


Abstract
We report our experience with using integrated molecular and anatomic hybrid imaging to assess infection in patients who have a left-ventricular-assist device (LVAD). Methods: Thirteen 99mTc-exametazime-leukocyte planar and SPECT/CT scans were obtained for 8 consecutive patients who had an implanted LVAD. SPECT/CT was used to assess suspected device-related infections (n = 8) and to evaluate the efficiency of current antibiotic therapy (n = 5). Results: Device-related infection was seen on 8 of the 13 scans. SPECT/CT was positive for infection in all 8 patients, whereas planar scans were positive in 6 of 8. SPECT/CT provided relevant information on the extent of infection and its exact location in all patients. Additional distant infectious foci were demonstrated in 3 of 13 patients. Conclusion: SPECT/CT led to an accurate diagnosis of LVAD-related infection, revealing both anatomic location and extent. This noninvasive approach could lead to improved therapeutic strategies.
Implantation of a left-ventricular-assist device (LVAD) is increasingly becoming a therapy of choice in patients with advanced heart failure (1). However, device-related infection continues to be a morbid problem and remains a serious limitation to long-term use of the device (2). Major clinical issues include diagnosing the infection early, determining the location and extent of the infection, and assessing treatment efficacy. Anatomic imaging modalities such as CT and MRI are of limited value because of the presence of metallic CT artifacts and MRI contraindications.
Leukocyte planar scintigraphy is indicated for the diagnosis of infection in various clinical settings (3,4) and has a documented high sensitivity (98%) and specificity (89%) for identifying vascular graft infection (4,5). However, the poor spatial resolution of planar scintigraphy and the lack of anatomic landmarks are limiting factors. Integrated SPECT/CT allows coregistration of functional and anatomic imaging (6) and has been successfully proposed for the assessment of infectious processes in patients prone to metallic artifacts, especially in the field of bone and joint infection (7,8). However, not enough data are available on patients with soft-tissue infection (9). This study reports our early experience with radiolabeled leukocyte SPECT/CT in patients with an LVAD and suspected ongoing infectious inflammatory processes.
MATERIALS AND METHODS
Patients
Between February 2007 and September 2008, 13 imaging procedures were performed on 8 consecutive men (mean age ± SD, 56 ± 11 y) who had an implanted LVAD. The mean duration that the device was in use was 666 d (range, 188–868 d). Patients were referred for leukocyte scintigraphy if device-related infection was suspected or to assess the outcome of antibiotic therapy. Five patients underwent 2 imaging procedures. Bacteriologic samples were taken from all patients (repeated blood cultures and local sample collection at the cable exit site). All patients were implanted with a HeartMate II (Thoratec) metallic rotary blood pump (130 × 45 mm) just below the diaphragm. The inflow cannula is inserted into the left ventricular apex, and the outflow polyester graft is inserted into the ascending aorta. A percutaneous electric cable connects the pump, through the skin of the right flank, to an external system controller linked to a power source (2,10).
Leukocyte Labeling and Imaging Protocol
Leukocyte scintigraphy was performed immediately after intravenous injection of 714 ± 58 MBq of 99mTc-exametazime-labeled autologous granulocytes, according to a validated protocol (11). The mean average labeling yield was 90% ± 4%. All trypan blue tests gave positive results (≥99% viable cells).
All images were acquired using a SPECT/CT system (Symbia T2; Siemens Medical Solutions). Planar scans (128 × 128 matrix) were obtained over the chest and abdomen at hours 1, 4 and 24. SPECT/CT was performed over the same areas at hours 4 and 24. The CT current was adapted for the patient's weight (110 kV and 40–60 mAs), with dose reduction (CareDose; Siemens Medical Solutions). SPECT data were acquired over 360° (matrix size, 128 × 128; 128 projections; 30 s/projection at hour 4 and 60 s/projection at hour 24), and images were corrected for attenuation, scatter, and collimator depth dependence. Transverse, sagittal, and coronal slices of corrected and uncorrected SPECT data were merged with CT and interpreted on a dedicated workstation (Leonardo; Siemens Medical Solutions). The mean effective dose for an entire imaging procedure was 14 mSv.
