consecutive patients: 15 with suspected bone infection (group 1) and 13 with suspected orthopedic implant infection (group 2). Planar scans were acquired 30 min, 4 h, and 24 h after injection. SPECT/CT was obtained 6 h after tracer injection, using a dual-head γ-camera coupled with a low-power x-ray tube. In all patients, scintigraphic results were matched with the results of surgery or cultures and of clinical follow-up. Results: 99mTc-HMPAO scintigraphy was true-positive for infection in 18 of 28 patients (for a total of 21 sites of uptake) and true-negative in 10 of 28 subjects. SPECT/CT provided an accurate anatomic localization of all positive foci. With regard to the final diagnosis, SPECT/CT added a significant clinical contribution in 10 of 28 patients (35.7%). In fact, SPECT/CT differentiated soft-tissue from bone involvement both in patients with osteomyelitis and in patients with orthopedic implants, allowed correct diagnosis of osteomyelitis in patients with structural alterations after trauma, and identified synovial infection without prosthesis involvement in patients with a knee implant. Conclusion: Our results indicate that SPECT/CT performed using a hybrid device can improve imaging with 99mTc-HMPAO–labeled leukocytes in patients with suspected osteomyelitis by providing accurate anatomic localization and precise definition of the extent of infection.
The diagnosis and localization of bone infection still represent a challenge for physicians. Because laboratory tests are relatively nonspecific, imaging is required to reach a correct diagnosis. Locating the site of infection is important for planning adequate treatment and evaluating the response to it (1). Previously published papers have reported that inflammatory processes can be imaged by several nuclear medicine methods (i.e., 67Ga-citrate, labeled white blood cells, and labeled antibodies) (2,3). However, 111In- and 99mTc-labeled leukocyte scintigraphy has proven to be clinically useful for diagnosing infections, especially in cases of bone or joint involvement (4).
In many cases, planar images alone may not be sufficiently accurate to assess the extent of disease. It has been reported that SPECT can increase the sensitivity of planar images (5), but SPECT does not provide precise anatomic characterization. The fusion of functional (i.e., SPECT) and morphologic (i.e., CT) images was introduced to overcome the lack of anatomic landmarks in nuclear medicine and has, in fact, significantly improved diagnostic accuracy over that with SPECT alone (6,7). In particular, the hybrid SPECT/CT device combining a dual-head, variable-angle γ-camera and a low-dose x-ray tube allows coregistration of SPECT and CT images acquired during the same session, thus providing a fusion image with precise functional–anatomic correlation (8). Horger et al. (9), in using 99mTc-labeled antigranulocyte antibodies, reported that SPECT/CT improves the accuracy of immunoscintigraphy for the diagnosis of chronic osteomyelitis, especially in discriminating soft-tissue from bone involvement. However, the sensitivity of antigranulocyte antibody scintigraphy decreases gradually from the periphery of the bone because of nonspecific uptake of the antibodies in bone marrow (10). Therefore, 99mTc-hexamethylpropylene amine oxime (HMPAO)–labeled leukocytes are often preferred for imaging inflammation, despite the relatively complex and time-consuming labeling procedure.
The aim of our study was to evaluate the additional contribution of SPECT/CT, performed using a hybrid camera, with respect to conventional 99mTc-HMPAO–labeled leukocyte scintigraphy in a group of patients with suspected bone and joint infection.
MATERIALS AND METHODS
Patient Population
Twenty-eight patients (17 men and 11 women; age range, 26−80 y; mean age ± SD, 50.3 ± 12.5 y) with suspected bone and joint infection were enrolled. All patients presented with clinical signs of infection (i.e., swelling, pain, heat, erythema, or fever) and abnormal laboratory test results (increased white blood cell count, percentage of neutrophils, erythrocyte sedimentation rate). In all patients, antibiotic therapy was withdrawn at least 20 d before scintigraphy. Patients were assigned to 1 of 2 different groups according to their clinical situation. Group 1 included 15 patients with suspected osteomyelitis: 6 with acute osteomyelitis (symptoms and signs for less than 2 wk) and 9 with a suspected relapse of chronic osteomyelitis. Group 2 included 13 patients with suspected infection of orthopedic implants: 7 with a hip prosthesis and 6 with a knee prosthesis. In all of them, scintigraphy was performed more than 12 mo after the prosthesis had been implanted. All patients were consecutively recruited as a part of a research protocol. This prospective study was approved by the institutional ethics committee. All subjects gave written informed consent before enrollment.
