


Abstract
CT images represent essentially noiseless maps of photon attenuation at a range of 40–140 keV. Current dual-modality PET/CT scanners transform them into attenuation coefficients at 511 keV and use these for PET attenuation correction. The proportional scaling algorithms hereby used account for the different properties of soft tissue and bone but are not prepared to handle material with other attenuation characteristics, such as oral CT contrast agents. As a consequence, CT-based attenuation correction in the presence of an oral contrast agent results in erroneous PET standardized uptake values (SUVs). The present study assessed these errors with phantom measurements and patient data. Methods: Two oral CT contrast agents were imaged at 3 different concentrations in dual-modality CT and PET transmission studies to investigate their attenuation properties. The SUV error due to the presence of contrast agent in CT-based attenuation correction was estimated in 10 patients with gastrointestinal tumors as follows. The PET data were attenuation corrected on the basis of the original contrast-enhanced CT images, resulting in PET images with distorted SUVs. A second reconstruction used modified CT images wherein the CT numbers representing contrast agent had been replaced by CT values producing approximately the right PET attenuation coefficients. These CT values had been derived from the data of 10 patients imaged without a CT contrast agent. The SUV error, defined as the difference between both sets of SUV images, was evaluated in regions with oral CT contrast agent, in tumor, and in reference tissue. Results: The oral CT contrast agents studied increased the attenuation for 511-keV photons minimally, even at the highest concentrations found in the patients. For a CT value of 500 Hounsfield units, the proportional scaling algorithm therefore overestimated the PET attenuation coefficient by 26.2%. The resulting SUV error in the patient studies was highest in regions containing CT contrast agent (4.4% ± 2.8%; maximum, 11.3%), whereas 1.2% ± 1.1% (maximum, 4.1%) was found in tumors, and 0.6% ± 0.7% was found in the reference. Conclusion: The use of oral contrast agents in CT has only a small effect on the SUV, and this small effect does not appear to be medically significant.
- PET/CT
- PET attenuation coefficient
- oral CT contrast agent
- CT-based PET attenuation correction
- attenuation correction artifact
Dual-modality PET/CT tomography performed on integrated scanners has several benefits over conventional PET imaging: The CT acquisition is rapid compared with PET transmission studies, shortening the total scan duration considerably, and provides high-quality images for anatomic correlation of functional PET images. Furthermore, the CT images are an essentially noiseless source of attenuation information usable in the reconstruction of attenuation-corrected PET images. This information is acquired with photons at energies ranging from 40 to 140 keV, whereby the effect of photoelectric absorption contributes significantly to photon attenuation. PET attenuation, however, occurs at the discrete energy of 511 keV and is dominated by Compton scattering, while photoelectric absorption is negligible for the atoms occurring in human tissue. To be usable in PET attenuation correction, the CT attenuation information must therefore be adequately transformed into linear attenuation coefficients at 511 keV, as described in several publications (1–3).
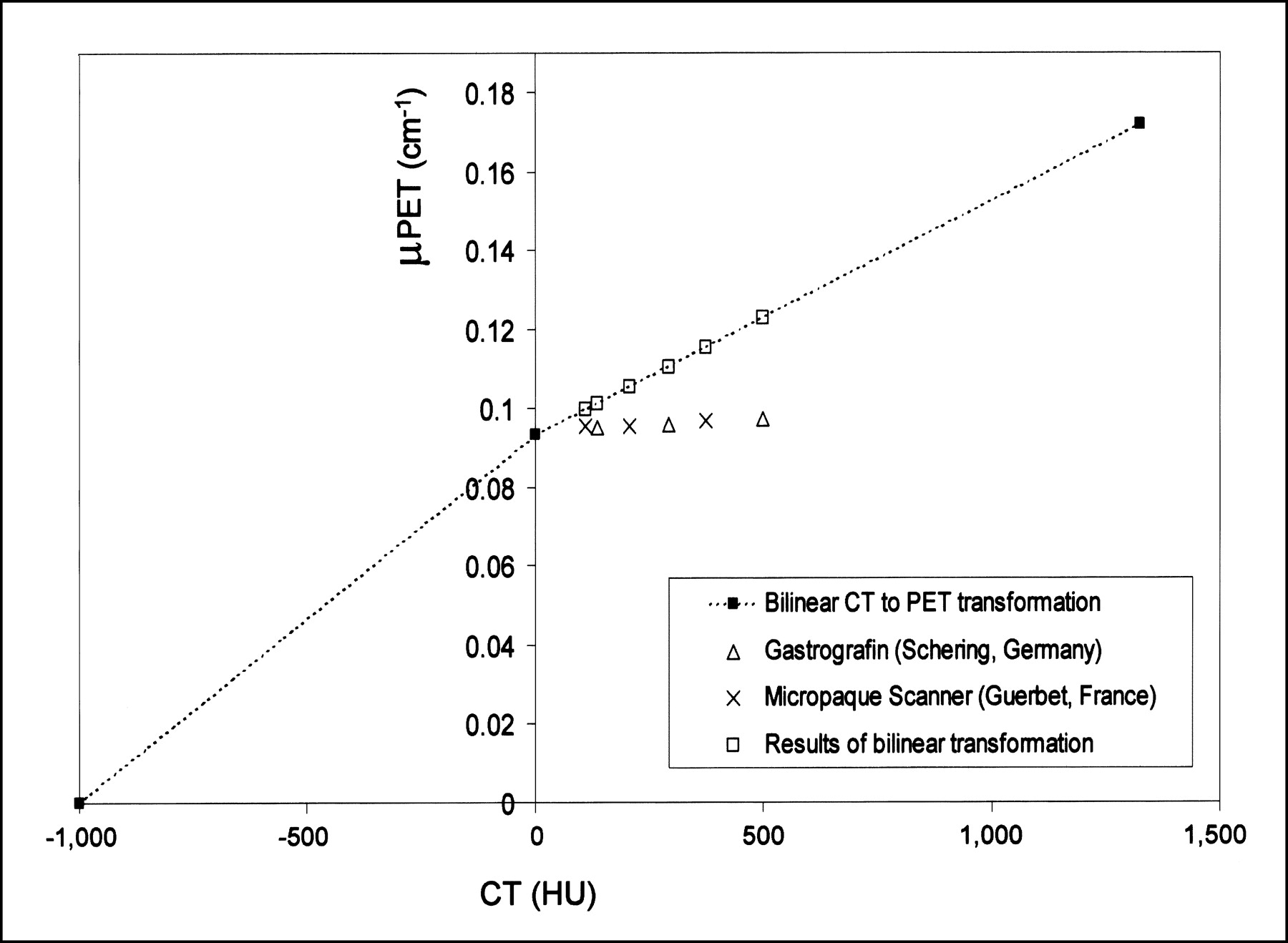
Clinical image reading of abdominal CT data is hampered by the minimal contrast between bowel loops and other abdominal organs due to the similarity in CT densities. Therefore, a contrast agent is orally administered to patients as a standard procedure in CT imaging to better delineate intestinal structures from other retro- and intraperitoneal organs. Barium sulfate and iodine-containing suspensions are widely used as oral CT contrast agents. Because of the high atomic numbers of barium (Z = 56) and iodine (Z = 53), these solutions have an increased photoelectric absorption component at the CT energies, as illustrated in Figure 1, thus highlighting the contrast-filled bowels in the CT images. At the 511-keV PET energy, however, photoelectric absorption is virtually absent even for barium and iodine. The essential problem when using contrast-enhanced CT images for PET attenuation correction, then, is that contrast agents have a significantly higher attenuation than does soft tissue in CT, whereas there is practically no difference in PET. The previously described strategies of CT-to-PET attenuation transformation (1–3), which are implemented in the current generation of PET/CT scanners, apply proportional scaling and hence neglect this effect. As a consequence, 511-keV photon attenuation is overestimated in regions containing a contrast agent, resulting in an overcorrection of the emission activity similar to the effect described in the vicinity of metals in the body (5,6).