Interpretation Criteria
Foci of abnormal uptake by leukocytes were analyzed on planar and SPECT/CT acquisitions by 2 experienced nuclear medicine physicians who worked in consensus and had no knowledge of the clinical context (i.e., diagnosis of suspected infection or antibiotic therapy assessment). Findings were considered positive when foci of labeled leukocyte uptake were greater than background activity and increased over time. Foci of nonphysiologic abnormal uptake that decreased at hour 24 were considered inflammatory.
RESULTS
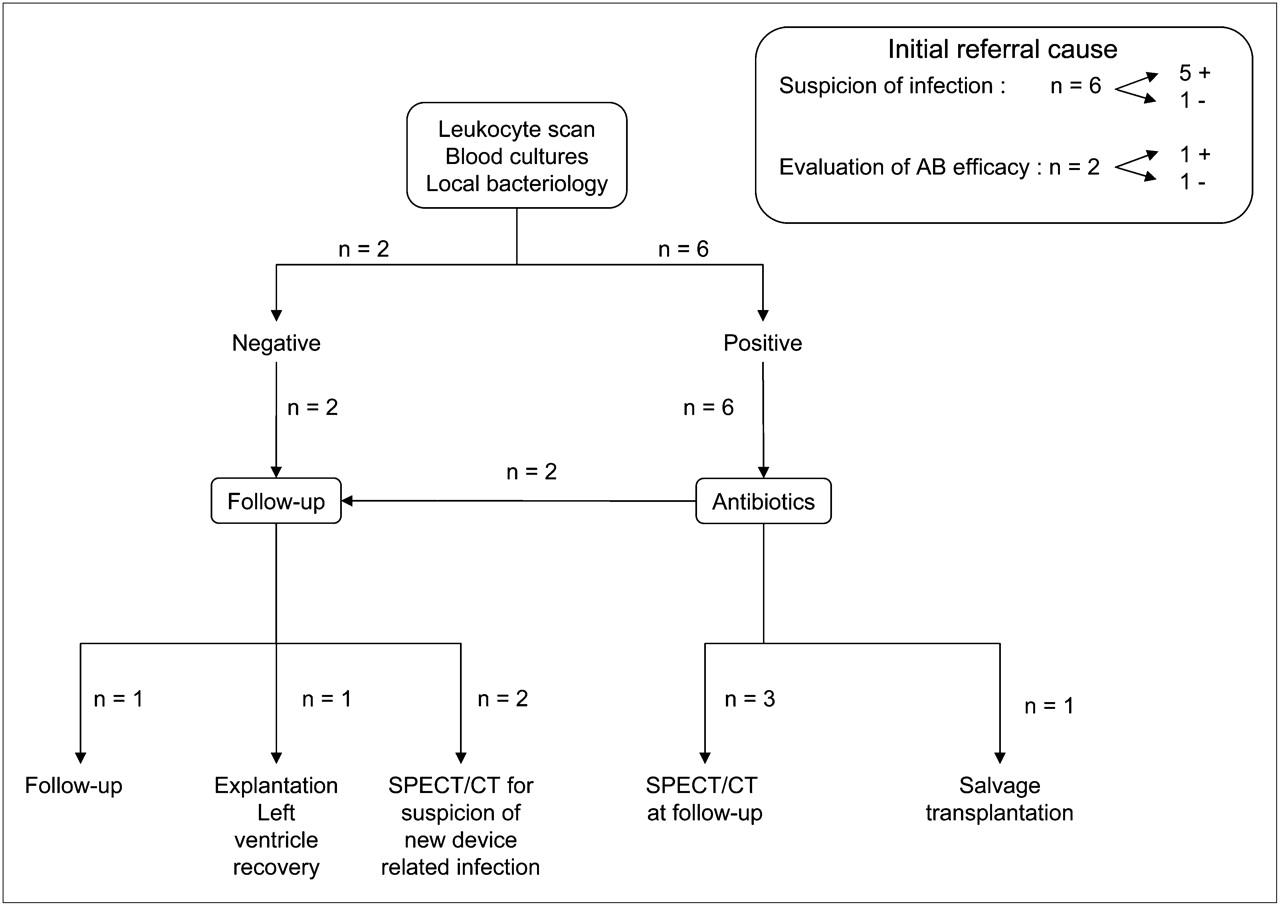
Scintigraphy was performed 337 ± 241 d (range, 52–701 d) after device implantation. The final diagnosis was based on bacteriologic cultures (needle or surgical samples) or patient follow-up. The patient management strategy is summarized in Figure 1.

