


Abstract
Cardiac sympathetic nerve activity is changed in patients with hypertrophic cardiomyopathy (HCM). However, the relationship between heterogeneity of this activity and systolic left ventricular dysfunction in patients with HCM is not well established. This study was performed to evaluate the sympathetic nerve activity in various cardiac regions and to investigate the relationship between cardiac dysfunction and heterogeneity of the cardiac sympathetic nerve activity in patients with HCM. Methods: Cardiac sympathetic nerve activity was evaluated in 25 patients with HCM and 10 control subjects using planar imaging and SPECT by 123I-metaiodobenzylguanidine (MIBG) myocardial scintigraphy. With planar 123I-MIBG imaging, the heart-to-mediastinum activity ratios (H/M), at early (20 min) and delayed (3 h) acquisition, and the washout rate were calculated. Polar maps of the left ventricular myocardium were divided into 20 segments, and the dispersion (maximal to minimal values) and SD of uptake and the washout rate in 20 segments were calculated. Results: The early H/M did not differ between the 2 groups. The delayed H/M was significantly lower and the washout rate of the whole heart was significantly higher in the HCM group than those in the control group. In patients with HCM, the delayed H/M, early uptake dispersion, and SD of early uptake showed good correlation with the left ventricular end-diastolic and end-systolic dimensions and the percentage of fractional shortening. A stepwise regression analysis revealed that the SD of early uptake was a powerful determinant for the percentage of fractional shortening in patients with HCM. Conclusion: These results suggest that the heterogeneity of regional cardiac sympathetic nerve activity may be correlated with cardiac dysfunction in patients with HCM.
Hypertrophic cardiomyopathy (HCM) is an inherited cardiac muscle disease and can be caused by a mutation in the genes that encode proteins in the sarcomere (1,2). Morphologic and functional characteristics of HCM include disproportionate left ventricular hypertrophy and diastolic dysfunction. However, some patients with HCM have systolic dysfunction and show dilated cardiomyopathy-like features (3,4). Using 123I-metaiodobenzylguanidine (MIBG) myocardial scintigraphy, we reported that patients with HCM and systolic dysfunction have an increased 123I-MIBG clearance (5). In addition, Brush et al. (6) found decreased neuronal uptake and metabolism of norepinephrine in patients with HCM. These results suggest that cardiac sympathetic nerve activity may play an important role in the maintenance of cardiac function in patients with HCM. However, the relationship between cardiac dysfunction and change in homogeneity of regional cardiac sympathetic nerve activity in patients with HCM is unclear. This study was performed to evaluate the sympathetic nerve activity in various cardiac regions and to investigate the relationship between cardiac dysfunction and heterogeneity of the cardiac sympathetic nerve activity in patients with HCM.
MATERIALS AND METHODS
Patients
The study group consisted of 25 patients with HCM (19 men, 6 women; mean age, 48.5 ± 12.7 y) and 10 age- and sex-matched control subjects (7 men, 3 women; mean age, 49.8 ± 15.2 y). The diagnosis of HCM was based on the echocardiographic demonstration of a nondilated, hypertrophied left ventricle in the absence of other cardiac or systemic causes for the left ventricular hypertrophy (7). Patients with hypertension, diabetes mellitus, or atrial fibrillation were excluded from the study. Informed consent was obtained from all subjects before participating in the study in accordance with the guidelines of Kanazawa University Hospital Human Subjects Committee.
Evaluation of Cardiac Sympathetic Nerve Activity
Patients were instructed to fast on the day of the radionuclide study and to continue fasting until the study was completed. No patients were taking reserpine or tricyclic antidepressants at the time of the study. An intravenous injection of 120–140 MBq 123I-MIBG was given between 9:00 and 10:00 am. Planar scintigraphic imaging in the anterior view and SPECT were performed 20 min (early) and 3 h (delayed) after 123I-MIBG injection. The SPECT system (model 9300A; Toshiba, Tokyo, Japan) consisted of a triple-head scintillation camera. The energy discrimination was centered on 159 keV with a 20% window; a total of 60 projection images were obtained in a 64 × 64 matrix over a 360° arc in 6° increments with 30-s acquisitions for each view. Tomographic images were reconstructed using a ramp filter with a Butterworth filter (order, 8; cutoff frequency, 0.47 cycle/cm). Attenuation correction was not performed.