Linear attenuation coefficient extrapolated from narrow-beam measurements at different photon energies (4). Plots 1 and 2 represent content of iodine and barium in oral CT contrast agents Gastrografin and Micropaque Scanner, respectively, mixed with water, cortical bone (plot 3), and soft tissue (plot 4). High attenuation of bone at 511 keV is due to its high density.
The aim of this study was to assess the errors in PET standardized uptake values (SUVs) induced by this effect. In a first step, the CT and PET attenuation of the oral contrast agents Gastrografin (Schering) and Micropaque Scanner (Guerbet) was measured at different concentrations in a series of phantom experiments. Furthermore, the CT density in the different sections of the gastrointestinal tract was measured in 10 patients to assess the in vivo contrast concentrations occurring at the time of the CT examination. As a reference, the average CT density in the same sections was measured in a control group of 10 patients examined without an oral CT contrast agent. In a second step, the SUV error due to the presence of contrast agent in CT images used for PET attenuation correction was directly assessed. To this end, the CT pixels representing oral contrast agent were replaced by the normal density values measured in the control group, and the PET emission data were attenuation corrected with this modified set of CT data. The SUVs obtained with correction by the original and the modified CT values were compared in tumor, in regions containing contrast agent, and in a reference region.
MATERIALS AND METHODS
Patient Selection
From February to June 2002, 10 patients were selected who underwent combined whole-body PET/CT with oral CT contrast agent. The selection criterion was the presence of a slice showing contrast enhancement in the CT image close to a tumor with high 18F-FDG uptake. The patients (8 men, 2 women; mean age, 56.2 y; age range, 20–79 y) had the following gastrointestinal diseases: Two had carcinoma of the stomach, 1 had a gastrointestinal stroma tumor of the small bowel, and 7 had carcinoma of the large bowel. These patients received contrast agent 1 h before PET/CT scanning: Four received 1,000 mL of Gastrografin, an iodine-based CT contrast agent, and the other 6 received 1,000 mL of a 1.5% diluted barium sulfate suspension (Micropaque Scanner). The control group (5 men, 5 women; mean age, 67.3 y; age range, 51–82 y) was selected from patients scheduled for radiation therapy who underwent a PET/CT study without oral CT contrast agent and who had no gastrointestinal tract tumors.
Patient Data Acquisition
All data acquisitions and reconstructions were performed on a commercial PET/CT system (Discovery LS; General Electric Medical Systems). The patients fasted for at least 4 h before the PET/CT study. One hour before the start of the examination, the oral CT contrast agent was administered, if applicable, and 45 min before the start of the examination, 370 MBq (10 mCi) of 18F-FDG were injected. The patient was positioned on the table in a head-first, supine position. Six to 7 