Strategy for diagnosis and patient management.
Three imaging procedures were performed early (mean delay, 54 d) after LVAD implantation (patient 4, scan 1; patient 5, scan 1; and patient 7, scan 1) because of postoperative infection; the other procedures were performed 422 ± 145 d after LVAD implantation. Clinical, scintigraphic, and bacteriologic findings are detailed in Table 1. Artifacts generated by the prosthetic material were observed in all SPECT/CT investigations, but the quality of the examination was considered suitable for analysis in all cases.
Clinical Situation, Imaging Findings, and Bacteriologic Findings for Each Scintigraphic Procedure
Planar Scans
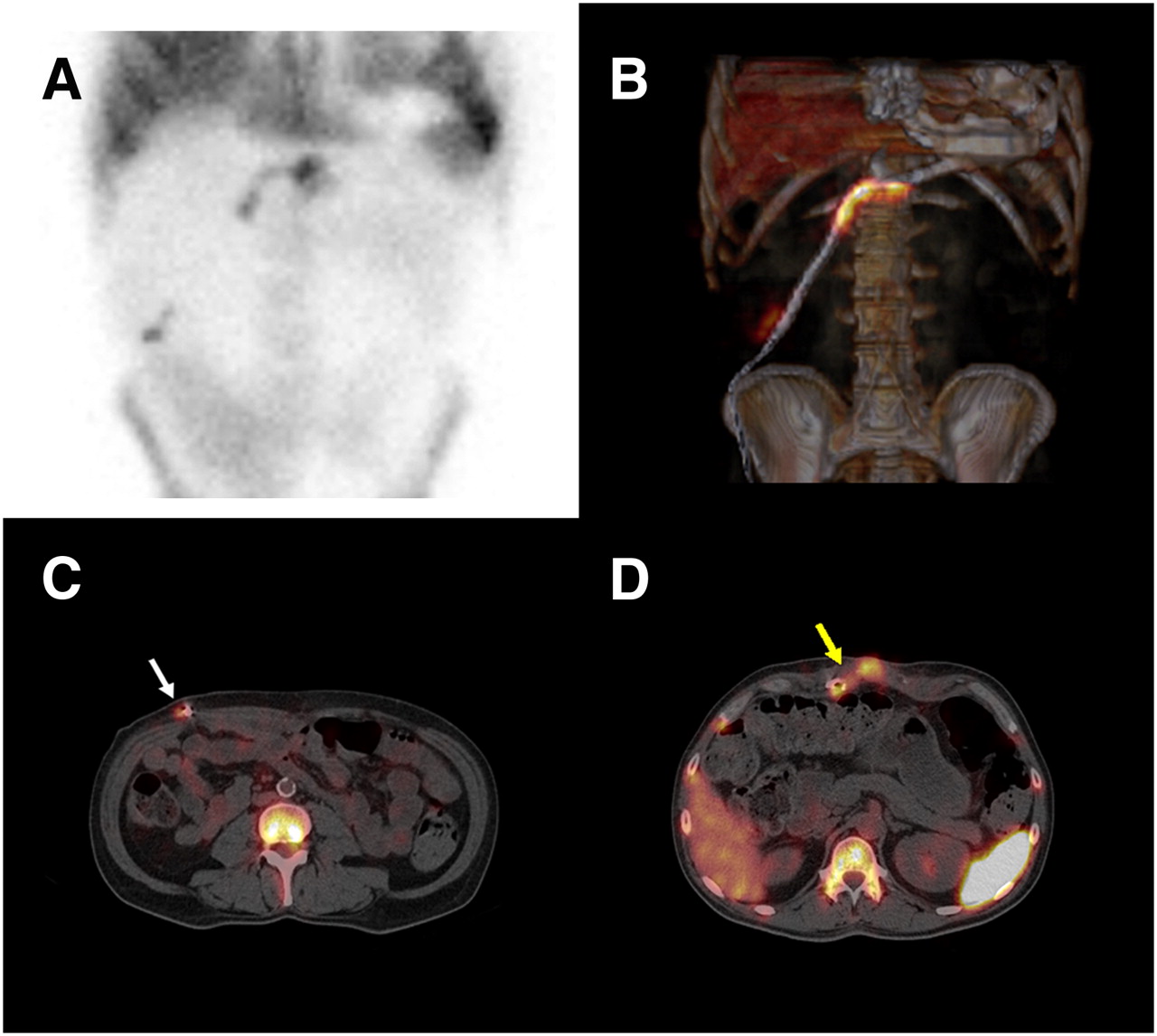
Foci of abnormal uptake considered positive for device-related infection were detected in 6 of 13 scans (46%). In these patients, planar analysis did not reveal any additional foci indicating distant infection and could not distinguish between deep infection and subcutaneous tissue infection at the cable exit site (Fig. 2A).