Imaging Protocol
After blood sampling, leukocytes were isolated and labeled as described by Biancone et al. (11). The average labeling yield was 70%−85%. The labeled cells were reinjected into each patient, and the administrated activity ranged from 400 to 555 MBq.
A hybrid SPECT/CT system (Millennium VG and Hawkeye; GE Healthcare) was used. It consists of a dual-head, variable-angle γ-camera equipped with high-resolution low-energy collimators and an x-ray tube with a set of detectors mounted on the opposite site of the γ-camera gantry (12). Multiple planar images of the suspected area were acquired at 30 min and 4 h and at 24 h after injection. The images were acquired in a 128 × 128 matrix using an imaging time of 10 min for the 30-min and 4-h views; for the late scans, an imaging time of 15 min per view was used. SPECT/CT was performed 6 h after tracer injection. CT data were acquired over 360° during 14 s for each transaxial slice. Multiple slices were obtained by moving the table by 1 slice step before acquisition of each subsequent slice. The full field of view consisted of 40 slices. SPECT was acquired in a 128 × 128 matrix, obtaining multiple views over 360° at a 30-s acquisition time per projection with an angular step of 3°. Images were reconstructed using Butterworth filtered backprojection (cutoff, 0.5; order, 10). Transverse, sagittal, and coronal slices were generated. Scintigraphic results were considered to be positive when one or more areas of uptake greater than background activity were identified.
Transmission data were reconstructed at a nuclear medicine workstation (eNTEGRA; GE Healthcare) to obtain cross-sectional attenuation images (256 × 256 matrix) in which each pixel represents the attenuation value of the corresponding tissue. The reconstructed CT data and nuclear medicine data were transmitted to a nuclear medicine database. The matching SPECT and CT data were subsequently fused.
Data Analysis
Initially, SPECT and planar images were separately assessed by a team of experienced nuclear medicine physicians, unaware of the results of any prior radiologic investigations (CT or MRI). Fusion imaging was subsequently evaluated, and the SPECT/CT findings were compared with the findings obtained with SPECT alone and with planar imaging alone.
SPECT/CT was considered contributory if it accurately localized the anatomic site of infection and, in particular, when it discriminated between bone and soft-tissue involvement.
The final diagnosis was verified for each suspected site by tissue cultures (12 sites) or surgery (19 sites) and by correlation with a clinical follow-up of up to 24 mo.
RESULTS
99mTc-HMPAO–labeled white cell scintigraphy was true-positive for infection in 18 of 28 patients (for a total of 21 sites of uptake) and true-negative in 10 of 28 subjects. The final diagnosis and a comparison of conventional scintigraphy (planar + SPECT) and SPECT/CT for groups 1 and 2 are summarized in Tables 1 and 2. The results of both methods in relation to the type and location of infection are shown in Table 3.
Results of Labeled Leukocyte Scintigraphy (Planar + SPECT) and SPECT/CT: Clinical and Scintigraphic Data on 10 Patients in Whom Osteomyelitis Was Suspected and Scan Findings Were Positive (Group 1)
Results of Labeled Leukocyte Scintigraphy (Planar + SPECT) and SPECT/CT: Clinical and Scintigraphic Data on 8 Patients in Whom Prosthesis Infection Was Suspected and Scan Findings Were Positive (Group 2)
Results of Conventional Scintigraphy (Planar + SPECT) and SPECT/CT Regarding Type and Location of Infection
Group 1 (Suspected Osteomyelitis)
Scintigraphy was positive for active infection in 10 of 15 patients, with a total of 12 sites of uptake, and true-negative in 5 of 15 patients. In all patients with positive findings, SPECT/CT was contributory with respect to SPECT and planar images, providing anatomic localization of all positive foci. In 3 patients with lower-limb osteomyelitis, SPECT/CT was able to precisely define the site of uptake, discriminating soft tissue from bone. In 5 subjects with structural bone alterations and focal labeled cell uptake on both planar and SPECT images, SPECT/CT precisely defined osteomyelitis (Fig. 1). In 2 patients with bone infection, SPECT/CT localized 2 additional sites of uptake in the soft tissue. SPECT/CT did not significantly contribute to the evaluation of patients with negative scan findings.