Whole cardiac 123I-MIBG uptake was measured as the heart-to-mediastinum activity ratio (H/M) on a planar image. The region of interest (ROI) was drawn manually over the whole left ventricle, and a rectangular ROI was set on the upper mediastinum in the early image and then the same ROIs were applied to the delayed image. Values of H/M were calculated by dividing the count density of the whole heart by that of the mediastinum. The washout rate was calculated using the following equation: washout rate = (Ec − Dc) × 100/Ec, where Ec is the early cardiac count density and Dc is the decay-corrected delayed cardiac count density.
Polar maps of all patients with HCM were divided into 20 segments (Fig. 1). An ROI was placed on each of the 20 segments. The maximal count in the polar map representing the entire left ventricular myocardium was normalized to 100, and the segmental early uptake was calculated as a ratio of the maximal count. In addition, the early uptake, delayed uptake, and washout rate of each segment were obtained. The SDs of the early uptake, delayed uptake, and washout rate in 20 segments and the differences of maximal and minimal values (dispersions) of segmental early uptake, delayed uptake, and washout rate were calculated as indices of regional 123I-MIBG variation.
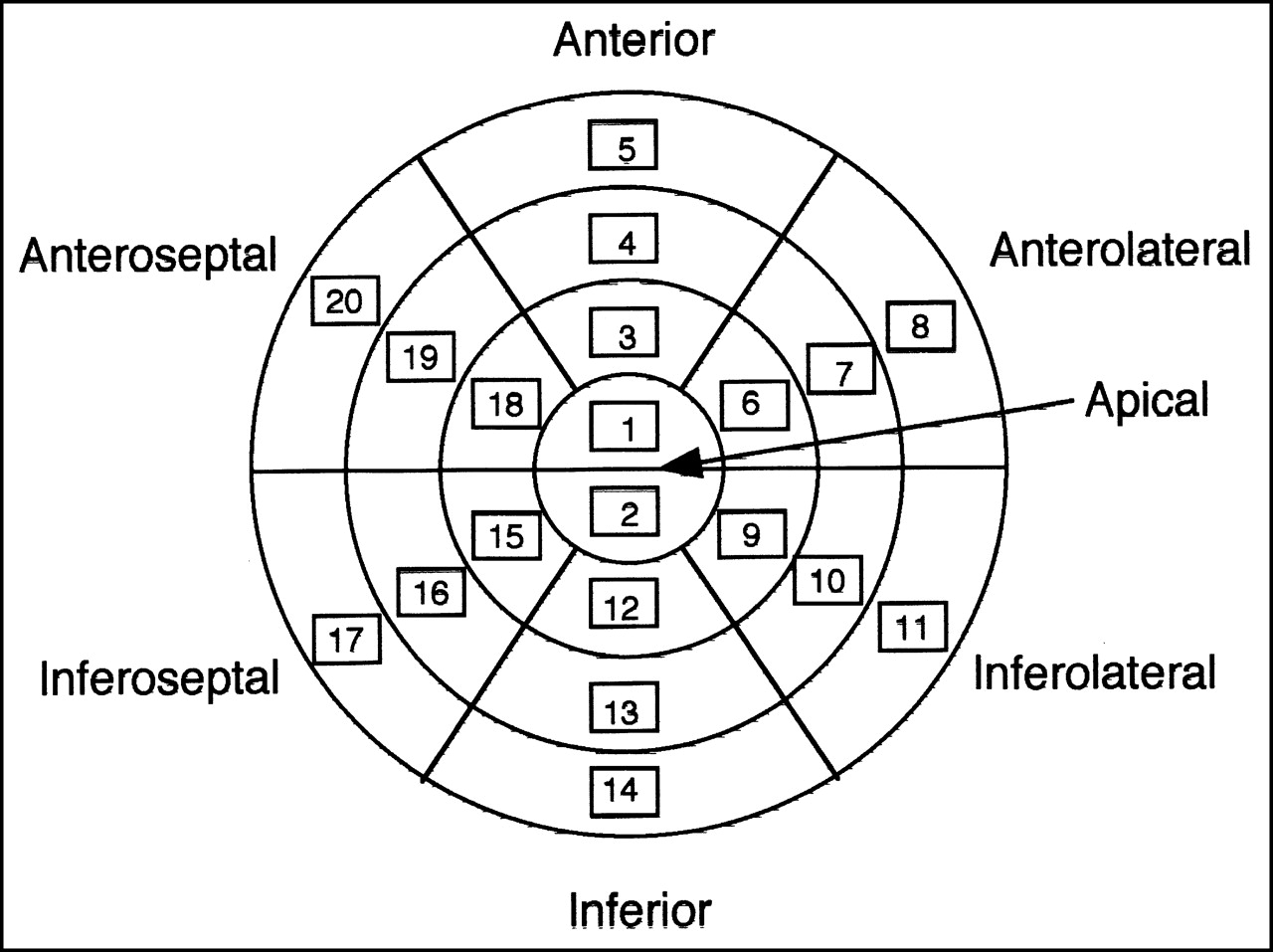
Left ventricular myocardium is divided into 20 segments, and uptake and washout rates in each section were determined.
Echocardiography
A transthoracic echocardiographic examination was performed within 1 wk of the 123I-MIBG injection in all patients with HCM. Standard M-mode and 2-dimensional echocardiographic studies, including long-axis, short-axis, and apical 4-chamber views, were performed to identify and quantify morphologic features of the left ventricular dimensions. The thickness of the septum and thickness of the left ventricular posterior wall were measured at the level of the tips of the mitral valve leaflets. The fractional shortening was calculated as the difference in end-diastolic and end-systolic dimensions divided by the end-diastolic dimension.