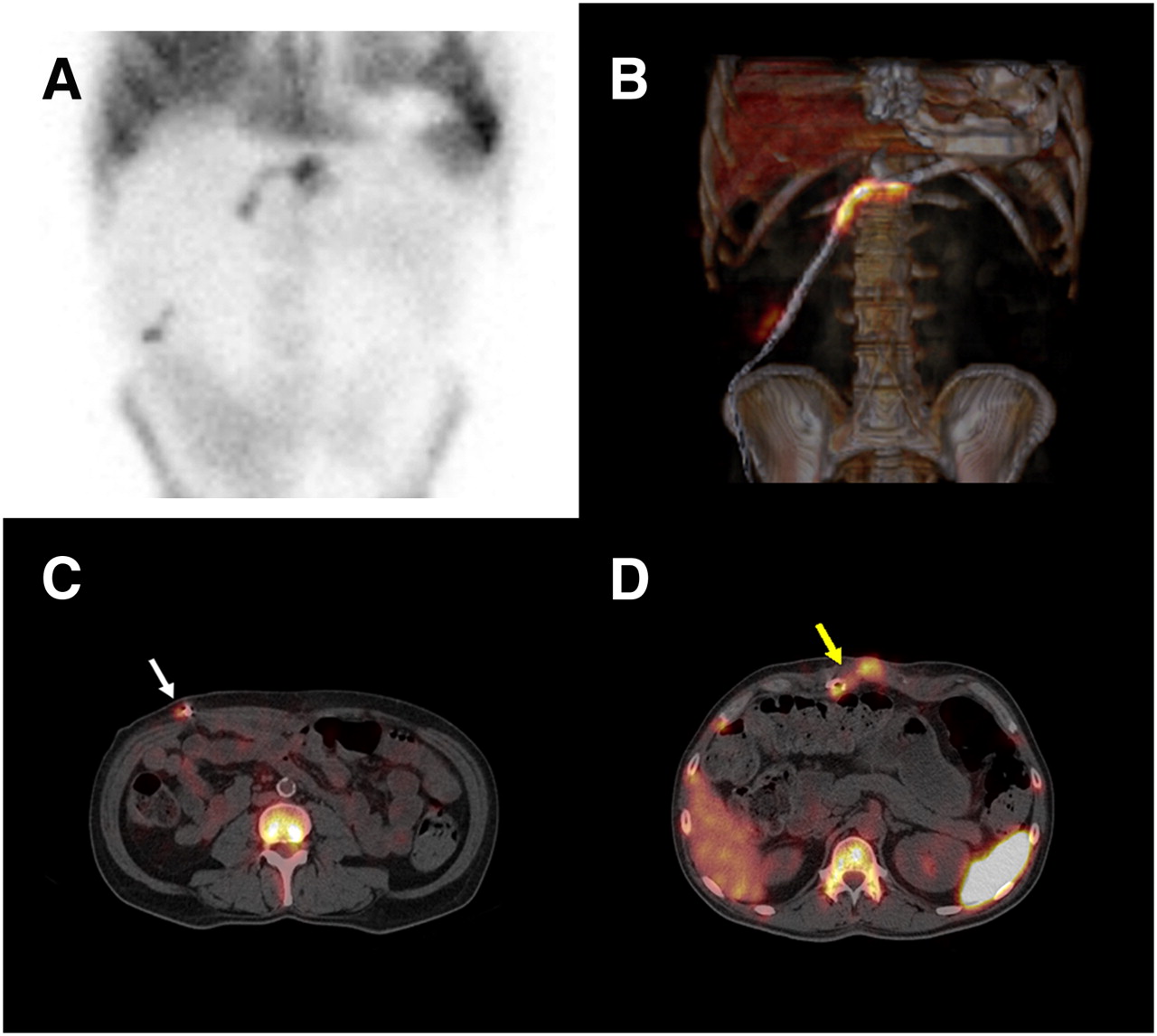
Planar and SPECT/CT images of multifocal device-related infection in patient 1. Patient had persistent infection of percutaneous site and fistulized epigastric abscess 225 d after implantation despite prolonged antibiotic therapy. (A) Planar scan demonstrates 2 foci of abnormal uptake by leukocytes. (B) Axial SPECT/CT with volume-rendering technique shows precise location and extent of infection. (C and D) First infectious focus (white arrow) was percutaneous (C), and second focus (yellow arrow), 9 cm in length, surrounded cable close to fistulized abscess (D).
SPECT/CT Scans
Foci of abnormal uptake considered positive for device-related infection were detected in 8 of 13 scans (62%), which included the 6 cases of infection detected on planar scans and 2 additional foci that were due to physiologic uptake (bone marrow and digestive excretion). In all cases, SPECT/CT provided additional information on the extent and location of infection (Figs. 2B–2D). In 5 cases (patient 3, scan 1; patient 4, scan 1; patient 6, scan 1; patient 7, scan 2; and patient 8, scan 1), SPECT/CT demonstrated a superficial infection limited to the percutaneous site (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org). In the 3 other cases (patient 1, scan 1; patient 1, scan 2; and patient 5, scan 1), SPECT/CT demonstrated deep infectious foci (Fig. 2).
In 1 of the 8 patients who had a device-related infection (patient 5, scan 1), SPECT/CT revealed 2 additional foci of abnormal distant uptake corresponding to previously unsuspected left basal pneumonitis and to an epigastric abscess near the device. The pneumonitis was near the splenic physiologic uptake, and the epigastric abscess was behind the sternum; both were therefore missed on the planar scan. These abnormal foci were confirmed by bacteriologic cultures and the patient's clinical course.