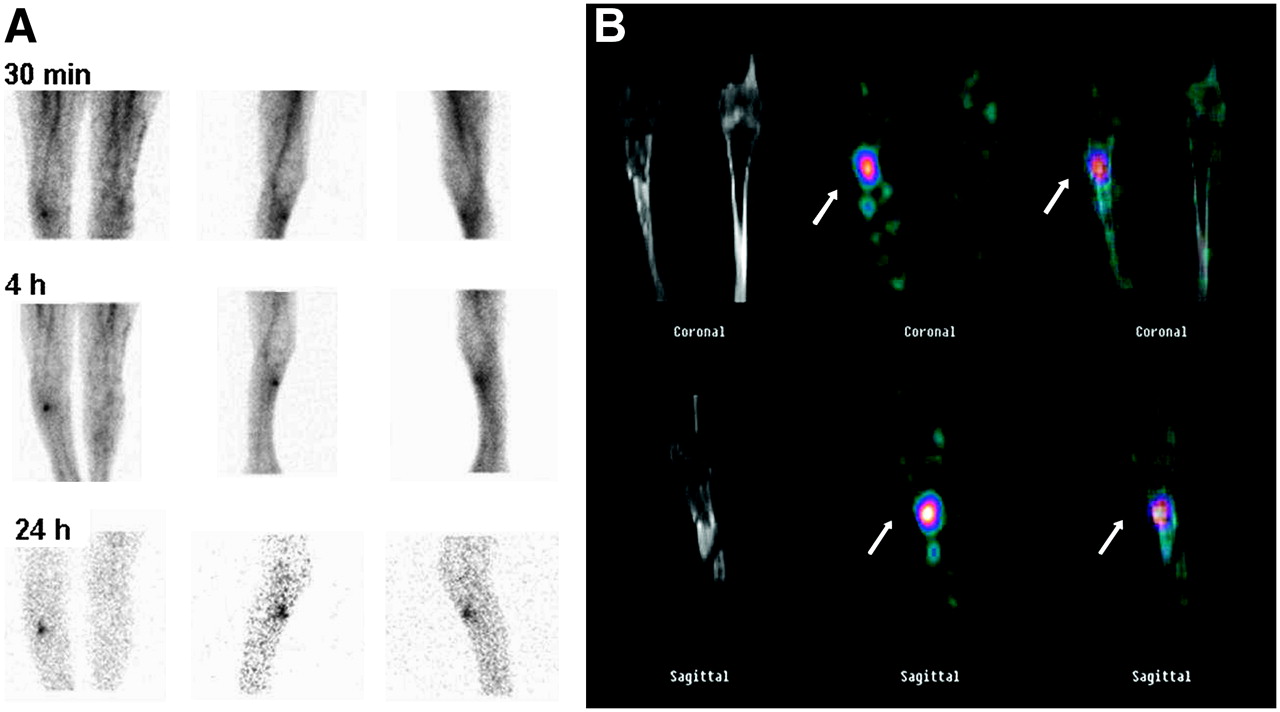
99mTc-labeled leukocyte scintigraphy of 50-y-old woman in whom posttraumatic osteomyelitis of right tibia was suspected. (A) Planar and SPECT images show focal area of tracer uptake in lower right limb. (B) SPECT/CT precisely localizes this focus to corresponding structural alteration in right tibia. Final diagnosis (made by surgery) was posttraumatic tibial osteomyelitis.
Group 2 (Orthopedic Implant Infection)
The results of scintigraphy were true-positive for infection in 8 of 13 patients, with a total of 9 sites of infection, and true-negative in 5 of 13 patients. SPECT/CT provided an accurate anatomic localization of all positive areas but did not help in the assessment of patients with negative scan findings. In particular, SPECT/CT was able to discriminate between prosthesis and soft-tissue uptake in 5 patients with a hip prosthesis. In 2 patients with a knee implant, SPECT/CT correctly localized leukocyte uptake in the synovium, thus excluding prosthesis involvement. In 1 patient with suspected hip prosthesis infection, SPECT/CT detected leukocyte accumulation along the femoral stem of the prosthesis and also revealed another site of infection in the neighboring soft tissue. Moreover, SPECT/CT disclosed 1 area of leukocyte uptake in the abdomen that was due to an unknown intestinal inflammatory polyp, which was then confirmed by colonoscopy and biopsy (Fig. 2).