Statistical Analysis
Values are expressed as the mean ± SD. Differences between groups were analyzed by the Student unpaired t test. Categoric data were compared using χ2 analysis. Correlation was assessed by linear regression analysis and the Pearson correlation coefficient. The relationship between various 123I-MIBG scintigraphic variables and the percentage of fractional shortening was examined by multiple regression analysis. Only variables with P < 0.10 in the univariate analysis were included in the stepwise regression analysis. P < 0.05 was considered statistically significant.
RESULTS
Baseline Characteristics of Study Patients
The clinical and echocardiographic data of the patients with HCM are summarized in Table 1. The number of patients in the New York Heart Association functional classes I, II, III, and IV were 14, 9, 2, and 0, respectively. The main left ventricular hypertrophy was present in the anteroseptal wall in 19 patients (76%), in the apex in 2 patients (8%), and globally in 4 patients (16%).
Baseline Characteristics of HCM Patients
123I-MIBG Scintigraphic Data
123I-MIBG scintigraphic data in patients with HCM and control subjects are summarized in Table 2. The early uptake ratio of heart and mediastinum (early H/M) did not differ between the 2 groups. The delayed uptake ratio of heart and mediastinum (delayed H/M) was significantly lower, whereas the washout rate of the whole heart was significantly higher in the HCM group than in the control group.
123I-MIBG Scintigraphic Data
Polar maps of a control subject and a patient with HCM are shown in Figure 2. The regional variation, early uptake dispersion, SD of the early uptake, washout rate dispersion, and SD of the washout rate did not differ between the 2 groups. The delayed uptake dispersion and SD of the delayed uptake were smaller in HCM patients than in the control group. No differences were found between these variables in HCM patients with and without chest pain.

Polar maps of control subject (early image [A] and delayed image [B]) and patient with HCM (early image [C] and delayed image [D]).