In 5 of 13 scans (38%), no device-related infection was observed. Both planar scans and SPECT/CT scans showed normal findings in 1 patient (patient 4, scan 2), who remained free from infection for several months. Distant cervical infectious foci were revealed in 2 patients by additional planar scans (no cervical SPECT/CT was performed): tonsillitis (patient 3, scan 2) associated with inflammatory uptake at the cable exit site on planar and SPECT/CT acquisitions (Supplemental Fig. 2), and an abscessed tooth (patient 5, scan 2) without any other scintigraphic abnormality (Supplemental Fig. 3). Because of the scintigraphic findings, these 2 patients received only short-term oral antibiotic treatment, and they were free of relapse for several months.
In the 2 remaining scans, isolated foci of inflammatory uptake were observed: the first (patient 2, scan 1) was a moderate focus at the cable exit site, close to physiologic digestive excretion, and detected only on SPECT/CT. This patient was weaned off the device after 692 d because the patient's heart recovered. All bacteriologic samples harvested during surgery were sterile. The second scan (patient 7, scan 1) presented foci of abnormal uptake on the shoulders, related to subcutaneous injection of antibiotics, and the patient was free of any clinical infection for more than 1 y. In these 5 of 13 scans, the scintigraphic results were considered true-negative on the basis of the patient's evolution (patient 3, scan 2; patient 4, scan 2; patient 5, scan 2; and patient 7, scan 1) or bacteriologic analysis (patient 2, scan 1).