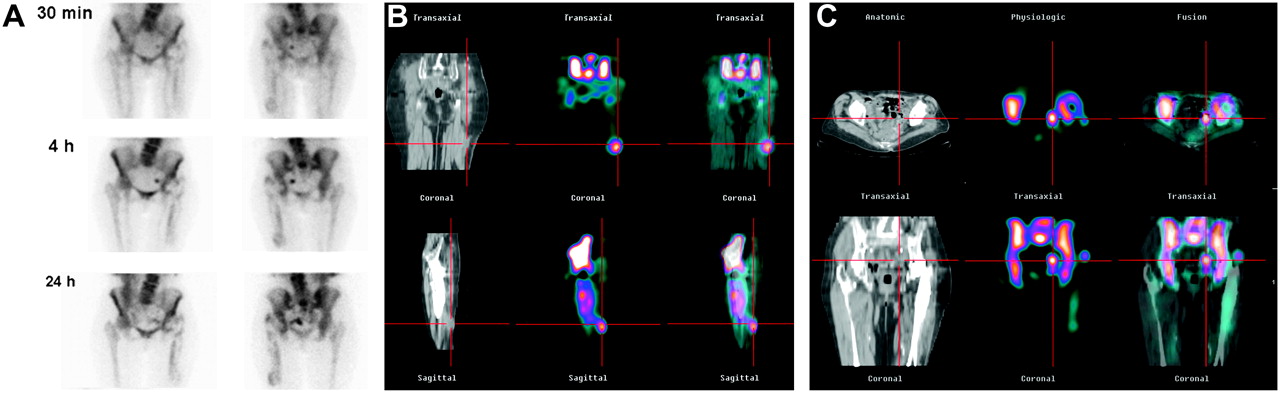
99mTc-labeled leukocyte scintigraphy of 60-y-old woman with left hip prosthesis. (A) Planar images show leukocyte uptake along hip prosthesis and additional focus of activity in left pelvis. (B) SPECT/CT localizes this leukocyte uptake to femoral stem of prosthesis and also detects cell accumulation in neighboring soft tissues. (C) SPECT/CT, moreover, discloses inflammatory polyp in left pelvis. Final diagnosis (made by surgery) was infected hip prosthesis and soft-tissue infection; for bowel lesion, diagnosis (made by colonoscopy and biopsy) was inflammatory polyp.
SPECT/CT Contribution to Final Diagnosis
The interpretation of conventional scintigraphy (planar + SPECT) was radically changed on the basis of SPECT/CT in 5 of the 15 patients of group 1 and in 5 of the 13 patients of group 2; in particular, osteomyelitis was excluded in 7 patients and the extent of infection was more correctly assessed in 3 patients. Overall, a significant contribution of SPECT/CT to the final diagnosis was therefore found in 10 (35.7%) of 28 patients.
DISCUSSION
Hybrid SPECT/CT has many clinical applications; however, relatively few reports have been published on its application to the labeled leukocyte imaging of infectious processes (13). In our series, the hybrid imaging device provided additional anatomic information on all patients with positive scan results (64.2%). With regard to the final diagnosis, SPECT/CT using a hybrid camera added a significant contribution in 35.7% of patients. In particular, SPECT/CT excluded bone involvement in patients with suspected osteomyelitis (group 1) and with orthopedic implants (group 2). Moreover, the hybrid system was able to localize additional sites of leukocyte uptake in neighboring soft tissue, thus more precisely defining the extent of infection. This ability is of particular importance because the therapeutic approaches to soft-tissue and bone infections are different (9).