contiguous volumes covering 867–1,011.5 mm were chosen carefully to ensure data acquisition of the entire region of interest (ROI), including the level of the pelvic floor to the cerebellum. The arms of the patient were elevated above the abdomen to reduce beam-hardening artifacts at the level of the liver. CT data were acquired first, with the following parameters: tube-rotation time, 0.5 s per revolution; 140 kV; 80 mA; 22.5 mm per rotation; a slice pitch of 6 (high-speed mode); and an acquisition time of 22.5 s for a scan length of 867 mm. Subsequently, PET emission data were acquired in 2-dimensional mode starting at the pelvis. Emission counts were collected during 4 min per table position, and adjacent fields of view shared 1 overlapping slice. Matched CT and PET images were reconstructed with a field of view of 500 mm and a 4.25-mm slice thickness. An iterative reconstruction (ordered-subsets expectation maximization with 2 iterations and 28 subsets) and CT-based attenuation correction were used for the PET SUV images.
Phantom Data Acquisition
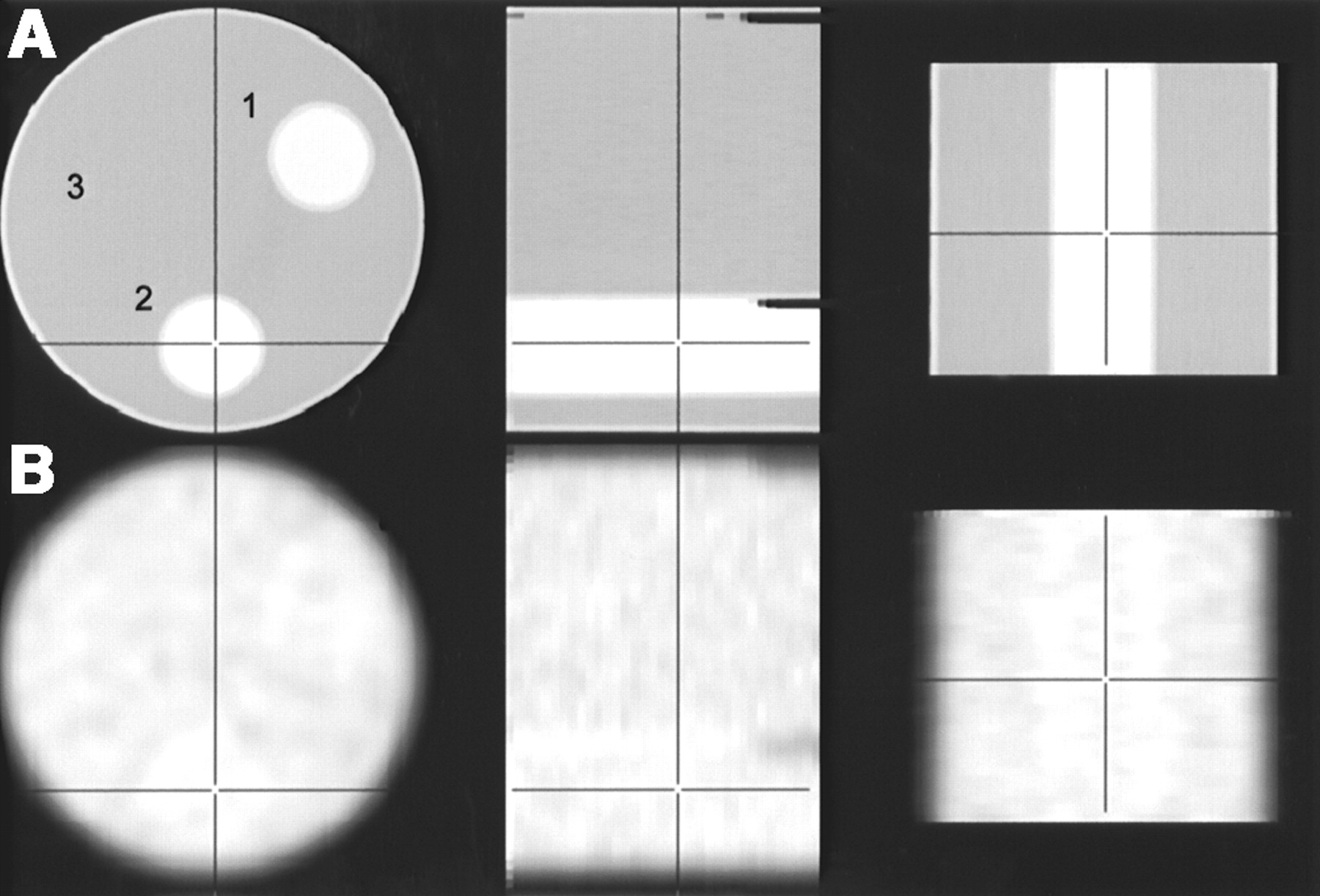
A National Electrical Manufacturers Association phantom was prepared with 2 cylindric inserts, as illustrated in Figure 2. One of the inserts was filled with Gastrografin, the other with Micropaque Scanner; the main cylinder contained water. Three configurations of the phantom were prepared whereby the CT contrast concentrations in the inserts varied: The first configuration represented the clinical concentration that was administered to the patients (Gastrografin: 30 mL diluted to 1 L; Micropaque: 150 mL diluted to 0.5 L), and the concentration was halved and doubled in the second and third configurations, respectively. These 3 phantom configurations were imaged in dual-modality acquisitions by CT and transmission PET. The CT images were acquired with 160 mA for better image statistics and with the other parameters as described above. The PET transmission measurements were performed with the 2 built-in 68Ge rod sources and an acquisition duration of 30 min. From these data, quantitative PET attenuation maps (in cm−1) were reconstructed by filtered backprojection and were inherently matched with the CT images.

Attenuation images of NEMA phantom containing 2 cylindric acrylic inserts with oral CT contrast agent in clinical concentrations. Row A shows orthogonal CT sections (140 kV, 160 mA); row B shows matched PET transmission images acquired with 68Ge rods in 30 min. Slight attenuation increase originating from insert walls is notable in transmission images. 1 = Micropaque Scanner; 2 = Gastrografin; 3 = water.
Image Analysis
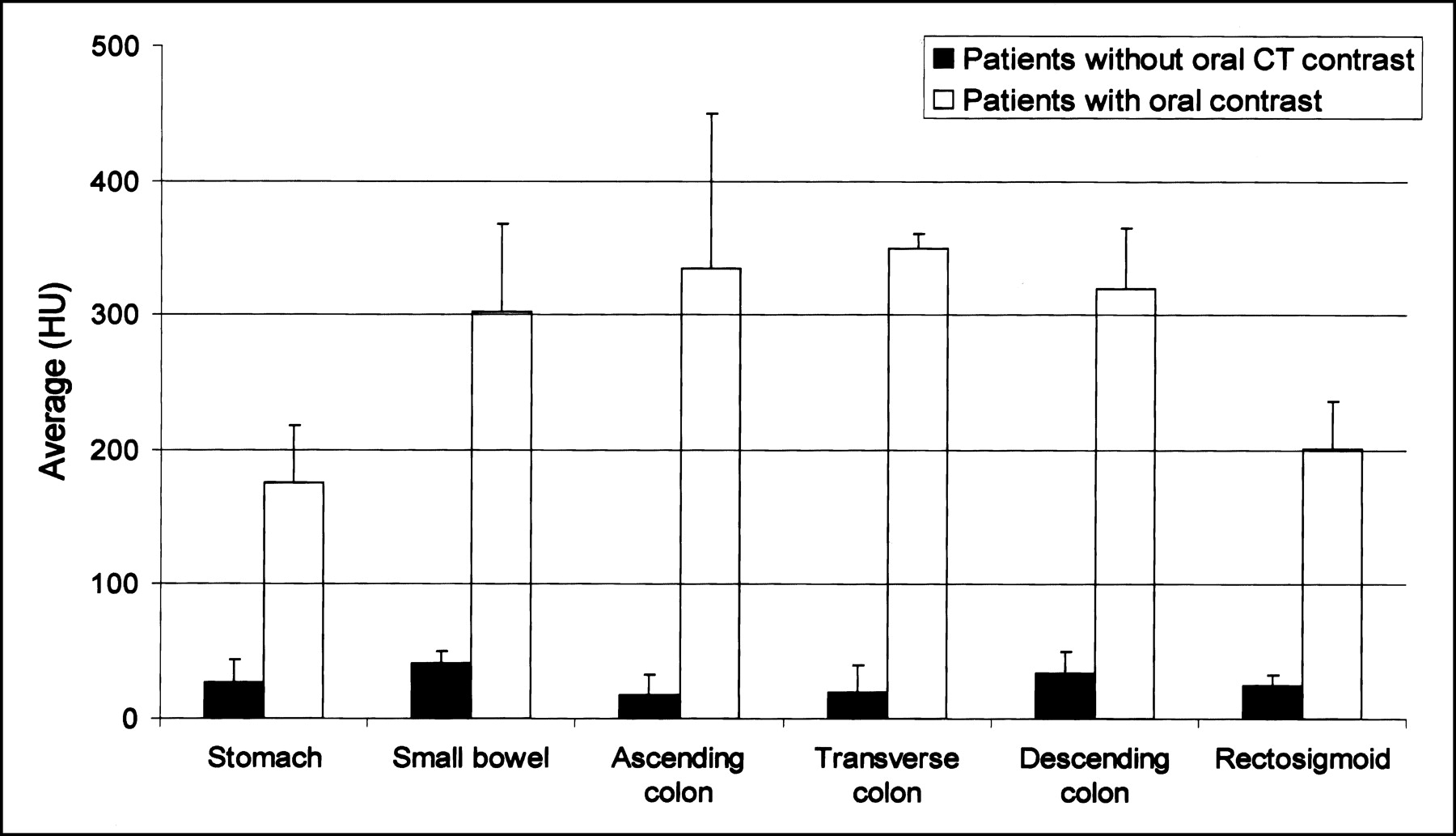
The gastrointestinal tract was divided into the 6 sections: stomach, small bowel, ascending colon, transverse colon, descending colon, and rectosigmoid. ROIs in these sections were manually outlined in the CT images of the 10 control patients, and the average CT value in Hounsfield units (HU) was calculated. The same procedure was performed on the CT images of the patients who had received oral CT contrast agent.