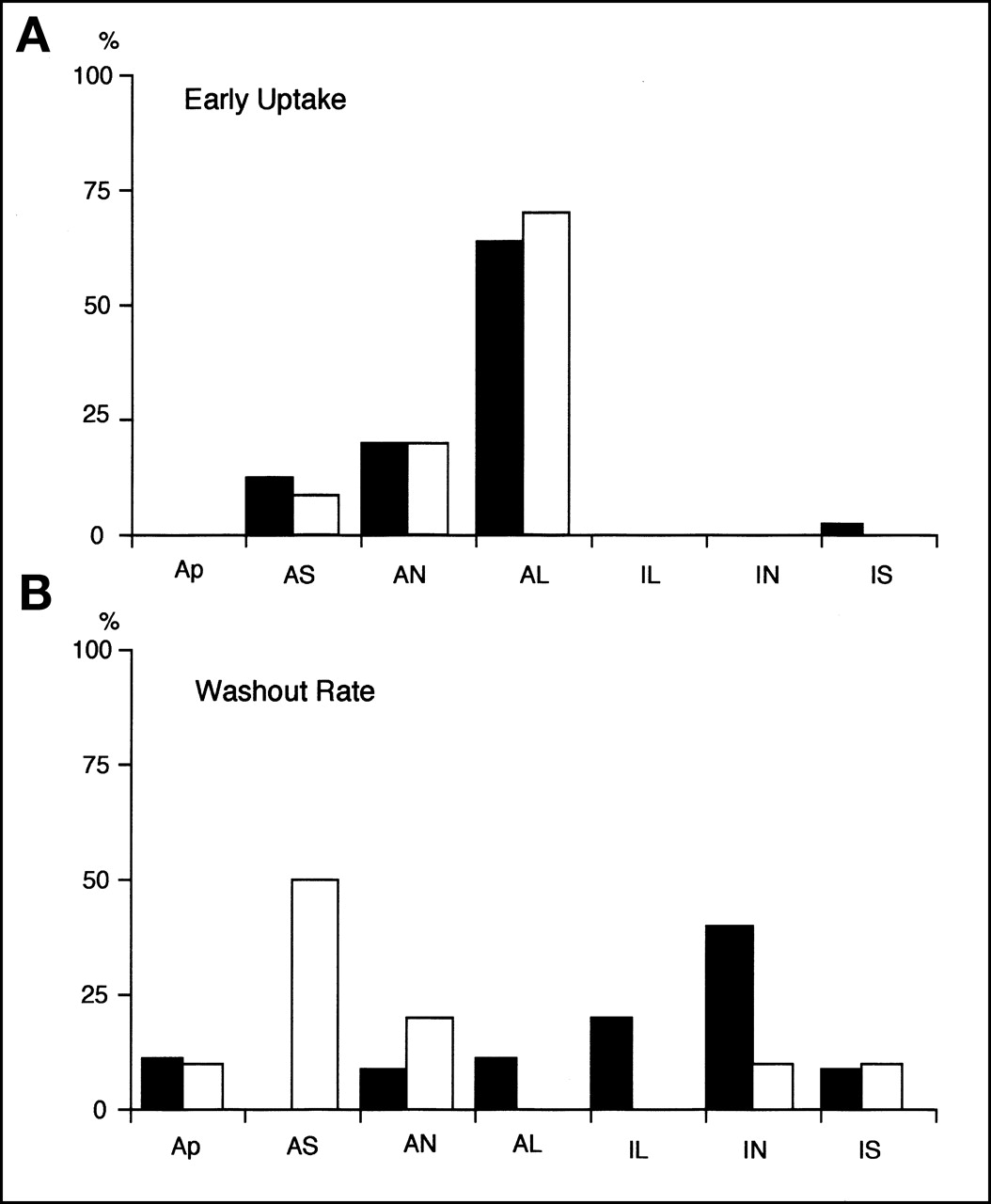
The region of maximal early uptake was the anterior or anterolateral wall in almost all patients with HCM and control subjects (HCM, 84%; control, 94%; not significant) (Fig. 3A). On the contrary, minimal early uptake was obtained frequently in the inferior or inferoseptal wall in patients with HCM and control subjects (HCM, 56%; control, 80%; not significant). The region of maximal delayed uptake was the anterior or anterolateral wall in almost all patients with HCM and control subjects (HCM, 68%; control, 100%; not significant). On the contrary, the region of minimal delayed uptake was the inferoseptal or inferior wall in patients with HCM in contrast to the anteroseptal or inferoseptal wall in control subjects, with a difference in distribution between the 2 groups (P = 0.0093). The region of maximal washout rate was the inferior or inferolateral wall in 60% of the patients with HCM, whereas it was the anteroseptal or anterior wall in 70% of the control subjects (P = 0.0047) (Fig. 3B). The minimal regional washout rate showed no specific region in either group.