DISCUSSION
In patients who have an LVAD, infection and sepsis have a high prevalence (23−58%) and mortality rate (15−44%) and remain a major cause of morbidity and mortality (2,12). The diagnosis and treatment of LVAD-related infection remain challenging and controversial (13,14). Microbiologic data obtained from the cable exit site or blood samples can confirm the existence of infection but fail to determine its precise location or extent. Morphologic imaging alone is unreliable because of the presence of metallic artifacts. Leukocyte scintigraphy, although representing the gold standard for specific detection of deep abscesses (15,16), lacks the anatomic landmarks that would allow for exact localization of the infection. Analysis of planar acquisitions of LVAD patients is especially difficult because of the device–anatomy relationship (splenic, urinary, and digestive hot spots) and cold artifacts generated by the metallic device. The use of SPECT/CT allows precise localization of infection and accurate interpretation of images (9). Although SPECT/CT registration mismatch may occur in areas of movement, such as the chest and upper abdomen (17), all our SPECT/CT scans provided excellent anatomic localization of the infectious foci.
When sepsis occurs in patients who have an LVAD, a device-related deep infection is always suspected. In the context of recurrent device-related infections, leukocyte scintigraphy with SPECT/CT can be repeated safely, delivering a mean effective dose equivalent to that of a diagnostic thoracic CT scan (18). Furthermore, scintigraphy allows whole-body imaging with simultaneous examination of the LVAD, enabling the detection of unsuspected sites of distant infection. In our series, leukocyte scintigraphy revealed unsuspected infectious foci in 3 examinations (23%), leading to treatment modifications.
Three imaging procedures (patient 4, scan 1; patient 5, scan 1; and patient 7, scan 1) were performed early after the LVAD implantation surgery (mean, 54 d). Although scintigraphic assessment of postoperative patients is challenging because of postoperative inflammatory reactions (19), we did not observe any false-positive results. Antibiotic strategies could be tailored to each individual patient, ranging from a short course of treatment for localized subcutaneous infections to long-term suppressive treatment for deep and persistent life-threatening infections. Interrupting antibiotics when the prosthetic material has not been removed leads, most commonly, to infection relapse. However, our series underlines the possibility of interrupting antibiotic therapy without the recurrence of infection when scintigraphic findings are normal. This possibility should be confirmed in a larger number of patients with a longer duration of follow-up.
In an era of heart-graft shortages, the high incidence of device-related infection is clearly a limitation to the implantation of an LVAD. Improved monitoring of infection by SPECT/CT, associated with advances in antibiofilm drugs, might increase the use of LVADs as the destination therapy rather than as a bridge to transplantation.
CONCLUSION
These preliminary data demonstrate the feasibility and highlight the potential usefulness of radiolabeled-leukocyte SPECT/CT in the management of infection in LVAD patients. Leukocyte SPECT/CT is able to determine the precise anatomic location and extent of a suspected infection. This noninvasive approach could improve the management of patients who have an LVAD in place long-term and should be considered when infection is suspected.
Acknowledgments
This study was supported by the A.R.C.T.C.V. (Research Association, Cardiac Surgery Department, Rouen University Hospital, Rouen, France).
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 20, 2009.
- Accepted for publication March 16, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Expanding the Scope of Multimodality Imaging in Durable Mechanical Circulatory Support
- FDG PET/CT for Early Detection and Localization of Left Ventricular Assist Device Infection: Impact on Patient Management and Outcome
- Targeting Cardiovascular Implant Infection: Multimodality and Molecular Imaging
- Positron Emission Tomography and Single-Photon Emission Computed Tomography Imaging in the Diagnosis of Cardiac Implantable Electronic Device Infection: A Systematic Review and Meta-Analysis
- SPECT/CT Assessment of Infected Intracardiac Devices With and Without Attenuation Correction
- Radiolabeled WBC Scintigraphy in the Diagnostic Workup of Patients With Suspected Device-Related Infections
- The Year in Molecular Imaging