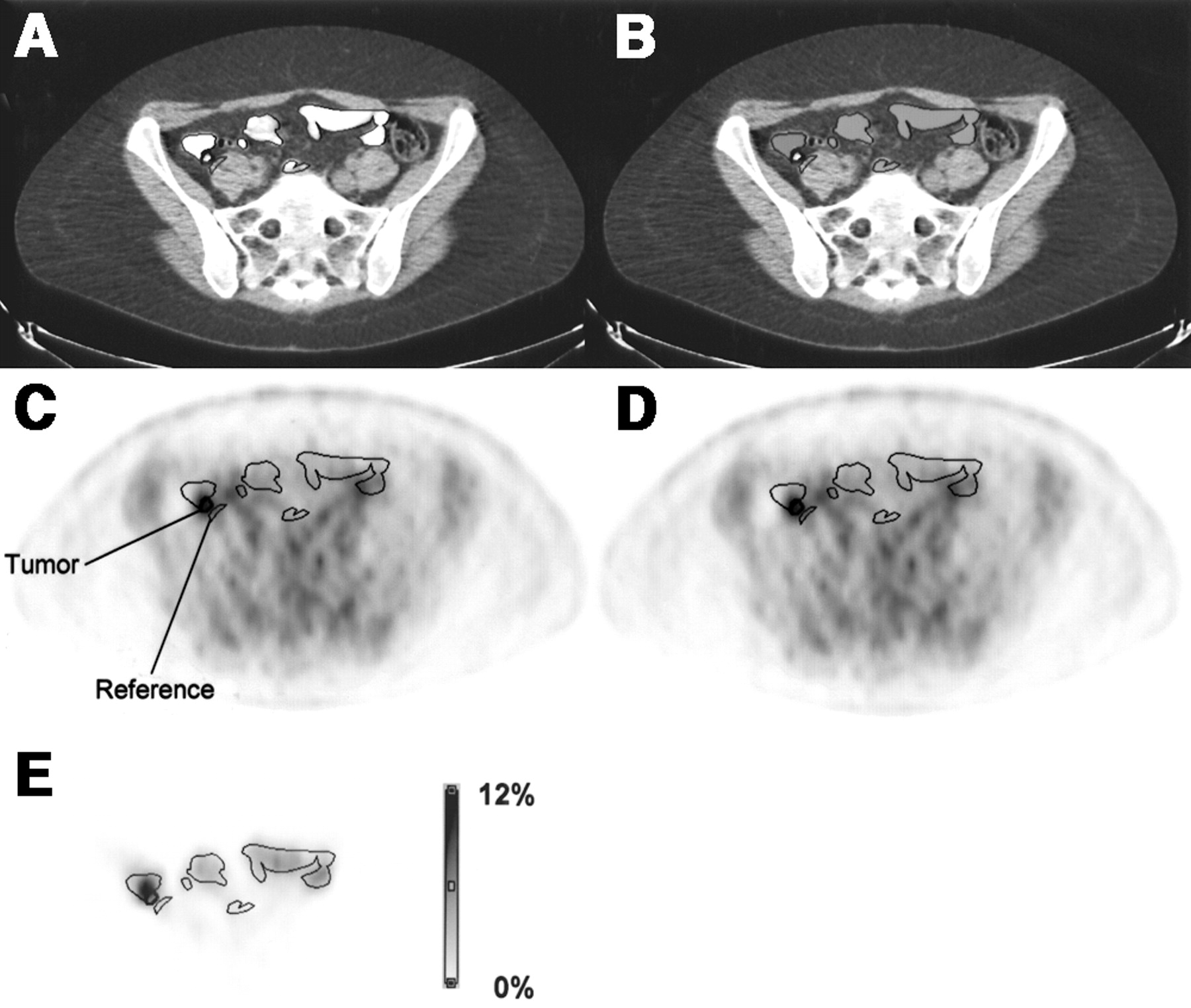
To assess the error induced by the presence of contrast enhancement in CT-based attenuation correction of PET data, the following processing steps were performed: The particular slice that showed significant contrast enhancement in the CT image and maximal 18F-FDG uptake by tumor in the PET image was identified as illustrated in Figure 3. The contrast region was manually outlined in the CT image, and the CT values in this ROI were replaced by the average CT value found in the control group for that particular gastrointestinal section. A similar modification was done in 1 adjacent slice. The modified CT values were then sent back to the PET/CT operator console and used to reconstruct a second set of PET SUV images. These PET images (PETcorr) were assumed to represent an approximation of the correct distribution of PET activity, since the wrong scaling of the contrast-containing pixels was avoided by the CT value replacement. The SUVs of the original PET images and the PETcorr images were compared in the contrast ROIs, in a ROI around the tumor, and in a reference ROI close to the tumor covering neither tumor nor contrast-enhanced CT areas. All processing steps except for image reconstruction were performed offline with the commercially available PMOD software (PMOD Group (7)), and data were exchanged using the Digital Imaging and Communications in Medicine protocol.