It is well known that nuclear imaging (both planar and SPECT) is characterized by a relatively limited spatial resolution, compared with that of other imaging methods (CT and MRI). Moreover, labeled leukocyte scintigraphy lacks anatomic landmarks. In patients with suspected osteomyelitis, soft-tissue involvement is routinely differentiated from bone involvement by combining the interpretation of labeled leukocyte bone scans and methylene diphosphonate bone scans (4). The use of SPECT has been proposed to avoid obtaining 2 scans. For a group of patients (n = 37) with osteomyelitis, Weon et al. (5) reported an overall sensitivity of 66% for planar imaging and of 92% for SPECT. In particular, in some cases of bone infection with adjacent soft-tissue involvement, planar images alone did not allow differentiation of soft tissue from bone. On the contrary, the greater contrast provided by SPECT allowed more precise localization of sites of leukocyte accumulation. Nevertheless, although improving diagnostic accuracy with respect to planar images alone, SPECT still lacks precise anatomic information. Therefore, SPECT images are often visually correlated to the corresponding slices on the MRI or CT scan after a separate examination of the different imaging modalities. However, this visual integration might not always be feasible and depends strictly on the spatial sense of the observer. For this purpose, image-based fusion methods of independently performed functional and structural studies are now available through the use of intrinsic or extrinsic fiducial markers (7). With regard to the imaging of inflammatory diseases, a computer-assisted method of fusing SPECT (111In-labeled leukocyte or gallium scintigraphy) and CT images was used to evaluate 10 patients with suspected inflammatory disease (14). SPECT/CT fusion correctly characterized and localized the site of uptake in all patients, thus having a substantial impact on the clinical management of 6 (60%) of 10 patients. However, these image-based techniques were found to be suboptimal because of possible movement by the patients between the 2 scans and the need for a relatively complex preparation. As an alternative, SPECT/CT hybrid systems allow the acquisition of functional and morphologic images in a single session, thus eliminating many possible pitfalls of the image-based fusion methods and the need for complex algorithms. Moreover, low-dose CT allows for attenuation correction, thereby improving SPECT image quality (15). However, attenuation correction might not be so useful in improving imaging quality in SPECT of the extremities, particularly if a patient with a prosthesis is studied with low-dose CT. Moreover, in such cases, metal artifacts due to prosthetic implants can complicate the assessment of an abnormal focus of leukocyte uptake in the immediate vicinity of the metal device.
In the present study, SPECT/CT was found particularly useful for the diagnosis of relapsing osteomyelitis in patients with structural bone abnormalities after trauma. After traumatic injury, anatomic alterations often persist in bone; therefore, morphologic methods of imaging (i.e., CT or radiography) may not be sufficiently accurate to detect infection in structurally damaged bone (16,17). Although fusion imaging with a hybrid camera can improve the diagnostic accuracy of SPECT, fusion imaging cannot be a substitute for conventional high-resolution CT, which maintains its diagnostic role in most clinical situations. However, with regard to bone imaging, reports show that the low-dose CT of the hybrid device may provide sufficient diagnostic anatomic information. Horger et al. (18) evaluated the clinical value of SPECT/CT in oncologic patients with suspected bone metastases: Seventy-eight patients with equivocal findings on conventional bone scanning underwent SPECT/CT. Fusion of the SPECT images with the corresponding CT slices improved the specificity of scintigraphy in about 80% of the suspected sites. In our series, SPECT/CT allowed diagnosis of infection and imaged the corresponding structural bone alterations in 5 patients with posttraumatic osteomyelitis.
Horger et al. (9) also investigated the value of SPECT/CT in the diagnosis of chronic osteomyelitis using 99mTc-labeled antigranulocyte antibodies. They showed that SPECT/CT enabled differentiation between soft-tissue and bone infections and precisely localized cortical, corticomedullary, and subperiosteal foci. Sensitivity (100%) was identical for SPECT and SPECT/CT, whereas specificity was higher (89% vs. 78%) for SPECT/CT, although 1 false-positive result was obtained by both methods. In our series, no false-positive or -negative result was obtained, thus confirming the high diagnostic accuracy of 99mTc-HMPAO–labeled leukocyte scintigraphy in evaluating bone infection. However, we share with Horger's group the conclusion that, in comparison with SPECT alone, SPECT/CT may improve the specificity more than the sensitivity of scintigraphic studies. Although the more skilled and experienced nuclear physicians might be able to reach a correct diagnosis in many clinical situations without fusing the SPECT images with the corresponding anatomic data, findings showed that SPECT/CT using a hybrid camera may help increase interobserver agreement, thus suggesting greater reliability for this method of imaging (9). However, SPECT/CT cannot be considered a routine protocol for patients with suspected bone or joint infections. SPECT/CT is useful in patients with planar images positive for active infection but equivocal for localization. In such cases, a substantial diagnostic gain can be obtained at the cost of a relatively low additional radiation burden (0.5 mSv) (15). Therefore, the following diagnostic algorithm can be proposed. If osteomyelitis is excluded by SPECT/CT, the additional radiation dose of the CT component allows avoidance of the performance of bone scans (5.6 mSv) and bone marrow scans (2.5 mSv). On the other hand, if fusion imaging localizes leukocyte uptake to bone, bone marrow scanning is recommended in cases of recent surgical manipulation or prosthetic implantation. According to our data, SPECT/CT does not significantly contribute to the evaluation of patients when planar scan findings are negative.