Segment shows maximal early uptake (A) and maximal washout rate (B). Black bars = patients with HCM; white bars = control subjects. Segments shown in Figure 1 are identified as follows: Ap = apical; AS = anteroseptal; AN = anterior; AL = anterolateral; IL = inferolateral; IN = inferior; IS = inferoseptal.
Relationships Between 123I-MIBG Scintigraphic and Echocardiographic Variables in Patients with HCM
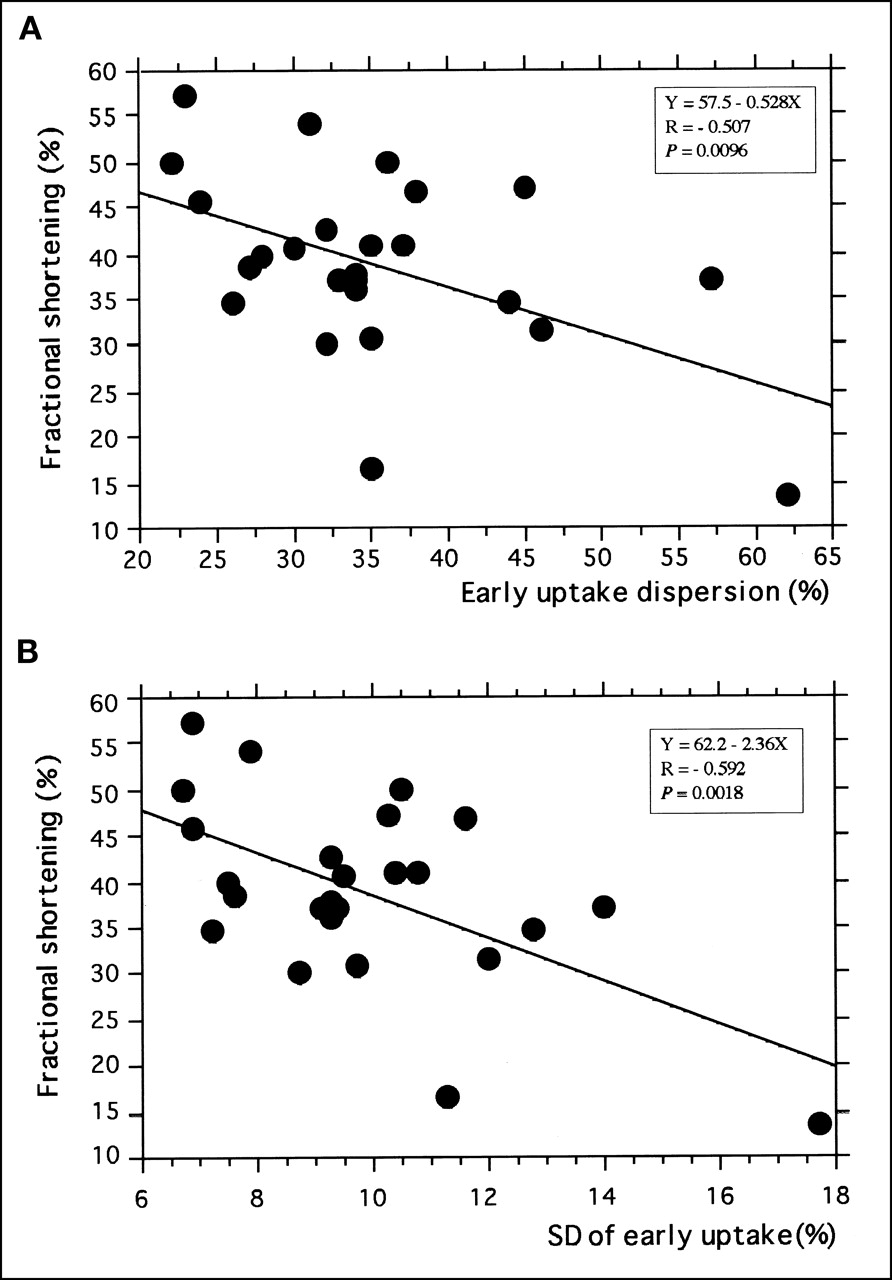
The correlation between 123I-MIBG scintigraphic and echocardiographic variables in patients with HCM are summarized in Table 3. The early H/M and washout rate of the whole heart did not correlate with the left ventricular end-diastolic dimension, the left ventricular end-systolic dimension, or the percentage of fractional shortening. However, the delayed H/M, the early uptake dispersion, and the SD of early uptake showed good correlation with the left ventricular end-diastolic dimension, the left ventricular end-systolic dimension, and the percentage of fractional shortening (Fig. 4). The delayed uptake dispersion did not correlate with these parameters, and the SD of delayed uptake correlated with the left ventricular end-systolic dimension and the percentage of fractional shortening. The washout rate dispersion and the SD of the washout rate showed only a weak correlation with the left ventricular end-diastolic dimension but showed no significant correlation with the left ventricular end-systolic dimension or the percentage of fractional shortening. A stepwise regression analysis revealed that the SD of the early uptake was the most powerful determinant for the percentage of fractional shortening in patients with HCM.

(A) Relationship between early uptake dispersion and percentage of fractional shortening. (B) Relationship between SD of segmental early uptake and percentage of fractional shortening.
Probability Values and Correlation Coefficients Obtained in Simple Regression Analysis for 123I-MIBG Scintigraphic Variables and Echocardiographic Indices in Patients with HCM
DISCUSSION