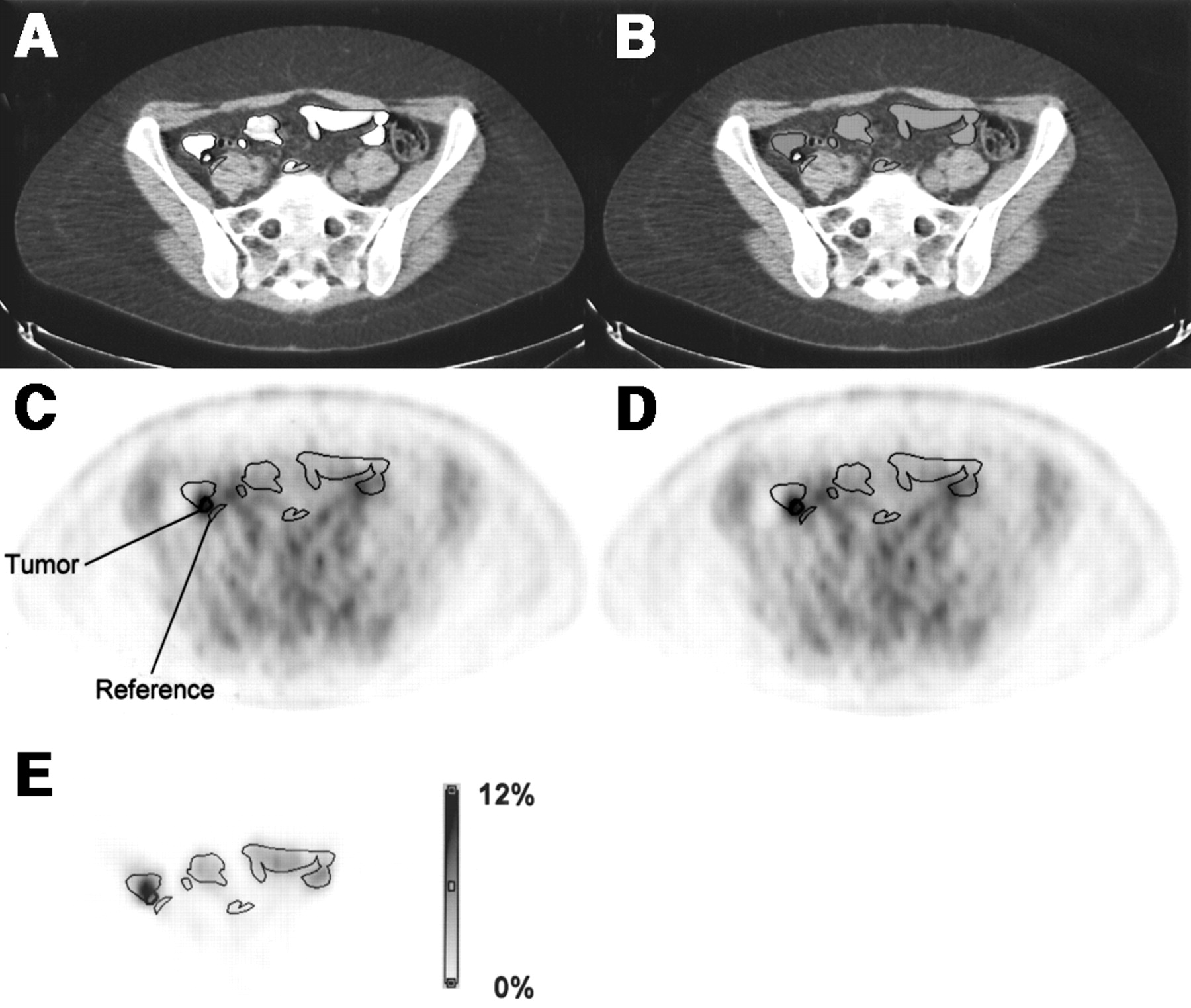
Example of the performed analysis. (A) CT image with thresholds [−160 HU, 240 HU] showing regions that define oral CT contrast, tumor, and reference tissue. (B) CT image after replacement of contrast-enhanced pixels by normal values. (C) PET emission image attenuation corrected with CT image A. (D) PET emission image attenuation corrected with CT image B, resulting in approximation of true 18F-FDG uptake. (E) Difference image C − D normalized to D, showing percentage error due to attenuation correction with CT contrast-enhanced pixels. Maximal difference is 9.6%.
RESULTS
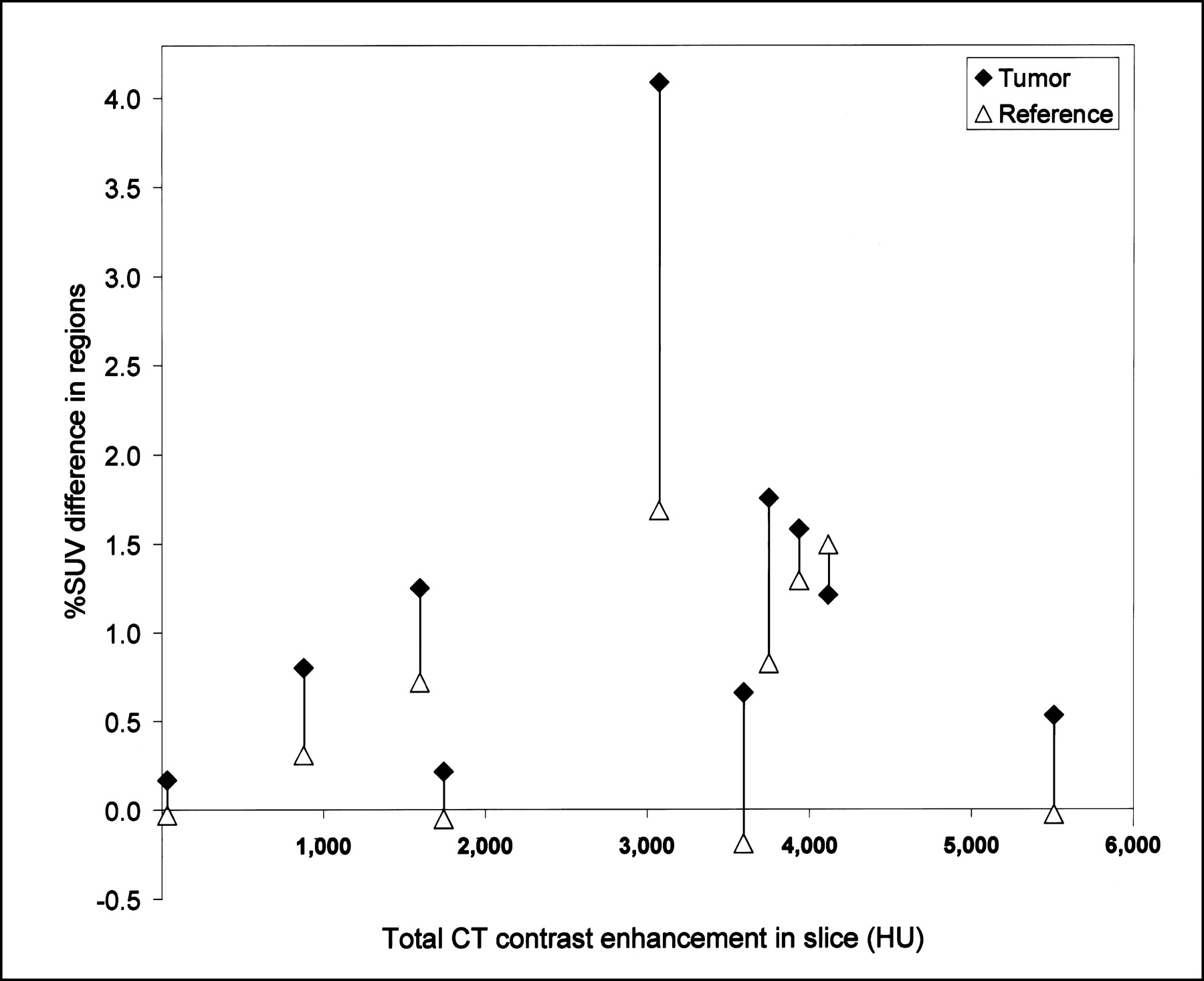
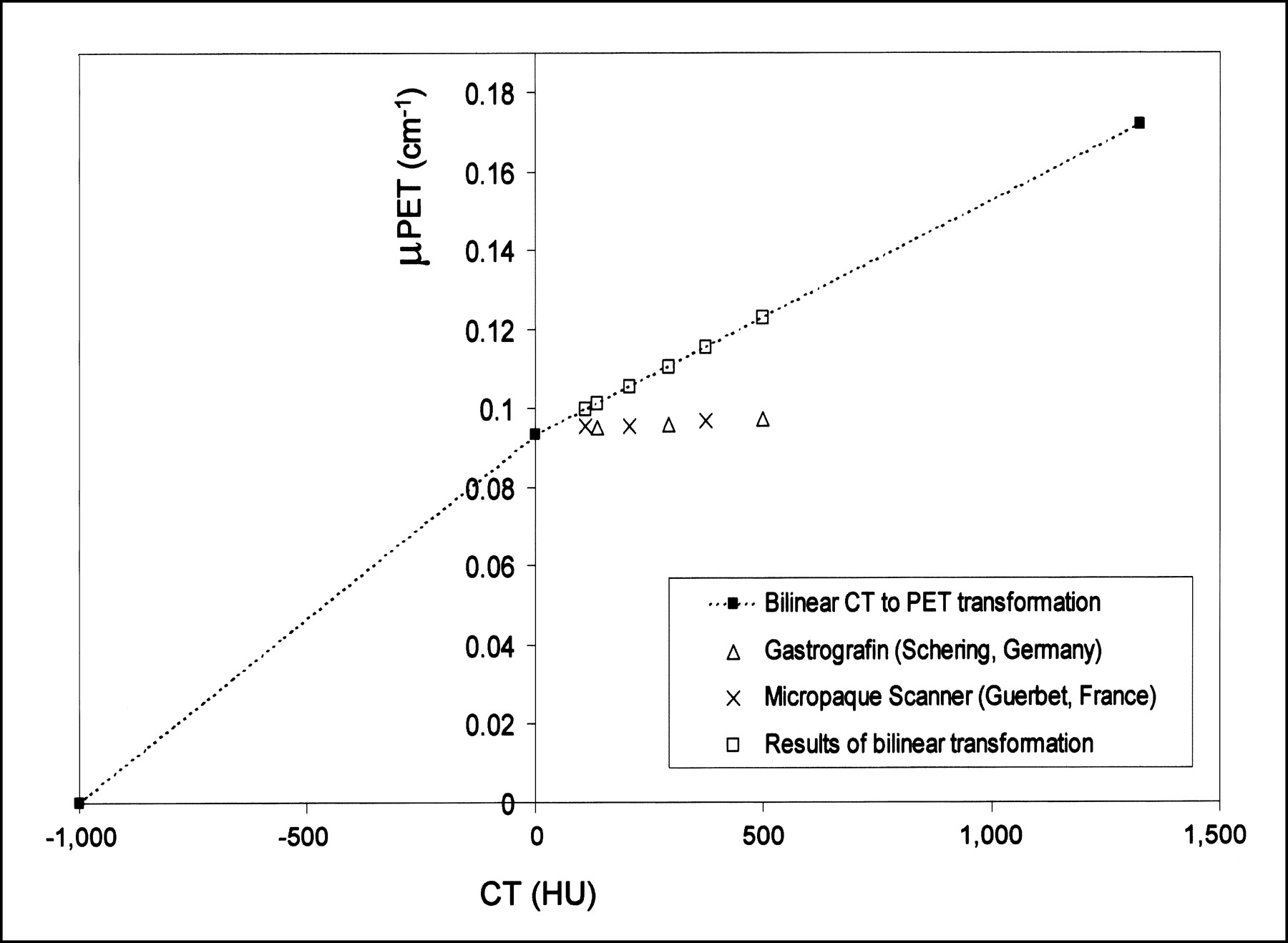
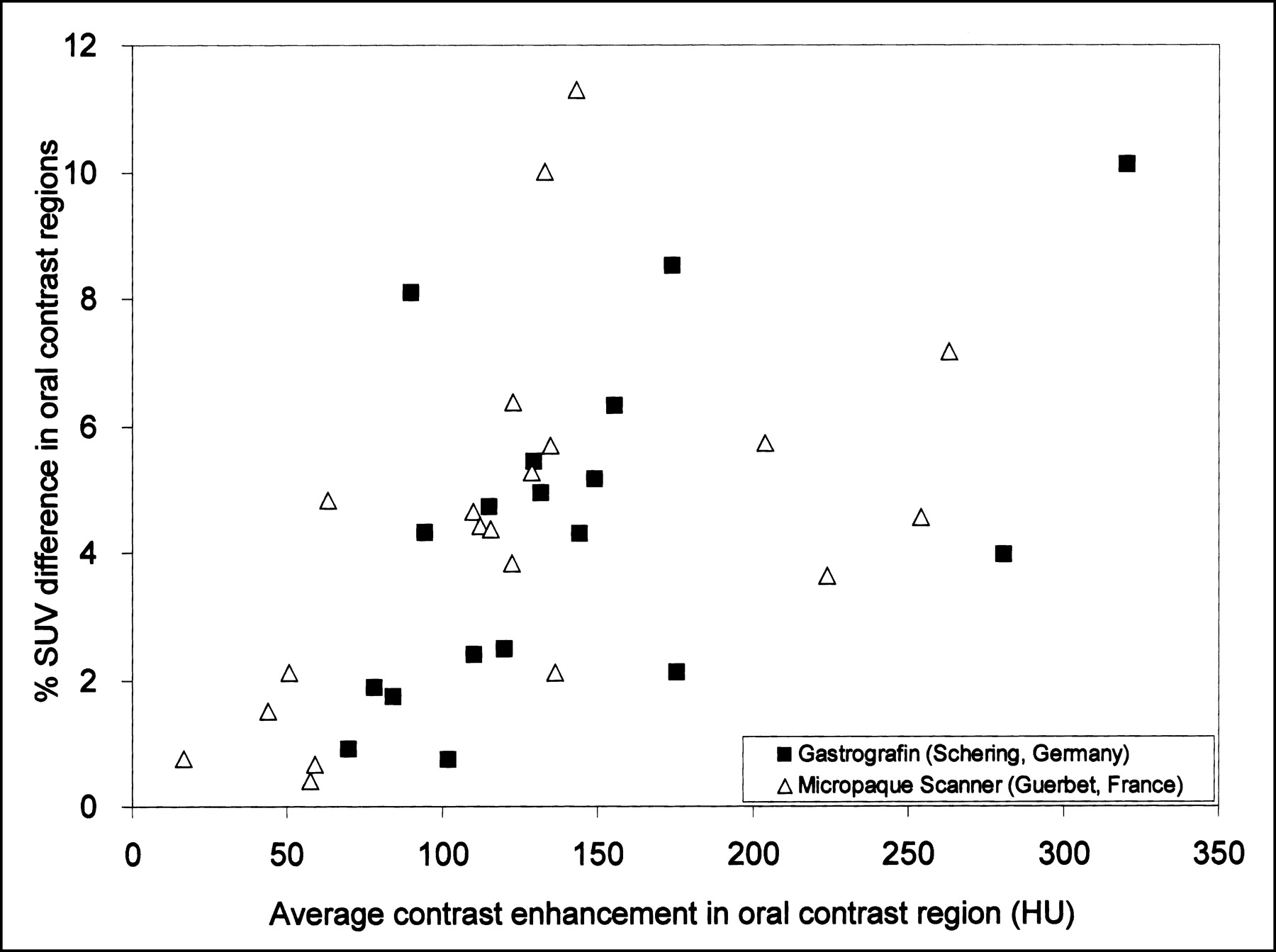
The results of the phantom experiments with different concentrations of the CT contrast agents are shown in Figure 4. The average attenuation measured with transmission PET is plotted as a function of the measured CT attenuation. If these CT values are subjected to the CT-to-PET transformation of the Discovery LS, too high PET attenuation coefficients are calculated. This overestimation ranges from 2.5% (77 HU) to 26.2% (500 HU). The CT values measured in the gastrointestinal ROIs in the patient studies with and without oral CT contrast agent are summarized in Table 1. To illustrate the different concentration of the oral contrast agent along the gastrointestinal tract 60–90 min after administration, the CT ROI averages are shown in Figure 5. The data resulting from the attempt to quantify the contrast-induced error of the SUVs in the patient studies are shown in Figures 6 and 7. It was assumed that PETcorr, the SUV images obtained when correcting with the contrast-removed CT images, represented a good approximation of the true SUVs. Consequently, the difference between PET and PETcorr, expressed as a percentage of PETcorr, served as a measure of the SUV error. Figure 6 shows the SUV overestimation in the 38 image regions with oral contrast agent in the underlying CT images (volume, 7.1 ± 10.0 mL). In the patient population studied, the error ranged up to 11.3%. Figure 7 shows the error found for tumor and reference tissue. It illustrates that the contrast-related overcorrection also has a moderate effect on remote tissues. The tumor and reference region volumes were 2.2 ± 2.4 mL and 2.2 ± 2.9 mL, respectively.