Recently, Bar-Shalom et al. (13) used 67Ga or 111In-labeled leukocyte scintigraphy and SPECT/CT to investigate 82 patients with known or suspected infectious processes. The contribution of SPECT/CT was analyzed on a patient and site basis and was compared for the 2 tracers and clinical indications. SPECT/CT provided an additional contribution for diagnosis and localization in 48% of patients and at 47% of sites. The investigators found that the clinical value of SPECT/CT was significantly higher for labeled leukocyte scanning than for 67Ga scanning (63% vs. 36% of patients). In particular, SPECT/CT performed with 111In-labeled leukocytes added significant information for 7 (47%) of 15 sites and for 55% of patients assessed for osteomyelitis. However, the main value of hybrid technology was related to the precise anatomic localization of infection and accurate delineation of the extent of the infectious process after its diagnosis with conventional scintigraphy. The investigators concluded that fusion of functional and anatomic data becomes more important when highly specific target-oriented tracers are used for imaging. Our results confirmed the findings of Bar-Shalom's group for 99mTc-HMPAO–labeled leukocyte scintigraphy.
The main limit of leukocyte imaging has been reported to be nonspecific cell accumulation in the reticuloendothelial bone marrow (19). Moreover, the presence of orthopedic implants or surgical manipulations might cause additional variations in bone marrow distribution (20). Therefore, labeled leukocyte scintigraphy is often compared with 99mTc-labeled sulfur colloid bone marrow imaging. However, combined leukocyte/bone marrow scintigraphy is a time-consuming procedure. In our experience, we have performed 99mTc-labeled sulfur colloid imaging only in cases of equivocal findings on leukocyte scans because of recent prosthesis implantation or surgical manipulation. Another potential disadvantage of leukocyte scanning is the high blood-pool activity. However, this factor is more important in thoracic or abdominal localizations because of the potential difficulty of characterizing foci of leukocyte uptake near the major vessels. In such cases, the hybrid technology might be of value in discriminating between blood-pool activity and infectious foci. Nevertheless, we investigated the value of SPECT/CT in imaging infection of the extremities or in cases of hip or knee implants, where high blood activity does not significantly interfere with scan interpretation.
Precise alignment of the body region of interest is of paramount importance in SPECT/CT. In particular, involuntary movements of the extremities may mislead the localization of an abnormal focus. Therefore, the whole procedure should be explained accurately to the patient, and the patient's legs should be fixed during the SPECT/CT acquisition.
A further consideration has to be mentioned. Among our patients, SPECT/CT disclosed an unknown inflammatory polyp in a 60-y-old woman with a hip prosthesis infection. In addition, Martinez Lazaro and Cortez-Blanco (21) previously reported a case of an inflammatory polyp occasionally detected by HMPAO scintigraphy. Conventional planar and SPECT images might be unable to localize sites of leukocyte accumulation in the abdomen because of nonspecific leukocyte accumulation in the bowel. We believe that the hybrid device, in providing spatial localization of SPECT functional data, may also be clinically useful for better characterizing possible collateral findings on 99mTc-labeled leukocyte imaging.
CONCLUSION
SPECT/CT with 99mTc-HMPAO–labeled leukocytes can be a useful clinical tool to image bone and joint infections because it precisely localizes sites of leukocyte accumulation and allows the differentiation of soft-tissue from bone involvement. Moreover, it might be of value for more accurately characterizing possible collateral findings on leukocyte scintigraphy.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 9, 2006.
- Accepted for publication August 28, 2006.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 68Ga-Pentixafor PET/CT Imaging of Chemokine Receptor CXCR4 in Chronic Infection of the Bone: First Insights
- Radionuclide Imaging of Musculoskeletal Infection: A Review
- SPECT-CT: applications in musculoskeletal radiology
- Indexing Severity of Diabetic Foot Infection With 99mTc-WBC SPECT/CT Hybrid Imaging
- Leukocyte SPECT/CT for Detecting Infection of Left-Ventricular-Assist Devices: Preliminary Results
- Diabetic Foot Infection: Usefulness of SPECT/CT for 99mTc-HMPAO-Labeled Leukocyte Imaging
- Incremental Value of 131I SPECT/CT in the Management of Patients with Differentiated Thyroid Carcinoma
- SPECT/CT
- Diagnosis of Vascular Prosthesis Infection: PET or SPECT?