This study showed a correlation between regional variability of 123I-MIBG early uptake and cardiac function in patients with HCM. MIBG is an analog of noradrenaline and shares the same reuptake pathway within the cardiac synapse. Previous studies have shown that sympathetic nerve dysfunction, such as diabetes or transplanted heart, involves reduced early uptake of 123I-MIBG (8,9). These reports indicate that early uptake reflects mainly neural uptake (uptake 1). Ungerer et al. (10) reported that uptake 1 density and the tissue norepinephrine content showed marked regional variation in the left ventricle of patients with dilated cardiomyopathy. However, regional variations in uptake 1 density or the norepinephrine content in the heart with HCM are unclear. Moreover, the relationship between regional variation of cardiac sympathetic nerve activity and cardiac function in HCM is also unknown. In this study, the early uptake dispersion and the SD of early uptake correlated with the left ventricular volumes and the percentage of fractional shortening in patients with HCM—that is, patients with larger regional variations of early uptake after 123I-MIBG injections had larger left ventricular volumes and a lower percentage of fractional shortening.
The attenuation effect attributed to the left ventricular size should be considered first. However, this effect may be very small. The early uptake dispersion and the SD of the early uptake correlated not only with the left ventricular volumes but also with the percentage of fractional shortening in patients with HCM, and the percentage of fractional shortening was not significantly correlated with the left ventricular volumes. Even after the exclusion of inferior and inferoseptal segments from the analysis, the early uptake dispersion and the SD of the early uptake correlated significantly with the left ventricular volumes and the percentage of fractional shortening (data not shown). These results suggest that regional variability of early uptake was caused by cardiac dysfunction not by a change in the left ventricular volume.