Average attenuation of 2 oral CT contrast agents at 3 different concentrations measured in CT and with PET 511-keV transmission scans. CT attenuation increases with increasing concentration of contrast agent. PET attenuation, however, depends minimally on concentration of contrast agent and is only slightly higher than attenuation of water. Transformation applied by scanner software to convert CT numbers into PET attenuation coefficients in Discovery LS scanner is indicated as dashed line (3). If it is applied to measured CT numbers, too high PET attenuation coefficients are calculated (□).
Average HU and SD measured in different sections of gastrointestinal tract for control group studied without oral contrast agent and for patient group.

Overestimation of SUV in image regions containing oral CT contrast agent. Shown is percentage SUV error induced by CT-based PET attenuation correction with contrast enhancement present in CT images.
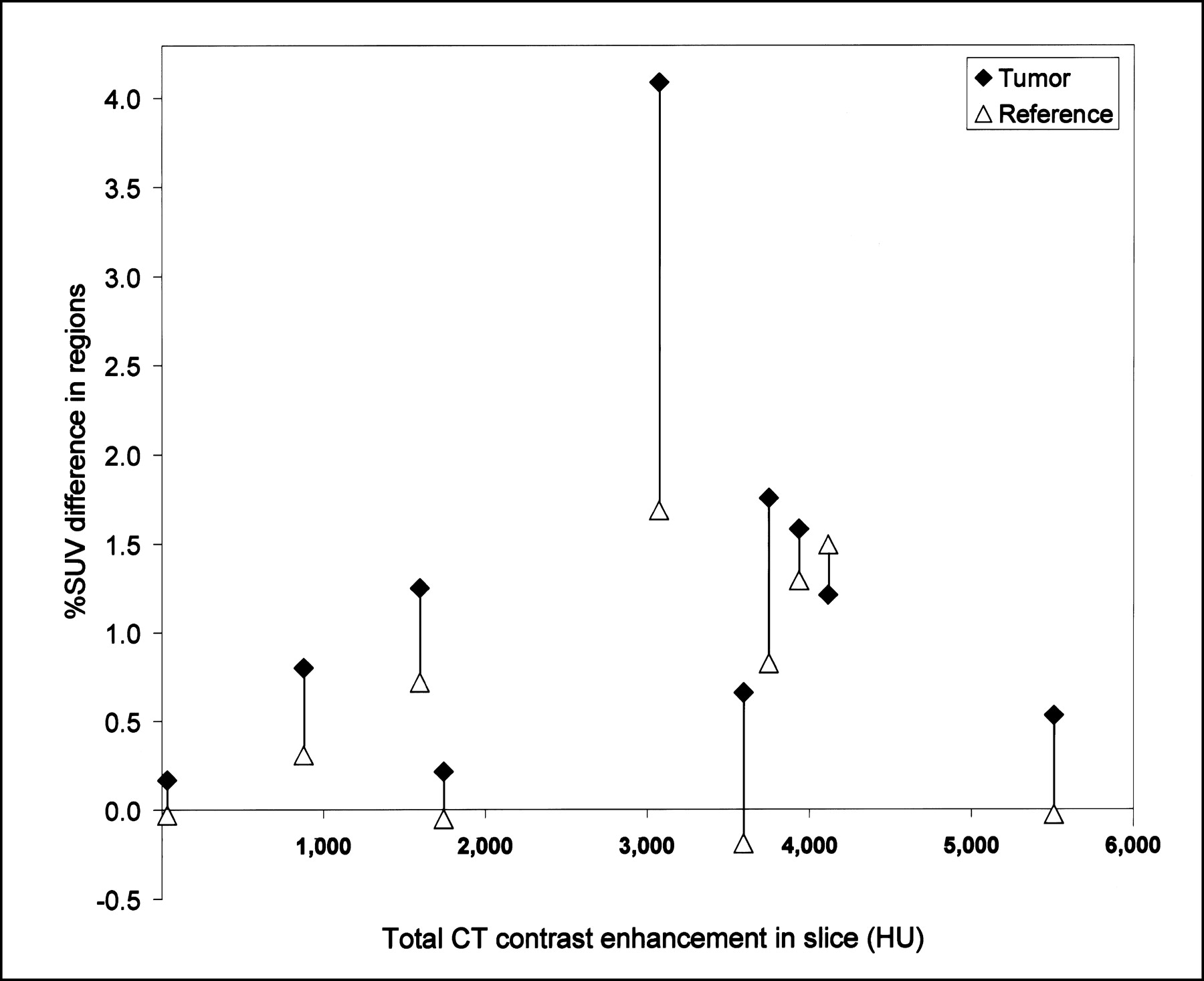
Overestimation of SUV in image regions absent of oral CT contrast agent. Shown is percentage SUV error induced by CT-based PET attenuation correction with CT contrast enhancement present in other parts of image.
CT Values Measured in ROIs of Different Gastrointestinal Tract Sections
DISCUSSION
One of the key diagnostic advantages of dual-modality PET/CT tomography is the availability of anatomic CT images matched to the functional PET images. However, standard procedures in radiology require that CT acquisitions of the abdomen be performed with oral contrast agents for an improved delineation of intestinal structures from other retro- and intraperitoneal organs. To optimize the acceptance and diagnostic value of PET/CT in diseases of the abdomen, the studies should therefore also be performed with an oral CT contrast agent. A problem arises if the contrast-enhanced CT images are used for attenuation correction of the PET emission data. The reason is that the attenuation characteristics of the CT contrast agents at the CT and the PET photon energies differ from those of human tissue. We have performed phantom experiments with 2 types of oral CT contrast agents, which enhance contrast by the presence of barium (Micropaque) or iodine (Gastrografin) atoms (Fig. 2). The results at different concentrations clearly demonstrate that an increase of CT contrast agent results in an increase of the attenuation measured by CT, as expected (Fig. 4). For PET, however, the presence of CT contrast agent is practically irrelevant. Even at a CT value of 500 HU, which is in the range of compact bone, the PET attenuation is elevated by merely 3.9%. The algorithm in the Discovery LS that calculates the PET attenuation coefficients from CT numbers ignores this effect. As a consequence, the PET attenuation coefficient of CT contrast agent is overestimated, up to 26.2% for the equivalent of 500 HU. When these CT-derived coefficients are applied for the correction of photon attenuation in PET, they cause an overcorrection of the effect. The result is an elevated activity most pronounced at the location of CT contrast agent but also affecting other regions within a slice.
To assess the magnitude of the expected artifacts with oral contrast agents, we reconstructed the PET data of 10 patients with gastrointestinal tumors twice with different CT-based attenuations. The first reconstruction used the original contrast-enhanced CT images. The second reconstruction used modified CT images wherein pixel values corresponding to oral contrast agent were replaced with normal CT values that had been measured in a control group absent of oral CT contrast agent. This replacement was based on the observation that CT contrast agents only minimally change PET attenuation over the range found in the patients and on the assumption that normal CT numbers would have been measured if the patients had not been given oral contrast agent. Because the calculation of the attenuation correction factors from the CT images includes spatial smoothing and forward projection, the use of discrete CT values instead of a continuous distribution is not expected to be a problem for quantification. Therefore, the PET images corrected with the modified CT data were assumed to provide a good approximation of the true PET SUV and served as the reference in the error calculations. This approach has several advantages over the comparison with transmission-corrected PET images. High-quality transmission studies expose patients to an additional radiation dose and are prone to patient motion due to the prolonged acquisition time. Furthermore, we avoided the problem of the remaining bias of CT-corrected PET images relative to transmission corrected images on the scanner used in the present study (8).
Figure 6 demonstrates that contrast agent in the CT image may induce an elevated 18F-FDG uptake in the PET image, which increases with increasing contrast concentration. The maximal error found was 11.3%, and the average error was 4.4% ± 2.8%. We have assessed the concentration of oral CT contrast agent in the different gastrointestinal sections and found a maximum CT value of 520 HU (Table 1). Because a CT contrast of 500 HU results in an error of the derived attenuation coefficient of 26.2% (Fig. 4) on the Discovery LS, we expect the maximal errors to remain well below 30%. A similar effect will most likely occur with other PET/CT scanners that rely on simple bilinear scaling to transform from CT to PET attenuation. However, if notable at all, these mimicked 18F-FDG uptakes will not be critical for clinical interpretation. It is worth mentioning that 18F-FDG uptake within a lumen can be increased only if a certain 18F-FDG concentration is present in the intraluminal fluid collection by a physiologic cause such as an 18F-FDG excretion from the intestinal glandular structures, as hypothesized by Dizendorf et al. (9).
All the patients had a gastrointestinal tumor with high 18F-FDG uptake in the slices examined. Tumor uptake was affected by the presence of CT contrast agent in the gastrointestinal sections within the slice, as demonstrated in Figure 7. There was a clear trend for the error to increase with increasing CT contrast in a slice. The overcorrection error ranged to a maximum of 4.1% for 1 small tumor in the direct neighborhood of a highly enhanced ascending colon section (338 HU) and was 1.2% ± 1.1% on the average. In reference tissue, the error was smaller, ranging from −0.2% to 1.3% and averaging 0.6% ± 0.7%. These results suggest that the tumor SUV overestimation induced by the presence of oral CT contrast agent will most likely change neither the visual appearance nor the grading of a tumor, since the reproducibility of the SUVs is reported in the range of 9%–10% (10,11).
CONCLUSION
We have shown that oral CT contrast agent behaves differently from human tissue with regard to photon attenuation at the CT and PET energies. If this behavior is not considered in CT-based attenuation correction, the presence of CT contrast agent causes an SUV overestimation. In a patient population having gastrointestinal tumors that are likely to produce the most severe artifacts, the SUV errors found for the tumors remained below the reproducibility of PET. Larger SUV errors occur in the gastrointestinal sections filled with CT contrast agent, but they can be managed on the basis of the CT images. We conclude that the use of oral contrast agent in CT introduces only a small effect in the SUV and that this small effect does not appear to be medically significant. However, it seems advisable to further develop the algorithms that transform CT values into PET attenuation coefficients. Improved methods must detect CT pixels representing oral contrast agent in a segmentation process and assign an adequate PET attenuation coefficient.
Acknowledgments
The authors thank Thomas Berthold for technical assistance. This study was supported by the Radium Foundation, University of Zurich, Switzerland.
Footnotes
Received Jul. 25, 2002; revision accepted Jan. 13, 2003.
For correspondence or reprints contact: Cyrill Burger, PhD, Division of Nuclear Medicine, University Hospital of Zurich, Raemistrasse 100, CH-8091, Zurich, Switzerland.
E-mail: burger{at}dmr.usz.ch
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SPECT/CT Assessment of Infected Intracardiac Devices With and Without Attenuation Correction
- Standards for PET Image Acquisition and Quantitative Data Analysis
- Measuring Response with FDG-PET: Methodological Aspects
- Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration
- Limitations of CT During PET/CT
- Effective Methods to Correct Contrast Agent-Induced Errors in PET Quantification in Cardiac PET/CT
- Evaluation of Image Registration in PET/CT of the Liver and Recommendations for Optimized Imaging
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- The 2006 Henry N. Wagner Lecture: Of Mice and Men (and Positrons)--Advances in PET Imaging Technology
- PET/CT in Lymphoma: Prospective Study of Enhanced Full-Dose PET/CT Versus Unenhanced Low-Dose PET/CT
- Procedure Guideline for SPECT/CT Imaging 1.0
- PET/CT Imaging Artifacts
- Concurrent PET/CT with an Integrated Imaging System: Intersociety Dialogue from the Joint Working Group of the American College of Radiology, the Society of Nuclear Medicine, and the Society of Computed Body Tomography and Magnetic Resonance
- Optimized Intravenous Contrast Administration for Diagnostic Whole-Body 18F-FDG PET/CT
- Do Implanted Pacemaker Leads and ICD Leads Cause Metal-Related Artifact in Cardiac PET/CT?
- Accuracy of Whole-Body Dual-Modality Fluorine-18-2-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography and Computed Tomography (FDG-PET/CT) for Tumor Staging in Solid Tumors: Comparison With CT and PET
- Technical Issues in Performing PET Studies in Pediatric Patients
- PET/CT: Panacea, Redundancy, or Something in Between?
- To Enhance or Not to Enhance? 18F-FDG and CT Contrast Agents in Dual-Modality 18F-FDG PET/CT
- PET/CT in Colorectal Cancer