Two possibilities may account for these observations. The first is an increase in heterogeneity by a greater increase in uptake in the high-uptake region, in which myocardial damage is small because of a compensation for cardiac dysfunction. In this condition, the washout rate in the high-uptake region may increase and the regional variability of the washout rate may also increase. However, we reasoned that this possibility is unlikely because there is no correlation between variability indices of the washout rate, the washout rate dispersion and the SD of the washout rate, and the percentage of fractional shortening. The second possibility is an increase in heterogeneity by a greater decrease in uptake in the low-uptake region. Whole cardiac early uptake (i.e., early H/M) in patients with HCM did not differ from that in control subjects. Because myocardial mass in patients with HCM was larger than that in control subjects, early uptake per myocardial unit was decreased in patients with HCM compared with that in the control group. The maximal early uptake region was the anterior or anterolateral wall in patients with HCM and control subjects. From these results, we hypothesize that the early uptake in the anteroseptal wall, which was the most hypertrophied region, in patients with HCM was decreased. In a study using PET, Li et al. (11) reported that neuronal uptake of catecholamines decreased in hypertrophied myocardium of patients with HCM. This report supports our hypothesis. The following findings suggest myocardial damage in the septum of patients with HCM: Systolic thickening and cyclic variation of integrated backscatter of the interventricular septum in HCM were small (12), washout rate in the interventricular septum in HCM increased (13), and regional wall motion abnormalities during dobutamine infusion occur more frequently in hypertrophied segments (14). In this study, the region of maximal washout rate was the inferior wall or inferolateral wall in patients with HCM in contrast to the anterior or anteroseptal wall in control subjects. From these findings, we suggest that the left ventricular systolic function may be preserved when contractility of inferior (posterior) wall is good. However, the left ventricular systolic function may be decreased when myocardial damage advances to the inferior wall in addition to the interventricular septum.
In this study, there was no significant difference in the early H/M and the early uptake variability indices between patients with HCM and control subjects. However, all of these indices are relative values. Evaluations that are based on absolute values with PET or other methods will be necessary in future studies. 123I-MIBG scintigraphy has been reported to be useful for the prognosis of patients with heart failure or dilated cardiomyopathy (15–17). The relationship between the heterogeneity of cardiac sympathetic nerve activity and the prognosis of patients with HCM should also be studied in the future. In addition, our study included relatively few patients. Additional studies with a larger number of patients are necessary to confirm and clarify our results.
CONCLUSION
The dispersion and the SD of the early uptake, the indices of regional 123I-MIBG variation, showed good correlation with the left ventricular dimensions and the percentage of fractional shortening in patients with HCM. The SD of the early uptake was a powerful statistical determinant for the percentage of fractional shortening in these patients. The heterogeneity of regional cardiac sympathetic nerve activity may be correlated with cardiac dysfunction in patients with HCM.
Footnotes
Received May 29, 2001; revision accepted Sep. 25, 2001.
For correspondence or reprints contact: Masami Shimizu, MD, Molecular Genetics of Cardiovascular Disorders, Division of Cardiovascular Medicine, Graduate School of Medical Science, Kanazawa University, Takara-machi 13-1, Kanazawa 920-8640, Japan.
E-mail: shimizu{at}med.kanazawa-u.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardiac 123I-MIBG Reflects Left Ventricular Functional Reserve in Patients with Nonobstructive Hypertrophic Cardiomyopathy
- 123I-MIBG Myocardial Scintigraphy in Patients with "Takotsubo" Cardiomyopathy
- Changes in Cardiac Sympathetic Nerve Innervation and Activity in Pathophysiologic Transition from Typical to End-Stage Hypertrophic Cardiomyopathy
- Cardiac Adrenergic Activity Is Associated with Left Ventricular Hypertrophy in Genetically Homogeneous Subjects with Hypertrophic Cardiomyopathy